
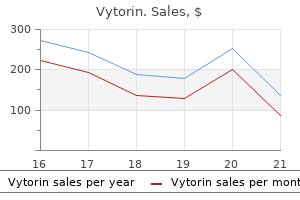
Vytorin dosages: 30 mg, 20 mg
Vytorin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Discount 20 mg vytorin with mastercard
Therefore cholesterol test kit dischem trusted 20 mg vytorin, fluid in the thick ascending limb of the loop of Henle turns into very dilute cholesterol unit conversion buy vytorin 30 mg, falling to a concentration of about 140 mOsm/L. The early distal tubule has properties similar to those of the thick ascending loop of Henle, so additional dilution of the tubular fluid to about 100 mOsm/L occurs as solutes are reabsorbed whereas water remains in the tubule. Because water reabsorption increases urea concentration within the tubular fluid, and since the internal medullary amassing ducts have specific urea transporters that greatly facilitate diffusion, much of the highly concentrated urea in the ducts diffuses out of the tubular lumen into the medullary interstitium. This absorption of the urea into the renal medulla contributes to the excessive osmolarity of the medullary interstitium and excessive concentrating capacity of the kidney. First, although sodium chloride is likely certainly one of the principal solutes that contribute to the hyperosmolarity of the medullary interstitium, the kidney can, when wanted, excrete a highly concentrated urine that contains little sodium chloride. The hyperosmolarity of the urine in these circumstances is as a end result of of high concentrations of different solutes, especially of waste products corresponding to urea. One situation during which this occurs is dehydration accompanied by low sodium intake. Second, massive quantities of dilute urine can be excreted without increasing sodium excretion. Therefore, if massive quantities of solute have to be excreted, they have to be accompanied by the minimal amount of water necessary to excrete them. For instance, if 600 milliosmoles of solute must be excreted every day, this requires at least zero. Conversely, when the urine is concentrated, solutes are excreted in extra of water. The complete clearance of solutes from the blood can be expressed because the osmolar clearance (Cosm). This is the amount of plasma cleared of solutes every minute, in the same means that clearance of a single substance is calculated: Uosm � V Cosm = Posm the place Uosm is the urine osmolarity, V is the urine circulate rate, and Posm is plasma osmolarity. For example, if the plasma osmolarity is 300 mOsm/L, urine osmolarity is 600 mOsm/L, and urine move rate is 1 ml/min (0. Free Water Clearance-Relative Rates at Which Solutes and Water Are Excreted urine-concentrating ability. When free water clearance is constructive, extra water is being excreted by the kidneys; when free water clearance is unfavorable, extra solutes are being faraway from the blood by the kidneys, and water is being conserved. Using the instance mentioned earlier, if urine flow price is 1 ml/min and osmolar clearance is 2 ml/min, free water clearance can be �1 ml/min. This implies that as a substitute of water being cleared from the kidneys in excess of solutes, the kidneys are actually returning water to the systemic circulation, as occurs during water deficits. Thus, every time urine osmolarity is bigger than plasma osmolarity, free water clearance is negative, indicating water conservation. Thus, water freed from solutes, called free water, is being misplaced from the body, and the plasma is being concentrated when free water clearance is optimistic. The primary abnormality noticed clinically in people with this condition is the massive volume of dilute urine. However, if water intake is restricted, as can happen in a hospital setting when fluid intake is restricted or the patient is unconscious. Desmopressin can be given by injection, as a nasal spray, or orally, and it rapidly restores urine output toward normal. In some circumstances, normal or Impairment within the capability of the kidneys to concentrate or dilute the urine appropriately can happen with one or more of the next abnormalities: 1. This condition is referred to as nephrogenic diabetes insipidus because the abnormality resides in the kidneys. In either case, massive volumes of dilute urine are formed, which causes dehydration unless fluid intake is increased by the identical quantity as urine quantity is increased. Many kinds of renal illnesses can impair the concentrating mechanism, especially those that damage the renal medulla (see Chapter 32 for further discussion). Also, impairment of the operate of the loop of Henle, as happens with diuretics that inhibit electrolyte reabsorption by this segment, such as furosemide, can compromise urineconcentrating ability. Lack of a prompt decrease in urine volume and an increase in urine osmolarity within 2 hours after injection of desmopressin is strongly suggestive of nephrogenic diabetes insipidus. The appropriate remedy for nephrogenic diabetes insipidus is to right, if attainable, the underlying renal disorder. The hypernatremia may also be attenuated by a low-sodium diet and administration of a diuretic that enhances renal sodium excretion, corresponding to a thiazide diuretic. Plasma sodium concentration is normally regulated within close limits of 140 to 145 mEq/L, with an average concentration of about 142 mEq/L. Osmolarity averages about 300 mOsm/L (282 mOsm/L when corrected for interionic attraction) and seldom modifications more than �2% to 3%. As mentioned in Chapter 25, these variables have to be exactly managed because they determine the distribution of fluid between the intracellular and extracellular compartments. For instance, with a plasma sodium concentration of 142 mEq/L, the plasma osmolarity can be estimated from this method to be about 298 mOsm/L. When osmolarity increases above regular due to water deficit, for instance, this suggestions system operates as follows: 1. An improve in extracellular fluid osmolarity (which in practical phrases means a rise in plasma sodium concentration) causes the special nerve cells known as osmoreceptor cells, positioned within the anterior hypothalamus close to the supraoptic nuclei, to shrink. Shrinkage of the osmoreceptor cells causes them to fire, sending nerve alerts to additional nerve cells within the supraoptic nuclei, which then relay these indicators down the stalk of the pituitary gland to the posterior pituitary. Normally, sodium ions and related anions (primarily bicarbonate and chloride) represent about 94% of the extracellular osmoles, with glucose and urea contributing about 3% to 5% of the entire osmoles. However, because urea easily permeates most cell membranes, it exerts little efficient osmotic pressure under steady-state situations. Therefore, the sodium ions in the extracellular fluid and related anions are the principal determinants of fluid motion across the cell membrane. Consequently, we are able to discuss the management of osmolarity and control of sodium ion focus on the same time. The elevated water permeability in the distal nephron segments causes increased water reabsorption and excretion of a small quantity of concentrated urine. Thus, water is conserved whereas sodium and other solutes continue to be excreted in the urine. This causes dilution of the solutes in the extracellular fluid, thereby correcting the preliminary excessively concentrated extracellular fluid. The opposite sequence of events occurs when the extracellular fluid turns into too dilute (hypo-osmotic). This in flip concentrates the physique fluids and returns plasma osmolarity towards regular. When the supraoptic and paraventricular nuclei are stimulated by increased osmolarity or other factors, nerve impulses move down these nerve endings, altering their membrane permeability and rising calcium entry. At the higher a half of this region is a structure known as the subfornical organ and, on the inferior part, is one other structure referred to as the organum vasculosum of the lamina terminalis. Between these two organs is the median preoptic nucleus, which has a number of nerve connections with the 2 organs, as well as with the supraoptic nuclei and blood stress management facilities in the medulla of the mind. It is also doubtless that they induce thirst in response to increased extracellular fluid osmolarity.
Cheap vytorin 30 mg with amex
Here cholesterol medication kidney failure generic 30 mg vytorin otc, the apotransferrin binds with free iron and also with certain iron compounds cholesterol levels for 35 year old man cheap vytorin 30 mg line, such as hemoglobin and myoglobin from meat, two of an important sources of iron in the diet. Then, by pinocytosis, the transferrin molecule, carrying its iron retailer, is absorbed into the epithelial cells and later released into the blood capillaries beneath these cells within the type of plasma transferrin. The porphyrin portion of the hemoglobin molecule is converted by the macrophages, via a sequence of stages, into the bile pigment bilirubin, which is released into the blood and later removed from the body by secretion by way of the liver into the bile. Some forms of anemia and their physiological causes are described in the following sections. For instance, exposure to high-dose radiation or chemotherapy for most cancers treatment can damage stem cells of the bone marrow, adopted in a couple of weeks by anemia. Likewise, excessive doses of sure toxic chemical compounds, similar to pesticides or benzene in gasoline, may trigger the identical effect. In autoimmune issues, corresponding to lupus erythematosus, the immune system begins attacking wholesome cells corresponding to bone marrow stem cells, which can lead to aplastic anemia. In about half of aplastic anemia circumstances the cause is unknown, a condition known as idiopathic aplastic anemia. Based on the sooner discussions of vitamin B12, folic acid, and intrinsic issue from the abdomen mucosa, one can readily perceive that loss of any certainly one of these can lead to sluggish replica of erythroblasts within the bone marrow. Thus, atrophy of the stomach mucosa, as happens in pernicious anemia, or lack of the complete stomach after surgical whole gastrectomy can lead to megaloblastic anemia. These crystals elongate the cell and provides it the looks of a sickle somewhat than a biconcave disc. The precipitated hemoglobin additionally damages the cell membrane, so the cells turn into extremely fragile, resulting in serious anemia. These antibodies make the Rh-positive cells fragile, leading to rapid rupture and inflicting the child to be born with a critical case of anemia. This change decreases the resistance to blood circulate in the peripheral blood vessels, up to now higher than normal quantities of blood move via the tissues and return to the guts, thereby greatly growing cardiac output. Moreover, hypoxia ensuing from diminished transport of oxygen by the blood causes the peripheral tissue blood vessels to dilate, allowing a further enhance in the return of blood to the heart and increasing the cardiac output to a nonetheless higher level-sometimes three to four instances regular. Thus, one of many main results of anemia is greatly increased cardiac output, as nicely as increased pumping workload on the guts. Even though 446 Chapter 33 Red Blood Cells, Anemia, and Polycythemia the increased cardiac output in individuals with anemia partially offsets the reduced oxygen-carrying effect of the anemia as a outcome of, even though every unit amount of blood carries only small portions of oxygen, the rate of blood move could also be elevated sufficient that just about normal quantities of oxygen are literally delivered to the tissues. Consequently, throughout exercise, which tremendously will increase tissue demand for oxygen, extreme tissue hypoxia outcomes and acute cardiac failure could ensue. A widespread sort of secondary polycythemia, called physiological polycythemia, occurs in those who live at altitudes of 14,000 to 17,000 feet, the place the atmospheric oxygen may be very low. The blood count is mostly 6 to 7 million/mm3, which allows these individuals to carry out moderately excessive levels of continuous work, even in a rarefied environment. In addition to physi- that regulate return of blood to the center, as discussed in Chapter 20, growing blood viscosity decreases the rate of venous return to the heart. Conversely, the blood quantity is significantly elevated in polycythemia, which tends to enhance venous return. The arterial pressure can be regular in most individuals with polycythemia, although in about one-third of them, the arterial strain is elevated. This means that the blood pressure�regulating mechanisms can normally offset the tendency for increased blood viscosity to improve peripheral resistance and, thereby, increase arterial strain. Beyond sure limits, nevertheless, these rules fail, and hypertension develops. The shade of the pores and skin depends to a fantastic extent on the quantity of blood in the pores and skin subpapillary venous plexus. Furthermore, as a outcome of blood passes sluggishly by way of the pores and skin capillaries before getting into the venous plexus, a bigger than regular amount of hemoglobin is deoxygenated. The blue color of all this deoxygenated hemoglobin masks the red colour of the oxygenated hemoglobin. Therefore, a person with polycythemia vera ordinarily has a ruddy complexion, with a bluish (cyanotic) tint to the pores and skin. Green R: Vitamin B12 deficiency from the attitude of a training hematologist. Renassia C, Peyssonnaux C: New insights into the hyperlinks between hypoxia and iron homeostasis. Polycythemia vera is attributable to a genetic aberration in the hemocytoblastic cells that produce the blood cells. In polycythemia vera, not solely does the hematocrit enhance, however the whole blood volume additionally will increase, generally to almost twice normal. Also, many blood capillaries turn into plugged by the viscous blood; the viscosity of the blood in polycythemia vera sometimes increases from the conventional of three instances the viscosity of water to 10 times that of water. Many of those infectious agents are capable of causing critical irregular physiological perform or even demise if they invade deeper tissues. We are also exposed intermittently to different extremely infectious micro organism and viruses apart from these which may be usually current, and these brokers can cause acute lethal diseases similar to pneumonia, streptococcal an infection, and typhoid fever. Our bodies have a special system for combating the different infectious and toxic brokers. These cells work collectively in two ways to forestall illness: (1) by actually destroying invading bacteria or viruses by phagocytosis; and (2) by forming antibodies and sensitized lymphocytes that will destroy or inactivate the invader. This article discusses the first of these methods, and Chapter 35 discusses the second. The granulocytes and monocytes defend the physique against invading organisms by ingesting them (by phagocytosis) or by releasing antimicrobial or inflammatory substances which have multiple results that help in destroying the offending organism. The lymphocytes and plasma cells function primarily in reference to the immune system, as discussed in Chapter 35. Finally, the perform of platelets is particularly to activate the blood-clotting mechanism, discussed in Chapter 37. They are formed partially in the bone marrow (granulocytes and monocytes and a few lymphocytes) and partially in the lymph tissue (lymphocytes and plasma cells). As we see later, the granulocytes and monocytes have a special capability to "search out and destroy" a international invader. The totally different cells of the myelocyte collection are proven: 1, myeloblast; 2, promyelocyte; three, megakaryocyte; 4, neutrophil myelocyte; 5, younger neutrophil metamyelocyte; 6, band neutrophil metamyelocyte; 7, neutrophil; 8, eosinophil myelocyte; 9, eosinophil metamyelocyte; 10, eosinophil; 11, basophil myelocyte; 12, basophil; 13�16, phases of monocyte formation. Then, when the necessity arises, various factors trigger them to be launched (these factors are discussed later). These megakaryocytes fragment within the bone marrow and the small fragments, known as platelets (or thrombocytes), then move into the blood. In instances of serious tissue infection, this whole life span is often shortened to only some hours as a outcome of the granulocytes proceed much more quickly to the contaminated area, carry out their capabilities, and in the process, are themselves destroyed. The monocytes also have a short transit time, 10 to 20 hours in the blood, before wandering by way of the capillary membranes into the tissues. These tissue macrophages are the premise of the tissue macrophage system (discussed in larger element later), which offers persevering with defense towards infection.
Diseases
- Batten disease
- Synovitis granulomatous uveitis cranial neuropathi
- Tricho-hepato-enteric syndrome
- Reflex sympathetic dystrophy syndrome
- Macroglobulinemia
- X-linked mental retardation De silva type
- Warman Mulliken Hayward syndrome
- Dementia, vascular
Buy vytorin 20 mg on line
Such ailments embrace the next: (1) chronic glomerulonephritis cholesterol medication niacin 20 mg vytorin cheap free shipping, which impacts primarily the glomeruli and infrequently causes tremendously increased permeability of the glomerular membrane; (2) amyloidosis cholesterol test by mail vytorin 20 mg buy generic on-line, which ends up from deposition of an irregular proteinoid substance in the walls of the blood vessels and seriously damages the basement membrane of the glomeruli; and (3) minimal-change nephrotic syndrome, which is associated with no major abnormality in the glomerular capillary membrane that could be detected with mild microscopy. As discussed in Chapter 27, minimalchange nephropathy has been related to an abnormal immune response and elevated T-cell secretion of cytokines that cause podocyte injury and elevated permeability to decrease molecular weight proteins, corresponding to albumin. Minimal-change nephropathy can occur in adults, however more incessantly it happens in children between the ages of two and 6 years. Increased permeability of the glomerular capillary membrane occasionally allows as a lot as forty grams of plasma protein loss into the urine every day, which is an excessive amount for a younger baby. As a consequence of this low colloid osmotic stress within the plasma, giant quantities of fluid leak from the capillaries all round the body into many of the tissues, inflicting severe edema, as mentioned in Chapter 25. In common, this condition may finish up from vascular, glomerular, or tubular injury that destroys individual nephrons, or it can contain major damage to the renal interstitium by poisons, medication, and bacterial infections. The an infection may finish up from various kinds of micro organism however particularly from Escherichia coli, which originate from fecal contamination of the urinary tract. These bacteria attain the kidneys both by means of the blood stream or, more commonly, by ascension from the lower urinary tract through the ureters to the kidneys. Although the traditional bladder is prepared to clear bacteria readily, there are two basic medical situations that will intervene with the conventional flushing of bacteria from the bladder: (1) the inability of the bladder to empty completely, leaving residual urine in the bladder; and (2) obstruction of urine outflow. With impaired ability to flush micro organism from the bladder, the micro organism multiply, and the bladder turns into inflamed, a condition termed cystitis. Once cystitis occurs, it may stay localized with out ascending to the kidney or, in some folks, micro organism may reach the renal pelvis because of a pathological situation by which urine is propelled up one or both of the ureters during micturition. Pyelonephritis begins within the renal medulla and due to this fact usually affects the operate of the medulla greater than it affects the cortex, a minimum of in the preliminary phases. Representative patterns of adaptation for different types of solutes in continual renal failure. Curve A shows the approximate adjustments in the plasma concentrations of solutes corresponding to creatinine and urea that are filtered and poorly reabsorbed. Curve B reveals the approximate concentrations for solutes such as phosphate, urate, and hydrogen ion. Curve C shows the approximate concentrations for solutes such as sodium and chloride. Further discount within the number of nephrons, nonetheless, leads to electrolyte and fluid retention, and dying usually ensues when the variety of nephrons falls under 5% to 10% of regular. In distinction to the electrolytes, most of the waste merchandise of metabolism, corresponding to urea and creatinine, accumulate nearly in proportion to the variety of nephrons which were destroyed. This maintenance is accomplished by tremendously reducing tubular reabsorption of these electrolytes. For instance, with a 75% loss of practical nephrons, each surviving nephron must excrete four instances as much sodium and four times as much quantity as under normal conditions (Table 32-6). Important results include: (1) generalized edema ensuing from water and salt retention; (2) acidosis ensuing from failure of the kidneys to rid the body of regular acidic merchandise; (3) excessive focus of the nonprotein nitrogens-especially urea, creatinine, and uric acid-resulting from failure of the body to excrete the metabolic finish products of proteins; and (4) excessive concentrations of other substances excreted by the kidney, including phenols, sulfates, phosphates, potassium, and guanidine bases. This complete condition is called uremia because of the high concentration of urea within the physique fluids. Development of isosthenuria in a affected person with decreased numbers of functional nephrons. One necessary impact of the speedy fee of tubular flow that happens in the remaining nephrons of diseased kidneys is that the renal tubules lose their ability to focus or dilute the urine fully. The concentrating capacity of the kidney is impaired mainly due to the following: (1) the fast flow of tubular fluid through the collecting ducts prevents sufficient water reabsorption; and (2) the fast flow by way of each the loop of Henle and accumulating ducts prevents the countercurrent mechanism from operating effectively to concentrate the medullary interstitial fluid solutes. The diluting mechanism within the kidney can be impaired when the number of nephrons decreases markedly because the fast flushing of fluid by way of the loops of Henle and excessive load of solutes such as urea trigger a comparatively high solute focus in the tubular fluid of this a part of the nephron. As a consequence, the diluting capacity of the 430 ter acute kidney damage begins, the total physique fluid content material might turn out to be only barely increased. The purpose for this, as discussed previously, is that the surviving nephrons excrete bigger amounts of salt and water. When kidney operate so decreased that dialysis is required to preserve life, hypertension nearly invariably develops. Chapter 32 Diuretics and Kidney Diseases In many of those sufferers, severe discount of salt consumption or removing of extracellular fluid by dialysis can management the hypertension. Some patients continue to have hypertension, even after excess sodium has been removed by dialysis. The nonprotein nitrogens include urea, uric ionized calcium focus, which, in flip, stimulates parathyroid hormone secretion. This secondary hyperparathyroidism then stimulates the release of calcium from bones, inflicting further bone demineralization. These nonprotein nitrogens, in general, are the tip merchandise of protein metabolism and should be removed from the body to ensure continued normal protein metabolism in the cells. The concentrations of these nonprotein nitrogens, significantly of urea, can rise to as excessive as 10 occasions regular throughout 1 to 2 weeks of total renal failure. Each day, the physique normally produces about 50 to 80 millimoles extra metabolic acid than metabolic alkali. Therefore, when the kidneys fail to perform, acid accumulates in the body fluids. The buffers of the physique fluids usually can buffer 500 to 1000 millimoles of acid with out deadly increases in extracellular fluid H+ focus, and the phosphate compounds within the bones can buffer a further few thousand millimoles of H+. However, when this buffering power is exhausted, the blood pH falls drastically, and the patient will turn out to be comatose and die if the pH falls below about 6. Abnormalities of kidney function can also cause hypertension, as discussed in Chapter 19. Not all forms of kidney disease cause hypertension as a result of injury to sure parts of the kidney causes uremia without hypertension. Nevertheless, some kinds of renal damage are notably vulnerable to trigger hypertension. A classification of kidney illness relative to hypertensive or nonhypertensive effects is offered in the following sections. Some specific forms of renal abnormalities that may trigger hypertension are as follows: 1. An instance is continual glomerulonephritis, which causes inflammation and thickening of the glomerular capillary membranes, thereby reducing the glomerular capillary filtration coefficient. An example is hypertension brought on by extreme aldosterone secretion, which will increase sodium reabsorption primarily in the cortical amassing tubules. Once hypertension has developed, renal excretion of sodium and water returns to regular as a end result of the high arterial strain causes stress natriuresis and pressure diuresis, so consumption and output of sodium and water become balanced as quickly as again. Likewise, when tubular reabsorption is increased, as happens with excessive aldosterone secretion, the urinary excretion rate is initially lowered however then returns to regular as arterial strain rises. Thus, after hypertension develops, there may be no obvious sign of impaired excretion of sodium and water apart from the hypertension.
Generic 20 mg vytorin
Often cholesterol test price philippines cheap vytorin 30 mg without prescription, pain from a spastic viscus occurs in the type of cramps cholesterol in raw shrimp buy 30 mg vytorin free shipping, with the pain increasing to a excessive diploma of severity after which subsiding. For example, every time a peristaltic wave travels alongside an overly excitable spastic intestine, a cramp occurs. The cramping sort of ache frequently happens in persons with appendicitis, gastroenteritis, constipation, menstruation, parturition, gallbladder disease, or ureteral obstruction. For instance, ache in one of many visceral organs typically is referred to an space on the physique floor. Knowledge of the various varieties of referred pain is important in medical analysis as a end result of, in plenty of visceral illnesses, the one scientific signal is referred pain. In this figure, branches of visceral pain fibers are proven to synapse in the spinal wire on the identical second-order neurons (1 and 2) that receive pain alerts from the skin. When the visceral ache fibers are stimulated, ache signals from the viscera are performed via no much less than a few of the similar neurons that conduct ache alerts from the skin, and the particular person has the feeling that the sensations originate in the skin. Extreme overfilling of a hollow viscus additionally can lead to ache, presumably because of overstretch of the tissues themselves. Overdistention can even collapse the blood vessels that encircle the viscus or that pass into its wall, thus perhaps promoting ischemic ache. Yet, the liver capsule is extraordinarily sensitive to each direct trauma and stretch, and the bile ducts are additionally delicate to pain. In the lungs, despite the very fact that the alveoli are insensitive, each the bronchi and the parietal pleura are very sensitive to ache. These parietal surfaces, like the skin, are supplied with intensive pain innervation from the peripheral spinal nerves. Second, sensations from the stomach and thorax are transmitted by way of two pathways to the central nervous system, the true visceral pathway and the parietal pathway. True visceral ache is transmitted via pain sensory fibers within the autonomic nerve bundles, and the sensations are referred to surface areas of the body which are typically removed from the painful organ. Conversely, parietal sensations are performed instantly into native spinal nerves from the parietal peritoneum, pleura, or pericardium, and these sensations are normally localized directly over the painful space. When visceral ache is referred to the nerves and enter the spinal wire between segments C3 and T5. These are the areas of the body floor that ship their very own somatosensory nerve fibers into the C3 to T5 wire segments. Usually, the pain is on the left side somewhat than on the best as a result of the left aspect of the guts is much more regularly concerned in coronary illness than is the best facet. The stomach originated approximately from the seventh to ninth thoracic segments of the embryo. Therefore, stomach pain is referred to the anterior epigastrium above the umbilicus, which is the surface area of the physique subserved by the seventh by way of ninth thoracic segments. Pain from the viscera is regularly local- surface of the body, the particular person typically localizes it in the dermatomal segment from which the visceral organ originated in the embryo, not essentially where the visceral organ now lies. Pain impulses cross first from the appendix by way of visceral ache fibers located inside sympathetic nerve bundles after which into the spinal cord at about T10 or T11; this ache is referred to an space across the umbilicus and is of the aching, cramping kind. Cross part of the spinal cord showing principal ascending tracts on the proper and principal descending tracts on the left. Tic Douloureux A lancinating or stabbing kind of ache occasionally occurs in some individuals over one aspect of the face within the sensory distribution area (or a half of the area) of the fifth or ninth nerves; this phenomenon is called tic douloureux (or trigeminal neuralgia or glossopharyngeal neuralgia). The ache looks like sudden electrical shocks, and it may seem for just a few seconds at a time or may be almost steady. The pain of tic douloureux can normally be blocked by surgically slicing the peripheral nerve from the hypersensitive area. The sensory portion of the fifth nerve is usually sectioned immediately inside the cranium, where the motor and sensory roots of the fifth nerve separate from each other, so that the motor portions, which are necessary for a lot of jaw movements, can be spared while the sensory elements are destroyed. Furthermore, sometimes the operation is unsuccessful, indicating that the lesion that causes the ache could be in the sensory nucleus within the brain stem and never in the peripheral nerves. Brown-S�quard Syndrome If the spinal wire is transected completely, all sensations and motor capabilities distal to the phase of transection are blocked, but if the spinal twine is transected on only one aspect, the Brown-S�quard syndrome occurs. All motor capabilities are blocked on the facet of the transection in all segments under the extent of the transection. Yet, solely a few of the modalities of sensation are misplaced on the transected side, and others are lost on the opposite side. The sensations of ache, heat, and cold-sensations served by the spinothalamic pathway- are lost on the opposite aspect of the physique in all dermatomes two to six segments beneath the level of the transection. These impulses trigger ache of the sharp sort directly over the irritated peritoneum in the right lower quadrant of the stomach. Some Clinical Abnormalities of Pain and Other Somatic Sensations Hyperalgesia-Hypersensitivity to Pain A ache nervous pathway typically turns into excessively excitable, which gives rise to hyperalgesia. Possible causes of hyperalgesia are the following: (1) excessive sensitivity of the pain receptors, known as major hyperalgesia; and (2) facilitation of sensory transmission, referred to as secondary hyperalgesia. An instance of primary hyperalgesia is the extreme sensitivity of sunburned pores and skin, which results from sensitization of the skin pain endings by local tissue merchandise from the burn-perhaps histamine, prostaglandins, and others. Secondary hyperalgesia frequently results from lesions in the spinal wire or the thalamus. Herpes Zoster (Shingles) Occasionally, herpesvirus infects a dorsal root ganglion. This infection causes severe pain within the dermatomal phase subserved by the ganglion, thus eliciting a segmental kind of ache that circles midway around the body. The illness is known as herpes zoster, or shingles, due to a skin eruption that often ensues. The reason for the ache is presumably an infection of the pain neuronal cells in the dorsal root ganglion by the virus. In addition to inflicting ache, the virus is carried by neuronal cytoplasmic flow outward by way of the neuronal peripheral axons to their cutaneous origins. Here the virus causes a rash that vesiculates within a few days and then crusts over within one other few days, all occurring inside the dermatomal area served by the contaminated dorsal root. Pain, Headache, and Thermal Sensations part in all dermatomes beneath the extent of the transection. Discrete "gentle touch" is impaired on the facet of the transection as a result of the principal pathway for the transmission of sunshine touch, the dorsal column, is transected. Headache Headaches are a kind of ache referred to the floor of the pinnacle from deep head constructions. Some complications result from ache stimuli arising contained in the skull, but others end result from ache arising outside the skull, corresponding to from the nasal sinuses. Even cutting or electrically stimulating the sensory areas of the cerebral cortex solely occasionally causes ache; as an alternative, it causes prickly kinds of paresthesias on the area of the body represented by the portion of the sensory cortex stimulated. Also, virtually any sort of traumatizing, crushing, or stretching stimulus to the blood vessels of the meninges could cause headache.
30 mg vytorin discount with mastercard
Thus cholesterol test kit walmart vytorin 30 mg order overnight delivery, by itself low carb cholesterol lowering foods purchase 30 mg vytorin fast delivery, lively transport of sodium chloride out of the thick ascending limb is capable of establishing only a 200-mOsm/L focus gradient, which is way less than that achieved by the countercurrent multiplier system. Once this fluid is in the ascending limb, extra ions are pumped into the interstitium and water remains in the tubular fluid till a 200-mOsm/L osmotic gradient is established, and the interstitial fluid osmolarity rises to 500 mOsm/L (step 5). Then, once again, fluid within the descending limb reaches equilibrium with the hyperosmotic medullary interstitial fluid (step 6) and, as the hyperosmotic tubular fluid from the descending limb of the loop of Henle flows into the ascending limb, still more solute is continuously pumped out of the tubules and deposited into the medullary interstitium. These steps are repeated time and again, with the net effect of adding more and more solute to the medulla in excess of water. With enough time, this course of gradually traps solutes in the medulla and multiplies the focus gradient established by the energetic pumping of ions out of the thick ascending loop of Henle, ultimately elevating the interstitial fluid osmolarity to 1200 to 1400 mOsm/L, as shown in step 7. Thus, the repetitive reabsorption of sodium chloride by the thick ascending loop of Henle and continued influx of recent sodium chloride from the proximal tubule into the loop of Henle known as the countercurrent multiplier. The sodium chloride reabsorbed from the ascending loop of Henle keeps including to the newly arrived sodium chloride, thus "multiplying" its focus in the medullary interstitium. Countercurrent multiplier system within the loop of Henle for producing a hyperosmotic renal medulla. As water flows up the ascending loop of Henle and into the distal and cortical accumulating tubules, little urea is reabsorbed as a outcome of these segments are impermeable to urea (see Table 29-1). As the tubular fluid flows into the inner medullary accumulating ducts, nonetheless more water reabsorption takes place, leading to a fair larger concentration of urea within the fluid. This high concentration of urea within the tubular fluid of the inner medullary accumulating duct causes urea to diffuse out of the tubule into the renal interstitial fluid. The simultaneous movement of water and urea out of the inside medullary collecting ducts maintains a excessive focus of urea in the tubular fluid and, eventually, in the urine, despite the very fact that urea is being reabsorbed. The basic role of urea in contributing to urineconcentrating ability is evidenced by the reality that individuals who ingest a high-protein food regimen, yielding massive quantities of urea as a nitrogenous waste product, can concentrate their urine significantly better than people whose protein consumption and urea manufacturing are low. Malnutrition is associated with a low urea focus within the medullary interstitium and appreciable impairment of urine-concentrating capacity. Recirculation of Urea from Collecting Duct to Loop of Henle Contributes to Hyperosmotic Renal Medulla. Note that the fluid leaving the loop of Henle is dilute but turns into concentrated as water is absorbed from the distal tubules and collecting tubules. The early distal tubule additional dilutes the tubular fluid as a result of this segment, just like the ascending loop of Henle, actively transports sodium chloride out of the tubule however is comparatively impermeable to water. Because large quantities of water are reabsorbed into the cortex, quite than into the renal medulla, this helps preserve the high medullary interstitial fluid osmolarity. Thus, by reabsorbing as much water as potential, the kidneys type extremely concentrated urine, excreting regular quantities of solutes in the urine while adding water back to the extracellular fluid and compensating for deficits of body water. Recirculation of urea absorbed from the medullary accumulating duct into the interstitial fluid. This urea diffuses into the thin loop of Henle, then passes by way of the distal tubules, and finally passes back into the accumulating duct. The recirculation of urea helps lure urea within the renal medulla and contributes to the hyperosmolarity of the renal medulla. Percentages of the filtered load of urea that remain in the tubules are indicated in the bins. This urea recirculation offers an extra mechanism for forming a hyperosmotic renal medulla. Without a particular medullary blood move system, the solutes pumped into the renal medulla by the countercurrent multiplier system can be rapidly dissipated. Two particular features of the renal medullary blood move contribute to the preservation of the high solute concentrations: 1. The medullary blood flow is low, accounting for lower than 5% of the entire renal blood circulate. This sluggish blood move is adequate to supply the metabolic needs of the tissues however helps minimize solute loss from the medullary interstitium. The vasa recta function countercurrent exchangers, minimizing the washout of solutes from the medullary interstitium. Blood enters and leaves the medulla through the vasa recta at the boundary of the cortex and renal medulla. The vasa recta, like other capillaries, are highly permeable to solutes within the blood, apart from the plasma proteins. As blood descends into the medulla toward the papillae, it becomes progressively more concentrated, partly by solute entry from the interstitium and partly by loss of water into the interstitium. By the time the blood reaches the tips of the vasa recta, it has a concentration of about 1200 mOsm/L, the identical as that of the medullary interstitium. As blood ascends again towards the cortex, it turns into progressively much less concentrated as solutes diffuse back out into the medullary interstitium and as water strikes into the vasa recta. The thick limb of the loop of Henle, distal tubule, and cortical accumulating tubule are all less permeable to urea, and solely small quantities of urea reabsorption usually happen in these tubular segments. Under steady-state conditions, the vasa recta carry away solely as a lot solute and water as is absorbed from the medullary tubules, and the Vasa recta mOsm/L 300 Solute 600 Solute 800 Solute a thousand H2O 600 600 350 Solute 600 H2O 800 H2O a thousand 1200 800 Solute 900 one thousand Solute Interstitium mOsm/L 300 excessive concentration of solutes established by the countercurrent mechanism is preserved. Certain vasodilators can mark- edly enhance renal medullary blood flow, thereby washing out a few of the solutes from the renal medulla and reducing the maximum urine-concentrating capacity. Large will increase in arterial pressure may increase the blood move of the renal medulla to a higher extent than in different areas of the kidney and tend to wash out the hyperosmotic interstitium, thereby decreasing urine-concentrating capacity. Plasma flowing down the descending limb of the vasa recta becomes more hyperosmotic because of diffusion of water out of the blood and diffusion of solutes from the renal interstitial fluid into the blood. In the ascending limb of the vasa recta, solutes diffuse back into the interstitial fluid, and water diffuses back into the vasa recta. Large amounts of solutes would be misplaced from the renal medulla without the U shape of the vasa recta capillaries. However, the proximal tubular membranes are extremely permeable to water so, every time solutes are reabsorbed, water also diffuses by way of the tubular membrane by osmosis. Therefore, the osmolarity of the fluid stays about the identical because the glomerular filtrate-300 mOsm/L. As fluid flows down the de- scending loop of Henle, water is absorbed into the medulla. Thus, the tubular fluid turns into more dilute as the sodium chloride diffuses out of the tubule and water stays in the tubule. Some of the urea absorbed into the medullary interstitium from the collecting ducts also diffuses into the ascending limb, thereby returning the urea to the tubular system and helping forestall its washout from the renal medulla. This urea recycling is an extra mechanism that contributes to the hyperosmotic renal medulla. The thick a part of the ascending loop of Henle is also nearly impermeable to water, but large amounts of sodium, chloride, potassium, and other ions are actively transported from the tubule into the medullary interstitium. Both the subfornical organ and organum vasculosum of the lamina terminalis have vascular provides that lack the typical blood�brain barrier that impedes the diffusion of most ions from the blood into mind tissue. This characteristic makes it potential for ions and other solutes to cross between the blood and local interstitial fluid on this area.
Vytorin 20 mg discount with mastercard
Defects are notably vulnerable to cholesterol levels normal values order vytorin 30 mg mastercard develop when the expectant mother contracts German measles (rubella) in the course of the first trimester of pregnancy cholesterol test las vegas vytorin 20 mg discount on-line. Some congenital defects of the heart are hereditary as a outcome of the same defect has been known to happen in that the main physiological problem caused by tetralogy 290 Chapter 23 Heart Valves and Heart Sounds; Valvular and Congenital Heart Defects similar twins, as properly as in succeeding generations. Children of patients surgically treated for congenital coronary heart disease have a few 10 times greater likelihood of getting congenital heart illness than different youngsters. Therefore, many kinds of synthetic heart-lung machines have been developed to take the place of the center and lungs through the course of an operation. Methods used for oxygenating blood embody the following: (1) effervescent oxygen via the blood and removing the bubbles from the blood earlier than passing it back into the patient; (2) dripping the blood downward over the surfaces of plastic sheets within the presence of oxygen; (3) passing the blood over surfaces of rotating discs; and (4) passing the blood between thin membranes or through thin tubes that are permeable to oxygen and carbon dioxide. The second cause is that fibrosis typically develops in the muscle, particularly in the subendocardial muscle the place the coronary blood circulate is poor, with fibrous tissue replacing degenerating muscle fibers. Because of the disproportionate increase in muscle mass relative to coronary blood flow, relative ischemia may develop as the cardiac muscle hypertrophies, and coronary blood circulate insufficiency might ensue. Anginal pain is due to this fact a frequent accompaniment of cardiac hypertrophy related to valvular and congenital coronary heart illness. Enlargement of the center can be associated with a higher risk for creating arrhythmias, which in flip can result in additional impairment of cardiac operate and sudden demise due to fibrillation. Ohukainen P, Ruskoaho H, Rysa J: Cellular mechanisms of valvular thickening in early and intermediate calcific aortic valve disease. One can calculate approximately how much hypertrophy will happen in each chamber of the heart by multiplying the ventricular output by the stress against which the ventricle should work, with an emphasis on pressure. Thus, hypertrophy occurs in most forms of valvular and congenital illness, typically inflicting the heart to weigh as much as 800 grams instead of the conventional 300 grams. Although the most common explanation for cardiac hypertrophy is hypertension, nearly all forms of cardiac ailments, together with valvular and congenital disease, can stimulate enlargement of the guts. Even the cardiovascular system itself-the coronary heart musculature, partitions of the blood vessels, vasomotor system, and different circulatory parts-begins to deteriorate, so the shock, as quickly as begun, is susceptible to turn into progressively worse. This situation may result from the next: (1) excessive metabolic price, so even a normal cardiac output is insufficient; or (2) abnormal tissue perfusion patterns, so many of the cardiac output is passing by way of blood vessels in addition to those who provide the native tissues with diet. For the current, it is very important notice that every one of them result in insufficient supply of vitamins to critical tissues and significant organs, as well as inadequate removal of mobile waste merchandise from the tissues. Therefore, any condition that reduces the cardiac output far below regular might result in circulatory shock. These abnormalities embrace specifically myocardial infarction but additionally poisonous states of the center, severe coronary heart valve dysfunction, heart arrhythmias, and different circumstances. The circulatory shock that results from diminished cardiac pumping capacity known as cardiogenic shock. The most typical reason for decreased venous return is diminished blood volume, however venous return can be reduced because of decreased vascular tone, particularly of the venous blood reservoirs, or obstruction to blood flow sooner or later in the circulation, especially within the venous return pathway to the center. In the minds of many physicians, the arterial pressure level is the principal measure of adequacy of circulatory perform. At instances, an individual may be in extreme shock and still have an nearly normal arterial stress because of highly effective nervous reflexes that hold the strain from falling. In most forms of shock, especially shock caused by extreme blood loss, the arterial blood strain decreases on the identical time the cardiac output decreases, although normally not as a lot. That is, the inadequate blood flow causes the physique tissues to begin deteriorating, including the center and circulatory system. This deterioration causes even larger decreases in cardiac output, and a vicious cycle ensues, with progressively rising circulatory shock, less enough tissue perfusion, and more shock till demise occurs. A nonprogressive stage (sometimes referred to as the compensated stage), during which the normal circulatory compensatory mechanisms eventually cause full restoration without assist from outside therapy. A progressive stage, in which, with out therapy, the shock becomes steadily worse till demise happens. We will now focus on the levels of circulatory shock caused by decreased blood volume, which illustrate the basic ideas. Sympathetic Reflex Compensations in Shock-Their Special Value to Maintain Arterial Pressure. Hemorrhage decreases the filling stress of the circulation and, as a consequence, decreases venous return. These reflexes stimulate the sympathetic vasoconstrictor system in most tissues of the physique, leading to three necessary results: 1. The arterioles constrict in most parts of the systemic circulation, thereby increasing the whole peripheral resistance. The veins and venous reservoirs constrict, thereby serving to preserve enough venous return, despite diminished blood quantity. Heart activity will increase markedly, typically increasing the guts rate from the conventional worth of 72 beats/min to as high as a hundred and sixty to a hundred and eighty beats/min. In the absence of the sympathetic reflexes, only 15% to 20% of the blood quantity could be eliminated over a period of 30 minutes before a person dies; in distinction, an individual can maintain a 30% to 40% lack of blood quantity when the reflexes are intact. Therefore, these reflexes extend the amount of blood loss that can occur with out inflicting demise to about twice that which is feasible in their absence. Greater Effect of Sympathetic Nervous Reflexes in Maintaining Arterial Pressure Than in Maintaining Cardiac Output. The reason for this distinction is that the sympathetic reflexes are geared extra for sustaining arterial strain than for sustaining cardiac output. They enhance the arterial pressure mainly by growing the whole peripheral resistance, which has no helpful effect on cardiac output. However, the sympathetic constriction of the veins is important to keep venous return and cardiac output from falling an extreme quantity of, in addition to their role in maintaining arterial strain. This second plateau outcomes from activation of the central nervous system ischemic response, which causes excessive stimulation of the sympathetic nervous system when the brain begins to expertise lack of oxygen or extra buildup of carbon dioxide, as mentioned in Chapter 18. This impact of the central nervous system ischemic response can be known as the "last-ditch stand" of the sympathetic reflexes of their attempt to keep the arterial stress from falling too low. A particular worth of the maintenance of nor- mal arterial pressure, even in the presence of decreasing cardiac output, is safety of blood circulate by way of the coronary and cerebral circulations. In addition, in both vascular beds, native blood flow autoregulation is great, which prevents moderate decreases in arterial strain from significantly reducing their blood flows. Therefore, shock of this lesser degree known as nonprogressive shock or compensated shock, meaning that the sympathetic reflexes and different elements compensate enough to stop additional deterioration of the circulation. The components that cause an individual to recover from moderate degrees of shock are the adverse suggestions control mechanisms of the circulation that attempt to return cardiac output and arterial strain again to normal levels. Baroreceptor reflexes, which elicit powerful sympathetic stimulation of the circulation 2. Increased secretion by the posterior pituitary gland of vasopressin (antidiuretic hormone), which constricts the peripheral arterioles and veins and tremendously will increase water retention by the kidneys 6. Increased secretion by the adrenal medullae of epinephrine and norepinephrine, which constricts the peripheral arterioles and veins and will increase the guts rate 7. The animals on this experiment were anesthetized and bled quickly till their arterial pressures fell to different ranges.
Pomegranate Leaf Extract (Pomegranate). Vytorin.
- Are there any interactions with medications?
- How does Pomegranate work?
- Dosing considerations for Pomegranate.
- High cholesterol (hyperlipidemia), heart disease, intestinal worm infestations, high blood pressure (hypertension), hardening of the arteries (atherosclerosis), obesity and weight loss, gum disease, fungal mouth infections, diarrhea, dysentery, sore throat, hemorrhoids, prostate cancer, and other conditions.
- What is Pomegranate?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96406
Generic vytorin 20 mg overnight delivery
Calcium entering the cell then activates calcium release channels test your cholesterol discount vytorin 20 mg without prescription, also known as ryanodine receptor channels cholesterol jaki powinien byc 20 mg vytorin cheap mastercard, within the sarcoplasmic reticulum membrane, triggering the discharge of calcium into the sarcoplasm. Calcium ions within the sarcoplasm then interact with troponin to initiate cross-bridge formation and contraction by the same primary mechanism as that described for skeletal muscle in Chapter 6. The T tubules of cardiac muscle, however, have a diameter five instances as great as that of the skeletal muscle tubules, which implies a quantity 25 instances as great. The strength of contraction of cardiac muscle relies upon to a great extent on the concentration of calcium ions in the extracellular fluids. In distinction, the energy of skeletal muscle contraction is hardly affected by reasonable adjustments in extracellular fluid calcium concentration. This is because skeletal muscle contraction is brought on almost completely by calcium ions launched from the sarcoplasmic reticulum inside the skeletal muscle fiber. At the top of the plateau of the cardiac motion potential, the inflow of calcium ions to the inside of the muscle fiber is all of a sudden reduce off, and calcium ions within the sarcoplasm are quickly pumped back out of the muscle fibers into the sarcoplasmic reticulum and T tubule�extracellular fluid house. Cardiac muscle begins to con- and continues to contract until a couple of milliseconds after the action potential ends. Therefore, the length of contraction of cardiac muscle is mainly a function of the period of the motion potential, including the plateau- about zero. Each cycle is initiated by the spontaneous era of an action potential within the sinus node, as explained in Chapter 10. This node is located in the superior lateral wall of the right atrium close to the opening of the superior vena cava, and the motion potential travels from right here quickly via both atria after which through the A-V bundle into the ventricles. This delay permits the atria to contract ahead of ventricular contraction, thereby pumping blood into the ventricles before the strong ventricular contraction begins. Events of the cardiac cycle for left ventricular operate, showing changes in left atrial stress, left ventricular pressure, aortic pressure, ventricular quantity, the electrocardiogram, and the phonocardiogram. These are electrical voltages generated by the center and recorded by the electrocardiogram from the floor of the physique. The P wave is attributable to the spread of depolarization by way of the atria and is followed by atrial contraction, which causes a slight rise in the atrial stress curve immediately after the electrocardiographic P wave. Finally, the ventricular T wave represents the stage of repolarization of the ventricles when the ventricular muscle fibers start to loosen up. Diastole and Systole the whole duration of the cardiac cycle, together with systole and diastole, is the reciprocal of the guts fee. For instance, if the heart fee is seventy two beats/min, the period of the cardiac cycle is 1/72 min/beat-about zero. The high three curves show the strain changes in the aorta, left ventricle, and left atrium, respectively. The fourth curve depicts the modifications in left ventricular volume, the fifth depicts the electrocardiogram, and the sixth depicts a phonocardiogram, which is a recording of the sounds produced by the heart-mainly by the guts valves-as it pumps. It is especially necessary that the reader study this determine intimately and understand the causes of all the events shown. When coronary heart fee increases, the length of each cardiac cycle decreases, together with the contraction and rest phases. The duration of the action potential and systole additionally decrease, but not by as nice a share as diastole. Then, atrial contraction normally causes a further 20% filling of the ventricles. Therefore, the atria function as primer pumps that improve the ventricular pumping effectiveness as much as 20%. However, the heart can proceed to operate underneath most conditions even with out this further 20% effectiveness as a result of Chapter 9 Cardiac Muscle: the Heart as a Pump and Function of the Heart Valves it normally has the capability of pumping 300% to 400% extra blood than is required by the resting physique. Therefore, when the atria fail to function, the difference is unlikely to be seen unless an individual exercises; then, symptoms of heart failure often develop, particularly shortness of breath. In the Outflow of Blood from the Ventricles During Systole Period of Isovolumic (Isometric) Contraction. Ordinarily, the right atrial stress increases 4 to 6 mm Hg throughout atrial contraction, and the left atrial stress will increase about 7 to eight mm Hg. The v wave occurs toward the end of ventricular contraction; it results from sluggish flow of blood into the atria from the veins while the A-V valves are closed throughout ventricular contraction. Then, when ventricular contraction is over, the A-V valves open, allowing this saved atrial blood to flow rapidly into the ventricles, inflicting the v wave to disappear. Therefore, throughout this era, contraction is happening in the ventricles, however no emptying happens. This interval is recognized as the interval of isovolumic or isometric contraction, which means that cardiac muscle tension is increasing but little or no shortening of the muscle fibers is happening. Immediately, blood is ejected out of the ventricles into the aorta and pulmonary artery. Approximately 60% of the blood in the ventricles at the finish of diastole is ejected throughout systole; about 70% of this portion flows out during the first third of the ejection period, with the remaining 30% emptying during the next two thirds. Therefore, the first third known as the interval of rapid ejection, and the final two thirds known as the period of slow ejection. At the During ventricular systole, giant quantities of blood accumulate in the proper and left atria due to the closed A-V valves. In a healthy heart, the interval of fast filling lasts for about the first third of diastole. During the middle third of diastole, solely a small amount of blood usually flows into the ventricles. This is blood that continues to empty into the atria from the veins and passes via the atria instantly into the ventricles. During the final third of diastole, the atria contract and provides an extra thrust to the inflow of blood into the ventricles. This mechanism accounts for about 20% of the filling of the ventricles throughout every heart cycle. The ventricles stiffen with growing older or diseases that trigger cardiac fibrosis similar to high blood pressure or diabetes mellitus. This causes much less blood to fill the ventricles within the early portion of diastole and requires more volume (preload; mentioned later) or more filling from the later atrial contraction to maintain enough cardiac output. The elevated pressures in the distended large arteries that have simply been filled with blood from the contracted ventricles immediately push blood again towards the ventricles, which snaps the aortic and pulmonary valves closed. During this period, the intraventricular pressures quickly lower again to their low diastolic ranges. During diastole, normal filling of the ventricles will increase the quantity of each ventricle to about a hundred and ten to 120 ml. Then, because the ventricles empty throughout systole, the quantity decreases by about 70 ml, which is recognized as the stroke volume output. The remaining quantity in every ventricle, about forty to 50 ml, is called the end-systolic volume. The ejection fraction proportion is often used clinically to assess cardiac systolic (pumping) capability.
Vytorin 30 mg generic with visa
The reabsorption of water in medullary accumulating ducts is managed by the focus of antidiuretic hormone cholesterol lowering drugs definition order 30 mg vytorin with mastercard. Thus good cholesterol chart levels discount vytorin 20 mg amex, the intercalated cells play a key role in acid� base regulation of the body fluids. This special characteristic offers an necessary mechanism for controlling the degree of dilution or focus of the urine. Unlike the cortical accumulating tubule, the medullary accumulating duct is permeable to urea, and there are special urea transporters that facilitate urea diffusion across the luminal and basolateral membranes. The medullary accumulating duct is capable of secreting hydrogen ions against a big concentration 354 gradient, as additionally occurs within the cortical amassing tubule. Thus, the medullary amassing duct additionally plays a key function in regulating acid-base balance. If a greater share of water is reabsorbed, the substance becomes more concentrated. If a higher share of the solute is reabsorbed, the substance becomes extra diluted. All the values on this figure represent the tubular fluid focus divided by the plasma focus of a substance. If plasma concentration of the substance is assumed to be fixed, any change within the tubular fluid/plasma concentration ratio reflects changes in tubular fluid focus. As the filtrate moves alongside the tubular system, the concentration rises progressively to higher than 1. Conversely, the substances represented at the backside of the figure, corresponding to glucose and amino acids, are all strongly reabsorbed. These are all substances that the physique must preserve, and almost none of them are misplaced within the urine. Tubular Fluid/Plasma Inulin Concentration Ratio Can Be Used to Assess Water Reabsorption by Renal Tubules. Changes in inulin focus at completely different points along the renal tubule, therefore, replicate modifications in the amount of water present within the tubular fluid. For example, the tubular fluid/plasma focus ratio for inulin rises to about 3. Some diploma of glomerulotubular balance also occurs in different tubular segments, particularly the loop of Henle. It is evident that the mechanisms for glomerulotubular steadiness can happen independently of hormones and may be demonstrated in fully isolated kidneys or even in utterly isolated proximal tubular segments. Changes in peritubular capillary reabsorption can in flip influence the hydrostatic and colloid osmotic pressures of the renal interstitium and, finally, reabsorption of water and solutes from the renal tubules. An important characteristic of tubular reabsorption is that reabsorption of some solutes may be regulated independently of others, particularly through hormonal management mechanisms. Fluid and electrolytes are reabsorbed from the tubules into the renal interstitium and from there into the peritubular capillaries. Reabsorption across the peritubular capillaries can be calculated as follows: Reabsorption = Kf � Net reabsorptive force the web reabsorptive force represents the sum of the hydrostatic and colloid osmotic forces that favor or oppose reabsorption across the peritubular capillaries. This opposition to fluid reabsorption is more than counterbalanced by the colloid osmotic pressures that favor reabsorption. The plasma colloid osmotic pressure, which favors reabsorption, is about 32 mm Hg, and the colloid osmotic pressure of the interstitium, which opposes reabsorption, is 15 mm Hg, inflicting a web colloid osmotic pressure of about 17 mm Hg, favoring reabsorption. Therefore, subtracting the net hydrostatic forces that oppose reabsorption (7 mm Hg) from the web colloid osmotic forces that favor reabsorption (17 mm Hg) gives a net reabsorptive force of about 10 mm Hg. This value is excessive, just like that found in the glomerular capillaries, but in the opposite direction. The different issue that contributes to the excessive fee of fluid reabsorption within the peritubular capillaries is a large filtration coefficient (Kf) due to the high hydraulic conductivity and enormous floor space of the capillaries. Because the reabsorption fee is often about 124 ml/ min and internet reabsorption pressure is 10 mm Hg, Kf normally is about 12. The peritubular capillary hydrostatic pressure is influenced by the arterial pressure and resistances of the afferent and efferent arterioles as follows: 1. Increases in arterial stress are probably to raise peritubular capillary hydrostatic strain and reduce the reabsorption fee. This impact is buffered to some extent by autoregulatory mechanisms that maintain relatively fixed renal blood circulate, in addition to relatively constant hydrostatic pressures in the renal blood vessels. An enhance in resistance of the afferent or efferent arterioles reduces peritubular capillary hydrostatic strain and tends to increase reabsorption price. Although constriction of the efferent arterioles will increase glomerular capillary hydrostatic stress, it lowers peritubular capillary hydrostatic strain. The second main determinant of peritubular capillary reabsorption is the colloid osmotic strain of the plasma in these capillaries; elevating the colloid osmotic strain increases peritubular capillary reabsorption. The colloid osmotic pressure of peritubular capillaries is set by the next: (1) the systemic plasma colloid osmotic strain (increasing the plasma protein focus of systemic blood tends to increase peritubular capillary colloid osmotic stress, thereby rising reabsorption); and (2) the filtration fraction-the larger the filtration fraction, the larger the fraction of plasma filtered by way of the glomerulus and, consequently, the extra concentrated the protein becomes within the plasma that continues to be behind. Thus, growing the filtration fraction also tends to improve the peritubular capillary reabsorption fee. Changes in the peritubular capillary Kf can also influence the reabsorption rate as a outcome of Kf is a measure of the permeability and surface space of the capillaries. Increases in Kf raise reabsorption, whereas decreases in Kf lower peritubular capillary reabsorption. Table 28-2 summarizes the components that may influence the peritubular capillary reabsorption price. Ultimately, modifications in peritubular capillary the 2 determinants of peritubular capillary reabsorption 356 physical forces influence tubular reabsorption by changing the physical forces within the renal interstitium surrounding the tubules. This action in flip raises renal interstitial fluid hydrostatic strain and reduces interstitial fluid colloid osmotic strain due to dilution of the proteins within the renal interstitium. These modifications then decrease the web reabsorption of fluid from the renal tubules into the interstitium, particularly in the proximal tubules. Once the solutes enter the intercellular channels or renal interstitium by lively transport or passive diffusion, water is drawn from the tubular lumen into the interstitium by osmosis. Furthermore, as quickly as the water and solutes are in the interstitial spaces, they can be swept up into the peritubular capillaries or diffuse back via the epithelial junctions into the tubular lumen. The so-called tight junctions between the epithelial cells of the proximal tubule are literally leaky, so appreciable amounts of sodium can diffuse in each instructions by way of these junctions. With the normal excessive price of peritubular capillary reabsorption, the web movement of water and solutes is into the peritubular capillaries, with little backleak into the lumen of the tubule. The opposite is true when peritubular capillary reabsorption increases above the traditional degree. An initial increase in reabsorption by the peritubular capillaries tends to reduce interstitial fluid hydrostatic stress and lift interstitial fluid colloid osmotic strain. Both these forces favor motion of fluid and solutes out of the tubular lumen and into the interstitium; subsequently, backleak of water and solutes into the tubular lumen is decreased, and internet tubular reabsorption is elevated. Reduced peritubular capillary reabsorption, in flip, decreases the online reabsorption of solutes and water by growing the quantities of solutes and water that leak again into the tubular lumen via the tight junctions of the tubular epithelial cells, particularly within the proximal tubule. In general, forces that enhance peritubular capillary reabsorption also increase reabsorption from the renal tubules. Conversely, hemodynamic changes that inhibit peritubular capillary reabsorption additionally inhibit tubular reabsorption of water and solutes.
30 mg vytorin otc
Among the damaging mobile results which are known to happen in most physique tissues are the next: 1 zoloft cholesterol levels 30 mg vytorin overnight delivery. Active transport of sodium and potassium by way of the cell membrane is significantly diminished cholesterol definition in food generic 30 mg vytorin. As a outcome, sodium and chloride accumulate in the cells, and potassium is misplaced from the cells. This phenomenon decreases the blood quantity much more, with a resultant further decrease in cardiac output, making the shock nonetheless more extreme. Mitochondrial exercise within the liver cells, in addition to in plenty of different tissues of the body, becomes severely depressed. Lysosomes within the cells in widespread tissue areas begin to break open, with intracellular launch of hydrolases, which cause additional intracellular deterioration. Cellular metabolism of nutrients, such as glucose, ultimately becomes greatly depressed within the final levels of shock. The actions of some hormones are depressed as nicely, together with nearly 100 percent depression of the actions of insulin. All these effects contribute to further deterioration of many organs of the physique, together with particularly the following: (1) the liver, with melancholy of its many metabolic and detoxification functions; (2) the lungs, with eventual development of pulmonary edema and poor ability to oxygenate the blood; and (3) the guts, thereby further miserable its contractility. Not all cells of the Positive Feedback Deterioration of Tissues in Shock and Vicious Cycle of Progressive Shock. All the fac- physique are equally damaged by shock as a end result of some tissues have better blood supplies than others. For example, the cells adjoining to the arterial ends of capillaries obtain higher vitamin than cells adjoining to the venous ends of the same capillaries. Therefore, extra nutritive deficiency happens around the venous ends of capillaries than elsewhere. Nevertheless, the cardiac lesions play an essential role in leading to the final irreversible stage of shock. Deteriorative lesions additionally occur within the kidneys, especially in the epithelium of the kidney tubules, resulting in kidney failure and occasionally uremic demise a number of days later. Deterioration of the lungs also typically results in respiratory distress and dying a quantity of days later, called the shock lung syndrome. Metabolic derangements that oc- tors just discussed that may lead to additional progression of shock are forms of constructive feedback-that is, each enhance within the degree of shock causes a further increase in the shock. In mild levels of shock, the adverse feedback mechanisms of the circulation, including sympathetic reflexes, reverse stress-relaxation mechanism of the blood reservoirs, and absorption of fluid into the blood from the interstitial areas, can easily overcome the optimistic suggestions influences and, due to this fact, trigger restoration. Ironically, even on this irreversible stage, therapy can, on rare occasions, return the arterial strain and even the cardiac output to normal or close to normal for short durations, however the circulatory system nonetheless continues to deteriorate, and death ensues in another jiffy to few hours. However, the cardiac output quickly begins to fall once more, and subsequent transfusions have much less and less effect. Progressive stage Transfusion cur in shocked tissue can lead to acidosis all through the body. This outcomes from poor supply of oxygen to the tissues, which greatly diminishes oxidative metabolism of the foodstuffs. When this happens, the cells get hold of most of their energy by the anaerobic strategy of glycolysis, which leads to excess lactic acid in the blood. In addition, poor blood move via tissues prevents normal removal of carbon dioxide. The carbon dioxide reacts locally in the cells with water to type high concentrations of intracellular carbonic acid, which, in turn, reacts with varied tissue chemical compounds to kind further intracellular acidic substances. Thus, another deteriorative effect of shock is generalized and local tissue acidosis, resulting in further progression of the shock. Therefore, in extreme shock, a stage is finally reached at which the individual will die, despite the actual fact that vigorous remedy may still return the cardiac output to normal for short durations. The high-energy phos- phate reserves in the tissues of the body, especially within the liver and coronary heart, are greatly diminished in extreme shock. Essentially all of the creatine phosphate has been degraded, and almost all of the adenosine triphosphate has downgraded to adenosine diphosphate, adenosine monophosphate and, ultimately, adenosine. Loss of fluid from all fluid compartments of the body is called dehydration; this situation can also cut back the blood volume and trigger hypovolemic shock just like that ensuing from hemorrhage. Some of the causes of this sort of shock are the following: (1) extreme sweating; (2) fluid loss in severe diarrhea or vomiting; (3) excess loss of fluid by the kidneys; (4) insufficient consumption of fluid and electrolytes; or (5) destruction of the adrenal cortices, with loss of aldosterone secretion and consequent failure of the kidneys to reabsorb sodium, chloride, and water, which happens within the absence of the adrenocortical hormone aldosterone. Often, the shock results merely from hemorrhage caused by the trauma, however it can also occur even with out hemorrhage as a result of extensive contusion of the body can injury the capillaries sufficiently to allow excessive loss of plasma into the tissues. This phenomenon results in tremendously lowered plasma quantity, with resultant hypovolemic shock. Various attempts have been made to implicate poisonous elements released by the traumatized tissues as one of the causes of shock after trauma. Traumatic shock, due to this fact, appears to outcome primarily from hypovolemia, though there may also be a reasonable degree of concomitant neurogenic shock caused by lack of vasomotor tone, as mentioned next. Distention of the gut in intestinal obstruction partly blocks venous blood move in the intestinal walls, which will increase intestinal capillary pressure, causing fluid to leak from the capillaries into the intestinal walls and intestinal lumen. Severe burns or other denuding situations of the pores and skin cause lack of plasma through the denuded skin areas so that the plasma volume turns into markedly reduced. Instead, the vascular capacity increases so much that even the conventional quantity of blood is incapable of filling the circulatory system adequately. One of the most important causes of this situation is sudden lack of vasomotor tone throughout the physique, resulting particularly in massive dilation of the veins. The position of vascular capacity in serving to regulate circulatory function was mentioned in Chapter 15, the place it was famous that a rise in vascular capacity or a decrease in blood quantity reduces the mean systemic filling pressure, which reduces venous return to the heart. Diminished venous return brought on by vascular dilation is known as venous pooling of blood. Some neurogenic components that can cause loss of vasomotor tone embody the next: 1. Deep general anesthesia usually depresses the vasomotor middle sufficient to cause vasomotor paralysis, with resulting neurogenic shock. Spinal anesthesia, particularly when this extends all the best way up the spinal cord, blocks the sympathetic nervous outflow from the nervous system and is often a potent explanation for neurogenic shock. Also, despite the very fact that mind ischemia for a few minutes almost always causes excessive vasomotor stimulation and increased blood strain, extended ischemia (lasting >5�10 minutes) could cause the opposite effect-total inactivation of the vasomotor neurons in the mind stem, with a consequent lower in arterial stress and growth of extreme neurogenic shock. Septic shock is extremely necessary to the clinician as a end result of, other than cardiogenic shock, septic shock is presently probably the most frequent explanation for shock-related dying within the hospital. Peritonitis caused by spread of an infection from the uterus and fallopian tubes, generally ensuing from an instrumental abortion carried out under unsterile situations 2. Peritonitis ensuing from rupture of the gastrointestinal system, typically caused by intestinal illness or by wounds three. Generalized bodily an infection ensuing from spread of a pores and skin an infection corresponding to streptococcal or staphylococcal an infection 4. Generalized gangrenous infection resulting particularly from gasoline gangrene bacilli, spreading first via peripheral tissues and eventually via the blood to the internal organs, especially the liver 5. Infection spreading into the blood from the kidney or urinary tract, usually caused by colon bacilli. It results primarily from an antigen-antibody response that rapidly occurs after an antigen to which the person is sensitive enters the circulation.
Vytorin 30 mg proven
Instead cholesterol levels change daily purchase vytorin 20 mg without a prescription, the base of the ventricles would repolarize forward of the apex cholesterol definition anatomy cheap 20 mg vytorin, and the vector of repolarization would level from the apex towards the bottom of the heart, opposite to the standard vector of repolarization. Consequently, the T wave in all three standard leads could be negative rather than the usual positive. Chapter 22, digitalis is a drug that can be used throughout coronary heart failure to increase the energy of cardiac muscle contraction. However, when an overdose of digitalis is given, depolarization duration in one a part of the ventricles may be increased out of proportion to that of other parts. As a end result, nonspecific adjustments, such as T-wave inversion or biphasic T waves, could occur in one or more of the electrocardiographic leads. Therefore, changes in the T wave during digitalis administration are often the earliest signs of digitalis toxicity. The objective of this chapter is to discuss the physiology of widespread cardiac arrhythmias and their effects on heart pumping, as nicely as their diagnosis by electrocardiography. For example, when a patient sustains severe blood loss, sympathetic reflex stimulation of the heart might improve the heartrateto150to180beats/min. Some causes of tachycardia embrace increased physique temperature, dehydration, blood loss anemia, stimulation of the center by the sympathetic nerves, and poisonous conditions of the guts. The coronary heart fee normally will increase about 10 beats/min for every degree Fahrenheit improve in body temperature (with an increase of 18 beats/min for each degree Celsius), up to abodytemperatureofabout105�F(40. Beyondthis, the heart price might decrease due to progressive debility of the heart muscle on account of the fever. Fever causes tachycardia because an elevated temperature increases the rate of metabolism of the sinus node, which in flip directly will increase its excitability and price of rhythm. Any circula- tory reflex that stimulates the vagus nerves causes launch of acetylcholine on the vagal endings within the heart, resulting inaparasympatheticeffect. Perhapsthemoststrikingexample of this phenomenon occurs in patients with carotid sinus syndrome. In these sufferers, the pressure receptors (baroreceptors) in the carotid sinus area of the carotid artery walls are excessively delicate. Sometimes this reflex is so highly effective that it truly stops the center for 5 to 10 seconds, resulting in lack of consciousness (syncope). Ischemia of the A-V node or A-V bundle fibers usually delays or blocks conduction from the atria to the ventricles. Coronary insufficiency could cause ischemiaoftheA- nodeandbundleinthesameway V that it may possibly trigger ischemia of the myocardium. Inflammation of the A-V node or A-V bundle can depress conduction from the atria to the ventricles. Inflammation results incessantly from several varieties of myocarditis which would possibly be triggered, for instance, by diphtheria or rheumatic fever. Extreme stimulation of the heart by the vagus nerves in rare circumstances blocks impulse conduction through the A- node. Such vagal excitation often V outcomes from sturdy stimulation of the baroreceptors in people with carotid sinus syndrome, discussed earlier in relationship to bradycardia. Degeneration of the A-V conduction system, which is sometimes seen in older sufferers. Medications corresponding to digitalis or beta-adrenergic antagonistscan,insomecases,impairA- conduction. To the left is the document when the topic was respiration normally; to the right, when the subject was respiration deeply. Note from this document that the center fee increased and decreased not more than 5% throughout quiet respiration (shown on the left half of the record). Then, during deep respiration, the guts rate increased and decreased with every respiratory cycle by as much as 30%. Sinus arrhythmia may result from any one of many circulatory circumstances that alter the strengths of the sympathetic and parasympathetic nerve alerts to the heart sinus node. The respiratory sort of sinus arrhythmia results mainly from the spillover of indicators from the medullary respiratory middle into the adjoining vasomotor heart throughout inspiratory and expiratory cycles of respiration. The spillover signals trigger alternate will increase and reduces in the number of impulses transmitted through the sympathetic and vagus nerves to the guts. This so-called P-R interval often decreases in length with a sooner heartbeat and will increase with a slower heartbeat. Type I second-degree atrioventricular block showing progressive P-R prolongation prior to the dropped beat. One means for determining the severity of some heart ailments, such as acute rheumatic coronary heart disease, for example, is to measure the P-R interval. Note prolongation of the P-R interval preceding the dropped beat, adopted by a shortened P-R interval after the dropped beat. In some situation inflicting poor conduction in the A- node or V A- bundle turns into severe, complete block of the imV pulse from the atria into the ventricles occurs. In this case, the ventricles spontaneously set up their very own sign, usually originating within the A- node or A- bundle disV V taltotheblock. Thedurationofblockmaybe afewseconds,afewminutes,afewhours,orevenweeks or longer before conduction returns. This condition happens in hearts with borderline ischemia of the conductive system. Overdrive suppression implies that ventricular excitability is at first suppressed as a result of the ventricles have been pushed by the atria at a fee greater than their pure price of rhythm. Consequently, most of those sufferers are supplied with a man-made pacemaker, a small battery-operated electrical stimulator planted beneath the skin, with electrodes usually connected to the right ventricle. Also, V the interval between the premature contraction and the following succeeding contraction is barely prolonged, which is called a compensatory pause. One of the reasons for this compensatory pause is that the untimely contraction originated in the atrium far from the sinus node, and the impulse needed to journey through a substantial quantity of atrial muscle before it discharged the sinus node. Consequently, the sinus node discharged late in the untimely cycle, which made the succeeding sinus node discharge also late in showing. Mild toxic circumstances resulting from such factors as smoking, lack of sleep, ingestion of an extreme quantity of espresso, alcoholism, and use of various medication can also provoke such contractions. Possible causes of ectopic foci are as follows: (1) local areas of ischemia; (2) small calcified plaques at different factors within the heart, which press against the adjacent cardiac muscle in order that a few of the fibers are irritated; and (3) poisonous irritation of the A- node, Purkinje system, or myocardium brought on by V infection, medication, nicotine, or caffeine. The mechanical initiation of premature contractions can be frequent throughout cardiac catheterization; giant numbers of premature contractions typically happen when the catheter enters the ventricle and presses in opposition to the endocardium. Thus, a deficit in the variety of radial pulses happens compared with the actual variety of contractions of the guts. Ingeneral,A- nodalpremaV ture contractions have the same significance and causes as atrial untimely contractions. The reason for this prolongation is that the impulse is carried out mainly by way of slowly conducting muscle of the ventricles quite than via the Purkinjesystem. When the conventional impulse passes through the center, it passes through each ventricles almost simultaneously.