
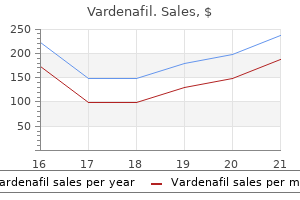
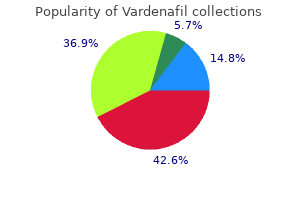
Vardenafil dosages: 20 mg, 10 mg
Vardenafil packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Proven vardenafil 10 mg
This easy guideline recommends oral analgesics which could be prescribed as per the severity of ache (mild erectile dysfunction yeast infection purchase vardenafil 10 mg with visa, average erectile dysfunction psychological causes purchase vardenafil 20 mg with amex, severe) from the first step to three. Analgesic potency gets escalated from nonopioid to weak-to-strong opioid like oral morphine. Opioid is combined with adjuvant analgesics which are used to improve pain reduction and cut back the side effects. Pharmacological Management of Cancer Pain the administration of cancer ache involves analgesic remedy along with anesthetic, neurosurgical, rehabilitative, psychologic and psychiatric methods. When opioid analgesics are prescribed, a daily bowel regimen together with cathartics and stool softeners must be started. Adjuvant Drugs these are generally used to: (1) Provide analgesia for sure kinds of pain, viz. The adjuvant analgesics may be divided into: (1) Antidepressants; (2) Anticonvulsants; (3) Neuroleptics; (4) Corticosteroids; (5) Oral muscle relaxants, antihistaminic and sympatholytic medicine. The most commonly used drugs are: phenytoin, carbamazepine, sodium valproate, clonazepam, gabapentin and pregabalin. It is used in patients with superior disease resulting in transient improvement in appetite, analgesia, and mood. Patients with refractory neuropathic ache, bone ache and headache due to raised intracranial rigidity benefit. In cancer pain syndromes such as epidural spinal cord compression, 85% of the sufferers receiving one hundred mg of dexamethasone reported important ache relief associated with marked reduction in analgesic requirement. A loading dose of sixteen mg and upkeep with 4 mg/day of dexamethasone is often effective in advanced cancer sufferers with ache. Use of ketamine infusion has been found to be effective in certain circumstances of refractory neuropathic ache. Metastatic illness to bone is the commonest reason for pain in sufferers with advanced cancers of breast, lung and prostate. The present bisphosphonates used for the therapy of bone ache include pamidronate, clodronate, and zoledronic acid. Opioid Analgesics Opioid analgesics are the mainstay in the administration of most cancers ache. Effective use of opioids requires the balancing of the most fascinating results of pain reduction to the undesirable results of nausea, vomiting, mental clouding, constipation, tolerance, and bodily dependence. These undesirable effects impose a practical limit on the dose useful for a specific affected person. The number of an opioid analgesic relies on the necessity to treat the severity of ache from moderate to severe ache. The morphine-like opioid drugs symbolize one end of the spectrum, which includes all other opioids (Box 2). Morphine: Although the oral bioavailability varies from 35% to 75%, its plasma half-life is considerably shorter than its period of analgesia, which limits its accumulation. There are a quantity of elements which result in clinical opioid dose escalation: disease progression, psychological causes (anxiety, depression), pharmacokinetic causes (poor absorption, drug interaction), opioid refractory ache. Anticipation and therapy of unwanted effects: the unwanted effects of the opioid analgesics typically restrict their efficient use. The commonest unwanted effects are: sedation, respiratory depression, nausea, vomiting, constipation, multifocal myoclonus and seizures. Sedation and drowsiness differ with the drug, dose and should happen after each single and repeated administration. Switching to different Box 2: Principles of opioid use � Chooseawell-toleratedopioid. Anesthetic and neurosurgical approaches are most effective in treating patients with welldefined, localized ache. However, most cancers sufferers typically have a blended somatic, visceral and neuropathic ache syndrome, the choice for these procedures become difficult at later stage of the disease. About 10% patients can benefit substantially from these procedures to cut back the unwanted side effects of analgesics. A momentary diagnostic block using a neighborhood anesthetic ought to always precede a neurolytic block. Palliative care is remedy to relieve, somewhat than cure, signs brought on by most cancers. Palliative care might help people stay extra comfortably and is an pressing humanitarian need for individuals worldwide with cancer and different persistent fatal illnesses. Being faced with a life-threatening or superior disease is a crisis that impacts affected person and family alike. When lively therapy ought to stop, and palliative care measures continued, ought to be a joint determination between oncologist, palliative care doctor, affected person and family. The frequent signs that patients current with are fatigue, pain, lack of energy, weak spot and urge for food loss. Other problems include bleeding from a surface wound, dyspnea, cachexia, nausea, vomiting, constipation or diarrhea and delirium. Effective administration of a palliative care group entails good management skills with inspirational and motivational leaders, constructions for supervision, monitoring and support, and appropriate referrals to mental health professionals for workers when required. Psychosocial care is, due to this fact, an essential side in helping patients with bone and soft-tissue tumors with superior illness and their caregivers, emphasizing the World Health Organization idea of high quality of life of adding life to years and never simply years to life. Care for patients and households suffering from religious distress is considered one of the difficult, but crucial areas of care. Paradoxically, the journey into dying is sometimes considered to be the final word automobile for spiritual discovery. Adhering to such a systematic approach, helps not solely in higher symptom management however will increase compliance and holistic care. Hospital vs Home Care vs Hospice Care this ought to be the selection of affected person and household. Family members typically feel inadequate and are one of the major causes for preferring hospital care. Arrangement with native family physicians is the choice to community nurses of the developed nations. Home take care of sufferers with advanced most cancers has been proven to be price efficient; but can only be effective if "Home Care" groups can provide efficient holistic care. Hospice care in a country like India is an possibility, not often exercised, as family units are sturdy and provide sufficient care with the help of the professionals. Patients prefer to be surrounded by their household and caregivers must be at house to take care of the the rest of the household. Quality of life is paramount; but varies with every particular person and thus should be based mostly on joint selections between affected person, physician and family. International guidelines show lack of good thing about such interventions when demise is estimated in weeks. Physicians should seek steerage and collaboration from colleagues, larger authorities and even the courtroom, the place decision-making is in conflict. All remedy selections ought to be shared decision-making between patient, family and professionals. Persons with superior most cancers can experience a spread of emotions together with sadness, anxiety, disbelief and denial on being informed of their prognosis.
Vardenafil 20 mg discount on-line
Radiographs can reveal sacral destruction but the presence of overlying bowel shadows can easily impede the prognosis erectile dysfunction pills from india vardenafil 10 mg purchase with mastercard. Surgical extensive excision of the tumor with a cuff of regular tissue is the one curative procedure for the reason that tumor is resistant to erectile dysfunction condom vardenafil 10 mg without a prescription radiotherapy and chemotherapy. Adequate tumor resection must be the objective and may have priority over saving neural components. If all sacral nerve roots can be preserved no much less than on one aspect, the patient can have normal bowel, bladder and sexual perform. If nerve root resection is required bilaterally, preservation of the S2 roots may preserve partial urinary and fecal continence in some patients. Preservation of a minimal of one S3 nerve root is required for preservation of bowel and bladder function in most patients. The kind of surgical approach and the need for fixation of bone is decided by the extent of sacral involvement. Tumors that contain solely the distal portion of the sacrum (S3 and below) can be handled with a single procedure from a posterior surgical approach. Tumors that involve the S1 and S2 segments or those who involve the whole sacrum require a mixed anterior and posterior resection. Sacropelvic reconstruction after intensive resection may require a number of levels to complete, and morbidity is sort of vital. Therefore, a diverting colostomy and ureterostomy should be performed and obviously, success of this complex surgical process requires the assist of a multidisciplinary group. Radiographically, chondrosarcoma shows massive areas of bone destruction and an related delicate tissue mass with flocculent calcifications inside it. Complete surgical excision supplies the only hope of tumor cure and remains as a challenge in vertebral lesions. En-bloc excision with removal of the overlying soft-tissue capsule, muscle, pleura or peritoneum, with a cuff of normal bone is crucial for a disease-free survival. Stabilization of collapsed vertebrae by way of either kyphoplasty or vertebroplasty provides quick ache reduction for sufferers. SpinalMetastasis the spinal column is the most common web site of skeletal metastases. At least 5�10% of all most cancers patients develop spine metastases during the course of their disease. Within the spinal column, the vertebral our bodies are affected the most (85%) however metastatic deposits can even happen within the paravertebral area (10%), the epidural space (<5%) and the intradural house (<1%). The most frequent places of the first tumors, in descending order, are the breast (21%), lung (14%), prostate (8%), renal (5%), gastrointestinal (5%) and thyroid (3%). Among girls, breast most cancers metastases account for nearly 50�55% of all spine metastases. Even though in most patients, metastatic collapse or twine compression of a single vertebral lesion is the most typical symptomatic lesion, metastases are current in multiple noncontiguous spine websites in as a lot as 40% of sufferers. The commonest location is the thoracic vertebra adopted by the lumbar and cervical vertebrae. The vertebral body is affected preferentially due to its trabecular nature and the wealthy vascular supply of the cancellous bone. The posterior one-half of the vertebral body typically is concerned first, adopted by the anterior one-half and the pedicles as cortical bone destruction advances. The tumor cells from the primary web site attain the vertebra by direct extension, by way of lymphatic channels, or through hematogenous routes. Batson proposed that carcinomatous cells from the pelvic and gastrointestinal tumors seed the vertebrae through the paravertebral Myeloma and Plasmacytoma Multiple myeloma and solitary plasmacytoma belong to plasma cell dyscrasias (B-cell lymphoproliferative diseases). The distinction between solitary plasmacytoma and a number of myeloma is essential as a end result of the prognosis of these differ significantly. True solitary plasmacytoma refers to localized plasma cell proliferation without any systemic abnormality in the bone marrow or peripheral blood. Solitary plasmacytoma could allow prolonged survival if local management could be obtained, although 40�50% of them develop a number of myeloma in due course. Multiple myeloma accounts for 1% of newly recognized malignancies and is fatal in most patients when spinal disease is identified. Anemia, elevated renal parameters, hypercalcemia and raised sedimentation price also are attribute on laboratory research. This plexus is a network of longitudinal, valveless veins operating parallel to the vertebral column that type innumerable anastomoses to the sinusoids of the vertebral marrow and the epidural venous channels. An increase in the intra-abdominal or intrathoracic strain throughout coughing and sneezing diverts venous move from the pelvic or azygous venous system into the epidural area and subsequently into the vertebral trabecular system. Once a tumor has metastasized to a vertebra, it may domestically spread to adjoining vertebrae alongside the anterior or posterior longitudinal ligaments or via the epidural veins. Metastasis normally indicates systemic spread of a complicated stage most cancers and therefore was not handled aggressively within the earlier days. However, with improved detection methods and management principles, appropriate surgical intervention/radiotherapy now provides excellent palliation and even the hope of treatment in some chosen sufferers. Clinical Features Patients with metastatic backbone lesions typically present with axial again ache. The ache accompanying spine tumors is characterised as a uninteresting, constant ache that often awakens the affected person from sleep. Patients with thoracic lesions may experience bilateral radicular ache along the intercostal nerves in a corset-like distribution. A third kind of ache in spinal metastasis is the instability back pain that develops when the affected vertebra fractures pathologically. The patient who initially has the classical rest pain develops a sudden improve in ache depth and finds it tough to change position (like getting up from mendacity down posture). The second necessary medical function is the development of signs of neurological deterioration. This contains myelopathic options of gait instability, clumsiness, weakness within the legs, numbness and paresthesia, urinary retention, constipation, and so on. Objective signs, corresponding to a palpable mass or spinal deformity, are rare and happen late within the development of illness. Although lower than 1% of backbone tumor sufferers expertise acute cord compression, as many as 5% of most cancers sufferers develop gradual symptomatic epidural metastases, characterized by localized paresthesia and muscle weak spot. Patients with superior tumor unfold may also have constitutional signs like lack of weight and urge for food, lethargy, malaise, generalized weak point, and so forth. Dynamic flexion and extension views can provide necessary clues regarding spinal stability. One of the first clues to vertebral metastasis is the unilateral destruction of the pedicle seen on the anteroposterior radiograph (the "winking owl" sign). This is often brought on by tumor invading from the posterior part of the vertebral physique into one of many pedicles. The flipside of using radiographs for learning spinal metastasis is that destruction of 30�50% of the trabecular bone by the tumor is crucial earlier than a lesion is detectable by plain radiographs. In up to 60% of spine sufferers with neoplastic twine compression, plain radiographs are regular. Further distinguishing neoplastic lesions from benign vertebral collapse because of osteoporosis is difficult.
Diseases
- Charcot Marie Tooth disease deafness dominant type
- Hypokalemic periodic paralysis type 1
- Infant respiratory distress syndrome
- Dyserythropoietic anemia, congenital
- Trisomy 14 mosaicism
- Cerebellar hypoplasia tapetoretinal degeneration
10 mg vardenafil purchase free shipping
The malunion to the left of center has the identical degree of angulation combined with translation towards the convexity of the deformity erectile dysfunction zenerx 20 mg vardenafil for sale. The malunion to the proper of middle has the identical degree of angulation combined with translation in the direction of the concavity of the deformity erectile dysfunction commercials order vardenafil 20 mg online. The former is called compensatory translation, whereas the latter is called aggravating translation. Notice the purpose of intersection of the mechanical axis lines of the proximal and distal tibia. Notice that in the femur translation towards the convexity is aggravating while translation in the path of the concavity is compensatory. The cause for that is that by convention we discuss with translation because the distal fragment relative to the proximal. Notice that the interpretation deformity shifts the true apex of the deformity both proximal or distal to the apparent apex on the stage of the malunion Osteotomy Consideration the axis of angulation is a line perpendicular to the aircraft of the angular deformity. The specific axis of angulation of a frontal airplane angular deformity passes by way of some extent on the bisector line of that angular deformity. An axis of angulation passing by way of the convex cortex on the bisector line leads to an open wedge kind of correction, whereas an axis passing through the concave cortex on the bisector line results in a closing wedge kind of correction. An axis passing in between the convex and concave cortices on the bisector line produces a partial open or partial closing wedge (neutral wedge) kind of correction. To realign the bone absolutely at a particular degree of angulation, the magnitude of angular correction must be equal to the magnitude of the angular deformity. Notice the simultaneous correction of the angulation and translation, as demonstrated by the colinearity of the medial tibial diaphysis. Preoperative planning demonstrates that the true apex of the deformity is proximal to the level of the malunion. Multiapical deformities permit extra versatility within the alternative of level and magnitude of correction. Although the proximal and distal bone axes are mounted, the middle axis could be manipulated to alter the levels and magnitudes of the angulation. This produces a zigzag within the anatomic axis of the bone and therefore leaves a small bump on the bone. This might present a cosmetic problem if the bump is on the subcutaneous surface of the bone. Clinical Choice of Osteotomy Level the selection of osteotomy level is based on the geometry of the deformity, the sort of fixation, the proximity of the osteotomy to the physis or joint, soft-tissue converge, bone high quality, and so on. If lengthening is required along with correction of angular deformity, corticotomy is completed in the metaphysis area. This is adopted by translation correction to realign the mechanical axis for both angulation and translation or to perform two osteotomies, one for lengthening and one for deformity correction. Between these two planes, any deformity lies in an indirect airplane somewhere within the frontal and sagittal airplane. The trigonometric actual formulae and graphic approximate formulae to calculate the magnitude (obl) and orientation of the oblique airplane to the frontal aircraft (pln) are as follows: Trigonometric: obl = tan�1 pln = tan�1 tan lat tan ap (Phythagorean Theorem) lat graphic: obl = plan = tan�1 ap size deformities. A second aircraft of angulation can exist provided that a second angular deformity at another degree is launched into these bone segments or strains. There are a number of ways to decide the magnitude and true aircraft of a deformity in a airplane indirect to the frontal aircraft. The aircraft 90� to this projection ought to show the maximum angulation profile of the deformity. The varied strategies by which osteotomies can be performed are: � Low power technique using solely osteotome � Multiple drill holes and osteotome � Gigli saw method these methods may be utilized to both external fixators and minimally invasive inside fixator. Method of Osteotomy After having determined the extent of the osteotomy one should carry out the osteotomy with minimal damage to the encircling delicate tissue and blood supply of the bone preserving in mind the varied neurovascular buildings. When performing the osteotomy, the dissection of the periosteum ought to be minimal to forestall harm to the construction. The Gigli Saw is tied to the suture material and pulled from posterior to anterior. The posterior and lateral cortices, and the medullary canal are cut with the saw underneath the protection of two elevators. The medial cortex is then elevated and the medial cortex is reduce by flattening out the path of pull of the noticed. This technique could be applied to the proximal tibia, distal tibia, supramalleolar region, proximal femur and distal femur. It has a well-defined function for the therapy of advanced Nonunions with an infection and bone loss. The fixator is in a position to control the position of the bone fragments with the help of software. It is based on the science of projective geometry and is the offshoot of the Chasles Theorem. The primary fixation to the bone is achieved with normal Ilizarov wires or half pins. These are then hooked up to the rings with wire fixation bolts and cubes with sleeves, and so on. Software the control over bony fragments for deformity correction, lengthening or fracture reduction is finished with the help of software. Special measurements which allow the software program to get oriented to the bone fragment position vis-�-vis the size and orientation of the rings, are taken with the help of a translucent grid on X-rays and fed into the software program. The ring and strut sizes are additionally fed in as are the specified correction parameters. A observe is taken of any construction in danger just like the peroneal nerve in the region of neck of fibula, so as not to stretch it. The software program then outputs a program, which guides the surgeon and affected person to turn the struts at particular intervals and quantities to achieve the specified result. Patients could comply with directions very simply because the struts are shade coded with tags. They have six tabs which project from the outer border, every having three holes for struts. They are partially radiolucent but could obscure the view of the fracture or regenerate web site. For the thighs, arcs comprising five-eighths of a circle of the similar design are available in various sizes and may be used within the Measurements and the Software All patients will need to have full length or full section X-rays earlier than and during therapy. The X-ray measurements wanted to fill in the software are as follows: Deformity Parameters: Deformity parameters are Coronal plane angulation (varus-valgus) and translation, sagittal aircraft angulation (recurvatum-procurvatum) and translation, axial view angulation (external or inside rotation) and translation (shortening and lengthening). Mounting Parameters: these are a set of measurements which assist the software program to orientate the bone fragments in 3D house.
Vardenafil 20 mg buy with visa
Indirect discount has an enormous benefit because they do minimal damage to tissues already traumatized by fracture and protect the fracture hematoma impotence young males vardenafil 10 mg buy low cost. All the devices and implants used for oblique discount are utilized away from the fracture zone impotence urinary generic vardenafil 20 mg mastercard. Fracture planning is first and an important step in the operative administration of any fracture. Type of implant, measurements of implants and its availability-all should be checked. Patient: A day before surgery the affected person ought to be carefully examined for any infection at the operative website, pustules dermatitis should be noted. General and systemic examination for fitness of the patient for surgical procedure should be carried out. Flexibility In splinting system of fracture fixation, elastic flexible fixation can only be achieved without interfragmentary compression. Flexibility is dependent upon the following elements: � Size of the metallic: the thinner the metallic, the more the flexibleness. The essential positions are screws immediately next to the fracture zone on either side and the screws at each ends of the plate. Three steps leading to the ultimate preoperative plan: Outlines of plates and screws have been drawn onto the decreased fracture using suitable templates. The product of the reconstructive section is a tracing of an intact bone with the decreased fracture fragments marked out on it. Primary bone therapeutic with out formation of callus was the goal, which was achievable when fractures had been lowered anatomically and fixation was rigid. This requires in depth subperiosteal exposure of the bone for reduction of fracture. The inflexible fixation of all bony fragments then was achieved through the use of clamp, forceps and lag screws positioned in mechanically optimal direction. Due to above causes, ideas were then shifted to biological fixation by oblique reduction. Reduction of the diaphyseal fracture is to convey the proximal and distal fragment into right relationship to each other. It is absolutely necessary in the intraarticular fractures to restore the articular floor. However, in the diaphyseal and metaphyseal fractures restoration of the alignment, mechanical axis, length and rotation are extra necessary than anatomic reduction. Healing of fractures is dependent upon (1) Mechanical standing at the fracture site and (2) Biological components of healing. X-ray of the whole bone together with proximal and distal joints is taken and fracture fragments are traced on a hint paper. Displacements of the fragment alongside three axes of the bone (sagittal, coronal and horizontal x, y and z axes) are traced on a hint paper. X-ray of the contralateral normal bone is taken and reversed 180� and used as a template. The fracture geometry is carefully studied and reconstructed in case with fracture of femur; draw the anatomical axis from piriformis fossa to 1 cm medial to heart of knee. How to Plan Reconstruction: Method this entails figuring out and reassembling the fracture fragments, very similar to doing a jigsaw puzzle: Step 1-tracing the intact bone: Place a piece of tracing paper over the normal X-ray and trace the outline of the intact bone (this is best done over a light box). Tracing of the outline of the fracture fragments: All overlapping fragments have been separated. Step 2-tracing the fracture: Put a separate piece of tracing paper over the fracture X-ray and hint across the fracture fragments. Restoration: the intact tracing is positioned over the fracture tracing and the fractures drawn onto the intact bone. Step 3-restoration: Place the tracing of the intact bone over the tracing of the fractured bone. By shifting the outlines of the intact Reduction Techniques Satisfactory discount increases the soundness. The method of discount should be as mild as potential to forestall additional damage to the delicate tissues and the vascularity on the fracture web site. Open oblique discount Direct discount: the fracture strains are uncovered surgically, and the bone fragments are reduced beneath direct vision and with devices instantly applied to every fragment, normally near the fracture web site. Direct reduction is of two sorts: (a) Open discount: by exposing the fracture website and manually lowering underneath direct vision. Traction applied to the entire limb via a fracture desk produces indirect reduction. However, oblique reduction achieved by massive distractor (femoral distractor) or by an implant is more effective and discount may be fine-tuned. In the diaphysis and metaphysis, right alignment of the two primary fragments carrying the joint surfaces is necessary. Closed indirect reduction: Biological fracture fixation is used often after some form of discount. Biological fixation methods are like locked nails, locked internal fixators and external fixators. Open oblique discount: Open indirect reduction entails an open method, however with indirect discount maneuvers and a "notouch" method. All open oblique discount requires exposure to apply the reduction gadgets, but not to visualize the fracture. Example of open indirect reduction is elevation of a depressed fragment of tibial plateau fracture using intramedullary nail in a single fragment. Indications for Direct Reduction � Intra-articular fractures � Simple transverse/metaphyseal or diaphyseal fractures � Forearm fractures the intra-articular fractures must be reduced exactly and anatomical. While doing open reductions soft tissue injury should be as minimum as possible with meticulous gentle tissue handling and with restricted epiperiosteal exposure of the bone. Open reduction requires use of compression of the fragments leading to absolute stability. In the direct reduction, the fracture website is opened surgically and the fragments are reduced by instrumentation and internally fixed. The most essential and demanding part of operative fracture remedy is alignment of the fracture fragment. The discount must be mild and atraumatic in order to preserve the blood supply on the fracture site, to the fragments and delicate tissue. This shown to improve fracture-healing time, reduce nonunion charges and cut back an infection. Indirect discount: Indirect discount implies that the forces and moments acting away from the fracture are used to manipulate and eventually scale back the fracture, by a limited open exposure. Reduction is carried out with devices or implants that are launched away from the fracture zone. Ganz and Mast have developed and popularized the technique of oblique discount with out opening the fracture web site. The aim of oblique reduction is to achieve alignment and proper rotation and shortening. Mechanical axis of each proximal and distal fragment, in all horizontal, coronal and sagittal planes, must be collinear.
Discount 10 mg vardenafil overnight delivery
Spinal cord compression could also be handled with radiotherapy (soft tissue compression/partial loss of power) or surgical decompression (bony compression/complete early motor loss) effective erectile dysfunction treatment 10 mg vardenafil cheap with visa. Appendicular skeletal lesions are handled with intramedullary fixation and adjuvant radiotherapy erectile dysfunction medication canada cheap vardenafil 20 mg line. A solitary focus, within the appendicular skeleton with out evidence of disseminated illness could additionally be handled with surgical excision and radiotherapy. Differential Diagnosis � � � � Skeletal metastasis form one other primary tumor Malignant lymphoma Monoclonal gammopathies of uncertain origin Waldenstrom hypergammaglobulinemia. The interval from onset of symptoms to termination varies from a few months to several years. In the overwhelming majority of cases, demise occurs within three years and in almost all inside 5 years. Combination chemotherapy versus melphalan and prednisone as remedy for a quantity of myeloma: an outline of 6,633 patients from 27 randomized trials. The extremities are the most typical web site with about 60% of soft-tissue sarcomas arising in the extremities. The different common sites of involvement are trunk (15�20%), head and neck region (10%), internal organs and the retroperitoneum (15%). Approximately, half of all sufferers with intermediate or highgrade soft-tissue sarcomas develop metastatic illness and the overall survival is roughly 50% at 5 years. Though in most patients, no specific etiology can be identified, the danger elements for soft-tissue sarcomas embody earlier radiation remedy, publicity to chemical substances. While sarcomas within the extremities could present earlier, analysis of sarcomas involving the pelvic cavity could also be delayed. Their location deep throughout the body precludes palpation of the tumor mass early in the middle of the illness. Consequently, these tumors usually reach tremendous dimension previous to diagnosis without causing overt symptoms. Any soft-tissue lump exhibiting any of the following clinical features ought to be thought-about to be malignant until proved in any other case: (i) growing in dimension, (ii) measurement greater than 5 cm, (iii) deep to the deep fascia, and (iv) painful. The more of these clinical options present, the larger the risk of malignancy with rising size being one of the best particular person indicator. An essential dictum may be that "any tumor discovered deep to the deep fascia or larger than 5 cm ought to be thought to be a soft-tissue sarcoma until confirmed otherwise. Often they are going to be normal and noncontributory, however, they may reveal a focal skeletal abnormality presenting as a soft-tissue mass. They are necessary in assessing the presence of soft-tissue calcification, which may be characteristic in lesions such as the phleboliths seen in hemangioma permitting a selected analysis to be made. Fine punctate calcification may alert the clinician to the chance of synovial sarcoma. The presence of the typical marginal calcification seen in myositis ossificans shall be extra easily appreciated on plain movies in contrast with magnetic resonance. It helps to determine whether or not the tumor has breached regular anatomical boundaries and in addition illustrates its relation with the adjacent neurovascular structures. The availability of titanium implants and improved picture suppression software may help to cut back however not totally remove this drawback. Here too, core needle biopsies, which are often achieved as an outpatient process beneath native anesthesia are preferred. Additional research, together with electron microscopy, histochemistry, flow cytometry, cytogenetics and tissue culture studies could allow identification of specific subtypes throughout the major histologic categories. Others are leiomyosarcoma (12%), liposarcoma (15%), synovial sarcoma (10%) and malignant peripheral nerve sheath tumors (6%). Pathologists assign grade based on variety of mitoses per high-powered field, presence of necrosis, mobile and nuclear morphology and the degree of cellularity. The metastatic potential of soppy tissue tumors is healthier mirrored by their histologic grade somewhat than the cellular classification. Factors related to a poorer prognosis include age older than 60 years, tumors larger than 5 cm or high-grade histology. Based on this idea and the connection of the dissection plane to the tumor and its pseudocapsule, Enneking has described 4 types of surgical excisions, which have been elaborated on within the earlier chapter "Principles of Management of Bone Tumors". Role of Radiotherapy Radiotherapy complements adequate surgery as commonplace remedy of intermediate and high grade, deep tumors with a diameter of greater than 5 cm. It can include preoperative or postoperative radiation relying on institution protocols. Preoperative radiotherapy can occasionally permit limb conservation of extremity sarcomas which in any other case would be inoperable or require amputation. Reports counsel that preoperative radiotherapy might cut back late toxicity but is associated with a greater threat of wound problems than postoperative radiotherapy. Intraoperative brachytherapy either exclusively or together with postoperative radiation is an option that can be typically employed. In brachytherapy, hollow catheters placed in the tumor bed intraoperatively are subsequently loaded with Iridium 192 wires to ship radiation within the desired space. Radical brachytherapy alone, when used judiciously has demonstrated good local management and useful outcomes with lowered treatment-related morbidity. Principles of Treatment Surgical Management When feasible, function-sparing surgical excision with wide margins is the cornerstone of effective remedy, with the aim of preservation of a practical extremity. This may be facilitated by delicate tissue reconstructive surgery together with using native or free flaps and occasionally vascular and nerve resection with suitable graft reconstruction. Sarcomas respect anatomical borders and native anatomy influences tumor growth by setting natural boundaries to unfold. Anatomic compartments have natural limitations to occult tumor extension like the most important fascial septa and the tendinous origins and insertions of muscle tissue. Sarcomas grow along the path of least resistance and initially extend throughout the compartment they come up from. In a later stage with advancing illness, they violate their compartmental obstacles and turn into extracompartmental. Unlike benign tumors, which are enclosed by a true capsule composed of compressed regular cells, sarcomas are generally surrounded by a pseudocapsule or reactive zone. High-grade sarcomas have a poorly outlined reactive zone that might be domestically infiltrated by tumor resulting in satellite tv for pc lesions Role of Chemotherapy the position of chemotherapy in soft-tissue sarcomas remains to be debatable. The histological type could play a role within the choice making to supply chemotherapy, since some varieties are felt to be extra chemosensitive, whereas others are much less so. Patients with highgrade tumors bigger than 5 cm in diameter have the best tendency for disease to metastasize and are probably candidates for potential medical trials of adjuvant chemotherapy. The chemotherapeutic brokers used embody doxorubicin alone or a mixture of doxorubicin plus ifosfamide. Management of Metastatic Disease Soft-tissue sarcomas have a predilection for creating pulmonary metastases at some point of their natural history.
Vardenafil 20 mg generic without a prescription
Primary bone tumors erectile dysfunction workup aafp vardenafil 10 mg overnight delivery, whether or not benign or malignant erectile dysfunction doctors purchase vardenafil 10 mg visa, could originate in cartilage cells, osteoblastic (osteoid or bone-forming) cells, fibroblastic cells, primitive mesenchymal cells, and hematopoietic cells, in addition to nerve and vascular tissue, notochordal remnants, and other rare sites. A simplified classification system for the frequent bone tumors is given in Table 1. A affected person with a bone tumor initially complains of ache with an alteration in his practical capability irrespective of the presence or absence of a palpable mass. Though histopathological analysis is important in establishing a prognosis within the majority of these tumors, a biopsy should solely be the final step in a systematic strategy to 614 TexTbook of orThopedics and Trauma An orthopedic surgeon have to be constantly aware of the truth that different conditions could often simulate bone tumors. Trauma, metabolic bone disease and infection, especially tuberculosis could often mimic tumors and be a pitfall for the unsuspecting clinician. The purpose of the diagnostic work up is to help in staging the illness, both for native extent and distant spread in order to acquire information relating to the aggressiveness of the lesion and help in formulating a management strategy. The lung is the commonest site for metastasis in bone and soft tissue sarcomas and metastatic unfold to the lung through the hematogenous route may be seen in approximately 20% of patients at presentation. A tc-99 bone scan while documenting the extent of local pathology also helps to rule out multifocal disease or skeletal metastasis. The purpose of a staging system for musculoskeletal neoplasms is to present prognostic data and counsel potential treatment strategies whereas allowing comparability of end result research in similar cohorts of sufferers. Staging describes the anatomic extent of the lesion, the degree of aggressiveness and the presence or potential to develop metastasis. The stage of the tumor is, therefore, influenced by its histological grading, native extent and distant unfold. Tumor grade, its native extent and the presence or absence of metastasis are the necessary thing components in staging for sarcomas. Correlation of medical information such as the age of the patient, site of the disease mixed with its clinical course and the radiological imaging helps to slender the possible diagnosis previous to obtaining a tissue sample. Additional ancillary investigations could be performed depending on the differential prognosis obtained after clinicoradiological correlation. Communicating all this relevant information to the pathologists also helps them in arriving at an correct prognosis. Radiograph should essentially be taken in two perpendicular planes visualizing the whole size of the affected bone. Various radiological options like location of the lesion, skeletal maturity of the bone, zone of transition and type of periosteal reaction and character of the matrix assist reach an applicable differential prognosis. It helps determine whether or not the tumor has breached normal anatomical boundaries and likewise illustrates its relation with the adjacent neurovascular constructions. This system was designed for sarcomas arising from the mesenchymal connective tissue of the musculoskeletal system. Lesions derived from the marrow, reticuloendothelial tissue and mesenchymal soft tissue are excluded. It is predicated on histological grade, local tumor extent (whether confined to an anatomical compartment or not) and the presence or absence of metastasis (Table 3). Enneking has additionally devised a staging system for benign bone tumors, which relies on the biologic behavior of those tumors (Table 4). The optimum integration of scientific and radiographic info previous to biopsy has essential implications for the diagnosis of bone tumors, and is important for accurate pathologic interpretation. This is where the multidisciplinary cooperation between radiologist, clinician and the pathologist turns into important. Ideally, the biopsy have to be performed by or beneath the supervision of the surgeon who shall be carrying out the ultimate remedy. Irrespective of the technique the complete biopsy tract needs to be excised at definitive surgery, hence the place of biopsy incision is critical and must all the time be in the line of deliberate definitive surgery. An Open Biopsy Involves � Greater tissue trauma � More blood loss � Higher danger of complications similar to hematoma, infection and pathologic fracture � A fear that the oozing from tumor vessels after the tourniquet (if used) is released may contaminate giant areas of the limb � General anesthesia � More elimination of pores and skin at last process (as the entire tract needs to be excised at definitive surgery), which might compromise closure during salvage surgery � In patient hospitalization and higher cost. An open biopsy is less forgiving and an accurate approach is of utmost significance if limb salvage is taken into account. Biopsy of Bone Tumors Biopsy plays a really important part within the diagnostic workup of bone tumors. It is essential that a clinician knows how to acquire enough materials within the least traumatic method without jeopardizing subsequent local control of the tumor. A poorly positioned biopsy incision, a poorly performed biopsy, or the complications of a biopsy make it tough to salvage an extremity and, in some instances, might affect the survival of the patient. Biopsy must be considered the final diagnostic procedure, not as a shortcut to diagnosis. In an open biopsy, the right approach is even more critical in order to scale back the complication charges � Incision should be as small as appropriate with the acquiring of an enough tissue specimen. If the bone have to be opened a small circular hole must be made with a trephine or drill, so that only minimum stress-risers are created. If a gap has been created within the bone, it ought to be plugged with Gelfoam or methylmethacrylate to forestall bleeding into the gentle tissues. If a drain must be used, the tract must be adjacent to and consistent with the biopsy incision. In case of a discrepancy he must focus on the identical with the radiologist and pathologist. Occasionally, a repeat biopsy could additionally be warranted in certain contentious cases to keep away from errors in subsequent administration. A biopsy, subsequently, plays a vital function in diagnosis and can even have a bearing on definitive management and supreme survival of the affected person. Though technically easy, it requires considerable have established an operative plan prior to biopsy. Tumors are heterogeneous and the entire tissue is finest despatched to a single heart for probably the most correct analysis. The resultant slides and paraffin blocks may be circulated for multiple opinions if essential. In such cases a good adage to bear in mind is: "Culture what you biopsy; biopsy what you tradition. After enough preparation of the skin the shortest path to the lesion is used, avoiding important neural and vascular structures and not traversing multiple anatomical compartments. In case of bone tumors with a soft tissue component the specimen could be obtained from the delicate tissue component using a Tru-cut needle-biopsy system. The sample from the delicate tissue mass is as principles of managemenT of bone Tumors thought and planning previous to its execution in order to be of maximum profit to the surgeon and the affected person. In bone, the obstacles are cortical bone and articular cartilage; in joints, articular cartilage and joint capsule; and in delicate tissues, the major fascial septa and the tendinous origins and insertions of muscular tissues. In a later stage with advancing disease they violate their compartmental barriers and turn into extracompartmental. Unlike benign tumors that are enclosed by a real capsule composed of compressed normal cells, sarcomas are usually surrounded by a pseudocapsule or reactive zone. High-grade sarcomas have a poorly outlined reactive zone that might be locally infiltrated by tumor leading to satellite tv for pc lesions at some distance from the tumor.
Sweet Weed (Marshmallow). Vardenafil.
- Are there any interactions with medications?
- Are there safety concerns?
- Sores, skin inflammation, burns, wounds, insect bites, chapped skin, diarrhea, constipation, stomach and intestinal ulcers, irritation of the mouth and throat, dry cough, and other conditions.
- Dosing considerations for Marshmallow.
- How does Marshmallow work?
- What is Marshmallow?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96755
20 mg vardenafil cheap visa
Nonarthritic symptoms in men are increased urinary output erectile dysfunction pills amazon generic vardenafil 20 mg otc, burning micturition medicare approved erectile dysfunction pump vardenafil 20 mg buy discount line, urethral discharge and prostatitis. In girls, there may be inflamed cervix, inflamed urethra, inflicting a burning micturition, salpingitis and vulvovaginitis. Ocular symptoms similar to red eyes, painful and irritated eyes and blurry vision, conjunctivitis and uveitis. There is must rule out other situations, similar to rheumatoid arthritis and lupus. Rest to scale back ache and inflammation and train to strengthen muscle tissue and enhance joint function are the others. Other peripheral musculoskeletal manifestations, corresponding to enthesitis or dactylitis, are additionally indications for immunomodulatory remedy. Disability and handicap in rheumatoid arthritis and ankylosing spondylitis-results from the German rheumatological database. Successful treatment of lively ankylosing spondylitis with the anti-tumor necrosis factor-alpha monoclonal antibody infliximab. An open examine of pamidronate in the therapy of refractory ankylosing spondylitis. A six-month randomized, managed, double-blind, dose-response comparison of intravenous pamidronate (60 mg versus 10 mg) within the treatment of nonsteroidal anti-inflammatory drug-refractory ankylosing spondylitis. EnteropathicArthritis:InflammatoryBowel Disease-associatedArthropathy42 Inflammatory bowel disease-associated arthropathy is considered a subtype of seronegative SpA, with axial, peripheral, or a mix of both joint manifestations. Peripheral arthritis is usually nonerosive and the oligoarticular variant notably may correlate with intestinal disease activity. Axial arthritis could embrace inflammatory back pain, sacroiliitis, or spondylitis, and is much less likely to correlate with gastrointestinal symptoms. While there have been advances in identifying predisposing genetic 508 textbook of orthopedics And trAumA 28. Magnetic resonance imaging examinations of the backbone in sufferers with ankylosing spondylitis, before and after successful therapy with infliximab: analysis of a brand new scoring system. Efficacy of etanercept in the treatment of the entheseal pathology in resistant spondylarthropathy: a clinical and magnetic resonance imaging research. Effects of a loading dose routine of three infusions of chimeric monoclonal antibody to tumour necrosis factor-alpha (infliximab) in SpA: An open pilot examine. Randomized doubleblind comparability of chimeric monoclonal antibody to tumor necrosis factor-alpha (infliximab) versus placebo in active spondylarthropathy. Recombinant human tumor necrosis issue receptor (etanercept) for treating ankylosing spondylitis: a randomized, controlled trial. Tuberculosis associated with infliximab: a tumor necrosis factor-alpha-neutralizing agent. Ankylosing spondylitis assessment group preliminary definition of short-term enchancment in ankylosing spondylitis. Comparison of sulfasalazine and placebo in the therapy of psoriatic arthritis: a Department of Veterans Affairs cooperative research. There are quite a few considerations which must be addressed before continuing to surgical procedure together with current serum levels, etc. Imaging research like radiographs, computerized tomography scans, radionucleotide scans and infrequently magnetic resonance imaging of the involved joint are crucial to resolve the extent of damage. When surgery is offered, explain that the main expected benefits are: � Pain aid. Do not let concerns in regards to the long-term durability of prosthetic joints affect choices to supply joint replacements to younger people. Monocompartmental arthritis of the knee is considered one of the common indications for deformity correction surgical procedure supplied the illness progression has stopped. Common Surgical Procedures Synovectomy Partial synovectomy is indicated in patients where joint destruction is minimal and if the primary cause of pain and swelling is synovitis not responding to conservative therapy (usually accomplished in knee and ankle). In elbow along with synovectomy, radial head excision could be tried in severe circumstances. In wrist dorsal synovectomy with or without resection of distal end of ulna could be attempted. In Nineties, several publications forged doubt on arthroscopic debridement for knee arthritis as a device for routine apply. But now it is extremely much clear that routine arthroscopic debridement has not a lot role in disease prognosis. Osteotomy If articular floor of hip or knee is partially damaged then osteotomy may be planned often with age of patient below 60. In seronegative arthropathies spinal osteotomy to appropriate spine deformity may be carried out. Anteriorly tibialis anterior and below lateral malleolus the peronei are concerned. The surgical approach is made through curvilinear incision 1 cm posterior to medial malleolus. Lack of movement after fusion of the wrist may be absorbed at the elbow and shoulder without significant useful improvement, however fusion of the hip puts lot of pressure on the backbone and knee. In these joints, the useful loss is much less disabling and arthroplasty is little much less dependable. Ankle Arthrodesis For over 40 years, ankle arthrodesis is the mainstay for end stage arthritis for which quite a few techniques and approaches exist. Unfortunately it results in 60�70% loss of sagittal movement in addition to decreased motion in subtalar joint. Usually exterior fixators are preferred if severe osteopenia is there and also when pre-existing septic joint state is there. Clinically strolling speed is decreased by 16% and in addition to different complications, an elevated incidence of arthritis in hindfoot and midfoot joints has been noticed. Surgery for Rheumatoid Hand and Wrist the surgical procedures generally required can be grouped as prophylactic surgical procedures and reconstructive surgeries. Prophylactic surgery because the name suggests, may delay the joint and tissue destruction by lowering the disease activity and by eradicating the infected granulation tissue. Reconstructive procedures are carried out in superior illness and embrace tendon transfer, arthroplasty and arthrodesis. The tendon sheath involvement can cause swelling over the dorsum or volar aspect of wrist. Each affected compartment is opened in a systematic manner and inflamed tenosynovium is excised utilizing sharp dissecting scissors. The wrist joint could be accessed through a flap or transverse incision of the capsule. Volar tenosynovitis could cause signs of carpal tunnel syndrome or flexor tendon attrition and subsequent rupture.
Cheap 10 mg vardenafil mastercard
Function favors osteogenesis: Healing of a fracture is instantly proportional to vascularity of the world impotence under 30 20 mg vardenafil buy mastercard. There is overwhelming evidence that function somewhat than relaxation is more beneficial in obtaining uneventful osteogenesis erectile dysfunction caused by hemorrhoids discount 20 mg vardenafil mastercard. Less muscular atrophy: When functioning, the power of the muscle tissue of the fractured limb is maintained until fracture therapeutic happens. When the gentle tissues are gliding, growth of inelastic deep scar of the delicate tissues. Pumping action of muscle helps to clear tissue edema and enhances mineralization of bone. The suppression of peripheral callus by surgical introduction of plates and screws is a extreme interference with the normal means of bone union. Such interference is demonstrated by the necessity to delayed elimination of steel units for about twice the time than it usually takes for a callus to turn out to be structurally environment friendly and consolidated. The practical treatment of fractures has significantly lowered the value of management of many widespread fractures and the period of hospitalization. He or she is up, can attend to his or her work earlier after healing of fractures. This has the Basic Principles of Functional Treatment3 Basic principles of closed therapy of fractures by practical cast and cast-brace have been extensively studied by Dehne, Sarmiento and others. The initial shortening: Soft tissues of the leg encased in a plaster solid stabilize the fracture and forestall shortening. The affected person can return to a close to regular practical activity throughout healing period. Functional cast or brace is very appropriate to fractures of lengthy bones such as tibia, humerus the place angulation, rotation and shortening could be managed. However, its utility to intraarticular and periarticular fractures could be very restricted. Prolonged immobilization of the limb, not the fracture itself causes "fracture disease". Nonunion is nearly absent: the large periosteal callus shaped offers structural rigidity and stabilizes the limb within the early as well as late stages of therapeutic. Ian Macnab quotes Girdlestone,6 "It is maybe timely, therefore, to keep in mind the phrases of Girdlestone who acknowledged in 1932". For a long bone is a plant, with its roots in the delicate tissues, and when its vascular connections are broken, it often requires, not the technique of a cabinet maker, but the patient care and understanding of a gardener. The inevitable injury to the periosteum occurring during open reduction and inside fixation should, preface, jeopardize the blood provide to the distal fragment and thereby delay union. Unless skillfully carried out, the potential disasters inherent in an open discount of a fractured tibia far outweigh its theoretical advantages. Sarmiento7 makes the next observations "Surgical intervention by internal fixation of long bones is a violation of the physiological strategy of osteogenesis. Fractures of the appendicular skeleton heal, not due to the surgery performed, however despite it. Internal fixation of fractures is commonly resorted to due to the concern that on functioning or weight bearing, the limb would become short, such a concern it ill-founded. Rigid fixation is unphysiological and deprives the skeletal structures of subjection to the conventional stresses, which preserve the physical and metabolic properties of bone. Likewise, the premise established by Robert Jones, the "relaxation enforced, uninterrupted and extended is the main basis of sound healing" when rigidly adhered to is deceptive and often damaging. Slight, controlled fracture movement associated with functional weight bearing provides early callus response most beneficially. The idea that closed therapy demands absolute immobilization of the joint proximal and distal to the fracture has additionally been disproved, particularly by the work of Sarmiento. The proof abounds that the practical movement somewhat than forced immobilization is most appropriate with effective healing. The results of operative remedy, even in probably the most experienced palms, might come close useful management. The surgeon who elects to carry out open reduction of fracture tibia assumes or causes the affected person to assume, the risks which are pointless in the majority of the fractures. Complications Preventable Malunion-angularly rotatory deformity and shortening are preventable so additionally compartment syndrome and thromboembolic disease. An necessary dictum for treating fractures of tibia is not to open the closed fracture for inner fixation and not to shut the open fractures on the major administration (debridement). Role of Soft Tissue Soft tissue controls the amount of motion at the fracture by three mechanisms: 1. The muscle compartments act as fluid-like buildings when surrounded by a inflexible plaster cast. For this "hydraulics"5 effect of the tissue, correct cosy match of the solid or brace to the leg is necessary. The second mechanism is the intrinsic strength of the delicate tissue as they help the bone fragments. The highly effective interosseous membrane that bridges the two bones additionally performs an essential role in stabilizing fragments, whether it is intact. Sarmiento5 summarizes the function of soft tissue in the stabilization of tibial fractures. Initial shortening at the time of fracture when immobilized in functional forged stays primarily unchanged. The place is maintained although features, or weight bearing is permitted previous to improvement of intrinsic stability. Hydraulic Vascularity Bone formation is instantly proportional to the vascularity at the fracture site. The affected person actively works on toe movements, and isometric quadriceps and leg muscle exercises and leg elevating. Pain on passive extension of toes and undue ache within the leg should alert the physician to search for compartment syndrome. The affected person must be off the bed as soon as possible even the following day and move on crutches or walker and bear weight to tolerance. The patient is instructed to take the load on his or her palms and never in the axillae. The reverse shoe needs a carry of 3/4 to 1 inch to compensate for the straight knee and the thickness of the plaster on the volar side of foot of the fractured leg. At about 2 weeks, he or she should discard the crutches and take a cane within the reverse hand or no strolling assist in any respect. Patient is admitted to hospital to monitor for any impending compartment syndrome.
Vardenafil 10 mg buy online
The patient is unable to abduct the thumb impotence from priapism surgery generic 20 mg vardenafil amex, and sensation is misplaced over the radial three and a half digits drugs for erectile dysfunction 10 mg vardenafil generic with visa. In long-standing instances, the thenar eminence is wasted and trophic changes may be seen. Symptoms are usually mild and intermittent pain within the hand with tingling and numbness within the median nerve distribution especially at night time when the hand is tucked in with the wrist flexed and immobile. Ulnar Nerve Injuries Anatomy Ulnar nerve arises from medial twine of brachial plexus and descends the interval between axillary artery and vein. At the insertion of coracobrachialis, nerve pierces medial intermuscular septum, enters the posterior compartment of the arm beneath cover of the medial head of triceps. At the elbow, it lies behind the medial epicondyle of the humerus and enters the entrance of the forearm by passing between two heads of flexor carpi ulnaris. It then runs down the forearm between flexor carpi ulnaris and flexor digitorum profundus muscle tissue. At the wrist ulnar nerve turns into superficial and lies between tendons of flexor digitorum superficialis and flexor carpi ulnaris. High Lesions High lesions are usually because of forearm fractures or elbow dislocation, but stabs and gunshot wounds may damage the nerve at any stage. The indicators are the same as those of the low lesions however, as well as, the long flexors to the thumb, index and the center fingers, the radial wrist flexors and the forearm pronator muscles are all paralyzed. Typically the hand is held with the ulnar fingers flexed and the index straight (the "pointing finger"). In the uncommon anterior interosseous nerve syndrome, this quick motor department of the median nerve could also be trapped slightly below the elbow underneath the humeral part of the pronator teres muscle. According to Spinner,7,8 anterior interosseous nerve syndrome may cause various indicators and signs. The sufferers complain of pain in the forearm and feeble pinch because of weakness of thumb and index finger flexion. Variations in the sensory provide of the median nerve may be confusing, however normally the volar floor of thumb, of the index and center fingers, and of the radial half of the ring finger and the dorsal surfaces of the distal phalanx, of the index and center fingers are supplied by the median nerve. Medial half of flexor digitarum profundus muscle is paralyzed, leading to lesser quantity of clawing than in lower nerve palsy. The sensory examination normally is simple, one have to study only the center and distal phalanges of the little finger, which make up the autonomous zone of the ulnar nerve. Complete anesthesia to pinpricks in this area strongly suggests complete division of the nerve. In patients suspected of having cubital tunnel syndrome, a constructive percussion take a look at over the ulnar nerve at the degree of the medial epicondyle and a positive elbow flexion check are strongly suggestive of a significant compressive neuropathy. With the elbow fully flexed, the patient will complain of numbness and tingling within the small and ring fingers, typically within 1 minute. Nerve conduction research will reveal slowing within the ulnar nerve velocities throughout the elbow. Electromyography might show fibrillations in the ulnar innervated intrinsic muscles. Ulnar neuritis13 may be attributable to chronic entrapment of the nerve in medial epicondyle tunnel causing tardy ulnar nerve palsy in extreme valgus deformity of the elbow. Traction of the nerve, subluxation or dislocation of the nerve, and entrapment syndromes can also cause ulnar nerve deficits that may require surgical remedy. Tardy ulnar nerve palsy10 could develop after malunited fractures of the lateral humeral condyle in kids, displaced fractures of the medial humeral epicondyle and dislocations of the elbow and contusions of the nerve. In 1958 Feindel and Stratford 11 coined the time period cubital tunnel syndrome to describe a compression neuropathy of the ulnar nerve in regards to the elbow with no antecedent trauma. In different areas, the nerve may be compressed by tight fascia or ligaments, neoplasms, rheumatoid synovitis, aneurysms, vascular thrombosis, or anomalous muscles. Postoperative ulnar nerve palsy may end result from both direct strain on the ulnar nerve on the elbow or prolonged flexion of the elbow throughout surgical procedure. The ulnar nerve is especially susceptible to compression when the forearm is allowed to relaxation in pronation. Alvine and Schurrer12 have suggested that some patients may have a preexisting subclinical cubital tunnel syndrome which will predispose them to this complication. Treatment Acute clean reduce accidents of ulnar nerve should be handled by exploration and end-to-end anastomosis. If the lesion is distal to the muscular branches within the forearm, gaps of 12�15 cm can be closed by mobilizing and transposing the nerve, flexing the wrist and elbow, intraneural dissection of the motor branches up the nerve, and sacrificing the articular branches. The nerve ought to be transposed solely after probably the most painstaking intraneural dissection of the branches to the flexor digitorum profundus and flexor carpi ulnaris. The nerve may be transposed anteriorly either subcutaneously or deep to the flexor-pronator muscular tissues by removing their origins from the medial epicondyle. The medial intermuscular septum must be divided proximal to the elbow to allow flexion and extension of the joint without kinking or stretching the nerve. As a substitute for awkward positioning and intensive mobilization of nerve, interfascicular nerve grafting should be thought of. Clinical Features and Examination Low lesions are often attributable to cuts at or around wrist. In long distance cyclists who lean with pisiform Results of Sutures of Ulnar Nerve Motor recovery is extra important than sensory recovery. After suture of the ulnar nerve about half of these patients could also be expected to show return of perform within the long flexors of the fingers and wrist, and some useful operate in the interossei and hypothenar intrinsic muscle tissue. Only 5% of the sufferers may recover unbiased function of the interossei, 78% might regain helpful motor restoration underneath favorable circumstances, and 16% may present unbiased finger movement. Sensory recovery not often occurs after 9 months in high lesions, however has been said to occur as late as 31 months after damage in low lesions. In cases of refractory tardy ulnar nerve palsy, removal of the nerve from its groove, neurolysis, if essential and anterior transposition15 of the nerve to the flexor floor of the elbow may be required. The surgical treatment of cubital tunnel syndrome14 includes easy decompression, medial epicondylectomy,16 and anterior transposition of the ulnar nerve either right into a subcutaneous, intramuscular, or submuscular mattress. Of the radial nerve accidents 33% are associated with fracture of middle third, 50% with fracture of distal one-third of humerus. Seven p.c with supracondylar fracture of the humerus and 7% with dislocation of radial head. Radial Nerve Injuries Anatomy Radial nerve is a continuation of the posterior cord of the brachial plexus, consists of fibers from cervical fifth, sixth, seventh, eighth and generally from first dorsal. The entry of the nerve in upper arm is accompanied with profunda brachii artery between the lengthy and medial head of triceps. The nerve is in direct contact with the humerus only within the distal arm where it enters in the anterior compartment by piercing the lateral intermuscular septum. At a distance of 10 cm proximal to the lateral epicondyle, radial nerve enters the anterior compartment of arm via the lateral intermuscular septum and lies between brachialis and brachioradialis. The motor branches to branchioradialis and extensor carpi radialis longus are given off on this space above the elbow. A department can also be given to brachialis, however is predominantly equipped by musculocutaneous nerve.
Cheap vardenafil 20 mg free shipping
This method is normally too complex erectile dysfunction treatment by injection cheap vardenafil 20 mg free shipping, timeconsuming and painful impotence 35 years old 10 mg vardenafil safe, since all the wires have to be loosened and retensioned. A mathematical analysis of the impact of flexion and rotation on apparent varus/valgus alignment at the knee. Presented on the North American Clinical Gait Lab Conference, Portland, April 9; 1994. Construct Considerations For Rotational Deformities Most rotational deformities are corrected by rotational modifications of the basic hinge frame. This geometric relationship may be applied to the Ilizarov equipment to calculate the appropriate variety of distractor turns. Here, the hinge is positioned immediately over the center of rotation of the ankle joint. For instance, if our equation tells us to distract three mm/day at the distractor, you could inform the patient to distract 1 mm (one complete turn) thrice every day. If you draw concentric circles centered on the hinge, you get a slightly extra accurate estimation. This is especially true when your body is unusual as is commonly the case from translation hinge frames. These numbers are the distances from the hinge point to the far rings and the gap from the hinge line to the distractor connection. Biomechanics of Soft Tissue Contractures during Limb Lengthening2 Muscle tendon unit is the main hurdle in limb lengthening. The knee tends to extend throughout femoral lengthening and valgus and flexion during tibial lengthening. The shoulder tends to lose abduction, while the elbow tends to lose flexion throughout a humerus lengthening. The elbow loses extension and the wrist tends to lose dorsiflexion throughout lengthening of the forearm. Rehabilitation is based upon a technique to overcome resistance of the stronger muscular tissues which create these deformities. Stretching of the muscular tissues stimulates the muscle development and maintains the size and prevents joint deformity. Because the joints develop compensatory deformation, within the extreme varus deformity of the femur and tibia, the subtalar joint goes into extreme valgus deformity. Therefore, often two or extra osteotomies are essential to appropriate the deformity and to restore the mechanical axis of the lower limbs. Because the correction is completed slowly during the postoperative period, if there are any neurovascular issues that develop throughout distraction, one can cease the distraction. One can choose the number of osteotomy one or two or more, and also the degrees of osteotomy. As a bow has multiple apices, normally a couple of osteotomy is required for its correction. The magnitude and level of the first osteotomy will decide the magnitude and degree of the second osteotomy (osteotomy rule 3). This produces a zigzag within the anatomic axis of the bone and, therefore, leaves a small bump on the bone. This might represent a beauty drawback if the bump is on the subcutaneous floor of the bone. The bump is usually of no practical significance as a outcome of the mechanical axis is realigned, and the joint orientation is restored to normal (corollary to osteotomy rule 3). In this affected person, the infected nonunion, the bowing deformity of the femur and the valgus deformity of the knee, all these were corrected with one equipment and one process. In Case 1, the corollary of osteotomy rule 3 of Paley was utilized and just one osteotomy was accomplished. Causes of Bowing1 Preoperative Planning of Bowing Deformity1 As in a simple angular deformity, perfect preoperative planning is critical before correction. It differs from easy angular deformity in that in distinction to simple deformity, it has a quantity of apices. Although the proximal and distal bone axes are fastened, the center axis could be manipulated to Steps of Planning Step zero: Draw the mechanical axis line from center of the top of femur to the middle of ankle. Step 1B: Draw the respective mechanical axis relative to these joint orientation strains, i. The intersection level of the proximal and distal femoral and tibia 1172 TexTbook of orThopedics and Trauma There is an alternative methodology for preoperative planning of bowing deformity. Step 0: Draw mechanical axis of the limb from the center of the hip to the center of the ankle. If the total angle is less than 20�, the deformity may be corrected at this level with the only osteotomy. Step 3: To find out two levels of osteotomy "center segment concept" is given by Dror Paley. Where it intersects proximal and distal mechanical axes strains are the two levels of osteotomies and the angle subtended at each level offers the angle of correction to be accomplished at that degree. Step 3B: the middle section could be shifted distally or proximally for the convenience of the extent of osteotomies. Step 4, 4A and 4B: Show complete correction of the bow by taking middle section at completely different levels. According to Paley and Tetsworth, recognizing the importance of joint reference lines and particular person segment mechanical axis lines permits the orthopedic surgeon to preoperatively plan correct correction of extraordinarily complicated multilevel angular deformities. Based on these rules, the quantity, type and placement of the osteotomies could be deliberate. It is completely unacceptable to perform mechanical axes offers whole angular deformity in each bone. If single osteotomy is performed at each of these ranges, mechanical alignment and joint orientation turn out to be normal. So, one can do osteotomy distal to the apex at the junction of center and decrease third. Step 2B: After correction at one osteotomy, one can locate the place the two mechanical axis lines subsequently intersect. So, the positioning of first osteotomy can be chosen at the level that empirically seems finest for correction. Step 3: the second apex is decided and the remaining correc tion of the angle is completed. Step 4: the mechanical axis line of the corrected femur is then prolonged distally. Intersection of proximal and distal tibial mechanical axes lines offers total angular deformity in tibia. Step 5: After correction of half the deformity at distal stage, intersec tion of proximal and distal mechanical axes lines provides second level of osteotomy. The femur is corrected to restore its mechanical axis and the hip and knee joint orientations to regular. The mechanical axis line of the femur from the center of the hip to the middle of the knee is then prolonged distally to act because the mechanical axis of the proximal tibia. The quantity of correction is performed related to a line drawn up the shaft of the center of the tibia.