
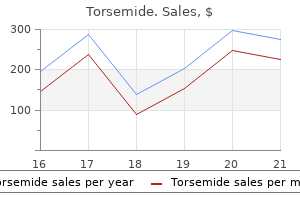
Torsemide dosages: 20 mg, 10 mg
Torsemide packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

20 mg torsemide buy with mastercard
Clamps running suture may be used blood pressure chart heart and stroke order torsemide 10 mg free shipping, carefully avoiding pursemay be used however very cautiously arteria radial purchase torsemide 20 mg amex. Second forceps utilized just distal to first and slid farther downstream to milk blood from intervening section. Treatment on the scene of the accident and at first medical contact strongly affects the finish result of later replantation. Improper dealing with of the amputated part or stump can seriously compromise the final result. The affected person must be hemodynamically secure earlier than either transportation or replantation is tried. If bleeding persists, nonetheless, it should never be stopped with the blind utility of a hemostat, because this will additional injury the neurovascular structures. Graft harvested from dorsum of finger or volar facet of wrist; for vein replantations in lower limb of buildings larger than digit, graft obtained from saphenous vein. Digital nerves include solely sensory fibers and are repaired with easy sutures via epineurium only. The severed part is cleaned of any gross contamination and international materials and cooled to reduce its metabolic rate. A severed digit must be wrapped in moist gauze and positioned in a watertight plastic bag, which is then immersed in ice water. The amputated half must not be allowed to are available to direct contact with any ice, and dry ice ought to by no means be used. Properly cooled, a digit could be successfully replanted within 30 hours of amputation. The amputated half is cleaned of all gross contamination, wrapped in a moist towel, and positioned in a plastic bag. Alternative method is to compress finger pulp and note time for return of turgor and shade corresponding to regular finger. The part is then placed in an insulated container (but not in touch with the ice) and maintained at 10�C. Thus ready, the amputated part is clearly labeled and quickly transported to the replantation middle. Cold ischemia can protect muscle up to 8 to 12 hours, after which irreversible changes may occur. Warm ischemia, which results from improper cooling, can lead to irreversible adjustments in as little as four to 6 hours, thus stopping successful replantation. Several attempts have been made to scale back ischemia time by perfusing the amputated limb with various substances corresponding to oxygenated fluorocarbon solutions. At present, essentially the most dependable fluid seems to be autologous arterial blood mixed with heparin. Perfusion plus cooling might make major replantations possible as much as 12 to 16 hours after injury. In the emergency division, tetanus prophylaxis and a broad-spectrum antibiotic are administered as soon as attainable. Once the decision to undertake replantation is made, the severed half is taken to the operating room. While one team prepares the affected person for surgical procedure, the opposite staff totally debrides the amputated half, viewing it beneath magnification. All devitalized and closely contaminated tissue is excised, together with frayed tendon ends, comminuted bone fragments, however solely a small margin of pores and skin, as a outcome of coverage is necessary and skin is more resilient than deeper tissues. Frayed tendon ends are excised because Pulse oxygen monitor Tracing exhibits occluded blood provide the harm to the exposed tendon surfaces tremendously increases the risk that adhesions will subsequently type and prohibit motion. Bone is trimmed to (1) remove avascular bone that might provoke the development of osteomyelitis; (2) provide flat, congruent surfaces for secure bone fixation; and (3) provide the mandatory skeletal shortening to facilitate tension-free vessel anastomoses and nerve coaptations after debridement. An interosseous wire or a Kirschner wire can be placed in the bone of the amputated part to facilitate later fixation. The distal arteries, veins, and nerves are identified and tagged with fine sutures. Only full-thickness skin flaps are mirrored; the subcutaneous tissue and veins are left intact for later dissection underneath microscopic visualization. While the amputated half is being prepared, the patient is transferred to the operating room and regional anesthesia is administered (preferably an axillary block). Regional anesthesia provides some sympathetic blockade and vasodilation as nicely as ache reduction. The surgeon thoroughly debrides the stump, shortening the bone and tendon to allow easier anastomosis of vessels and coaptation of nerves. Once corresponding constructions within the stump and the amputated half have been identified, replantation is begun. Because stability is essential for the vascular reconstruction, bone fixation is carried out first. The technique of bone fixation must be applicable for the type and degree of amputation and provide secure fixation for early mobilization. Fixation units include interosseous wires, Kirschner wires, and compression plates and may decrease additional delicate tissue disruption. Replantation on the phalangeal stage could be secured with interosseous wires with or without the added stability of a Kirschner wire; some surgeons prefer to use crossed Kirschner wires. Replantations on the joint level require a removable fixation system if the joint is to be preserved; in any other case, any commonplace method for arthrodesis of small joints is appropriate. If contamination is significant, nevertheless, an exterior fixator ought to be used to cut back the risk of an infection. Severed palmar metacarpal arteries from deep palmar arch to common digital arteries ligated to keep away from hematoma. Kirchmayr (Kessler) sutures are used to repair flexor tendons, and interrupted figure-of-eight sutures are used for extensor tendons. Repair of Blood Vessels and Nerves After repair of bone and tendon, microvascular clamps are applied to the ready arteries and veins, the tourniquet is launched, and the blood circulate is famous. Flap with sufficient subcutaneous tissue dissected free with vascular pedicle entering at one finish and leaving at other. Repairing rather than resecting injured and compromised vessels to keep away from use of vein grafts nearly at all times ends in failure as a outcome of thrombosis occurs virtually immediately in these injured vessels. Generally, the arteries are repaired first to scale back ischemia time and to permit the surgeon to assess the adequacy of the venous debridement and determine which veins are best suited for repair. Tendons are then repaired by tying the two core stitches in each finish, including a second core sew and then an epitendinous restore. Then the skin is loosely approximated to avoid constriction of the vasculature when postoperative edema develops. For instance, the lateral forearm rotation flap or free flow-through flap (see Plate 4-65) can be utilized to cowl pores and skin defects to the thumb after replantation. Use of normal pores and skin and subcutaneous tissues from an uninjured zone brings excellent vascularity to the compromised digit. However, nerve and tendon restore is usually delayed until all digits are replanted and successfully perfused.
False Indigo (Wild Indigo). Torsemide.
- Are there safety concerns?
- Ulcers, open wounds, or inflamed nipples when put on the skin, or use as a vaginal douche.
- Dosing considerations for Wild Indigo.
- What is Wild Indigo?
- How does Wild Indigo work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96595
Discount torsemide 10 mg with visa
History of current illness: It contains the details of all of the complaints talked about within the chief complaints that start with the looks of first symptom and extend as much as arrhythmia causes 20 mg torsemide for sale the time of session hypertension blood tests discount torsemide 20 mg line. It normally consists of the mode of onset (sudden/gradual), preceding events inflicting onset, course of symptoms (progressive/constant/fluctuant; and continuous/intermittent), elements aggravating/relieving, other accompanying complaints, and the therapy taken. If each the sides of ear and/or nostril are affected then it must be talked about which is worst affected. History of past illness: It includes history of similar complaints in the past and the remedy taken and history of surgical procedures, fundamental Sciences 5. Patients may be allergic to certain drugs, diets, pollens, fungi, animals and dusts. Following a specific order facilitates complete examination without missing any area. Later changes in the swelling must be inquired similar to softening, ulceration, fungation and inflammatory. Site: the location from the place the swelling started must be inquired in instances of enormous swellings. Personal historical past: Chewing of Paan (betel leaf), Sopari (betel nut), tobacco, slaked lime, smoking, alcohol, Chutta most cancers of hard palate (smoking of reverse cigars with burning end in mouth), Khaini or Masala most cancers (mixture of lime and tobacco kept in vestibule of mouth). Pain suggests acute inflamma- Examination of a swelling mainly consists of inspection and palpation and assess following parts: 1. Site and shape: the frequent sites of dermoid cysts are line of fusion of embryonic processes and embody outer canthus of eye (between frontonasal course of and maxillary process), behind the ear (between mesodermal hillocks). Note the diffuse (indistinct edge) purple colour tender swelling of tip of the nose 2. Fixity to pores and skin: these swellings include skin swellings (papilloma, epithelioma, sebaceous cyst) and subjacent malignant swelling involving skin such as secondary metastatic neck nodes and carcinomas of oral cavity, larynx, laryngopharynx, thyroid, and salivary glands. Edge: Well-defined (neoplasms), irregular (malignant), smooth (benign neoplasms and cysts), diffuse or vague (acute inflammation). It is extending from the angle of mandible to the mastoid and elevating the ear lobule 8. On palpation of the edge of swelling cyst margin slips away whereas lipoma margin yields. Consistency: Soft (lipoma), cystic (cyst, hematoma, abscess), agency (fibroma), hard (bony, cartilaginous and malignant tumors), variable (malignancy), crepitus (surgical emphysema), molded due to inside putty-like (pultaceous) materials (sebaceous and dermoid cysts), pits on strain (inflammatory). Translucent: Translucency is current in the cysts that contain clear fluid similar to cystic hygroma and laryngocele. Tubercular ulcers are oval form to begin with however later on coalesce and provides irregular crescent edge. Number: Inflammatory lesions such as herpetic, tubercular and syphilitic can be a quantity of. Mild tenderness could additionally be seen in persistent infections corresponding to tuberculosis and syphilis. Base: the marked induration (hardness) of the bottom on which flooring of the ulcer rests is the feature of malignancy. Surface: Cauliflower (squamous cell carcinoma), irregular multiple branching (papilloma), irregular and rough (carcinoma). Note the involvement of the lower third of facial pores and skin supplied by the mandibular division of trigeminal nerve. In instances of malignancy regional lymph nodes could also be enlarged because of secondary infection. Nose and paranasal sinuses: Rhinosinusitis, deviated nasal septum (touching middle turbinate), vacuum headache (negative stress in sinuses) and tumors b. Oropharynx: Peritonsillar abscess, parapharyngeal abscess, retropharyngeal abscess and tumors. Infections: Encephalitis and meningitis brought on by suppurative otitis media and sinusitis. Patients typically complain of poor concentration and different obscure nonspecific symptoms. Aggravating elements: Headache is fixed daily and may be exacerbated by emotional stress, fatigue, noise or glare. It is related to ipsilateral conjunctival congestion (red eye), lacrimation, nasal congestion and rhinorrhea. Oxygen: Inhalation of 100 percent oxygen (12�15 L/min for 15 minutes) by way of a non-rebreather mask. Xylocaine and corticosteroid: Greater occipital nerve block with native injection of xylocaine and corticosteroid. Headache growing after 2 weeks of injury is normally not related to head damage. Other related complaints which can be current include impaired reminiscence, emotional instability and increased irritability. If easy analgesics fail then amitriptyline, antiseizure medication, propranolol, or ergot derivatives are used. Baclofen (10�20 mg three or four instances a day): It could also be used both alone in combination with above molecules. Noninvasive procedures: � Radiofrequency rhizotomy: this simple process is most popular in elderly patients with a restricted life expectancy. Exploration of posterior cranial fossa: Simple decompression and separation of anomalous vessel from the nerve root usually produce lasting reduction. Clinical features: this transient (few minutes or less) however extreme headache is produced by coughing, straining, sneezing and laughing. Section 1 w basic Sciences big cell (temporal or cranial) arteritis In addition to the superficial temporal, other arteries which are sometimes affected are vertebral, ophthalmic and posterior ciliary arteries. The headache is often related or preceded by myalgia, malaise, anorexia and weight reduction. Biopsy reveals lymphocytes, histiocytes, plasma cells and large cells in media and adventitia. In circumstances of blindness intravenous pulse Methylprednisolone (1 gm day by day for three days) is given. Initially the burning ache has restricted distribution however soon spreads to remainder of the face. Treatment: Patients could also be given analgesics, tricyclic antidepressants, carbamazepine, oxcarbazepine or phenytoin however the response is usually not passable. Clinical features: this neuralgic ache (similar in high quality to trigeminal neuralgia) happens often in tonsillar fossa. Risk elements: They include old age, extreme rash (long duration, painful and scarring), involvement of ophthalmic division of trigeminal nerve and delayed acyclovir remedy. Myogenic disorders embrace myofascial pain, fibrositis, muscle splinting (trismus), spasm and swelling (myositis), contracture, bruxism, hypertrophy and dyskinesia. Predisposing elements: Nocturnal or diurnal bruxism (grinding or clenching) is very common. Clinical options: the commonest grievance of the patients is diffuse facial ache. Patient develops sensation of painful swollen gland just beneath the angle of mandible.
Cheap 10 mg torsemide visa
Abdominal fats mass contributes to the systemic inflammation in chronic obstructive pulmonary disease blood pressure chart by height and weight 10 mg torsemide with amex. Prognostic worth of weight change in persistent obstructive pulmonary disease: results from the Copenhagen City Heart Study blood pressure medication and weight loss 20 mg torsemide discount amex. Nutritional assist in continual obstructive pulmonary illness: a systematic evaluate and meta-analysis. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary illness. Prevalence, danger factors, activity limitation and health care utilization of an overweight, population-based sample with persistent obstructive pulmonary illness. Total respiratory system, lung, and chest wall mechanics in sedatedparalyzed postoperative morbidly overweight patients. Combined results of weight problems and continual obstructive pulmonary illness on dyspnea and train tolerance. Effects of body mass index on static lung volumes in patients with airway obstruction. Dyspnea on exertion in overweight women: affiliation with an increased oxygen cost of breathing. Obesity in maturity and its consequences for all times expectancy: a lifetable evaluation. Body-mass index and cause-specific mortality in 900000 adults: collaborative analyses of fifty seven prospective research. Weight loss is a reversible factor within the prognosis of continual obstructive pulmonary illness. Inspiratory-to-total lung capacity ratio predicts mortality in sufferers with persistent obstructive pulmonary disease. The affiliation between metabolic syndrome and restrictive ventilatory dysfunction in older persons. Lung function impairment and metabolic syndrome: the critical function of belly weight problems. Association between continual obstructive pulmonary disease and systemic irritation: a scientific evaluation and a meta-analysis. Metabolic and inflammatory profile in overweight sufferers with persistent obstructive pulmonary disease. Anorexia in continual obstructive pulmonary disease - affiliation to cachexia and hormonal derangement. Local and systemic inflammation in patients with chronic obstructive pulmonary illness: soluble tumor necrosis issue receptors are elevated in sputum. Low-grade adipose tissue inflammation in patients with mild-tomoderate chronic obstructive pulmonary illness. Osteoporosis is a skeletal disease characterised by low bone mineral density or micro-architectural deterioration, leading to increased danger of fracture. Interventions in opposition to common risk components, like smoking cessation, exercise and healthy diet, would possibly scale back the chance of fracture in sufferers with osteoporosis. In addition to these way of life tips, pharmacological treatment with calcium and vitamin D supplementation and antiresorptive remedy. The Tscore is outlined as the variety of normal deviations by which the bone mineral density differs from the typical bone mineral density of a young adult at peak bone density. With this technique, vertebral deformities are categorized in to wedge, biconcave or crush and in to grade 1 (20� 25% reduction in top and 10�20% reduction of the projected vertebral area), grade 2 (25�40% discount in peak and 20�40% discount of the projected vertebral area) and grade three (. Pathophysiology of osteoporosis Bone is mostly categorized in to two varieties: 1) cortical bone, which is dense and powerful and primarily current within the shafts of lengthy bones; and 2) trabecular bone, which is weak and porous and current at the ends of long bones or at the inside of vertebrae and flat bones. Bone remodelling is a complex interplay between osteoblasts, osteoclasts and osteocytes. These cells take away an area of bone after which exchange the misplaced bone with new matrix which subsequently mineralises. Excessive bone resorption, as a outcome of an imbalance within the amount of bone removed relative to the quantity of bone changed, will result in a decline within the complete amount of bone and will enhance the risk of fracture. When taking the vertebral fractures in to account, the prevalence of osteoporosis even elevated to 51% [11]. A assortment of these threat elements is summarised within the fracture threat evaluation software, which predicts the 10-year chance of fracture [16]. Airflow obstruction and emphysema Osteoporosis has been associated to severity of airflow obstruction. The third National Health and Nutrition Examination Survey, which included 9,502 members, confirmed that the prevalence of osteopenia and osteoporosis increased with more severe airflow obstruction [17]. In addition to its association with severity of airflow obstruction, bone density has been related to the extent of emphysema [23]. They showed that radiographic emphysema was an impartial predictor of low bone mineral density. Since bone mineral density was shown to be correlated independently with both the severity of airflow obstruction and the extent of emphysema, recent analysis has been centered on frequent hyperlinks between the skeletal and pulmonary methods [23]. Regarding the direct pathways, the Wnt/b-catenin signalling is concerned in bone remodelling and repair of micro-fractures, nevertheless it has also been associated with lung epithelial harm and repair processes. Therefore, it could be the case that impairment of Wnt/ b-catenin signalling results in each osteoporosis and emphysema. However, only oblique and experimental evidence supporting this interplay is on the market to date. The underlying patho-physiological mechanism of the connection between superior age and bone loss has been widely studied [34]. In a wholesome young skeleton the speed of bone formation and matrix mineralisation equals the speed of bone resorption and matrix degradation. However, in the course of the means of ageing important quantities of bone are misplaced as a result of enhanced bone resorption coupled with decreased bone formation. In addition to bone loss, superior age is associated with increased fall danger because of muscle weakness and stability issues leading to elevated threat of fracture [35, 36]. Body composition Low body mass/fat-free mass Low physique mass and low fat-free mass are well-known danger elements for osteoporosis within the general population [2, 16]. Indeed, astronauts lose bone mass within the proximal femur throughout area flights [41], and long-term mattress relaxation results in lack of bone mass [42]. In addition to decreased mechanical loading, poor exercise capacity might trigger sarcopenia and decrease limb muscle weakness, which has been associated to elevated fall danger and, therefore, increased risk of fracture. This may be because of an interaction between fats and bone tissue such as the results of fat mass on the secretion of bone lively hormones from the pancreatic b-cells. Several research have investigated the results of leptin, an adipokine which is said to the quantity of physique fats [44, 45]. Leptin acts through the central nervous system and by way of the circulation, leading to different effects on bone metabolism (fig. Circulating leptin increases the proliferation and differentiation of osteoblasts and promotes bone nodule formation. Leptin has the other effect through the central nervous system, by influencing satiety and insulin secretion.
Purchase 20 mg torsemide mastercard
The mammographic appearances of benign epithelial lesions are various blood pressure medication gynecomastia torsemide 20 mg cheap amex, but frequent lesions similar to cysts and fibroadenomas are usually seen as well-defined or lobulated mass lesions blood pressure 210120 cheap torsemide 10 mg mastercard. Calcification can be a common feature of cysts, columnar cell change, and sclerosing adenosis. Other benign lesions such as radial scar, complicated sclerosing lesion and fat necrosis can produce ill-defined or spiculated mass lesions, which are indistinguishable from some forms of breast carcinoma. Adenosis is a lobular-based lesion, with variably elevated numbers of acinar structures. Several histological types of adenosis have been described, and their chief importance is of their occasional mimicry of an invasive carcinoma. Epidemiology this lesion occurs most regularly in ladies in the third or fourth decade of life. Clinical options Adenosis is most frequently an incidental microscopic discovering, however may be detected mammographically because of associated microcalcifications. A few circumstances assume the looks of a agency, rubbery gray mass (nodular adenosis or adenosis tumour). On rare events, 112 Benign epithelial proliferations associated microcalcifications could additionally be so plentiful as to impart a gritty reduce surface. Histopathology Adenosis in its easiest kind is characterised by a lobulocentric, loosely-structured proliferation of acinar or tubular buildings, composed of an epithelial and myoepithelial cell layer and surrounded by a basement membrane. The acini may be elongated, and infrequently have at least a focally parallel association. The normally unfastened intralobular connective tissue is replaced by denser fibrous connective tissue with compression and distortion of the acinar buildings. B High-power view of the same lesion showing distorted and compressed tubular buildings and intervening hyaline stroma. Such lesions could pose difficulties relating to the differential prognosis with invasive lobular carcinoma. Recognition on low energy of a lobulocentric association is most useful in recognizing a non-invasive course of. Immunohistochemical research to reveal myoepithelial cells (sometimes attenuated), could also be a helpful diagnostic adjunct. Apocrine adenosis is recognized as a benign process of no recognized clinical significance and no implications for elevated risk of cancer. Microglandular adenosis, atypical microglandular adenosis and microglandular adenosis with carcinoma Definition An uncommon glandular proliferation that in most cases follows an indolent scientific course but, in uncommon cases, offers rise to carcinoma. The epithelial cells are cytologically bland with amphophilic, clear or barely granular cytoplasm. However, the presence of coalescent and expanded glandular structures with solid epithelial progress and high nuclear grade is more according to the analysis of invasive carcinoma. A haphazard proliferation of small spherical glands with open lumina composed of a single layer of flat to cuboidal epithelial cells. Radial scar and complicated sclerosing lesion Definition A benign lesion that on imaging, gross examination, and low-power microscopy may resemble an invasive carcinoma as a end result of the lobular structure is distorted by a sclerosing course of with related elastosis. Synonyms Radial scar; sclerosing papillary lesion; radial sclerosing lesion; scleroelastotic scar; stellate scar; benign sclerosing ductal proliferation; non-encapsulated sclerosing lesion; infiltrating epitheliosis. On breast imaging, the irregular stellate configuration might mimic an invasive carcinoma. Very occasionally the lesion is of adequate size to produce a palpable mass 1340. Macroscopy these lesions could also be undetected on gross examination or may be of enough measurement to produce an irregular space of firmness that may exhibit yellow streaks reflecting the elastotic stroma. A two-cell layer is retained, though this will likely not always be seen on staining with haematoxylin and I. The molecular characteristics of the various epithelial hyperplastic processes discovered inside them and the forms of malignancy related to them are described elsewhere in the relevant sections of this volume. The tubular lumina are normally empty, but might rarely contain proteinaceous materials or mucin 215. Prognosis and predictive factors Tubular adenomas are benign lesions with no known threat of recurrence when fully excised. Rarely, carcinoma can involve a tubular adenoma 576; this seems to be a fortuitous association. Definition Benign, often round, nodules fashioned by a compact proliferation of tubular buildings lined by epithelial and myoepithelial cells, much like these of the conventional resting breast. Clinical options Tubular adenoma presents clinically as a painless, palpable, nodule. Findings on imaging studies are usually a mass with well-circumscribed borders with microcalcification not often present 1352, 1369. Diagnosing tubular adenomas by fineneedle aspiration cytology may be troublesome 215,1228, and needle-core biopsy may be more dependable. Macroscopy Tubular adenomas are agency, well-circumscribed and homogeneous with a uniform, yellowish or tan-brown cut floor. B At greater magnification the glands are lined by common epithelial and myoepithelial cells. However, most lesions categorized as "lactating adenoma" symbolize nodular areas of hyperplastic lobules with secretory or lactational adjustments. Clinical options An area of increased firmness appearing throughout both being pregnant or lactation. Preoperative diagnosis is predicated on ultrasound and magnetic resonance imaging together with fine-needle aspiration or needle-core biopsy 92,483. Macroscopy Lactating adenomas vary in size, once in a while reaching giant dimensions 92. Histopathology the localized collections of lobules comprising the lesion show lactational modifications. B Lactating adenoma is characterised by secretory adjustments within the epithelial cells. Prognosis and predictive factors Lactating adenomas are benign lesions with no identified recurrences when fully excised. Histopathology Apocrine adenoma is characterised by a nodular assortment of glands lined by apocrine epithelium. Prognosis and predictive components this lesion is benign and local excision is healing. Definition A nodular collection of cysts or glands lined by apocrine metaplasia or papillary apocrine change 88,1075. The proliferating tubules might turn into distorted in the sclerotic stroma, imparting a pseudoinfiltrative look. Definition A well-circumscribed, benign glandular proliferation situated, at least partially, within a duct lumen 86. Clinical features these lesions may present as a tough mass or, hardly ever, as bloody nipple discharge 756,1033. Mammography reveals a spherical lesion with well-defined margins, sometimes with microcalcifications 628,1033.
20 mg torsemide order amex
Antidepressants: Tricyclic and serotonin-reuptake inhibitors are helpful within the management of continual pain arrhythmia technologies institute torsemide 10 mg purchase without a prescription. The generally used agents include amitriptyline (10�25 mg/ day) blood pressure joint pain purchase torsemide 20 mg fast delivery, imipramine (10�25 mg/day), fluoxetine (5 mg/day), sertraline (50 mg/day), citalopram (20 mg/day), venlafaxine (75 mg/day), nortriptyline (10�25 mg/day), bupropion (100 mg bd) and paroxetine (20 mg/day). Bite-appliance (splint) therapy: the splint is worn on the tooth and stabilizes the occlusion (in bruxism) and reduces the load. The details of surgical options, which include arthrocentesis, arthroscopy, arthrotomy (arthroplasty) and meniscal restore (plication), are past the scope of this chapter. Changing developments in otorhinolaryngological diseases at a non-government clinic in Jaipur. Emergency otorhinolaryngological cases in medical school, Kolkata-A Statistical analysis. The table also reveals the findings of clinical examination as well as their causes. The exterior auditory canal may be examined by pulling the pinna upward (in kids, downward), backward and laterally whereas the tragus is pulled forward. This procedure not solely spreads open the meatus but in addition straightens it and reveals tympanic membrane. The use of the most important ear speculum that can easily enter the canal is secure and offers a greater view. Otoscope is especially helpful in examining both the ear as well as the nostril of infants. Ear Inspection: the pharyngeal opening of Eustachian tube may be seen by posterior rhinoscopy mirror, nasal sinuscope and nasopharyngoscope. After anesthetizing the nasal cavity with 4% lignocaine, Eustachian catheter is handed in to the nasopharynx alongside the ground of nostril. Hearing of the sound of air entering the center ear indicates the patency of Eustachian tube. The most commonly used tuning fork is 512 Hz however forks of other frequencies corresponding to 256, 1,024 and a pair of,048 Hz are also desirable. It is necessary to test facial nerve and know the grade of palsy (chapter of Facial Nerve Disorders). Local causes (Primary otalgia) � Auricle: Skin lesion, perichondritis/chondritis, trauma � External auditory canal: Furuncle*, impacted wax*, otitis externa*, trauma*, foreign bodies especially reside insects*, otomycosis*, myringitis bullosa, herpes zoster oticus (Ramsay Hunt Syndrome), and malignant neoplasms � Middle ear: Acute otitis media*, Eustachian tube obstruction*, cholesteatoma*, mastoiditis*, Barotrauma, and malignancy middle ear � Intracranial issues of otitis media: Extradural abscess B. Area provided by C2 and C3 spinal nerves � Cervical arthritis/disc illness � Cervical spondylosis*, injuries of cervical spine, caries backbone 5. The vagus nerve additionally provides to vallecula, epiglottis, larynx or laryngopharynx, trachea, esophagus, and thyroid gland and cardiopulmonary system. Dental eruptions: Ear pulling in preverbal youngsters could indicate erupting dentition. Such patients often give historical past of extreme gum chewing, malocclusion and bruxism. Herpes zoster oticus: the earache can occur even in the absence of vesicular eruption. Glossopharyngeal neuralgia: the patient presents with sharp and lancinating pain that radiates to ear and originates in the tongue base, soft palate, or tonsillar fossa. Exertional left earache: In instances of exertional earache on left aspect, patient will must have cardiac session to rule out coronary artery illness. In case of suspected malignancy of oral cavity, pharynx, larynx, nose and paranasal sinuses, biopsy will affirm the analysis. Otitis externa: It might not permit center ear microscopic examination and may be secondary to otitis media. Hearing aids: Scanty serous otorrhea in regular ears may represent moisture trapping after washing or may be due to the utilization of listening to assist or ear plug. Otitis externa: It tends to delay an intensive ear microscopic examination due to edema, particles and tenderness. Contraindication: In cases of glomus tumors it should be averted as it may find yourself in profuse bleeding. Open mastoid cavity otorrhea: It wants debridement and remedy with topical antifungal or antimicrobial eardrops or acidifying and drying brokers similar to boric acid and alcohol resolution. Granulation tissue and mucosalized epithelium within the mastoid bowl requires chemical cauterization. History and Examination Section 2 Associated symptoms: Ear polyp is usually associated with otorrhea and listening to loss. High cardiac output: Pregnancy, anemia, train, thyrotoxicosis Otosclerosis Hypertension ii. M iddle ear: Otitis media, patulous Eustachian tube, hemotympanum (head injury) iii. Following two elements are advised: Deprivation of enter, or Abnormal input from the ear Neuronal plasticity and modifications in neuronal input may end result to following structural or practical changes: Changes in the nuclei of the ascending auditory pathways. Any change in the tinnitus that has occurred through the course of illness should be noted. Table three exhibits the necessary thing medical options of some common causes of pulsatile vascular tinnitus. Venous pulsatile tinnitus: In circumstances of pseudotumor cerebri and venous pulsatile tinnitus, turning of head and strain over inner jugular vein will lower or cease the tinnitus. Light pressure over ipsilateral jugular vein and turning of head on one explicit aspect diminish or obliterate jugular venous tinnitus. Audiologic Evaluation � Tuning fork checks � Pure tone audiometry � Speech perception in quiet and noise � Tympanometry D. Section 2 w Tinnitus Management Program In spite of treating every affordable medical cause for tinnitus, majority of sufferers report little improvement. The transverse-sigmoid-jugular venous system are right-sided dominant (superior sagittal sinus continues as right-sided transverse sinus) in 75% of people. The tinnitus and its coincident symptoms corresponding to insomnia, anxiety/stress, despair and fatigue form a vicious circle of signs. These coincident signs need effective remedy (medical and psychotherapy) as a result of their enhance would worsen the tinnitus. In-the-ear gadgets: For many sufferers direct sounds to their ears are more practical than environmental sounds. In-the-ear gadgets, although comparatively costly are most portable, inconspicuous and efficient in acquiring aid from the tinnitus. Though train could increase tinnitus drawback in patients, it ought to be done often because it helps in stress reduction and improve cardiovascular well being, muscle tone, mood and sleep patterns. This noninvasive remedy supplies not only quick aid however there additionally happens tinnitus suppression or temporary disappearance of tinnitus (residual inhibition). These sufferers may develop phonophobia and overprotect their ears by sporting earplugs and earmuffs. Factors aggravating tinnitus � Stress/fatigue � Excessive noise publicity � Upper respiratory tract infections and allergy � Moving jaws/clenching teeth � Head and neck trauma � Changes in altitude � Too a lot use of aspirin, alcohol, caffeine, acetaminophen, or ibuprofen � Changes in body position � Tobacco and marijuana B.
Buy torsemide 20 mg line
To understand the relationships and approaches to the proximal stomach aorta blood pressure medication causes nightmares torsemide 10 mg cheap without prescription, one should understand thean~~yofthem~~Theili~~ consists of a crown of axial muscle fibers originating from the rim of the inferior thoracic aperture and inserting in to a robust arrhythmia in 4 year old order torsemide 10 mg mastercard, aponeurotic, three-lobe central tendon. These slips of origin interdigitate pexpendicularly with the origins of the transversus abdominis muscular tissues. The last elements of the origins are the crura, which originate from the anterior surfaces and anterior longitudinal ligament of the first three lumbar vertebrae on the proper and the primary two on the left. Note the ascending association of aortic, esophageal, and inferior vena cava openings. The rim of the diaphragm reflects the inverted V of the costal margin anteriorly, runs transversely across the posterior flanks, and seems to sprout from the roots of the crura. The domes present a bilobed mammillation depressed centrally on the seat of the heart and indented posteriorly by the vertebral column and aorta. In this view, the appliance ofthe crura to a number of centimeters of terminal thoracic aorta above the aortic hiatus can be appreciated. The inferior vena caval aperture is essentially the most cephalad and lies at the junction of the middle and Right phrenic n. The motor innervation to the diaphragm is by way of the phrenic nerves, which also cany sensory fibers. The right phrenic nerve sends a department to the cephalad surface of the diaphragm and then penetiates the best leaf ofthe centml tendon simply lateral to the vena caval orifice. Viewed from behind, the enfolding of the aorta by the diaphragmatic crura is clear, as is its anterior-posterior proximity to the lower esophagus. The surest approach to determine the esophageal hiatus on belly exploration is to locate the pulsations of the aorta transmitted by way of the esophageal walls. The aortic passage posterior to the diaphragm lies between the median arcuate ligament connecting the crura anteriorly and the physique of the T12 vertebra posteriorly. The origin of the thoracic duct from the cisterna chyli lies to the best ofthe aorta and passes beneath the best crus. The supraceliac aorta consists of the portion between the celiac arteiy and the mediastinum. The juxtarenal space is the portion within 1 em above and beneath the renal arteries that regularly overlaps with the visce:ral section. Exposure of the supraceliac aorta could also be completed utilizing transabdominal or retroperitoneal approaches. This strategy has been used in the elective therapy of aortic illnesses of every kind and seems to confer necessary physiologic advantages compared with transperitoneal exposures. A longitudinal incision is nwle within the belly midline from the xiphoid course of to the umbilicus. Increased exposure may be gained by dividing the left triangular ligament ofthe liver. Care must be taken to keep away from injuring a changed or accent (50:50) left hepatic artery, arising from the left gastric in 10% to 15% of individuals. Retraction of the esophagus and stomach to the left exposes the best crus of the diaphragm, which lies beneath the posterior peritoneum of the lesser sac. The aorta is uncovered by incising the posterior peritoneum and separating the 2 limbs of the right crus to create a 5-cm opening over the anterior aortic wall. It is commonly necessary to divide venous and arterial branches that cross this area, but care ought to be taken to keep away from transecting a changed left hepatic artery (see above). A: the torso is twilrkd such that the pelvis lies horizontally and the left shoulder is rotated 900 from the working desk. B: the desk is jackknifed to widen the area between the costal margin and pelvic brim. To expose the visceral aorta on its anterolateral surface, the kidney must be mobilized anteriorly, allowing the ureter to be swept in to the medial wound along with the. This is accomplished by opening the anterior renal fascia and growing a plane posterior to the kidney. A massive lumbar department tethering the left renal vein on the lateral floor of the aorta should be fastidiously ligated and divided during this maneuver. Exposure is improved by inserting deep blades of a self-retaining retractor to hold the kidney and peritoneum anteriorly. Vascular control of the aorta must be accomplished by confining dissection to the anterior and posterior surfaces; circumferential control dangers injwy to the vena cava or different giant venous constructions. In addition to restoration of intravascular volume, all patients ought to bear optimization of cardiac and pulmonary parameters. Use of a double-lumen endotracheal tube enhances exposure of the thoracic aorta in the course of the procedure by allowing the left lung to collapse whereas maintaining adequate proper lung air flow. The left scapula is elevated approximately 60" away from the working table so that the trunk is twisted. The most generally used classification of thoracoabdominal aneurysms was originally proposed by Crawford et al. A Crawford type I aneurysm begins just distal to the left subclavian a:rteiy and extends to the viscetal aorta above the renal arteries. The incision ought to be prolonged to the belly midline to expose thoracoabdominal aneurysms involving the visceral aorta. C: An prolonged belly incision is required for anewysms extending to the infi:arenal aorta. More distal publicity may be gained by continuing the belly incision in the midline to the level of the symphysis pubis. The stomach incision is deepened by way of subcutaneous tissue, the exterior belly indirect aponeurosis, and the anterior rectus sheath. The external abdominal indirect muscle is break up in the direction of its fibers, and the underlying inner indirect and transversus abdominus muscle tissue are divided between the costal margin and lateral edge of the rectus sheath. The transperitoneal strategy could additionally be most popular in circumstances in which visceral artery revascularization is planned, especially bypasses to the right renal artery. The extraperitoneal strategy proceeds by growing the aircraft between transversalis fascia and parietal peritoneum. The peritoneum is separated from the lateral and posterior stomach walls and then from the diaphragm superiorly. Some su:rgeons carry out the incision radially,28 whereas others29 favor partial or complete division ofthe diaphragm in a circumferential fashion roughly 3 em from the inner costal margin to avoid slicing main branches of the phrenic nerve. This advantage might show extremely essential as a end result of ventilatory failure is likely considered one of the most typical complications of thoracoabdominal incisions. However, advocates of the radial incision method have famous that circumferential division is cumbersome, tough to shut, and related to equivalent results. The anterior renal fascia is opened, and the airplane posterior to the left kidney is developed. The left kidney is mobilized anteriorly together with the adrenal gland, spleen, and pancreas. The large lumbar blanch of the left renal vein must be ligated and divided during this maneuver. The left ureter ought to be identified and reflected with the mobilized retroperitoneal tissue. As the peritoneum is faraway from the undersurface of the diaphragm, the pancreas is reflected anteromedially together with the peritoneal contents.
Syndromes
- Methadone: 2 to 3 days
- Weakness
- Are you a runner? If so, how far and how often do you run?
- Oral thrush ("yeast infection")
- Losing interest in things you previously enjoyed, flat mood
- Cardiomyopathy - ischemic
- Concussion
- Increased risk for infection after splenectomy (post-splenectomy sepsis or other infections -- children are at higher risk than adults for infection)
Purchase torsemide 10 mg with visa
The radial nerve is recognized in the latter method because it passes through the lateral intermuscular septum from posterior to anterior arrhythmia types ecg torsemide 10 mg discount on line. The lateral or Kocher approach to the elbow is often used for so much of procedures on the lateral facet of the elbow hypertension reading chart buy 10 mg torsemide with amex, corresponding to fracture fixation (radial head, capitellum), radial head replacement, and lateral collateral ligament restore or reconstruction. The strategy utilizes the internervous airplane between the extensor carpi ulnaris (posterior interosseous nerve) anteriorly and the anconeus (radial nerve) posteriorly. The posterior interosseous nerve can be protected by preserving the forearm pronated, and the radial nerve is averted by not straying too far proximally or anteriorly. Posterior approaches to the elbow can involve mobilization of the triceps tendon or leave the triceps intact. This approach reflects the olecranon and triceps insertion proximally to expose the distal humerus and elbow joint. Outstanding exposure of the joint is achieved, and the strategy is especially helpful in fixation of complex, intra-articular distal humerus fractures and complete elbow arthroplasty. The Bryan-Morrey posterior approach is an alternative choice to olecranon osteotomy and involves reflection of the extensor mechanism laterally, including the triceps and anconeus. The anteromedial portal is made approximately 2 cm proximal to the medial epicondyle and anterior to the intermuscular septum. The ulnar nerve and medial antebrachial cutaneous nerve are at risk with this portal. The anterolateral portal is similarly made on the lateral facet of the elbow, taking care to keep anterior to the humerus. The posterocentral and posterolateral portals are mostly employed to visualize the posterior compartment of the elbow. Finally, the direct lateral "gentle spot" portal is made on the "delicate spot" on the lateral facet of the elbow to help with visualization and instrumentation within the lateral gutter, corresponding to when working on a capitellar osteochondritis dissecans. The medial floor of the distal extremity of the radius can be concave and articular. Dorsally, the distal part of the radius reveals its tubercle and is otherwise somewhat ridged and grooved for the passage of the tendons of the forearm extensor muscles. The distal radius and ulna have a wealthy vascular supply coming from the radial, ulnar, anterior interosseous, and posterior interosseous arteries. The vessels that offer the dorsum of the distal radius may be described for the corresponding extensor tendon compartments as either intercompartmental or compartmental. Nutrient vessels branch off the main vessels and penetrate the retinaculum and underlying bone. A department off the radial artery, it offers nutrient branches to the bone between the first and second extensor tendon compartments. Clinically, the vessel and its corresponding branches and underlying bone may be harvested and utilized for vascularized bone grafting procedures within the carpus (for instance, for a scaphoid nonunion with avascular proximal pole). Ossification begins in the distal extremity of the radius at the finish of the first 12 months, and fusion takes place at age 19 to 20. An ossification middle for the distal end of the ulna seems at age 5 or 6 and fuses with the shaft at age 18 to 20. Carpal articular floor the skeleton of the wrist consists of eight small bones organized in two rows, proximal and distal. The bones of the proximal row, from the radial to the ulnar side, are the scaphoid, the lunate, the triquetrum, and the pisiform. Those of the distal row, in the identical order, are the trapezium, the trapezoid, the capitate, and the hamate. Their dorsal and palmar surfaces are nonarticular and supply for the attachment of the dorsal and palmar ligaments that maintain them closely together. The other surfaces are articular, aside from the subcutaneous surfaces of the bones that type the borders of the wrist. The proximal articular surfaces are typically convex; the distal surfaces are often concave. Foramina for the entrance of blood vessels are found on nonarticular areas of every bone. The clean distal floor is triangular however concave and receives each the trapezium and the trapezoid. The lunate is crescentic; its proximal convexity is for the extra medial of the articular surfaces of the distal end of the radius. The distal floor is deeply concave for the capitate and for a small contact with the hamate. On its radial floor, this bone contacts the scaphoid; medially, it has a surface for the bottom of the triquetrum. The triquetrum is pyramidal, with the base of the pyramid towards the lunate and the apex downward and ulnarward on the ulnar border of the wrist. The inferior surface is sinuously curved for articulation with the hamate, and the palmar floor has an oval side for the pisiform. The pisiform could additionally be thought to be a sesamoid formed in the tendon of the flexor carpi ulnaris muscle. Its proximomedial floor is concave for articulation with the scaphoid, and its distal floor has Trapezoid Trapezium Radial styloid process Scaphoid Dorsal tubercle of radius (Lister) Radius Triquetrum Lunate Ulnar styloid course of Ulna a saddle-shaped side for the base of the primary metacarpal. On the palmar surface of the bone is a tubercle and a deep groove, via which passes the tendon of the flexor carpi radialis muscle. The tubercle provides attachment to the superficial lamina of the flexor retinaculum and to a number of thumb muscular tissues. The medial floor of the trapezium has a large concave facet proximally for articulation with the trapezoid and has a small, flat oval floor on the distal angle of the bone for the second metacarpal. The trapezoid is somewhat wedge formed, with the broader base of the wedge dorsally. The lateral floor is convex for the trapezium, whereas the medial surface has a smooth facet for the capitate. The capitate is the most important of the carpal bones and occupies the center of the wrist. The distal, considerably cuboidal extremity articulates mainly with the base of the third metacarpal, but by means of small lateral and medial facets it also makes contact with the bases of the second and third metacarpals. The lateral floor has, distally, a small, smooth facet for the distal extremity of the trapezoid, and the medial surface has an rectangular articular surface for the hamate. The hamate is wedge shaped and has a characteristic hooklike process, the hamulus, or hook. The apical proximal part of the wedge articulates with the lunate; the broad distal surface has two concave sides for the bases of the fourth and fifth metacarpals. Articular surfaces laterally and medially are for the capitate and triquetrum, respectively. It begins first within the capitate and then within the hamate early in the 1st year; within the triquetrum, during the third 12 months; in the lunate, in the 4th year; within the trapezium, trapezoid, and scaphoid, in rather shut sequence, in the 4th to sixth years; and in the pisiform, in the eleventh or twelfth 12 months. Ossification starts earlier within the feminine and is completed between ages 14 and 16. An os centrale, usually part of the scaphoid, may be present between the scaphoid, capitate, and trapezoid.

Buy torsemide 20 mg with visa
Antibiotics never used in being pregnant: Aminoglycosides blood pressure levels women torsemide 10 mg buy discount, erythromycin estolate arrhythmia generator torsemide 10 mg amex, clarithromycin, quinolones and tetracyclines. It can be used in severe staphylococcal infections (bone and joint) together with another anti-staphylococcal antibiotic. Spectrum: They are given for severe Gram-negative and staphylococcal infections especially hospital acquired an infection together with E. Common unwanted effects: Isoniazid: Hepatitis (age-dependent), peripheral neuritis (use vitamin B6). Rifampicin: Proteinuria, hepatitis, flu-like syndrome, thrombocytopenia, red-orange metabolites. Anaphylaxis with antimicrobial agents is an unusual occasion that happens in about 1 in 100,000 treatments. Metabolic bone marrow melancholy can occur with zidovudine, ganciclovir and sulphonamides. Hepatocellular damage (hepatitis) is most frequently seen with rifampicin and isoniazid (5% cases). Granulomatous hepatitis although uncommon can happen with highdose ampicillin and flucloxacillin and prolonged quinine remedy. With antibiotics diarrhea can be caused by the alteration of colonic flora and over development of Clostridium difficile. It is used in the after care of tympanomastoid surgery and keeps the cavity clear and dry. Staphylococci are differentiated from streptococci by catalase take a look at with hydrogen peroxide. The large number of M-protein sorts and nonimmunogenic capsule of hyaluronic acid ends in repeated Strep. Drugs that can cross blood-brain barrier also can seem within the milk of lactating mother and will affect the infant. Candida opportunistic pathogen may cause acute or continual deep seated infection of mucosa in debilitated or immunocompromised sufferers. Otomycosis: this superficial, diffuse, fungal infection of external ear canal is described in chapter Diseases of External Ear. In temperate areas Candida is extra widespread while in tropical and subtropical regions Aspergillus niger is commonest. It is frequent in heat and humid environment and in adult sufferers with seborrheic dermatitis, psoriasis and prolonged use of antibiotic steroid drops. Rhinosporidium seeberi, in tissue types massive, thick-walled sporangium-like constructions containing many endospores. Noninvasive fungal sinusitis: this chronic noninvasive fungal infection (sinus ball or sinus mycetoma) is described in chapter Nasal Manifestation of Systemic Diseases. Allergic fungal sinusitis: this frequent reason for persistent rhinosinusitis is described in chapter Nasal Manifestation of Systemic Diseases. Polyenes: They bind to the sterols of fungal cell membranes and end in leakage of cell content material. Nystatin: It is used topically for yeast an infection similar to otomycosis and candidiasis. Clotrimazole: Topical clotrimazole is powerful against oral, vaginal and pores and skin candidiasis and dermatophytes infections. Fluconazole: It covers Candida sp and Cryptococcus and has no exercise against invasive moulds. Itraconazole and voriconazole: They have higher exercise in opposition to invasive fungi together with Aspergillus and Fusarium. It is used in severely energetic Candida sp and Cryptococcus sp solely and in addition utilized in severe infections like meningitis. Terbinafine): They inhibit ergosterol synthesis and used in extensive pores and skin and nail dermatophytes infection. Diagnosis Viral pathogens may be recognized with the help of following methods: 1. Tissue culture: Nasopharyngeal secretions are most popular for inoculation in sufferers with respiratory tract infections. Primary oral disease presents with sore throat, pharyngitis, fever and painful vesicles on oropharynx and oral cavity, which persists for a quantity of days. Recurrent labial herpes: Initial itching, burning, tingling and pain last between 6 hours to 2 days. Interferon: this naturally occurring therapeutic agent is much less efficient and unwanted effects restrict its use. Influenza neuraminidase inhibitors: They block the virus launch, by inhibiting neuraminidase that forestalls the clumping of viruses and their binding to the surface of cells which have been already contaminated. Oseltamivir: It is efficient, secure and well tolerated and is the primary line of antiviral in influenza. Majority of those who died had some underlying ailments and reported late to the identified well being care facility. On 3rd August 2009, India registered its first swine flu death when a 14-year old girl grew to become victim to this disease. Epidemiology Causative organism: Genetic sequencing reveals a brand new subtype of influenza A (H1N1) virus with segments from 4 influenza viruses: North American Swine North American Avian Human Influenza Eurasian Swine Transmission: the transmission is by droplet an infection and fomites. People could turn out to be infected by touching a floor or object- with flu viruses on it after which touching their mouth, nostril, or eyes. Children or folks with weakened immune techniques could unfold the virus for a longer interval. Course: the vast majority of H1N1 flu sufferers recovered with none medical therapy but hospitalizations and deaths have occurred. Clinicians ought to expect problems to be much like seasonal influenza: sinusitis, otitis media, croup, pneumonia, bronchiolitis, status asthamaticus, myocarditis, pericarditis, myositis, rhabdomyolysis, encephalitis, seizures, poisonous shock syndrome and secondary bacterial pneumonia with or without sepsis. Individuals at extremes of age and with preexisting medical situations are at larger danger of problems and exacerbation of the underlying conditions. Extrapulmonary: Myositis, rhabdomyolysis, myocarditis, encephalitis and transverse myelitis. Emergency warning signs: the signal and signs proven in Table 3 point out that sufferers need emergency medical care. The sample must be collected by a skilled physician/microbiologist ideally before administration of the antiviral drug. Treatment Guiding ideas of remedy embody: Early implementation of an infection control precautions to reduce nosocomial/household unfold of illness. Equipment: Portable X-ray machine, ventilators, large oxygen cylinders, pulse oxymeter. Standard operating procedures: Reinforce normal infection management precautions: All those coming into the room should use high effectivity masks, robes, goggles, gloves, cap and shoe cowl. Dispose waste properly by inserting it in sealed impermeable bags labeled as Bio-Hazard. If patients have elevated issue breathing, they should stop Relenza and get medical attention instantly.
Torsemide 20 mg order on line
Pyriform sinus (Fossa): Each pyriform fossa prehypertension remedies cheap torsemide 20 mg otc, which lies on either side of the larynx hypertension 20 year old male torsemide 10 mg discount online, varieties the lateral channel for meals. Communications Superior: It is steady with oropharynx at the level of hyoid bone. Anterior: It communicates with larynx through the laryngeal inlet, which is bounded by the epiglottis, aryepiglottic folds and arytenoids. Postcricoid area: Parapharyngeal nodes and nodes of supraclavicular and paratracheal chain. Upper and center jugular nodes are commonly affected however retropharyngeal, paratracheal, paraesophageal, and parapharyngeal area nodes may also be concerned esophagus inclines to the left from its origin to thoracic inlet. Thoracic esophagus additionally inclines to the left from T7 to the esophageal opening within the diaphragm. Constrictions Esophagus shows four regular constrictions, which could be seen in esophagogram in addition to throughout esophagoscopy. These constrictions, the place foreign our bodies can be held up, are on the following levels: Pharyngoesophageal junction (C6)-15 cm from the upper incisors. The muscle fibers are striated in upper third, easy in the decrease third and each striated and easy in the middle third of esophagus. It is located at decrease portion of esophagus just above the esophagogastric junction. It opens in response to main peristalsis and vomiting and permits air to escape from the abdomen. Bolus of meals is taken in to the stomach with the peristaltic waves and then gastroesophageal sphincter closes. Oral phase: the food is chewed, lubricated and converted in to a bolus, which is then propelled in to the pharynx. There occurs momentary cessation of respiration and rising of larynx beneath the bottom of tongue. Esophageal phase: Once the meals enters in to the esophagus, cricopharyngeal sphincter closes and first peristalsis of w Section 1 Pharyngeal arches. Muscles: Intrinsic and extrinsic muscles of tongue develop Section 1 w Clinical highlights 1. Philtrum: Vertical midline sulcus of higher lip extending from nasal columella to vermilion border. Structures passing between superior and center constrictors: Glossopharyngeal nerve and stylopharyngeus muscle. Types: Hyaline: Thyroid, cricoid and most of the arytenoid cartilage (except its tip) are hyaline cartilages, which endure 62 fig. Cricoid: this ring shaped cartilage has narrow anterior arch and expanded posterior lamina, over which articulate arytenoids. Epiglottis: this leaf-like, yellow, elastic cartilage forms anterior wall of laryngeal inlet. Parts: the anterior surface of epiglottis is attached to body of hyoid bone by hyoepiglottic ligament that divides epiglottis in to two elements suprahyoid and infrahyoid. Arytenoid cartilages: the pyramidal form arytenoid cartilage has the following parts: Base: It articulates with cricoid cartilage. Section 1 w basic Sciences JointS Cricoarytenoid joint: this synovial joint is shaped between the bottom of arytenoid and a aspect on the higher border of cricoid lamina. Thyrohyoid membrane: this membrane, which is pierced by neurovascular bundle of superior laryngeal vessels and internal laryngeal nerve, connects thyroid cartilage to hyoid bone. Hyoepiglottic ligament: It connects the epiglottic cartilage to the body of hyoid bone. Subglottic international our bodies sometimes get impacted in the region of conus elasticus. Cricothyroid membrane: the anterior part of conus elasticus is thick and types cricothyroid membrane, which connects thyroid cartilage to cricoid cartilage. Its free decrease border varieties the vestibular ligament, which lies within the vestibular fold (false cord). Mucous glands are plentiful on the epiglottis, posterior a part of the aryepiglottic folds and within the saccule. Saccule: this diverticulum of mucous membrane starts from the anterior a half of ventricle and extends superiorly between vestibular folds and thyroid lamina. Infraglottic: Lymphatics drain in to prelaryngeal (Delphian node) and pretracheal nodes (through cricothyroid membrane) after which to lower deep cervical and mediastinal nodes. Some lymphatics pierce cricotracheal membrane and drain in to lower deep cervical nodes. The vocal cord consists of a vocal ligament (upper edge of cricovocal membrane), which is covered with mucous membrane that has scanty subepithelial connective tissue. Paraglottic area: It communicates with pre-epiglottic area and is bounded by Anterolateral: Thyroid cartilage and cricothyroid membrane. Anterior two-third of glottis is fashioned by membranous vocal cords whereas posterior one-third by vocal Growths invading paraglottic space destroy cricothyroid membrane and current within the neck. Vocal wire tumors involving thyroarytenoid muscle invade paraglottic space and then subglottic and extralaryngeal region. There happen two types of part differences through the phonation (vibrations of the closed vocal folds) vertical and horizontal: Vertical phase difference: Inferior vocal fold edges separate earlier than superior edges and return back in identical order. Horizontal phase difference: the anterior part separates earlier than posterior half and shut in same order. Larynx beneath the vocal cords is supplied by the inner branch of recurrent laryngeal nerve. Further divisions of lung buds type the lung lobes and bronchial tree together with bronchopulmonary segments all the method down to alveolar sacs. It loops around aortic arch and ascends in to the neck in the tracheoesophageal gutter. Right recurrent laryngeal nerve: It arises from the vagus on the degree of subclavian artery and loops around subclavian artery and then ascends within the tracheoesophageal gutter. External laryngeal nerve: It travels in relation with the superior thyroid artery and provides cricothyroid muscle. Arytenoids: They are relatively large and canopy significant posterior part of glottis. DeveLopment the hypobranchial eminence appears in the floor of primitive pharynx between the 2nd, third and 4th branchial arches (Table 2). The subglottis is the narrowest portion of larynx in kids and has the complete cartilaginous ring (cricoid). Vocal cords: They descend to C5 degree and improve in length particularly in males and result in voice changes (Table 3). Vocal folds are adducted and pressure of shifting air causes vibrations of the elastic vocal folds.
Torsemide 20 mg generic visa
Most trendy techniques use nuclear grade alone or in combination with necrosis and/or cell polarization prehypertension the rationale for early drug therapy 10 mg torsemide buy with amex. The solid pattern may present microacini by which cells are polarized round small extra-cellular lumina in a rosettetype arrangement blood pressure zap nerves 20 mg torsemide order with visa. The nuclei are of uniform measurement and have a daily chrom-atin pattern with inconspicuous nucleoli; mitotic figures are rare. Nuclei are pleomorphic, poorly polarized, with irregular contours and distribution, coarse, clumped chromatin and prominent nucleoli. Comedo necrosis, with abundant necrotic particles in duct lumina surrounded by a generally stable proliferation of large pleomorphic tumour cells, is frequently present. Amorphous microcalcifications are widespread and are often associated with necrotic intraluminal debris. A Micropapillary pattern characterised by numerous, typically bulbous epithelial projections in to the duct lumen. The micropapillae lack fibrovascular cores and are composed of uniform cells with rounded, monomorphic nuclei. Multiple adjacent ducts are distended by a sieve-like proliferation of monotonous uniform cells. The multiple spaces within the proliferation are rounded and distributed in an organized fashion. A extremely uniform inhabitants of cells with round nuclei distributed equidistant from one another and polarized around extracellular lumina. Ductal carcinoma in situ 91 a single space with the typical morphological features is sufficient for analysis. Some experts imagine that assessment of nuclear options and necrosis can additionally be applied to grading of the unusual variants. A comparable reduction for any breast most cancers was noticed within the contralateral breast. E Clinging sample with vital nuclear pleomorphism and a variety of other mitotic figures. There have been 4 randomized clinical trials evaluating excision only to excision adopted by radiation remedy 137,589, 600,1550; these studies present that the addition of radiation reduces the risk of native recurrence by approximately 50%. However, a newer report showed that the speed of native recurrence for these patients rose to 15. In one research, adjuvant tamoxifen additional reduced the risk of local recurrence among sufferers treated with breastconserving surgery and radiation remedy 1550. C Micropapillary sample with epithelial projections in to the duct lumen that lack fibrovascular cores. The cells present some variation in nuclear dimension and the nuclei exhibit variably prominent nucleoli. As in different areas of breast pathology, a multidisciplinary dialogue together with imaging findings will serve to guide a sensible scientific strategy. Historically, there has been wide variation within the definition of microinvasive carcinoma of the breast. Some authors have proposed that the definition of microinvasive carcinoma requires extension of the invasive cells past the specialized lobular stroma. However, it may be difficult to ascertain this, and there might be instances in which microinvasive carcinoma is recognized when convincing histological appearances are current, regardless of malignant cells or nests of cells not being clearly past the specialised lobular stroma. Epidemiology Microinvasive carcinoma is infrequent and is usually over-diagnosed. On ultrasonography, a strong hypoechoic mass has been reported in a small sequence 1515. Macroscopy the macroscopic look of microinvasive carcinoma, as with the scientific features, is that of the underlying in situ lesion. Most usually, ill-defined fibrous areas with comedo-type necrosis extruding from the surface are seen on shut inspection of a sliced excision specimen, however in many instances no visible abnormality is clear. Malignant cells are seen throughout the stroma, most frequently in small angulated clusters and less incessantly as single cells. Additional histological options generally seen in affiliation with microinvasive foci are stromal oedema, desmoplasia, and continual inflammatory cells. Care must be taken not to overdiagnose this lesion, particularly in uncertain circumstances. Indeed, subsequent histology review frequently "downgrades" a diagnosis of microinvasion or of lesions suspicious for microinvasion; in one sequence, only 21 of 109 instances (19. The incidence of metastatic disease in axillary lymph nodes in microinvasive carcinoma of the breast is low. Review of the literature for accurate dedication of the frequency of metastatic disease in sentinel lymph-node biopsy is impeded by the different definitions applied for the diagnosis of microinvasive carcinoma in addition to pathological methods for handling and evaluating sentinel lymph nodes 136. Between 0% and 20% of patients with microinvasive carcinoma are reported to have axillary metastasis (mean, 9. However, warning is required in interpretation of those figures as most of these information are from very small collection. For instance, the very best reported frequency (20%) is reported from a series of 15 sufferers 291. Nevertheless, in lots of centres sentinel lymph-node biopsy is undertaken in ladies with microinvasive carcinoma of the breast. However, it appears that, if this restrictive definition is A Differential prognosis the differential prognosis of microinvasive carcinoma contains pure in situ illness and, conversely, frankly invasive breast carcinoma. The size of the primary target should be fastidiously measured with an ocular micrometer to exclude the latter. Immunohistochemistry may be of value in distinguishing microinvasion from its mimics. Stains for keratins may be of specific value in highlighting the microinvasive foci and complement stains for myoepithelial cells. [newline]Particular problem in reaching a correct prognosis may be seen when the patient has undergone earlier needle biopsy (either needlecore or fine-needle aspiration) for pre-operative prognosis, since displacement of benign epithelium (particularly from papillomas) or cells of carcinoma in situ may mimic microinvasion. The presence of granulation tissue and reparative fibrosis, adjacent fats necrosis and haemosiderin deposition, that are often evident after B C. A Two ducts are crammed by ductal carcinoma in situ, whereas small clusters of carcinoma cells invade the stroma (upper left quadrant of the field) admixed with a dense lymphocytic infiltrate. B Higher magnification reveals small invasive cell clusters within stromal areas distributed over a 0. C Immunostaining for actin highlights the vessel partitions, while absence of myoepithelial cells around the tumour cell clusters confirms their invasive nature. Ichihara Definition Intraductal papillomas are benign lesions which are characterized by finger-like fibrovascular cores coated by an epithelial and myoepithelial cell layer. They are broadly divided in to two groups: central (solitary) and peripheral (multiple) 1030. A yellowish-white, broadly lobulated nodule tasks in to a cystically dilated duct from its attachment to the duct wall. Peripheral papilloma: microscopic papilloma Epidemiology In a big cohort of benign breast biopsies (9108 cases), intraductal papillomas were seen in 5. Patients current over a wide age vary, but most circumstances happen between age 30 and 50 years 30,787,1282.