
Tetracycline dosages: 500 mg, 250 mg
Tetracycline packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

500 mg tetracycline cheap fast delivery
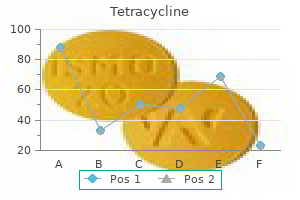
Although very excessive plasma epinephrine levels have been reported after main burn excision antibiotics enterococcus safe tetracycline 250 mg, systemic manifestations are very rare in acute burn sufferers (probably 2� persistent high-level endogenous catecholamine secretion) antibiotics rabbits purchase tetracycline 500 mg visa. In some centers, subcutaneous injection of a diluted (1:1,000,000) epinephrine solution under the burn wound also is used to minimize blood loss; nonetheless, the ensuing vasoconstriction makes the end level of excision -i. Fascial excision includes eradicating the burn eschar and all underlying fat en bloc to the extent of muscle fascia or beyond. Its disadvantages, however, are the marked beauty deformities and useful limitations that occur because of the lack of all delicate tissue overlying the musculature. Because of its disadvantages, fascial excision is reserved for 4th-degree burns or for sufferers with very intensive, lifethreatening, full-thickness (3rd-degree) burns. If eschar excision may be completed earlier than secondary sepsis supervenes, management of the patient is easier and the complications and morbidity are lessened considerably. Adverse effects occurring after 3�4 h of operative time are usually the outcome of large transfusion or hypothermia. Due to loss of pores and skin integrity and huge uncovered surfaces, these sufferers lose heat quickly. All areas not in the operative area must be lined, and a warming blanket (Bair Hugger) is used regularly. Coverage: After excision of wounds and attainment of hemostasis, wounds are coated, using either an autograft or momentary protection with an allograft, xenograft, or synthetic/biologic dressing. An autograft is used for protection when the wound mattress is deemed suitable, a donor site is available, and the patient is secure. Depending on the placement of donor websites, many surgeons use subcutaneous infiltration of diluted (1:1,000,000) epinephrine in saline answer to smooth out irregularities. A substantial quantity of saline may be infiltrated, and this should be added into the whole fluids administered to the affected person. For example, donor pores and skin could also be harvested from the back for software to the chest or abdomen. To defend against this eventuality, grafts are secured with circumferential dressings and splints. This procedure could also be time consuming, and any uncontrolled patient movement ought to be prevented. In this case, temporary protection of the excised wound is accomplished with the application of an allograft, porcine xenograft, or synthetic/biologic dressing. The wound is maintained in this means, with further debridement and biologic dressing changes as essential, until autograft becomes available. This determine demonstrates the connection between dying, increasing age, and burn size. Blood loss and hypothermia are the predominant considerations during surgical procedure on burn patients. Regional techniques are rarely feasible, given the multiple surgical sites for harvesting and grafting. Some surgeons will make use of tumescent infiltration of the burn and donor sites utilizing a big quantity of lidocaineepinephrine-saline answer to facilitate debridement and graft harvest (blood loss + postop pain). Cranial dysostosis is the congenital maldevelopment of the cranial base and/or vault, 2� untimely fusion of cranial sutures. More generally referred to as craniosynostosis, the surgical correction of this disorder involves removal of the affected suture(s) and reconstruction of the cranial, orbital, or facial bones. The most common form of craniosynostosis-scaphocephaly-is caused by the fusion of the sagittal suture, which results in a long and slender calvarium. Other forms of craniosynostosis, so as of reducing frequency, are coronal synostosis (brachycephaly), metopic synostosis (trigonocephaly), and lambdoidal synostosis (posterior plagiocephaly). Deformational occipital plagiocephaly refers to flattening of the occiput 2� preferential sleep place and the resultant deformation of the cranium, ear, and face. Crouzon and Apert syndromes are inherited craniofacial issues related to craniosynostosis and facial/orbital dysmorphism. The facial deformities widespread to Crouzon and Apert are shallow and misplaced orbits, exophthalmos, and midface hypoplasia. In each form of craniosynostosis, sporadic or inherited, the abnormality is current at start, however could not become recognizable till the rapid phase of mind growth, occurring within the 1st yr of life, begins to intensify the restrictions on skull shape produced by the untimely suture closure. In simple phrases, the growth of the underlying brain drives the growth of the cranium, and closure of a suture produces decreased skull development in the other way. Early recognition and correction of craniosynostosis leads to the most effective beauty and neurologic outcome as a outcome of, with launch of the fused suture, the rising mind helps right the irregular cranial form. Most procedures are scheduled in the course of the 1st 6 mo of life; thus, the difficulty of blood quantity and alternative turns into a important issue for surgical and anesthetic consideration. The major rules of surgical treatment of craniosynostosis involve removal of the abnormal suture via a craniectomy or craniotomy, adopted by reconstruction of the calvarium and/or orbit to overcome the cranial deformity and optimize the chance for regular cranial growth. The surgical procedure most often is done along side a pediatric neurosurgeon and a plastic surgeon. Patient positioning varies, relying on the method to the craniectomy, and is mostly prone for sagittal and lambdoidal synostosis and supine for coronal and metopic synostosis. Another surgical precept essential for synostosis surgery is to reduce intraop blood loss. The surgical team ought to make every effort to reduce blood loss in the course of the process by infiltrating the scalp with 1:400,000 epinephrine, using level electrocautery, preserving the pericranium, and fastidiously waxing the bone edges. The most common skin incision is a bicoronal opening that enables for access to the entire calvarium. The extent of the bone elimination and reconstruction varies, relying on the type and variety of sutures concerned. Surgical correction of patients with Crouzon or Apert syndromes is often staged with correction of the cranial part, adopted by a later process for the face, as described by Tessier and colleagues. Invariably, blood loss occurs from the scalp and bone, and the surgeon must stay mindful of the quantity contained throughout the surgical field and readily talk to the anesthesiologist when bleeding is felt to be either steady or excessive. Injury to the underlying dural venous sinuses is uncommon, however the potential for catastrophic blood loss is great. Recent advances in endoscopy have led to the development of minimally invasive techniques for craniosynostosis in some centers, and reviews recommend that use of the endoscope may scale back blood loss. Recombinant erythropoietin administered preop also has been studied in an try to cut back the need for intraop transfusion associated with repair of craniosynostosis. In healthy infants, hematocrit values of 21� 23 are tolerated, reducing the necessity for and amount of blood transfusion. It can range from a minor (endoscopic) to reasonable (strip craniotomy) to main (cranial vault remodeling) surgical procedure. Management of those issues is made more difficult as a outcome of the repair is usually performed in the course of the first 6 months of life. The room and the bed must be kept heat previous to incision because the time from induction to draping may be in depth for line placement. Infants can unexpectedly cool rapidly during this period resulting in coagulopathies. Dahmani S, et al: Perioperative blood salvage during surgical correction of craniosynostosis in infants. This ends in an open neural placode joined to the incomplete epithelial defect, often located within the thoracolumbar backbone, and infrequently within the cervical backbone.
Order tetracycline 500 mg mastercard
Ultrasound Guidance � the patient is positioned within the supine place with the affected limb prolonged and supported and ankle in full dorsiflexion antibiotics for acne and the pill 250 mg tetracycline discount visa. Ultrasound-guided interventional procedures for sufferers with continual pelvic pain � a description of techniques and review of literature antibiotic jock itch order tetracycline 250 mg amex. Treatment of genitofemoral neuralgia after laparoscopic inguinal herniorrhaphy with fluoroscopically guided tack injection. Incidence of genitofemoral nerve block during lumbar sympathetic block: comparison of two lumbar injection websites. Susceptibility of the genitofemoral and lateral femoral cutaneous nerves to problems from lumbar sympathetic blocks: is there a morphological reason Iliopsoas myofascial dysfunction: a treatable reason for "failed" low again syndrome. Anatomic variability of the ilioinguinal and genitofemoral nerve: implications for the treatment of groin pain. Postsurgical pain syndromes: persistent pain after hysterectomy and cesarean section. Ultrasound-guided pulsed radiofrequency ablation of the genital department of the genitofemoral nerve for therapy of intractable orchalgia. Involvement of the lateral femoral cutaneous nerve as source of persistent pain after total hip arthroplasty. Pulsed radiofrequency neuromodulation treatment on the lateral femoral cutaneous nerve for D. Musculoskeletal findings in overweight subjects earlier than and after weight loss following bariatric surgical procedure. In parallel with the current evidence, reproducible pain relieving diagnostic blocks ought to be carried out under fluoroscopy before continuing to radiofrequency neurolysis. This took into consideration the benefits versus risks, methodological quality of supporting proof, and implications (Table 33. It is situated within the pterygopalatine fossa close to the sphenopalatine foramen posterior to the foramen rotundum and anterior to the pterygoid canal. Olfactory bulb Nerve of pterygoid canal Maxillary nerve Nasopalatine nerve Uvula 33 Sphenopalatine Ganglion Blocks 523. This ought to span the world posteriorly from the nostril toward the ear and inferiorly from the zygomatic arch towards the mandible. Intranasal Approach � the benefit of this method is that it might be carried out in an workplace setting. The needle is then advanced till the tip is in the fossa, adjacent to the palatine bone. Day � Using a sterile scalpel, the tip of the sheath is cut obliquely at 45� creating a sheath bevel to expose 2 mm of the spinal needle tip. This is to affirm appropriate distinction flow within the pterygopalatine fossa with no intravascular uptake. Note that the minimize finish of the tubing reaches the proximal finish of the cotton tip of the applicator and the infusion port lies instantly towards the proximal tip of the applicator. Paresthesia at the root of the nostril must be described by the patient at lower than zero. The sphenopalatine ganglion, additionally termed the pterygopalatine ganglion, is a parasympathetic ganglion with a number of connections to common sensory fibers of the top and to the inner carotid plexus without synapses. Reproducible pain-relieving diagnostic blocks should be carried out under fluoroscopy earlier than proceeding to radiofrequency neurolysis. Complications documented embody epistaxis, native or retroorbital hematoma, infection, reflex bradycardia, and transient hypesthesia or anesthesia of the palate or pharynx. Side Effects and Complications � Epistaxis secondary to aggressive placement of a cotton-tipped applicator into the nasal passage or needle penetration of the lateral nasal wall utilizing the infrazygomatic approach. Sphenopalatine endoscopic ganglion block: a revision of a conventional technique for cluster headache. Exposure of the dorsal root ganglion in rats to pulsed radiofrequency currents activates dorsal horn lamina 1 and a pair of neurons. Endoscopic transnasal neurolytic sphenopalatine ganglion block for head and neck most cancers pain. Anatomically and physiologically based pointers for use of the sphenopalatine ganglion block versus the stellate ganglion block to reduce atypical facial pain. Sphenopalatine neuralgia and cluster headache: comparisons, contrasts, and therapy. Sphenopalatine ganglion block for remedy of sinus arrest in postherpetic neuralgia. Sphenopalatine ganglion blockade: a evaluation and proposed modification of the transnasal approach. Long-term relief of posttraumatic headache by sphenopalatine ganglion pulse radiofrequency lesioning: a case report. Unexpected effects due to radiofrequency thermocoagulation of the sphenopalatine ganglion: 2 case reports. Efficacy of sphenopalatine ganglion blockade in sixty six sufferers suffering from cluster headache: a 12- to 70-month follow-up evaluation. Sphenopalatine blocks in the treatment of pain in fibromyalgia and myofascial ache syndrome. Complex regional ache syndrome involving the lower extremity: a report on 2 instances of sphenopalatine ganglion block as a treatment possibility. The effect of intranasal cocaine and lidocaine on nitroglycerin-induced attacks in cluster headache. Sphenopalatine ganglion block: a protected and simple method for the administration of orofacial pain. Does topical anesthesia of the sphenopalatine ganglion with cocaine or lidocaine relieve low back ache Sphenopalatine ganglion block relieves signs of trigeminal neuralgia: a case report. Pulsed radiofrequency V2 therapy and intranasal sphenopalatine ganglion block: a combination remedy for atypical trigeminal neuralgia. In: Essentials of interventional techniques in managing chronic ache: New York, Springer; 2017. Bleeding threat in the interventional ache apply: evaluation, administration, and evaluation of the literature. The historical past of an initiating noxious event similar to trauma generally exists in approximately 10% of the sufferers. Thus, thoracic and cervical sympathetic blocks are two completely different entities, particularly contemplating the stellate ganglion block which only influences nerve fibers that really cross through this structure earlier than reaching the higher extremities. History � the historical past of the description of sympathetic nervous system and sympathetic blocks dates back to Galen [12], who offered one of many earliest historic descriptions of the sympathetic nervous system. Positive sensory abnormalities Spontaneous ache Mechanical hyperalgesia Thermal hyperalgesia Deep somatic hyperalgesia 2. Vascular abnormalities Vasodilatation Vasoconstriction Skin temperature Skin colour changes 3. Clinical use: One or extra symptoms in three or more of the categories and one or more indicators in two or more classes Sensitivity zero.
250 mg tetracycline purchase otc
Endoscopic sinus instruments are used to view the choanae and remove the posterior nasal septum antibiotics for dogs amoxicillin dosage 500 mg tetracycline buy amex. If a transpalatal restore is carried out virus 85 250 mg tetracycline mastercard, a Dingman mouth gag is placed in the mouth, a palatal flap is raised, and the posterior portion of the hard palate and posterior septum is removed. The infant should have the ability to breathe spontaneously via the nose at completion of either process. Unilateral atresia is often asymptomatic; bilateral lesions usually respiratory misery in the neonatal period, however often are asymptomatic. In selected infants, the tracheostomy can be carried out with a inflexible bronchoscope in the airway through which the affected person is being ventilated. A midline horizontal neck incision is made just inferior to the cricoid cartilage. Stay sutures may be placed in the best and left sides of the trachea on either aspect of the incision to facilitate replacement of the tracheotomy tube should it turn into displaced. Alternatively, a formal tracheal stoma could additionally be created by securing the pores and skin flaps on to the trachea. One methodology of formalizing the stoma is a starplasty the place the tracheal incision is made within the form of a "+", the skin incision an "x", and the pores and skin is sutured to the trachea. The ventilation tubing is moved and related to the tracheotomy tube, which is secured with neck sutures and/or ties around the neck. The starplasty has the advantage that in case the tracheotomy tube is dislodged accidentally, it can be pretty easily reinserted, even on the primary postoperative day, offering an extra security factor over the traditional approach. Ostium secundum defects-the commonest (80%)-result from an incompletely formed or fenestrated septum primum overlaying the fossa ovalis. A right anterolateral thoracotomy by way of the 4th intercostal area additionally supplies satisfactory exposure and provides female patients with better cosmesis. Repair is affected by direct suture closure or patch closure, using autologous pericardium or prosthetic material. To achieve this goal, the anesthetic approach should be adjusted to enable for early extubation. Parasternal intercostals block with ropivacaine for postoperative analgesia in pediatric patients undergoing cardiac surgery: a double-blind, randomized, controlled research. Gadhinglajkar S, Sreedhar R, Jayakumar K, Misra M, Ganesh S, Mathew T: Role of intraoperative echocardiography in surgical correction of the superior sinus venous atrial septal defect. Torracca L, Ismeno G, Alfieri O: Totally endoscopic computer-enhanced atrial septal defect closure in six patients. This results in the absence of septal tissue instantly above and under the level of the A-V valves and defects within the A-V valves in continuity with these septal defects. Partial A-V canal defects (or ostium primum atrial septal defects) involve the atrial septum and mitral valve, whereas complete A-V canal defects contain the atrial and ventricular septa and have a typical atrioventricular valve. Intermediate or transitional A-V canal have varying diploma of pathology between the above two frequent patterns. A modified single-patch technique where the A-V valve is plastered all the way down to the ventricular septum is at present utilized by some surgeons. The anterior and posterior bridging leaflets often are divided and resuspended to the patch, thereby creating two separate valves. One of the commonest places is the perimembranous (conoventricular) in the area of membranous septum near the tricuspid and aortic valves. The penetrating bundle is carefully associated to the inferior margin of the conoventricular defect and diverges away from this margin into the trabecular septomarginalis beneath the muscle of Lancisi. Deep hypothermia (18�C) with circulatory arrest is used in neonates < 1800 g to facilitate repair. Early administration of indomethacin may promote ductal closure in plenty of untimely infants, obviating surgical intervention; nonetheless, this mode of therapy usually is contraindicated within the setting of renal insufficiency or intracranial bleeding. The ductus often may be uncovered through a small, left, posterolateral thoracotomy within the 4th intercostal area or via the thoracoscopic method. The ductus is recognized and dissected with special care taken to avoid harm to the phrenic and left recurrent laryngeal nerves. The ductus is interrupted with a surgical clip in neonates; in older children, the ductus is double- or triple-ligated or divided between vascular clamps, and the ends are oversewn. The ductus arteriosus must be open for blood to enter the pulmonary arteries; as the ductus arteriosus closes, pulmonary blood move is lost, and the patient turns into cyanotic. B: Dependence on the ductus arteriosus for perfusion of the distal aorta is shown in a patient with interrupted aortic arch. Variant process or approaches: Percutaneous coil embolization and thoracoscopic clip ligation are commonplace various approaches. These sufferers are intubated, mechanically ventilated, hemodynamically unstable, and will require inotropic help. Ductal runoff causes diastolic blood stress thereby compromising coronary perfusion strain and distal organ perfusion. More just lately, a hybrid approach has been applied in select patients in some centers. In older asymptomatic patients, danger of bacterial endocarditis necessitates closure. If a neuraxial block is contraindicated or not desired, a subcostal or paravertabrel block are affordable alternate options for postop analgesia. Although in small patients, retraction of the left lung could additionally be enough to expose the surgical website. Chaudhary V Chauhan S, Choudhury M, Kiran U, Vasdev S, Talwar S:, Parasternal intercostals block with ropivacaine for postoperative analgesia in pediatric patients present process cardiac surgical procedure: a double-blind, randomized, managed research. Surgical restore of aortic coarctation, first carried out by Crafoord in 1944, consisted of resection of the narrowed aortic phase, adopted by an end-to-end restore. The same year, Blalock and Park proposed another technique in which the left subclavian artery was divided distally and sutured into the descending thoracic aorta, making a bypass. Subsequently, the use of an onlay prosthetic graft to widen the world of coarctation and the usage of a subclavian artery flap have been described by Waldhausen. Prosthetic interposition tube graft repairs have been described in sufferers with diffuse aortic hypoplasia. The lung is retracted anteriorly, and the pleura are incised vertically over the aorta, along the left subclavian artery and the descending aorta. The aortic arch, all of the arch branches, and the descending aorta are thoroughly mobilized. The coarctated phase and all ductal tissue from the descending aorta are excised. An aortotomy is made within the aortic arch (may extend on to the distal ascending aorta), and the descending aorta is anastomosed to the aortic arch.
Purchase 250 mg tetracycline free shipping
The dorsal roots comprise primarily afferent axons which originate from pseudounipolar neurons with cell bodies contained within the dorsal root ganglion antibiotic 6340 tetracycline 250 mg cheap with amex. These pseudounipolar neurons include A-delta and C fiber pain afferents whose peripheral processes advance outward with the peripheral combined nerves and whose central processes synapse with ascending ache afferents within the spinal wire dorsal horn as depicted schematically in infection prevention technologies 500 mg tetracycline order otc. Each dorsal root usually followers out into six or eight rootlets which enter the wire in a vertical row. The first cervical nerve known as the suboccipital nerve and is primarily motor with the dorsal major ramus supplying the suboccipital musculature [6]. The second cervical nerve is a larger combined sensory-motor nerve with a distinguished dorsal root ganglion which lies directly dorsal to the atlantoaxial joint. The medial branch of the dorsal primary ramus of C2 is recognized as the larger occipital nerve, and it courses dorsally and superiorly to provide sensory and motor innervation to the occiput. Occipital neuralgia is a common ache syndrome typically associated with irritation or entrapment of the greater occipital nerve because it pierces the neck extensors. Other causes for continual occipital pain could include damage or arthritis involving the atlanto-occipital, atlantoaxial, and/or upper cervical zygapophysial joints. Since there are seven cervical spinal ranges and eight cervical spinal nerves, the spinal nerve numbering convention is totally different in the cervical region from that in the thoracic and lumbar regions [6]. From C2/C3 to C7/T1, the spinal nerve exiting the foramen is called by the last number of the spinal degree. Numbering modifications at the C7/T1 foramen the place the C8 nerve exits since from T1/T2 and under, the numbering convention is reversed with the exiting nerve named for the first variety of the level. The Spinal Cord and Its Coverings the relatively substantial dura mater surrounds the brain and the spinal twine and accommodates the central nervous system inside a single compartment crammed with cerebrospinal fluid. Cephalad the spinal dura mater is bound to the perimeters of the foramen magnum and to the posterior elements of the C1 and C2 vertebral bodies. The spinal dura is then contiguous with the intracranial dura which continues intracranially to encompass the brain. The dura tapers caudally into the sacrum and ends with the filum terminale at approximately S1/S2. The spinal fluid is created in the third, fourth, and lateral ventricles of the mind by the actions of the highly vascular choroid plexuses. Radioactive tracers injected into the lumbar intrathecal house can typically be detected contained in the skull inside 12 h. The spinal fluid is reabsorbed into the venous circulation via the arachnoid granulations which are located primarily inside the superior sagittal sinus. The whole volume of spinal fluid is approximately 150 mL with one hundred twenty five mL surrounding the brain and 25 mL occupying the intrathecal area. The epidural space extends from the level of C1 right down to the sacral hiatus and encircles the spinal dura in a circumferential method. Schultz Cranial dura Occipital bone Medulla oblongata Spinal wire Epidural area Subarachnoid space T-1 Subarachnoid area Epidural house T-7 Dura T-12 Nerve roots L-2 L-1 Internal filum terminale Filum terminale S-1 S-3 External filum terminale Sacral hiatus dorsally by the ligamentum flavum and ventrally by the posterior longitudinal ligament. Thin fibrous bands could course through the epidural space, binding the dura to the inside walls of the spinal canal. The arachnoid mater lies just beneath the dura and surrounds the brain, spinal cord, and spinal fluid. There is a potential space between the intently apposed dura and arachnoid membranes called the subdural space. This house can sometimes be inadvertently entered with needles or catheters meant for both the epidural or intrathecal areas. Anterior posterior view of lumbar myelogram demonstrating regular nerve root filling. Lateral view of lumbar myelogram demonstrating ventral deformities (white arrows) of the thecal sac on the L3/L4 and L4/L5 levels (b). Lateral view of subarachnoid placement of distinction demonstrating ventral deformities of the thecal sac on the L3/L4 and L4/ L5 levels (d) (Adapted from Botwin [16] and Manchikanti and Singh [17]) actions of local anesthetics injected into the subdural area are intermediate between actions expected for equal doses of native anesthetic injected epidurally or intrathecally, and unintended subdural injection can generally account for excessive sensory-motor block after epidural injection procedures. This is relevant for interpretation of cervical distinction dye patterns when making an attempt to decide whether or not distinction is intrathecal or epidural. A distinction dye unfold sample that stops at the upper aspect of C1 is according to an epidural location, whereas distinction that extends above C1 is likely intrathecal. All rights reserved) 7 Anatomy of the Spine for the Interventionalist 85 Blood Supply to the Spinal Cord the spinal wire receives its blood provide from three longitudinal arteries and a variable number of segmental arteries. The longitudinal arteries embody a single anterior spinal artery and two posterior spinal arteries. The anterior spinal artery is formed from paired branches which exit the bilateral vertebral arteries just previous to their anterior convergence to type the basilar artery. These paired branches course caudally and unite within the anterior midline to kind the only anterior spinal artery. From its origin, it descends anterior to the spinal cord and to the tip of the conus medullaris. The diameter of the anterior spinal artery is biggest within the cervical and decrease thoracic areas and smallest along the mid-thoracic zone from the T3 to the T9 spinal levels. This mid-thoracic area of the wire is taken into account to be the "weak zone" with respect to circulation and is most easily damaged by severe hypotension. The spinal cord receives bilateral segmental arteries, which provide blood to the exiting spinal nerve roots at every degree. These segmental radicular arteries enter the spinal canal by way of the neuroforamina to arborize round and penetrate the parenchyma of the spinal nerve roots and supply blood to each the dorsal and ventral nerve roots. In the cervical region, the segmental radicular arteries might originate from the vertebral arteries or less generally from ascending or deep cervical arteries. In the thoracic area, the segmental arteries originate from the posterior intercostal arteries which department immediately from the aorta, and within the lumbar area, they branch from the assorted lumbar arteries. In addition, the anterior spinal artery is bolstered at numerous ranges by feeder arterial branches from varied arteries including lumbar arteries, intercostal arteries, and vertebral arteries. These segmental arteries are called "segmental anterior medullary arteries" and are essential to the spinal injectionist because they constitute a direct route for delivery of doubtless damaging particulate medicine into the parenchyma of the spinal cord. There is a mean complete of eight anterior medullary feeder arteries (inclusive of all spinal ranges bilaterally), the most important of which is the good anterior medullary artery or artery of Adamkiewicz. The complete variety of anterior medullary feeder arteries varies from 2 to 17 in several individuals, with a mean of three in the cervical region, three in the thoracic region, and two in the lumbar area. The artery of Adamkiewicz sometimes enters the cord on the left side (77% of specimens) anyplace from T7 to L4 (most generally between T9 and T12) and may be the main blood provide to the decrease 2/3 of the spinal cord. In the cervical region, the biggest anterior medullary arteries sometimes enter at C4/C5 or C5/C6 [8]. Since the number and place of segmental medullary spinal feeder arteries is variable and comparatively unpredictable, great care should be taken with any injection into any intervertebral neuroforamen. The foramina most probably to comprise these arteries are in the lower cervical, decrease thoracic, and upper lumbar areas of the backbone, though any intervertebral foramen could include a feeding spinal artery. These arteries usually anastomose with the anterior spinal arteries and supply direct routes for blood circulate into the parenchyma of the spinal wire. Any particulate matter (including particulate steroid) has the potential to occlude the distal arterioles of those spinal finish arteries, creating intensive twine infarction in the downstream spinal tissue. There have been a selection of cases of paralysis and death related to inadvertent injection of particulate steroid into intraforaminal segmental spinal feeding arteries throughout interventional pain procedures [9�13].
Purchase 250 mg tetracycline with amex
Suggested Viewing Links are available on-line to the next movies: Posterior Spinal Instrumentation & Fusion for Idiopathic Scoliosis 02 antibiotic 500 mg tetracycline generic visa. Major trauma mechanisms produce pelvic-ring accidents treatment for vre uti tetracycline 250 mg cheap free shipping, and sufferers with pelvic-ring disruptions incessantly have related systemic injuries, which may be life-threatening. This is along side an exploratory laparotomy performed by a trauma surgeon. These procedures are sometimes lengthy and are staged, requiring adjustments in affected person place. The posterior approach requires a big operative field, which can stop the use of an epidural catheter. The objective of pelvic reconstruction is to restore the anatomy and stability of the pelvis, which will decrease hemorrhage in the hemodynamically unstable affected person, aid in mobilization of the multiply injured patient, and enhance long-term perform. Schematic view of the principal pelvis damage patterns, as decided by the vector of the provocative blow. The pins for the external fixator are inserted into the iliac crest either percutaneously or by way of small incisions. In some centers, this process is done within the emergency division as a lifesaving procedure. The objective of surgical remedy of acetabulum fractures is to protect the hip joint by precisely reconstructing the supporting bony anatomy. Associated injuries to the pelvis are common, as are associated systemic injuries. The most tough portion of the procedure is the reduction; it might be facilitated by neuromuscular leisure, pelvic discount instruments, and traction. A radiograph is also obtained at the end of the case to verify a satisfactory reduction and place of the implants. Patients are anticoagulated within the postop period to stop thromboembolic issues. Weight-bearing restrictions are maintained until enough therapeutic has occurred to allow useful ambulation. Ilioinguinal strategy, right aspect: (i) Penrose drain around iliopsoas, femoral nerve, and lateral femoral cutaneous nerve; (ii) Penrose drain round femoral vessels; (iii) bladder and house of Retzius; (iv) pubis; (v) pubic tubercle; (vi) symphysis pubis; (vii) Penrose drain around spermatic wire. Extended iliofemoral method: (i) Gluteus minimus tendon; (ii) gluteus medius tendon; (iii) gluteus maximus tendon; (iv) superior gluteal neurovascular bundle; (v) sciatic nerve; (vi) piriformis and conjoint tendons; (vii) hip joint capsule; (viii) higher trochanter; (ix) medial femoral circumflex artery overlying quadratus femoris. This situation of the hip produces joint incongruity and instability, finally leading to arthrosis and a dysfunctional hip joint. In children, bone grafting alone could also be enough; in adults, however, pelvic osteotomy, to reorient or broaden the weightbearing surface, is necessary. In sure situations following pelvic osteotomy, incongruity of the hip might persist. In this example, the pelvic osteotomy is mixed with a proximal femoral osteotomy to restore congruence. Pelvic and proximal femoral osteotomies often are fixed internally with screws and plates to permit early mobilization with out displacement. The incision follows the iliac crest from the anterior superior iliac backbone past the convexity of the iliac tubercle; the aponeurosis of the external abdominal musculature is elevated from the iliac crest. A straight vertical incision is made simply lateral to the posterior superior iliac backbone. The origin of the gluteus maximus is elevated from its origin off the posterior ilium and sacrum and reattached laterally. Prevezas N: Evolution of pelvic and acetabular surgery from historical to trendy instances. An anterior, racquet-shaped incision is made, and all muscles crossing the hip joint are incised or detached. The femoral artery, vein, and nerve; obturator vessels; sciatic nerve; and deep vessels are isolated and ligated. The gluteal flap is introduced anteriorly and sewn to the anterior portion of the incision. In a hindquarter amputation, excision of the lower extremity, hip joint, and a portion of the pelvis is carried out. Anterior and posterior incisions are used, the iliac wing is split posteriorly, and the symphysis pubis is disarticulated anteriorly. Either the frequent iliac or exterior iliac vessels are ligated, as are all nerves to the lower extremity. These procedures are carried out very rarely-for extreme trauma, tumor, or infection-and are sometimes lifesaving surgical procedures. They often are carried out along side a common surgeon, and normal bowel prep is done. Usual preop prognosis: Malignant tumor of femur, hip or pelvis; traumatic amputation to femur, hip, or pelvis; uncontrollable an infection to leg, hip, or pelvis. If the patient can be made hemodynamically secure with volume resuscitation, a radical evaluation for coexisting neurological, thoracic, or stomach trauma should be undertaken before anesthesia. Because of enormous intraop blood loss and 3rd-spacing of fluids, invasive hemodynamic monitoring is important. Although epidural anesthesia is seldom sufficient for surgical procedure, postop epidural analgesia is an effective means of controlling the tremendous ache attributable to this type of surgery. Other affected person populations lined in this section embrace in any other case healthy sufferers with congenital or acquired hip dysplasia presenting for augmentation procedures. Regional anesthesia is generally inadequate for major pelvic surgical procedure; however, in elective surgical procedures, serious consideration ought to be given to postop epidural analgesia. Harris T, Davenport R, Hurst T, Jones J: Improving outcome in extreme trauma: trauma techniques and preliminary management: intubation, air flow and resuscitation. The femoral head is dislocated from the acetabulum, and the arthritic femoral head and a portion of the neck are excised. The acetabulum is reamed to accept a cemented or cementless cup manufactured from metal and plastic. The femoral stem and head are normally modular, allowing for quite a few shapes, sizes, lengths, etc. A hybrid complete hip combines a cemented femoral stem and a cementless acetabular cup. After relocation of the new prosthetic hip joint and closure of the tissues, the patient could also be given an abduction pillow to decrease the risk of dislocation. Revision procedures are extra arduous and time consuming, as the "failed" or unfastened component(s) must be eliminated and the bone prepared to accept new cemented or cementless components. These procedures require extra specialised tools for extracting prostheses and cement and rebuilding the femoral or acetabular bone stock (allografts, autografts, etc. In the Girdlestone process (resection arthroplasty), the components are eliminated, but not changed. Sugano N: Computer-assisted orthopaedic surgery and robotic surgical procedure in complete hip arthroplasty.
Buy cheap tetracycline 500 mg line
Use of a probe with a 7 mm lively tip will enable the cannula to stay anchored to the bone whereas nonetheless lesioning the ganglion infection from bug bite 500 mg tetracycline order visa. If symptoms are primarily in the hand virus jc tetracycline 500 mg purchase otc, contemplate T2�T3 thoracic sympathetic lesioning. Neurolytic Procedures � If good but only temporary reduction occurs with a stellate ganglion block or thoracic sympathetic block, a chemical neurolytic block may be appropriate. Injection to both vessel might result in catastrophic strokes, seizure, demise, or bleeding with neural or airway compromise. Secondary emotions of "a full throat" after the injection are common unwanted aspect effects and are usually self-limited. All too typically, this block is carried out without the good factor about fluoroscopic imaging, additional enhancing the potential for opposed end result. Considerations to secondary gain, incorrect analysis, inappropriate sickness habits, and psychiatric illness, in addition to anatomical variance, should be thought of. Side Effects and Complications Cervical and thoracic sympathetic ganglion blocks are associated with a number of issues that are divided into technical, infectious, and pharmacological. Thus, these procedures may be associated with injection of steroid into radicular arteries leading to numerous issues. Cervical and thoracic sympathetic blocks are related to multiple problems that are based on technical, infectious, and pharmacological features. Thoracic sympathetic block for the treatment of advanced regional ache syndrome type I: a double-blind randomized controlled research. Efficacy and security of a single intrathecal methylprednisolone bolus in continual complicated regional pain syndrome. Distribution of the sympathetic rami to the brachial plexus: its relation to sympathectomy affecting the higher extremity. Injuries of nerves and their penalties, 1872 (American Academy of Neurology Print Series). The historical past of the description of sympathetic nervous system and sympathetic blocks dates again to Galen as early as 1528. Since then, a quantity of procedural descriptions have been offered for cervical stellate ganglion blocks and thoracic sympathetic ganglion blocks. Anatomical, technical, and clinical variables of stellate ganglion block in comparison with cervical and thoracic sympathetic blocks individually have led to the impressions that stellate ganglion block is probably not the most effective remedy for higher extremity sympathetic block. Thoracic sympathetic blocks have been assessed in one randomized double-blind controlled trial and two uncontrolled studies, displaying efficacy with enchancment in ache reduction at 12-month follow-up, nonetheless, with injection of steroids. Psychological aspects of reflex sympathetic dystrophy: a evaluate of the adult and pediatric literature. Pharmacological approaches to the remedy of continual ache: new ideas and important points. International affiliation for the research of pain: classification of persistent ache: description of continual ache syndromes and definitions of ache phrases. Is nociceptor activation by -1 adrenoceptors the wrongdoer in sympathetically maintained pain The plasticity of cutaneous hyperalgesia during sympathetic ganglionic blockade in sufferers with neuropathic pain. Electrical stimulation of the higher thoracic portion of the sympathetic chain in man. Clinical and neurophysiological observations regarding pathophysiological mechanisms of reflex sympathetic dystrophy. Predisposing psychological components in the growth of reflex sympathetic dystrophy. Etiopathogenesis of reflex sympathetic dystrophy: a evaluate and biopsychosocial speculation. Psychological traits of reflex sympathetic dystrophy versus myofascial pain syndromes. Critical evaluation of controlled medical trials for peripheral neuropathic ache and complicated regional pain syndromes. Complex regional ache syndrome kind I: incidence and risk components in patients with fracture of the distal radius. Complex regional ache syndrome sort I: incidence and prevalence in Olmsted county, a population-based research. Reflex sympathetic dystrophy: a retrospective epidemiological examine of 168 sufferers. Management of complex regional pain syndrome kind I in upper extremity � evaluation of steady stellate ganglion block and steady infraclavicular brachial plexus block: a pilot study. The results of stellate ganglion block with lidocaine and ultrasound in complex regional pain syndrome: a randomized, double blind, placebo managed examine. Analysis of peak magnitude and length of analgesia produced by native anesthetics injected into sympathetic ganglia of complex regional pain syndrome patients. Intravenous regional block is much like sympathetic ganglion block for ache management in patients with complicated regional ache syndrome kind I. Early thoracic sympathetic block improves the remedy effect for higher extremity neuropathic pain. Stellate ganglion block in reflex sympathetic dystrophy: a double-blind crossover examine. Thermographic evaluation of the sympathetic blockade by stellate ganglion block (2) comparison and evaluation A. Comparison of different injectate volumes for stellate ganglion block: an anatomic and radiologic examine. Comparison of the efficacy of a lowvolume stellate ganglion block with a "conventional" method. Radiofrequency lesions of the stellate ganglion in continual pain syndromes: retrospective evaluation of scientific efficacy in 86 patients. Pai, and Laxmaiah Manchikanti 35 Introduction Lumbar sympathetic block is amongst the most typical procedures carried out in managing ache issues of the abdomen and decrease extremity. As prognostic indicators, lumbar sympathetic blocks are helpful in figuring out the candidates and the potential unwanted facet effects of patients for neurolytic or surgical sympathectomy. In addition, lumbar sympathetic interventions are utilized for remedy of varied circumstances. A resurgence of curiosity appeared in the Fifties when Bonica [4] and Arnulf [5] described intimately the importance of lumbar sympathetic blockade, especially in relationship to therapy of S. Considering the incidence of genitofemoral neuritis of 5% to 10% following a neurolytic lumbar sympathetic block, Ohno and Oshita [7] advocated a transdiscal method. A paradiscal, extraforaminal strategy to the lumbar sympathetic block also has been mentioned as a method of avoiding potential problems as properly as attaining the best block [8]. Techniques for neurolysis of the lumbar sympathetic chain appeared after 1924 when Royle [9] tried to modify skeletal muscle tone in sufferers with spastic paralysis.
Buy discount tetracycline 500 mg on-line
Such visceral ache could also be seen with continual benign issues antibiotics for acne resistance 250 mg tetracycline proven, nevertheless antibiotics for uti how long to work cheap tetracycline 500 mg mastercard, more commonly with gastrointestinal malignancies such as hepatic metastasis, an intestinal tract tumor, and pancreatic most cancers. Of all the visceral ache circumstances seen by interventional pain physicians, pancreatic cancer is the commonest which is the fifth leading explanation for cancer-related mortality within the United States [3]. Sympathetic blockade by means of a celiac plexus block or splanchnic nerve blocks or neurolysis has been proven to be an efficient therapy in managing continual visceral pain [1�7, 24]. They included a total of seven randomized managed trials of pain aid from pancreatic cancer by remedy with medical management alone to celiac plexus block with medical administration. Indications � Image-guided celiac plexus blocks or splanchnic nerve blocks with local anesthetic or neurolysis are indicated in persistent and intractable stomach pain caused by [4]: � Chronic pancreatitis � Pancreatic carcinoma � Gastric carcinoma � Esophageal carcinoma � Biliary carcinoma � Liver metastasis � Retroperitoneal lymph node metastasis � Celiac plexus blockade has been reported to be useful in managing extreme nausea and vomiting in patients with pancreatic most cancers. Evidence Base � the evidence for the efficacy and effectiveness of celiac plexus blockade has been determined. Sympathetic trunk Spinal sensory (dorsal root) ganglion Dorsal (posterior) root Thoracic part of spinal wire Intermediolateral cell column Ganglion of sympathetic trunk Spinal nerve to vessels and glands of pores and skin Ventral (anterior) root Meningeal branch to spinal meninges and spinal perivascular Stretch plexuses (usually arises from (distention) spinal nerve) Abdominopelvic (greater, lesser, and least) thoracic splanchnic nerves Pain Vagus nerve (X) White ramus communicans Gray ramus communicans Ganglion of sympathetic trunk Celiac ganglion Ganglion of sympathetic trunk Enteric plexuses of intestine Superior mesenteric ganglion Sympathetic Preganglionic fibers Postganglionic Parasympathetic fibers Preganglionic Postganglionic Afferent fibers. The main sympathetic visceral innervation is as follows: � Celiac plexus/splanchnic nerves: � Innervates visceral: gastrointestinal tract (from distal esophagus to mid-transverse colon), pancreas, abdomen, liver, adrenals, ureters, and belly vessels � Superior hypogastric plexus: � Innervated visceral: descending and sigmoid colon, rectum, vaginal fundus, bladder, prostate, prostatic urethra, testes, seminal vesicles, uterus, and ovaries � Ganglion impar: � Innervates visceral: perineum, distal rectum and anus, distal urethra, vulva, and distal third of vagina the sympathetic innervations of stomach organs arise within the anterolateral horn cells in the spinal twine. Preganglionic fibers from T5 to T12 go away the ventral roots of the spinal cord to join with white rami communicans. Preganglionic nerves from T10 to T11 be a part of together to type the lesser splanchnic nerve and subsequently converge to kind the celiac plexus. The least splanchnic nerve arises from the T12 sympathetic ganglion and courses by way of anteriorly to be a part of the celiac plexus. The celiac plexus is positioned anterior to the aorta at the degree of the L1 vertebral body and anterior to the crura of the diaphragm. Technical Aspects Celiac Plexus Blockade � There have been multiple strategies described (up to 13 approaches) for sympathetic blockade at the level of the celiac plexus [21, 35, 36]. However, the needle tip ought to be positioned cephalad to the celiac artery to achieve a wider unfold of either native anesthetic or a neurolytic answer [38, 39]. The needle is then withdrawn and redirected at a steeper angle (60 levels from midline) so the needle tip is walked off the L1 vertebral physique. The puncture point was outlined because the lateral margin of the L2 upper finish plate underneath 20� indirect angle fluoroscopic view, and the needle was superior to the target as shown in. Splanchnic Nerve Blocks � the splanchnic nerve block is much like the above classic retrocrural approach. The needles, nonetheless, are aimed extra cephalad to the anterolateral margin of the T12 vertebral physique, being careful to hug the vertebral body. Although now not commercially out there, phenol has the benefit of minimal pain on injection. Only one side is needed if the neurolytic solution spreads across the midline, significantly if the tip of the needle is visualized cephalad to the celiac artery [46]. If the neurolytic answer begins to unfold posteriorly toward the nerve roots, the injection ought to be stopped to keep away from damage. Several approaches have been subsequently promoted, including retrocrural, transcrural, and transaortic by way of blind-landmark-derived strategies and fluoroscopic steering. There have also been direct semi-open methods of video-assisted thorascopic radiofrequency ablation and open radiofrequency ablation for persistent ache states. Two widespread techniques are really helpful with fluoroscopic steerage: the transcrural and retrocrural techniques. Following profitable diagnostic injections, neurolytic modalities can be initiated to provide extended efficacy. The use of cutaneous landmarks to perform these procedures is ill-advised in gentle of recent imaging strategies. The efficiency of these strategies are fraught with potential catastrophic problems, even in experienced hands. The complications associated with splanchnic nerve and celiac plexus blockade embrace ache on the injection website, bleeding, infection, trauma to adjoining tissue, and inadvertent injection into unintended tissue or buildings. The most important issues from blockade of the splanchnic nerves and the celiac plexus can be mitigated by use of modern imaging strategies by well-trained physicians. Side Effects and Complications � Side results after celiac plexus block occur secondary to blockade of sympathetic fibers and the unopposed motion of parasympathetic fibers. Side results embody diarrhea, belly cramping, and orthostatic hypotension and are generally transient. There should be a high clinical suspicion for pneumothorax in any patient noting dyspnea throughout post-procedure monitoring. To help avoid such complications, the smallest gauge needles potential must be used. The evidence of effectiveness for reduction of ache in the structures innervated by the splanchnic nerves and celiac plexus following their blockade has been demonstrated. Acknowledgments this e-book chapter is modified and updated from a previous book chapter, "Celiac Plexus and Splanchnic Blockade" by Allen W. Anesthesiology-important advances in clinical medicine: celiac plexus alcohol block for upper abdominal most cancers pain. Nervi splanchnici durch Leitungsanesthesia bei Magenoperationen und anderen Eingriffen in der oberen Bauchule. Acute pancreatitis; an analysis of the classification, symptomatology, analysis and remedy. Management of upper stomach cancer pain: treatment with celiac plexus block with alcohol. Alternative technique of retrocrural strategy during celiac plexus block utilizing a bent tip needle. Single-needle celiac plexus block: is needle tip position important in patients with no regional anatomic distortions A potential randomized comparison of endoscopic ultrasound- and computed tomographyguided celiac plexus block for managing chronic pancreatitis pain. Comparison between celiac plexus block and morphine remedy on quality of life in sufferers with pancreatic most cancers ache. Prospective randomized doubleblind trial of neurolytic coeliac plexus block in patients with pancreatic most cancers. Effect of neurolytic celiac plexus block guided by computerized tomography on pancreatic most cancers ache. Celiac plexus block for therapy of ache associated with pancreatic most cancers: a meta-analysis. An open randomized comparison of clinical effectiveness of protocol pushed opioid analgesia, celiac plexus block or thoracoscopic splanchnicectomy for ache management in patients with pancreatic and different abdominal malignancies. Randomized, double-blind, controlled trial of early endoscopic ultrasound-guided celiac plexus neurolysis to forestall ache progression in patients with newly identified, painful, inoperable pancreatic most cancers. A roentgenographic, anatomic examine of methods and unfold of resolution in sufferers and corpses.
500 mg tetracycline generic otc
Fluoroscopy radiation security for backbone interventional ache procedures in college educating hospitals antibiotic resistance research purchase 500 mg tetracycline otc. Schultz 10 Introduction Placing needles and different instruments of interventional pain administration safely into the body requires advanced tactile skills antibiotic gonorrhea tetracycline 500 mg purchase line, complete knowledge of anatomy, and experience with fluoroscopy [1]. Specialists inside the new specialty of interventional pain management come from various backgrounds together with anesthesiology, radiology and physiatry. Practitioners with an anesthesiology background usually start interventional ache follow with excellent tactile skills honed from years of performing "blind injections" for regional anesthesia however could lack expertise in using fluoroscopic imaging. Those with radiology background could additionally be skilled in using fluoroscopy but may not have developed the learned tactile strategies of regional anesthesia. Physical drugs physicians might have an excellent understanding of anatomy and physical analysis with little experience in regional anesthesia or fluoroscopy. The aspiring interventional pain specialist doctor must develop expertise in regional anesthesia, radiological imaging, and anatomy to be able to turn out to be an effective and secure practitioner. The following step-by-step outline for performing interventional ache procedures relies on the premise that consistency and preparedness in the preinjection routine fosters efficiency, effectiveness, and safety. Set Up the Room Prior to performing injection procedures, the procedure room ought to be thoughtfully set up for optimum effectivity and security. Facilities that provide interventional treatments should have on-site nursing staff skilled in resuscitation techniques and resuscitation tools including a whole crash cart with D. Orient the Fluoroscope Prior to performing the procedure, the practitioner should first orient the fluoroscope. Schultz from a familiar place and viewing an image with comparable orientation each time, the brain will type associations that improve hand-eye coordination and facilitate quick and efficient needle placement. Once the fluoroscope is powered up and its image oriented, the injectionist could begin with the procedure. Position the Patient Positioning the affected person optimally on the procedure table is extremely necessary and may make the difference between success and failure of the process. Most interventional ache procedures are performed with the patient within the susceptible position, though for sure procedures the affected person is positioned supine or lateral. Radiolucent foam bolsters, pillows, wedges, and other assorted positioning aids are available commercially or may be produced from common radiolucent materials. These aids are useful for comfy and secure patient positioning especially when the patient is inclined. For supine and prone positions, the patient ought to be oriented on the desk as straight as possible alongside the long table axis and as flat as attainable in the horizontal aircraft of the table. Rotated or contorted affected person postures will translate into issue with subsequent picture interpretation and should require awkward positioning angles for the C-arm, including pointless complexity to the procedure. After the patient is comfortably positioned on the fluoroscopy desk, the fluoroscopy technician should transfer the fluoroscope up to the desk and orient it into the neutral position over the patient. The neutral place of the fluoroscope is outlined as the place at which all rotation axes are zero. An picture should then be obtained and manipulated on the monitor in order that the highest of the picture on the display represents the cephalad a half of the patient and the left facet of the image represents the left aspect of the patient when the patient is susceptible. This picture orientation ought to remain normal and ought to be checked and reestablished initially of each day and after restarting the machine for any cause. As the injectionist features experience working 10 Needle Manipulation Techniques 127. The fluoroscope base unit should be positioned sq. to the desk at a distance that allows the forward-sliding shaft of the C-arm to move the picture intensifier to the left and right edges of the desk. The numerous angle arms of the C-arm should be aligned with each other and the C-arm should project outward at a 90 degree angle from the bottom unit. As the C-arm is moved during the process, the view on the fluoroscopic monitor will change. Starting with easily identifiable anatomic landmarks viewed with commonplace orientation permits the injectionist to maintain an understanding of the anatomic landmarks as their fluoroscopic appearance adjusts with altering fluoroscopy views. Especially with more advanced procedures in severely degenerative spines, because the procedure progresses and the C-arm is moved into increasingly unfamiliar oblique angles with cephalad or caudad tilt, fluoroscopic anatomy might seem much less acquainted and the injectionist could become disoriented and lose an understanding of the fluoroscopic shadows that were beforehand identified as identified anatomic structures. If these later images in a sequence of photographs have been seen in isolation, the injectionist might not be in a position to identify any relevant anatomic landmarks. Choose the Skin Insertion Point Choosing the proper pores and skin insertion level is amongst the most essential features of successful fluoroscopic injection. The appropriate pores and skin insertion point for any specific procedure should be fastidiously selected so that the needle can be directed to the goal in as straight a line as possible with out obstruction by bony parts between the pores and skin insertion level and the target. Although needles can be steered round bony obstacles to some degree, the more a needle must deviate from a straight line to arrive on the target, the tougher the process turns into. The easiest procedures are these corresponding to an uncomplicated posterior interlaminar lumbar epidural steroid injection the place an unobstructed fluoroscopic view of the target can be obtained readily and the needle can follow a straight line to its destination. During this procedure, the injectionist may be required to advance the needle down a protracted, slender hall extending from the skin insertion level to the target. The needle might should initially move medial from the skin insertion point to find a way to keep away from the ileum at an approximate depth of two, then transfer lateral to keep away from the superior articulating pro- Visualize the Target In order to efficiently advance a needle by way of the pores and skin and right into a pain-generating goal within the body, one ought to first have the power to visualize the trail resulting in the goal with the fluoroscope. The fluoroscope reveals tissues of varying densities which are represented by various shades of gray on the monitor screen. Advance the Needle in Small, Incremental Fashion to the Target Advancing needles in small, incremental steps to specific targets throughout the body is the essence of interventional ache management. The remainder of this chapter describes the varied strategies used for correct, efficient, protected, and humane needle placement. Local Anesthesia Pain aid during interventional procedures is of primary importance. For sure superior procedures such as percutaneous disc decompression or vertebroplasty, intravenous conscious sedation could also be indicated to scale back the ache of the process. Once the needle is superior via the preliminary skin and subcutaneous wheal, the needle stylet may be removed in order that small, incremental doses of local anesthetic could be injected because the needle is superior further. It is typically advisable to advance the needle with the native anesthetic syringe hooked up so as to expedite native anesthetic injection. The poisonous dose of 1% lidocaine with out epinephrine is bigger than 30 cc though far less volume will often present excellent ache relief during a procedure if the lidocaine is injected liberally previous to incremental needle advancements and/or each time the patient begins to experience discomfort. As a degree of reference, an uncomplicated interlaminar lumbar epidural injection in an anxious affected person could require 5 cc of native anesthetic injected from the pores and skin to the ligamentum flavum in order to hold the patient comfortable during needle placement. With transforaminal epidural injections close to infected nerve roots, additional small doses (as low as zero. These small, incremental doses of native anesthetic close to nerve roots normally create little sensory-motor impairment however could dramatically scale back discomfort. The Art of Needle Placement the artwork of safely and precisely putting needles into the physique and directing them to suspected pain-generating targets takes time to develop. Prior to the advent of fluoroscopy in the pain clinic, interventional ache practitioners relied solely on contact with bony landmarks and the tactile really feel of the needle as it traversed various tissues so as to decide needle tip location. This is the standard approach of the anesthesiologist performing regional anesthesia. Schultz improve with expertise and it could take hundreds of procedures before the injectionist is able to respect the subtle differences in really feel among varied tissues. For surgical functions within the operating room, regional anesthesia is profitable without fluoroscopy because large quantities of native anesthetic are used and since the end-point of surgical anesthesia is enough neural blockade previous to surgical incision.