
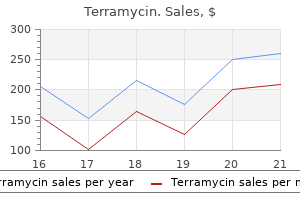
Terramycin dosages: 250 mg
Terramycin packs: 90 pills, 180 pills, 360 pills

Discount terramycin 250 mg with mastercard
Diminished -cell secretory capacity in patients with non-insulin dependent diabetes mellitus antimicrobial journal pdf cheap terramycin 250 mg line. Risk elements for worsening to diabetes in subjects with impaired glucose tolerance antibiotics for uti cost discount 250 mg terramycin amex. Action of -hydroxybutyrate, acetoacetate and palmitate on the insulin launch from the perfused isolated rat pancreas. Opposite results of shortand long-term fatty acid infusion on insulin secretion in healthy topics. Effects of fatty acids and ketone bodies on basal insulin secretion in type 2 diabetes. Long time period publicity of rat pancreatic islets to fatty acids inhibits glucose-induced insulin secretion and biosynthesis via a glucose fatty acid cycle. Prolonged elevation of plasma free fatty acids desensitizes the insulin secretory response to glucose in vivo in rats. Oral glucose augmentation of insulin secretion: interactions of gastric inhibitory polypeptide with ambient glucose and insulin ranges. Glucagon-like peptide-2 stimulates insulin release from isolated fee pancreatic islets. Prior cholecystokinin exposure sensitizes islets of Langerhans to glucose stimulation. Synergistic influence of cholecystokinin and gastric inhibitory polypeptide on the regulation of insulin secretion. Response of truncated glucagon-like peptide-1 and gastric inhibitory polypeptide to glucose ingestion in non-insulin dependent diabetes mellitus: effect of sulfonylurea therapy. Preserved incretin exercise of glucagon-like peptide 1(7-36 amide) but not of synthetic human gastric inhibitory polypeptide in patients with type 2 diabetes mellitus. Reduced gastric inhibitory polypeptide however regular glucagon-like peptide 1 response to oral glucose in postmenopausal girls with impaired glucose tolerance. Gallbladder emptying and cholecystokinin and pancreatic polypeptide responses to a liquid meal in sufferers with diabetes mellitus. Oral glucose ingestion stimulates cholecystokinin launch in normal topics and patients with non-insulin-dependent diabetes mellitus. Glucagonostatic actions and reduction of fasting hyperglycemia by exogenous glucagon-like peptide I(7-36) amide in sort I diabetic sufferers. Glucose-lowering and insulinsensitizing actions of exendin-4: studies in obese diabetic (ob/ob, db/ db) mice, diabetic fatty Zucker rats, and diabetic rhesus monkeys (Macaca mulatta). Additive insulinotropic effects of exogenous artificial human gastric inhibitory polypeptide and glucagon-like peptide-1-(7-36) amide infused at near-physiological insulinotropic hormone and glucose concentrations. Effects of cholecystokinin receptor blockade in circulating concentrations of glucose, insulin, C-peptide, and pancreatic polypeptide after varied meals in healthy human volunteers. Physiological concentrations of cholecystokinin stimulate amino acid-induced insulin launch in people. Effects of secretin, pancreozymin, or gastrin on the response of the endocrine pancreas to administration of glucose or arginine in man. Mechanisms of impaired acute insulin launch in adult onset diabetes: research with isoproterenol and secretin. Starvation diabetes within the rat: onset, recovery and specificity of lowered responsiveness of pancreatic -cells. Inhibitory impact of prednisone on insulin secretion in man: mannequin for duplication of blood glucose concentration. Correlation of hyperprolactinemia with altered plasma insulin and glucagon: similarity to results of late human pregnancy. Lack of management by glucose of ultradian insulin secretory oscillations in impaired glucose tolerance and in non-insulin-dependent diabetes mellitus. Glucagon-like peptide 1 increases mass however not frequency or orderliness of pulsatile insulin secretion. In people no much less than 75% of insulin secretion arises from punctuated insulin secretory bursts. Effects of glucose ingestion versus infusion on pulsatile insulin secretion: the incretin impact is achieved by amplification of insulin secretory burst mass. Impaired pulsatile secretion of insulin in family members of sufferers with non-insulin-dependent diabetes. Estimating false-positive and false-negative errors in analyses of hormonal pulsatility. Quantification of evolution from order to randomness in sensible time sequence analysis. Efficacy of pulsatile versus steady insulin administration on hepatic glucose production and glucose utilization in kind I diabetic people. Effects of extended pulsatile hyperinsulinemia in humans: enhancement of insulin sensitivity. Low- and highfrequency insulin secretion pulses in normal topics and pancreas transplant recipients: function of extrinsic innervation. Insulin secretory profiles and C-peptide clearance kinetics at 6 months and a pair of years after kidneypancreas transplantation. Computer model for mechanisms underlying ultradian oscillations of insulin and glucose. Diurnal variation in oral glucose tolerance: blood sugar and plasma insulin ranges morning, afternoon, and night. Circadian variation of the blood glucose, plasma insulin and human progress hormone ranges in response to an oral glucose load in normal topics. Role of apoptosis in failure of beta-cell mass compensation for insulin resistance and beta-cell defects within the male Zucker diabetic fatty rat. Changes in pancreatic islet glucokinase and hexokinase actions with rising age, obesity, and the onset of diabetes. Quantitative estimation of beta cell sensitivity to glucose within the intact organism: a minimal mannequin of insulin kinetics in the canine. Quantitative study of insulin secretion and clearance in regular and obese subjects. Alterations in the glucose-stimulated insulin secretory dose-response curve and in insulin clearance in nondiabetic insulin-resistant individuals. Insulin sensitivity and B-cell responsiveness to glucose during late pregnancy in lean and 551. Nutrient and hormonal regulation of the threshold of glucose-stimulated insulin secretion in isolated rat pancreases. Human placental lactogen: research of its acute metabolic results and disposition in normal man. Dynamics of insulin launch by perfused rat pancreases: results of hypophysectomy, growth hormone, adrenocorticotropic hormone and hydrocortisone. Vagal regulation of insulin, glucagon, and somatostatin secretion in vitro within the rat. Mechanism of sympathetic neural regulation of insulin, somatostatin, and glucagon secretion.
Syndromes
- Where is it exactly? Is it all over or only in a specific area?
- Muscle pains
- Headache
- Body temperature problems
- Do not expose your child to secondhand smoke.
- The person develops heart failure as a result of damaged heart valves
- Improvement in heart and blood vessel problems, such as high blood pressure
- Low self-esteem
- Surgery to remove small balloon-like tissues (blebs) that cause lung collapse (pneumothorax)
- Chills
Cheap terramycin 250 mg with mastercard
Priorities Consider the diagnosis � Headache is normally frontal treatment for dogs eating chocolate discount 250 mg terramycin with visa, although might take any type bacteria waste terramycin 250 mg discount line. It is primarily caused by stress effects in the pituitary fossa and often induces nausea and vomiting. Haemorrhage and the resultant stress results is most likely not maximal at presentation and repeated examination is essential to detect progressive neurological deficit, the presence of which can set off escalation to emergency neurosurgical intervention. If severe sufficient this may manifest as haemodynamic instability, since the lack of glucocorticoid obtunds the pressor impact of catecholamine signals. Conditions causing broad variations of blood pressure, including major surgery, are incessantly implicated. Other identified danger factors include head trauma, anticoagulant therapy or clotting disorders and being pregnant (especially within the peripartum phase, when pituitary apoplexy is recognized as Sheehan syndrome). Resuscitate the patient In the primary hour of therapy the next goals should be achieved: � Rapid evaluation of airway, breathing, circulation and conscious degree. Images should be linked or downloaded to a suitable digital medium to journey with the patient. Guidelines exist (see further reading), and generally these with a significant neuro-ophthalmic deficit and those with reduced acutely aware degree require surgical decompression and people without may be managed conservatively. However, the choice to proceed both on a conservative or a surgical path have to be taken by an skilled and multidisciplinary staff of endocrinol ogists, neurosurgeons and ophthalmologists. Manipulation of the tumour is likely to trigger a disaster in a patient with out adequate alpha-adrenergic blockade and exclusion of catecholamine extra is critical previous to surgery on any tumour located at a website typical for paragangliomas. Priorities In the affected person presenting with a suspected catecholamine-induced disaster (Table 94. Often secrete catecholamines (adrenaline, noradrenaline, dopamine) however could secrete different hormones as nicely. Caution is required; the circulating quantity could also be considerably reduced as a physiological response to increased vascular resistance. Plasma metanephrine ranges are essentially the most specific of those checks and less prone to the effects of intercurrent illness than ranges of adrenaline or noradrenaline themselves. The overwhelming majority of paragangliomas will secrete one or both of these hormones, pure dopamine-secreting paragangliomas are very uncommon. Functional imaging is also useful as it might identify metastases and/or verify uptake of a tracer by malignant paragangliomas, which can then be utilized in focused radiotherapy ought to this be necessary post-surgery (peptide-receptor radionuclide therapy). This carries a risk of inducing profound hypotension (see above) and is greatest undertaken as an inpatient. This allows for more speedy up-titration of the dose and more accurate fluid alternative as the diploma of alpha blockade will increase. The dose is sequentially increased until normotension is achieved or adverse effects (chiefly nasal congestion and postural hypotension) turn into intolerable. Beta blockade to management tachycardia or tachyarrhythmia may safely be commenced as quickly as adequate alpha blockade is in place. Multidisciplinary management Early involvement of the surgical team to plan surgical procedure is necessary, and administration of paragangliomas is finest under a multidisciplinary group of endocrinologists, endocrine surgeons, radiologists and nuclear drugs physicians. Evidence of neurofibromatosis kind 1 (caf�-au-lait spots, cutaneous neurofibromata), a quantity of endocrine neoplasia type 2A (medullary thyroid cancer, hyperparathyroidism) or kind 2B (as for kind 2A plus Marfanoid habitus, and mucosal ganglioneuromas) and von Hippel Lindau (haemangioblastoma, renal cell cancer, pancreatic islet cell tumours) must be sought. Predisposing components embody earlier episodes of cellulitis, limb oedema and lymphoedema. Streptococcus pyogenes and Staphylococcus aureus are the most typical causative organisms. Erysipelas is an acute bacterial an infection of the higher dermis and epidermis, which can be clinically distinguished from cellulitis by a more clearly demarcated border between contaminated and wholesome pores and skin. Necrotizing fasciitis is a rapidly progressive infection of the deep fascia and muscle, and ought to be suspected in an sick patient with extreme ache and marked local tenderness. The majority of instances are polymicrobial and attributable to anaerobes, Gram- unfavorable bacilli and streptococci (not S. Management requires resuscitation, antibiotic remedy and urgent referral to an orthopaedic or plastic surgeon for consideration of debridement. If cellulitis is the likely analysis, assess the severity of the illness, on the premise of the medical features and comorbidities, and manage the patient accordingly (Tables 95. Full blood count C-reactive protein Electrolytes and creatinine Blood tradition (in class three or 4 sickness (Table 95. Class 1 2 3 Features No important systemic sickness No uncontrolled comorbidities Significant systemic illness or comorbidity. Setting Organisms to be covered in addition to Streptococcus pyogenes and Staphylococcus aureus Not allergic to penicillin Otherwise well Strep. Practice guidelines for the diagnosis and management of skin and gentle tissue infections: 2014 Update by the Infectious Diseases Society of America. The erythrodermic affected person should be managed in a monitored mattress with shut nursing enter. Meticulous fluid balance have to be maintained, bearing in mind insensible losses from the pores and skin. The room should be warm and a Bair-Hugger blanket or equal utilized, to prevent heat loss and preserve core temperature. History Take a full medical and drug historical past, specializing in a personal and household history of underlying pores and skin disease, atopy and new medicines in the previous eight weeks, to embrace topical agents, natural and over-the-counter therapies. Establish the timing of onset of the rash; drug reactions are inclined to evolve quickly, whereas inflammatory skin illness could additionally be extra insidious. Assess for cutaneous symptoms; pores and skin pain may be experienced with drug rashes and unstable psoriasis, itch with atopic dermatitis. Systemic signs should be sought including fever and prodromal flu-like illness. Examination Physiological observations and basic examination Examine the palms and nails Inspect scalp, oral mucosa, natal cleft and genitalia along with the physique skin. Multiple sterile micropustules are seen in erythrodermic psoriasis patients and drug reactions. In chronic erythroderma, ectropion, hair loss and thickening of the skin on the palms and soles is seen. For erythrodermic atopic dermatitis, potent topical steroids and oral steroids could additionally be indicated. It is uncommon, affecting 1�2 persons per million inhabitants per year and related to significant morbidity and mortality. It is a extreme muco-cutaneous response, often drug-induced, characterized by fever, full thickness skin necrosis affecting more than 30% of the physique surface area, erosion or ulceration of at least two mucous membrane sites (ocular, oral, anogenital) and variable systemic organ involvement. History A cautious historical past of comorbidities and detailed drug historical past of the final eight weeks is crucial, together with prescribed, over-the-counter and natural therapies. Muco-cutaneous signs in established illness embody a spectrum of intensive blistering, erosions and haemorrhagic mucositis. Examination Careful pores and skin and mucous membrane examination is required to assess the extent of involved sites. The skin could additionally be friable and denude easily on examination; therefore assistance shall be required to minimize direct handling of the skin throughout examination. Assessment of the proportion body surface space involved should be made, to include erythema (which may take the looks of refined slate gray pigmentation in darker pores and skin types or where full thickness skin necrosis is already established), erosions and bullae.
Terramycin 250 mg purchase amex
Assess and meet the non secular and psychological wants of the affected person and those close to virus 3d project order terramycin 250 mg with visa the affected person bacteria yeast and fungi slides generic terramycin 250 mg online. Symptom Drug Dose for subcutaneous administration 2�5 mg up to 2-hourly 2�5 mg as much as 2-hourly 1�2 mg as a lot as 2-hourly 0. Keep good notes Details of the plan of care, and summaries of conversations with the patient and members of the family must be documented in the medical document. Review the patient the affected person should be seen a minimum of daily; plans ought to be reviewed. After demise the body of the deceased particular person ought to be cared for in accordance with their non secular and cultural beliefs. Failure to obtain consent might open the doctor to a legal cost of assault or battery, or a discovering of misconduct by the regulator. Age and capability the legal age of capability in England, Wales and Northern Ireland is 18 years, when an individual is assumed to be a competent adult able to consenting to or refusing remedy, unless different factors forestall them from making knowledgeable choices. The Family Law Reform Act 1969 made provisions for these aged sixteen and 17 years; asserting the presumption that virtually all of young people had capacity to provide affirmative consent (assent) to investigation or treatment deemed of their finest interests, but that could be overruled in distinctive circumstances. Capacity is time and decision-specific, so someone might lack capacity to make one choice however have the flexibility to make one other. For consent to be valid, three criteria must be met: � the patient should have the psychological capability to make the decision. The Act, which was enacted in October 2007, was largely based on previous widespread regulation and sets down the framework for decision making. It is supported by a Code of Practice and imposes an obligation on health-care professionals to observe that code. The Act sets down the circumstances during which a person perhaps detained and handled for a psychological health situation. Medicolegal points in acute medicine 635 Self-harm A explicit challenge is those patients who present having tried suicide. There is often confusion between the Mental Health Act and Mental Capacity Act (Table 111. If a patient presents with a potential psychiatric condition, they may require remedy for the condition and therefore shut liaison with the psychiatric staff can be advisable. When a hospital identifies that a person who lacks capacity is being disadvantaged of their liberty, they must apply to the local authority for an authorization of deprivation of liberty. The affected person ought to be totally knowledgeable the General Medical Council and the courts count on a affected person to be given enough info to make a decision. However, this person must be suitably trained and have sufficient knowledge about the dangers and advantages, and understand their responsibilities to the affected person. Confidentiality Doctors have an obligation to maintain details about their patients confidential. If consent is refused, or the affected person lacks capability, numerous points need to be considered to determine if disclosure is justified. Public curiosity disclosure might be justified if relevant data could prevent hurt to a third get together or aid the detection, investigation or prosecution of a Medicolegal issues in acute drugs 637 severe crime. Suction � If vomit, secretions, or different debris is current within the oropharynx, these can be eliminated with a wide-bore inflexible Yankauer sucker, to relieve obstruction and stop aspiration. Oropharyngeal airway � In an unconscious affected person, obstruction might occur in an anatomically regular airway owing to loss of muscle tone with collapse on the degree of the soft palate, epiglottis or tongue base. An oropharyngeal (Guedel) airway may restore airway patency sufficiently for spontaneous or bag-mask ventilation. Nasopharyngeal airway � As an different to the oropharyngeal airway, a delicate lubricated tube could also be inserted into the nostril. The system may be inserted upside-down (a) earlier than rotation into final position (b). Familiarize yourself with the particular supraglottic airways available in your cardiac arrest trolleys in advance of needing one. Any degree of impairment of consciousness is related to elevated risk of aspiration pneumonia, though many medical patients on this class might moderately be managed in a closely monitored surroundings with equipment and personnel available to intervene if needed. Endotracheal intubation supplies a definitive airway, allowing mechanical ventilation (with excessive airway pressures if needed) and safety from aspiration, and is due to this fact thought-about a gold normal. The choice to sedate, paralyse and attempt endotracheal intubation with direct laryngoscopy should solely be taken by a clinician with appropriate expertise. Beware false-positive outcomes from preliminary breaths after oesophageal intubation with an insufflated stomach, and false-negative leads to cardiac arrest. It is blindly inserted into the oropharynx and ventilation can be delivered via both of two ports, depending on where the gadget has settled. For management of the affected person with complications referring to an present tracheostomy, and details of emergent surgical airway strategies, see Chapter 59 which discusses the method to the affected person with upper airway obstruction. Time spent with the patient in the first 30 min helps to reassure the patient and prevents future issues. Tighten the straps to type a seal across the face, but not so tight as to squash the membranes of the masks. Consider whether or not the oxygen supply is excessive; oxygen may be added at a flow price of 1�4 L/min, goal arterial oxygen saturation of 88�92%. Do not simply tighten the straps, as this can squash the membranes and improve the danger of nasal bridge ulceration. Persistent hypercapnia, when none of the above applies, is likely to be because of insufficient ventilation. Changes could be made to set off sensitivity, inspiratory and expiratory instances and back-up respiration fee as acceptable. Nasal bridge ulceration Ulceration of the pores and skin of the nasal bridge from a tightly or poorly-fitting mask is a standard drawback. Regular checks of pores and skin integrity must be carried out, in addition to checking for masks leak, as air leaks could cause corneal harm. It can be utilized to information chest drain insertion for people who have approved British Thoracic Society training (Chapter 122). Note that: � Left ventricular wall-motion evaluation may be tough and must be performed by an accredited echocardiographer. Clinical situation Cardiac arrest/peri-arrest/hypotension/shock Pulmonary oedema Breathlessness/hypoxaemia Lower respiratory tract an infection Chest ache Abdominal ache y Cardiac scan + + + + + Thoracic scan (+) + + + (+) Abdominal scan (+)y +y To exclude pressure pneumothorax. Cardiac scan Probe: � Cardiac Positioning: � Left lateral � Supine (subcostal view) Views: � Parasternal long-axis � Parasternal short-axis � Apical four-chamber � Subcostal Uses: Loading conditions Critical pathology in four areas of the guts: � the left ventricle � the proper ventricle � Valve stenosis and regurgitation � Pericardial effusion Thoracic scan Probe: � Cardiac: for B-lines and pleural effusion � Curved: for all functions � Linear: for pleura and detect pneumothorax Positioning: � Seated forward with arms folded on pillow for pleural effusion � Any place for pulmonary oedema � Supine/near-to-supine for pneumothorax Views: � Posterior method for pleural effusion � Anti-dependent zones for pneumothorax (anterior sag gital, second intercostal space, mid-clavicular line) � Dependent zones for cardiogenic pulmonary oedema Uses: � Pleural effusions � Pulmonary oedema (cardiogenic, non-cardiogenic) � Consolidation � Pneumothorax Bladder scan Probe: � Curved Positioning: � Supine with full bladder Views: � Pelvis � sagittal � transverse Uses: � Incomplete voiding � Reduced urine output vs catheter blockage Abdominal scan Probe: � Curved Positioning: � Supine Views: � Central belly � Left lower lateral Uses: � Ascites and paracentesis Ultrasonography in acute medication 653 Table 114. Ultrasound is more correct than a chest X-ray on which lobar collapse and elevated hemidiaphragm could mimic a pleural effusion. Abdominal scan � In a tense distended stomach ultrasound can confirm the presence of ascites immediately. Suggests ascites � Dark and hypo-echoic appearances within the flanks � Loops of gas-filled bowel afloat around the centre/periumbilical region Points of concern before ascitic faucet � Hepatomegaly or enlarged gallbladder � Splenomegaly � Full bladder. A frequent mistake is to insert a needle into the fluid of the bladder, so guarantee several planes of view are evaluated earlier than continuing in real-time. A-lines are regular horizontal reverberation artefacts, and B-lines are pathological vertical reverberation artefacts.
250 mg terramycin buy fast delivery
Fractures are uniquely different in youngsters than adults due to antibiotic resistance obama generic terramycin 250 mg overnight delivery the increased elasticity of the immature skeleton antibiotics join the fight buy 250 mg terramycin. The torus fracture (top right) outcomes with low-energy damage, buckling the cortex. With increasing power, the greenstick fracture (bottom left) could happen, with a cortical break alongside the tension side and plastic deformation on the compression aspect of this fracture. This leads to a symmetric bulge and slight sclerotic band throughout the metaphysis. The fractures may reangulate and ought to be imaged 1-2 weeks after discount and casting. A greenstick distal ulnar diaphysis fracture is seen with a concomitant radius bowing deformity (> 15�). These distal radius and ulna fractures could seem full on a single view, but an orthogonal view confirmed a minimum of 1 space of intact cortex, indicating greenstick fractures. Comparison with the adjacent regular radius highlights the sign abnormality in the ulna. This transverse metaphyseal fracture results in a dorsal angulation of the distal fragment. The distal fragment is dorsally angulated and displaced, making a silverfork deformity. This results in a garden spade deformity with a proximal dorsal deformity and distal indentation. Note the carpals transfer dorsally & proximally with the fracture fragment & are now not aligned with the radial shaft. The shearing harm leads to dorsal displacement of the distal fragment with carpals, maintaining anatomic relationship with the fracture fragment. The intraarticular fracture is located volarly & the fragment is displaced volarly & proximally. An accompanying scapholunate ligament damage leads to widening of the scapholunate interval. This die-punch fracture outcomes from axial loading with the lunate punching into the distal radius on the lunate fossa. Radial shortening & probable scapholunate ligament tear are indicators of poor prognosis. The look suggests rickets, but this pattern can be seen as a persistent Salter-Harris I harm, related to substantial repetitive stress. This fracture extends into the radiocarpal joint however spares the distal radioulnar joint. The carpals stay aligned with the dorsal fragment, just like a Barton fracture. Four K-wires cross the radial styloid & radial shaft, restoring radial top & angulation. There is a 4-mm step-off at the radial articular surface & ulnar optimistic variance has returned. The lunate fossa is impacted with a coronal fracture line separating the dorsal and volar portions and an additional volar fragment, or spike. Note the diffuse edema of the lunate, which impacted ("punched") the distal radius, causing the intraarticular fracture. This tip fracture could outcome from impaction on adjoining carpals or from avulsion of the ulnar collateral ligament complex. Yilmaz S et al: Ulnar styloid fracture has no influence on the result but decreases supination strength after conservative treatment of distal radial fracture. K-wires can be utilized to manipulate and align fragments previous to being positioned via a quantity of fragments for fracture stabilization. Wires cross through the radial styloid and are used to lever the medial fragments into place. The 2nd radius pin was barely bent throughout placement and could also be a degree of failure. The 2 lateral wires have withdrawn, and the 2 medial wires have superior proximally. Apparent interruption in plate is artifactual: this sagittal slice is through the center of a screw gap. The high quality of the image is sweet as a end result of the world of curiosity is distant from the metallic artifact. The development plate develops individually from epiphyseal ossification & is composed of four zones: Growth (chondroblasts divide & columnate), maturation (cells hypertrophy & calcified matrix penetrates between columns), transformation (calcification turns into more organized as metaphyseal vessels penetrate matrix), & remodeling. Poor metaphyseal vessel penetration into the transformation zone limits deposition of calcified matrix between hypertrophied chondroblasts, resulting in a widened, nonmineralized growth plate. This irregular metaphysis is as a outcome of of widening of the hypertrophic zone of the growth plate & might evolve to a extra cystic appearance with continued trauma. These bridges might end in development deformity if significant growth potential stays. Medial radial development plate is prematurely closed, resulting in an ulnar optimistic variance. Note the low signal band paralleling the slightly irregular metaphysis in this athlete who was recovering from a prior progress plate injury. Do not neglect that these athletes are at risk for other injuries which will clinically mimic osteolysis. Though dorsal dislocation is the most common pattern, this affected person sustained a volar dislocation. Despite discount of the distal radius fracture, disruption of the volar radioulnar ligament permits ulnar subluxation. The proximal pole fracture is the least widespread but essentially the most problematic because of its tenuous blood provide. This nondisplaced fracture will heal with out complication as a outcome of the generous blood provide to the distal pole. This fracture happens because the scaphoid is trapped between the capitate and radial styloid while being stabilized by volar ligaments. Fractures on this location tend to isolate the fragment from its key blood supply from the dorsal scaphoid department of the radial artery, putting it at risk for osteonecrosis. Three weeks later, indirect view (right) clearly exhibits the fracture line as a outcome of fracture margin resorption. Absence of edema within the proximal pole, significantly in the setting of an acute injury, is suggestive of ischemia of that fragment, which may result in osteonecrosis. This outcomes when the proximal fragment extends, maintaining its alignment with the lunate, while the distal fragment flexes.
Best terramycin 250 mg
Common Cancer involving bone (carcinoma of breast antibiotic soap purchase 250 mg terramycin amex, bronchus anti bacteria buy 250 mg terramycin free shipping, renal, thyroid, and prostate); haematological cancer, for instance myeloma and lymphoma. Mechanisms: secretion of parathyroid-hormone-related protein; bone metastases; elevated manufacturing of 1,25-dihydroxy vitamin D; ectopic parathyroid hormone manufacturing. Chronic kidney illness with tertiary hyperparathyroidism and treatment with calcium and vitamin D metabolites. Principles of management Treat the underlying disorder: causes of hypercalcaemia are listed in Table 87. Avoid thiazides and lithium carbonate, which contribute to hypercalcaemia and in addition patient immobilization. Moderate or severe hypercalcaemia (total calcium >3 mmol/L) 1 the first-line remedy is rehydration. In sufferers with mild symptoms, oral rehydration (a fluid consumption of no much less than 2�3 L/day) could additionally be enough. The use of furosemide is no longer really helpful within the administration of hypercalcaemia. Acute severe hypocalcaemia (with tetany) is most commonly seen in patients with chronic kidney disease after elective subtotal parathyroidectomy or whole thyroidectomy. Be conscious that hyperventilation can also trigger carpopedal spasm because of reduced ionized calcium, resulting from a respiratory alkalosis. Following parathyroidectomy or whole thyroidectomy Hypoparathyroidism, for instance autoimmune, infiltration, Di George syndrome Acute pancreatitis Severe hypomagnesaemia Vitamin D deficiency, for instance poor intake, malabsorption Chronic kidney disease Cancer (either involving bone, with increased osteoblastic exercise, or in response to chemotherapy, with phosphate launched from tumour cells forming complexes with plasma calcium) Multiple citrated blood transfusions Rhabdomyolysis Septic shock Pseudohypoparathyroidism Hypercalciuric hypocalcaemia Drugs, for example loop diuretics, phenytoin Ethylene glycol poisoning Disorders of plasma calcium focus 517 Acute severe hypocalcaemia, for instance with tetany Give 10 mL of calcium gluconate 10% (2. This could be repeated and, if indicated, followed with infusion of calcium gluconate 10% infusion 40 mL (9 mmol) over 24 h. It is essential to monitor serum calcium concentrations frequently and also exclude and handle concomitant hypomagnesaemia. If hypocalcaemia is more probably to continue, give oral vitamin D with patient follow-up. It can be important in cell membrane perform and can antagonize calcium in cellular responses. Increased consumption of magnesium Certain antacids Milk-alkali syndrome Magnesium-containing purgatives Inappropriate magnesium infusion Reduced renal excretion of magnesium Acute kidney harm Chronic kidney disease Others Familial hypocalciuric hypercalcaemia Lithium remedy Hypothyroidism Adrenal insufficiency Symptomatic extreme hypermagnesaemia Treat the underlying cause. Insulin and glucose infusion can be utilized in severe hypermagnesaemia, as for extreme hyperkalaemia. If renal function is normal, urinary magnesium loss can be elevated by compelled saline diuresis. The manifestations of hypomagnesaemia are very comparable to these of hypocalcaemia (Chapter 87). Hypocalcaemia, hypophosphataemia and hypokalaemia are associated with hypomagnesaemia, and plasma levels of those ions must be checked. Measurement of 24-h urinary magnesium excretion can be helpful in assessing the response to remedy. It acts as a buffer, performs a central role in metabolic processes similar to oxidative phosphorylation and glycolysis, as nicely as nucleotide pathways and nervous system conduction. Pseudohyperphosphataemia may be as a result of phosphate leakage out of cells if the sample is haemolysed or delivery to the laboratory is delayed. Acute phosphate load Endogenous Rhabdomyolysis Tumour lysis syndrome Crush damage Malignant hyperpyrexia Exogenous Phosphate-containing medications (laxatives, fosphenytoin) Intestinal uptake (vitamin D toxicity) Cellular shift Acidosis, for example lactic acidosis or diabetic ketoacidosis Decreased renal clearance Reduced glomerular filtration price Acute kidney damage Chronic kidney disease Increased tubular reabsorption Hypoparathyroidism or pseudohypoparathyroidism Acromegaly Bisphosphonates Vitamin D toxicity (also will increase intestinal absorption) Familial tumoral calcinosis Pseudohyperphosphataemia In vitro haemolysis Delayed sample supply Symptomatic severe hyperphosphataemia Treat the underlying trigger. The major scientific consequence of extreme hyperphosphataemia is hypocalcaemia (Chapter 87). The reason for this is that calcium phosphate precipitation into the tissues occurs when the phosphate and calcium plasma concentrations exceed their solubility product ([calcium] � [phosphate]). Mild to average hyperphosphataemia Treat with oral phosphate-binding agents, for example magnesium hydroxide or calcium carbonate. These may include rhabdomyolysis, impaired skeletal muscle operate, weak point and myopathy, impaired diaphragmatic contractility and issue weaning patients off mechanical ventilators and cardiomyopathy. Severe hypophosphataemia can provoke seizures, paraesthesiae, and renal tubular impairment and osteomalacia. Give oral phosphate (although gastrointestinal side-effects similar to diarrhoea is usually a downside and phosphate correction could additionally be delayed), for instance Phosphate-Sandoz one pill (containing phosphate 524 Acute Medicine 16. Acute adrenal insufficiency mostly occurs as an acute exacerbation of an underlying chronic or subacute insufficiency, triggered by concomitant illness such as an infection. Priorities In the patient presenting with acute circulatory collapse and suspected adrenal insufficiency (Tables 90. Hyperpigmentation is finest seen over the palmar creases, knuckles, old scars and the oral mucosa. The commonest explanation for permanent secondary adrenal insufficiency is a pituitary tumour and consequent treatment, with adequate damage to pituitary operate to end in hypopituitarism. In a critically unwell affected person, a degree of <500 nmol/L is suspicious for insufficiency. Further administration Steroid alternative � If unsure, hydrocortisone substitute should continue till adrenal sufficiency may be conclusively confirmed or excluded. Making the patient safe for discharge � Educating the patient on what to do within the presence of acute illness is of paramount significance and may be a life-saving intervention. Confirming the diagnosis When nicely, definitive determination of adrenal standing may be sought. Determining the cause � If primary adrenal insufficiency is confirmed, further investigations are required to elucidate the aetiology. The presence of adrenal autoantibodies suggests an autoimmune process that may be a part of a polyglandular syndrome, and medical options of different related conditions should be sought (Table ninety. If secondary adrenal insufficiency is recognized, a radical seek for a history of exogenous steroid is the first step. Inhaled and topical steroids can be absorbed systemically in sufficient quantities to end in adrenal Acute adrenal insufficiency 529 Table 90. Oestrogens, for instance in oral contraceptives, must be stopped six weeks before the take a look at. Measure plasma cortisol immediately before, and 30 and 60 min after the injection. However, in secondary hypoadrenalism which is gentle or of current onset, the test may be regular. Emergency management of acute adrenal insufficiency (adrenal crisis) in grownup sufferers. Thyrotoxic storm is an acute life-threatening metabolic emergency brought on by extremely excessive levels of thyroid hormone activity. If the diagnosis is suspected, antithyroid therapy have to be started before biochemical confirmation.
Ipecac. Terramycin.
- What other names is Ipecac known by?
- Causing vomiting (emetic).
- Thinning mucous to make coughing easier, bronchitis associated with croup, hepatitis, amoebic dysentery, loss of appetite, cancer, and other conditions.
- Dosing considerations for Ipecac.
- What is Ipecac?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96194
Buy 250 mg terramycin with visa
The naked area can generally mimic a Hill-Sachs lesion on extra inferior slices; a true Hill-Sachs lesion shall be seen on slices through the superior side of the humeral head antibiotics for uti prevention terramycin 250 mg generic with amex. The axillary view (green) is finest for showing anterior or posterior glenohumeral joint dislocations virus 2014 september terramycin 250 mg buy discount. Note the anterior tilt of the scapula so that the resulting pictures are largely transverse via the anterosuperior and posteroinferior labrum. There will be some partial averaging of the anteroinferior labrum, which courses obliquely by way of the sections. The ensuing photographs have less partial averaging of tears of the anteroinferior and posterosuperior labrum. There is much less elongation of the glenoid, and the section is more perpendicular to the Bankart fracture line. The clavicle is often barely superiorly positioned relative to the manubrium due to the interposed triangular disc. Tepolt F et al: Posterior sternoclavicular joint accidents in the adolescent population: a meta-analysis. The medial clavicle lies adjoining to the brachiocephalic vein, however there was no vascular damage. In this type I lateral 1/3 fracture, the fracture is interligamentous, and the conoid coracoclavicular ligament is intact. Such fractures have the next danger of nonunion than sort I lateral clavicle or nondisplaced center 1/3 fractures. These account for only 5% of clavicle fractures and are sometimes as a outcome of extreme influence to the lateral shoulder. Staging, Grading, & Classification � Allman classification Group 1: Middle 1/3 (80%) 4. Type V is a severe superior dislocation of the distal clavicle, which lies subcutaneously. There is elevation of the distal clavicle relative to the acromion, in addition to widening between the clavicle and the coracoid process by > 50% in contrast with the conventional side (not shown). There is also some resorption of the medial acromion much less widespread in this situation and doubtless from hyperemia/synovitis. The subchondral fracture in this patient might be a fatigue-type stress fracture. Minimally displaced or angulated coracoid course of fractures are normally handled conservatively. There is an impacted fracture of the scapular neck and midclavicular clavicle, in maintaining with a floating shoulder injury. This is a Bankart fracture and is seen in ~ 15% of patients after an preliminary anterior dislocation. These can go on to nonunion or resorption of the fragment if repeated anterior dislocations happen. A Bankart fracture signifies that the affected person has had a previous anterior dislocation. Gyftopoulos S et al: Hill-Sachs lesion location: does it play a role in engagement The patient additionally has a small Hill-Sachs impaction fracture of the posterolateral superior humeral head. Glenoid rim deficiency from resorption of a Bankart fragment &/or mechanical wear of the glenoid rim can happen from repeated dislocations. Note the broad glenohumeral joint, the so-called rim sign, and lack of the traditional halfmoon overlap. The humerus can be internally rotated, causing the sunshine bulb signal, the place the lesser tuberosity initiatives medially. Note the reverse Bankart fracture, reverse Hill-Sachs fracture, and damage to the periosteum. There can be a trough signal indicating a reverse Hill-Sachs impaction fracture of the anteromedial humeral head. The affected person had a subscapularis tendon switch to stop recurrent dislocations. The humerus is parallel to the backbone of the scapula, the frequent position in luxatio erecta. Greater tuberosity fractures can happen either from a fall with direct impaction of the tuberosity onto acromion or from anterior subluxation/dislocation. There is a excessive sign fracture line now with slight displacement of the larger tuberosity. Mutch J et al: A new morphological classification for greater tuberosity fractures of the proximal humerus: validation and medical implications. The cartilagebone interface is the weakest point, thus many acute trauma defects prolong to the subchondral bone plate. The affected person underwent arthroscopic physique removing and debridement of the chondral lesion. There is a grade 4 osteochondral defect of the glenoid involving the subchondral bone with a cartilage flap. At arthroscopic surgical procedure, the body was eliminated and the affected person underwent microfracture of the grade 4 cartilage defect. There are fractures involving the surgical neck as properly as the greater tuberosity and lesser tuberosity. Because the higher tuberosity fracture is just minimally displaced, it is a Neer 3-part fracture/dislocation. Because there was either > 1 cm displacement or > 45� angulation at all 3 fractures, it is a 4-part fracture. It is troublesome to tell if the medial humeral head ridge is a separate fracture fragment or osteophyte. There is a lipohemarthrosis, indicating intraarticular involvement, and decreased muscle tone inflicting gentle inferior subluxation. Surgical fixation prevents malunion, which is related to continued pain and weak point. Comparison with the other shoulder can generally be useful in more refined circumstances of physeal widening. The broad physis distinguishes the periostitis of this harm from different illnesses, similar to leukemia or osteomyelitis. Although there was no cortical irregularity on this patient, some sufferers will current with cortical thickening and areas of hyperlucency. She had a successful closed discount underneath anesthesia performed because of radial nerve palsy and varus angulation. Of patients with humeral shaft fractures, 16% have a radial nerve palsy, presenting as wrist drop.
Terramycin 250 mg discount with visa
Next bacteria article generic terramycin 250 mg on-line, the marrow has an edema-like appearance with decreased T1W signal and elevated signal on T2W photographs virus - zippy discount terramycin 250 mg without prescription. Lastly, the marrow becomes darkish on both T1W and T2W pictures, indicative of fibrosis and sclerosis. Infarcts within the metaphyses and diaphyses might come to clinical consideration due to pain. On radiographs, these lesions might mimic other lesions, especially a chondroid lesion. The bone infarcts otherwise trigger little morbidity, although they could rarely differentiate into malignant fibrous histiocytoma. Continued stress by way of weight-bearing results in attribute findings of subchondral fracture, articular surface collapse, fragmentation, and secondary osteoarthritis. The strategy of therapeutic contains "walling off" the lifeless bone by forming a fibrotic, and eventually sclerotic, margin on the interface between residing and lifeless bone. The issues come up as the physique starts to take away the useless bone as part of this therapeutic course of. It is that this activity that weakens bone, resulting in the subchondral fractures and eventual articular surface collapse and fragmentation with subsequent secondary osteoarthritis. The lag is on the scientific side by means of discovering an applicable remedy, which is ready to either reverse the process of ischemia &/or assist the bone through the healing process. Patients with sickle cell disease are at risk and those with sickle cell thalassemia are at an even larger threat. Imaging Protocols Radiographs the quantity and type of views will differ with the anatomic website being imaged. Many findings, together with articular floor collapse, could solely be visible on a single view. The time frame for improvement of imaging-related modifications is unknown and has been proposed to be so lengthy as six months after the insult. In most sites, axial images might be least delicate to articular surface collapse since this plane is along the short axis of the bone. Sagittal and coronal photographs oriented to the lengthy axis of bone will finest depict these abnormalities. This discovering is best to recognize in the massive femoral head as in comparison with the small bones of the hand and feet. As healing progresses, uptake will occur within the ischemic bone, diminishing sensitivity after the earliest stages. Features widespread to both circumstances embrace articular floor collapse, fragmentation, and 2� osteoarthritis. Once this stage has been reached, the lesion is irreversible; osteoarthritis is likely and may require eventual surgical intervention. A subchondral crescentic fracture is present and is accompanied by articular surface collapse. This alignment alters the mechanics via the wrist, putting elevated stress on the lunate. Changes include patchy sclerosis and collapse, particularly along the proximal articular floor. Patchy sclerosis is present throughout the epiphysis of the proximal humerus with subtle collapse of the articular floor. Serpiginous low signal geographic abnormalities are present within the femoral metaphysis and subchondral bone of each the femur and tibia. The inner marrow sign on T1 is relatively maintained, differentiating this look of infarct from tumor. Extensive marrow edema extends from the top into the neck and is accompanied by joint effusion. This fracture usually marks the purpose of irreversible disease and normally continues to articular surface collapse. Marrow edema is again famous within the lunate with out fracture, articular floor collapse, or fragmentation. Correction of the ulna minus may lead to reversal of the lunate adjustments at this stage. Pattern of edema has shifted, with much less intensive changes laterally and new edema medially and within the proximal tibia. Regional migratory osteoporosis may migrate from one joint to one other, or as on this case, from one location to one other in the identical joint. Joshi V et al: Painless transient bone marrow edema syndrome in a pediatric patient. There can be a subchondral infarct, extra conventionally termed osteonecrosis, within the femoral condyle. Although diagnosis of bone infarcts is usually primarily based on the presence of serpiginous calcification, regularly they present simply as diffuse patchy sclerosis. This patient had Rocky Mountain spotted fever, which can lead to necrotizing vasculitis, in turn leading to osseous infarction. The infarcts contain the subchondral area in addition to the metadiaphysis, although no articular collapse is seen at this time. Of all bone infarcts, 1/3 have a diagnosable etiology; among these, chronic steroid use is common. However, no radiographic modifications of arthritis are seen inside the acetabular articular surface. The hypointense outer darkish line represents sclerosis on the border between the infarcted and normal bone. The shiny line is created by the advancing granulation tissue/inflammatory response. The lateral location of the insult has the next threat of collapse than a extra medially positioned lesion. Once collapse has occurred, surgical choices are restricted to hemiarthroplasty or complete joint replacement. While the etiology is identical, terminology associated with these lesions is usually complicated. Band-like foci of low T1W signal are present within the anterior aspect of each femoral head. Axial aircraft is least prone to reveal articular floor collapse, which often involves the superior articular surface. It demonstrates full absence of enhancement within the head, indicative of posttraumatic loss of blood supply and the need for alternative. Core decompression is designed to relieve intramedullary hypertension and improve blood move.
Order 250 mg terramycin fast delivery
Note that the extracellular calcium concentration is well maintained antibiotics lecture 250 mg terramycin generic, although completely different underlying mechanisms are concerned in the two circumstances (see textual content for details) antibiotics for uti how long terramycin 250 mg with mastercard. The concomitant increase in net bone resorption causes release of phosphate as well as calcium into the extracellular fluid. The decline in intestinal calcium absorption is the major safeguard in opposition to calcium overload, though this mechanism could also be overridden with terribly high intakes of calcium due to the persistence of the passive, non�vitamin D�dependent mode of calcium absorption. Moreover, nonenteral sources of calcium, similar to intravenous calcium infusion or extreme net bone resorption (as from immobilization or malignancy), may readily overwhelm the limited homeostatic variations that stay once suppressed intestinal calcium absorption is bypassed. In such conditions, the kidney rather than the intestine becomes the principal defense towards hypercalcemia, and calcium homeostasis becomes critically depending on sufficient renal perform. If renal perform is impaired in these settings, as regularly occurs clinically, severe hypercalcemia and pathologic calcium deposition in extraskeletal sites could ensue. Although it appears plausible that such assays may show significantly helpful in some clinical conditions, their role is presently unclear. They offer no advantage over older two-site assays, for instance, in diagnosing primary hyperparathyroidism. Note some overlap between regular people and patients with main hyperparathyroidism, but no overlap between hypercalcemic sufferers with major hyperparathyroidism and those with hypercalcemia of malignancy. Advances in methods for measurement of parathyroid hormone: present applications in scientific drugs and instructions for future research. The measurements are based on single or double antibody radioimmunoassays or enzyme immunoassays, a number of of which are sufficiently delicate to detect calcitonin deficiency. However, the double antibody assays are thought to provide the same data with less sample manipulation. The only medical use of the calcitonin assay is as a tumor marker, primarily in medullary carcinoma of the thyroid. Because the assays measure each protein-bound and unbound vitamin D metabolites, results may not always reflect the levels of biologically related ("free") metabolites. This limitation might lead to misleading ends in sufferers with nephrotic syndrome and vitamin D intoxication. With the move away from utilizing radioligand-based assays, different methods for measuring vitamin D metabolites, together with chemiluminescent assays, have been pioneered. Two normocalcemic sufferers with most cancers (filled triangles) subsequently became hypercalcemic. Immunochemical characterization of circulating parathyroid hormone�related protein in patients with humoral hypercalcemia of cancer. The National Institute of Standards and Technology in the United States has developed normal reference supplies for this purpose. Measurement of this metabolite should, subsequently, be carried out when vitamin D deficiency is suspected. Impaired 1-hydroxylation can contribute to the hypocalcemia of sufferers with renal dysfunction, oncogenic osteomalacia, and hereditary defects of vitamin D metabolism (see "Hypocalcemic Disorders"). An assay for the intact hormone is a basic sandwich assay with antibodies directed towards both the N- and C-terminus of the hormone. Primary hyperparathyroidism outcomes most frequently (75-80%) from the incidence of one or more adenomas in beforehand normal parathyroid glands, though in 20% of instances diffuse hyperplasia of all parathyroid glands could also be current or, rarely, parathyroid carcinoma could also be discovered (less than 1-2%). The bone disease "osteitis fibrosa cystica" first was described by von Recklinghausen in 1891, but the etiologic link between this disease and parathyroid neoplasms was not established till 1925, when Mandl noticed clinical improvement following removal of a parathyroid adenoma from a young male with severe bone disease. In early clinical descriptions of primary hyperparathyroidism, the disease emerged as a distinctly uncommon dysfunction with vital morbidity and mortality charges, during which nearly all affected patients manifested radiographically important or symptomatic skeletal or renal involvement, or both. The skeletal involvement in "classical" major hyperparathyroidism displays a hanging and generalized increase in osteoclastic bone resorption, which is accompanied by fibrovascular marrow substitute and elevated osteoblastic exercise. Note the dramatic transforming associated with the intense region of excessive bone turnover in the third metacarpal in addition to widespread evidence of subperiosteal, endosteal, and trabecular resorption. The cranium could exhibit a finely mottled, "salt-andpepper" radiographic look, with lack of definition of the inner and outer cortices. Dental radiographs usually show erosion or disappearance of the lamina dura because of subperiosteal resorption, often with extension into the adjoining mandibular bone. The erosion and demineralization of cortical bone may result in radiographic disappearance of some bones, most notably the tufts of the distal phalanges of the palms, the inferolateral cortex of the distal third of the clavicles, the distal ulna, the inferior margin of the femoral neck and pubis, and the medial facet of the proximal tibia. The medical correlates of those modifications may include aching bone ache and tenderness, "bowing" of the shoulders, kyphosis and lack of top, and collapse of lateral ribs and pelvis with "pigeon breast" and triradiate deformities, respectively. The renal manifestations of classical severe major hyperparathyroidism embrace recurrent calcium nephrolithiasis, nephrocalcinosis, and renal functional abnormalities that vary from impaired concentrating capability to end-stage renal failure. Associated signs and signs include recurrent flank ache, polyuria, and polydipsia. No unique features of the stone disease in primary hyperparathyroidism serve to distinguish it from that associated with different, more frequent causes of calcium kidney stones. The stone illness more usually may be recurrent and severe, and in some patients, the stones could additionally be composed entirely of calcium phosphate, as a substitute of the pure oxalate or mixtures of oxalate and phosphate extra generally encountered in other disorders. In sufferers diagnosed earlier than 1965, the frequency with which nephrolithiasis sophisticated major hyperparathyroidism was as high as 60% to 80% (the frequency is at present lower than 25%), but in studies of unselected sufferers carried out throughout the previous 50 years, major hyperparathyroidism has accounted for fewer than 5% of all calcium kidney stones. Other clinical features which have been reported in association with classical severe main hyperparathyroidism are conjunctival calcifications, band keratopathy, hypertension (50%), gastrointestinal indicators and signs (anorexia, nausea, vomiting, constipation, or abdominal pain), peptic ulcer illness, and acute or chronic pancreatitis. The issue of whether primary hyperparathyroidism will increase the risk for peptic ulcer disease and pancreatitis remains controversial. Although hyperparathyroidism is associated with the next threat of hypertension, profitable parathyroidectomy has not been proven to appropriate the hypertension. Signs and signs in major hyperparathyroidism may end result from the involvement of bone (fracture, bone pain) or kidneys (renal colic, renal failure), peptic ulcer disease, pancreatitis, or hypercalcemia per se (weakness, apathy, despair, polyuria, constipation, coma). The presence and severity of neuropsychiatric signs, specifically, correlate poorly with the serum calcium focus, though few patients with extreme hypercalcemia are entirely asymptomatic. A peculiar neuromuscular syndrome, first described in 1949 but rarely encountered now, consists of symmetric proximal weakness and gait disturbance, with muscle atrophy, attribute electromyographic abnormalities, generalized hyperreflexia, and tongue fasciculations. The scientific spectrum of main hyperparathyroidism was changed dramatically in the early Seventies by the introduction of routine multichannel serum chemistry screening, which unearthed a big population of sufferers with previously unsuspected, asymptomatic illness. In Rochester, Minnesota, for instance, the annual incidence of the disease increased abruptly from zero. Subsequently, the incidence of primary hyperparathyroidism has fallen; this decreased incidence could not merely be a residual effect of "sweeping the inhabitants," because it remained low when serially checked in Rochester, Minnesota, most lately from 1992 to 2001, when the incidence was zero. On the opposite hand, insistence upon overt hypercalcemia as a diagnostic criterion may underestimate the true incidence of the disease. Not surprisingly, on condition that main hyperparathyroidism now normally is recognized incidentally, few patients are discovered to have overt indicators or signs of the classical illness and thus are thought of to be "asymptomatic. Many clinicians argue, however, that the majority patients thought to be having "asymptomatic" main hyperparathyroidism and only minimally elevated serum calcium truly endure from numerous neuropsychiatric or different signs which will improve following healing surgical procedure.
Order terramycin 250 mg without a prescription
This mass prolonged alongside the fascial plane between the gluteus medius and gluteus minimus muscle tissue antibiotics for acne scars buy 250 mg terramycin visa. This proximal-type epithelioid sarcoma has a predilection to arise within the pelvis antibiotic before surgery 250 mg terramycin generic overnight delivery, genital tract, and perineum. This mass extended from the region of the spermatic twine into the subcutis and measured lower than 2 cm. The affected person had a painless mass excised from this region eight years prior with unclear pathology. These lesions typically comprise hemorrhage of varying ages and necrosis, giving them a variable appearance on imaging. This tumor had metastasized to the intraabdominal delicate tissues and lymph nodes on the time of presentation. Oike N et al: Extraskeletal myxoid chondrosarcoma arising in the femoral vein: a case report. The central areas lacking enhancement histologically corresponded to outstanding areas of infarct-like necrosis. Despite the large size of this lesion, no metastases were evident at presentation. The mass accommodates matrix, which is rare for extraskeletal myxoid chondrosarcoma. It contains hyperintense material centrally, doubtless representing hemorrhage (frequently seen in this lesion). There is central high signal in a portion of the lesion that doubtless represents hemorrhage. The thigh is the most typical location of this lesion, and the lobulated appearance is typical. The mass is heterogeneously isointense to hyperintense relative to skeletal muscle. The degenerative, fibrosing changes that involve the plantar digital nerve can also contain the encompassing delicate tissue, thus obscuring the borders of the mass. This is centered within the location of the third widespread digital branch of the medial plantar nerve. Compression is useful for distinguishing between a neuroma and bursitis, as bursal fluid will dissipate with compression. Altered weight-bearing, related to the implant placement, might have contributed to the event of the neuroma. The bulbous mass contour and location at the finish of a transected nerve make this typical for a terminal type traumatic neuroma. The enlarged nerve fascicles are faintly visible, giving it a phone cable or fascicular appearance. Fusiform nerve enlargement over a a number of centimeter segment of intact nerve is typical for a spindle sort traumatic neuroma. The mass is in an intermuscular location, with out invasion of the surrounding structures. The central portion of the mass extra intensely enhances compared with the peripheral portion of the mass. No inside blood circulate was seen, nor was the mass clearly contiguous with a nerve. These lesions characterize diffuse and localized neurofibromas in a affected person with recognized neurofibromatosis type 1. One of the masses has a central focus of decreased sign, according to a goal signal. There is outstanding bowing of the flexor retinaculum and displacement of the flexor tendons. The nerve may be seen extending from the mass distally, and the mass deviates the lateral head of the gastrocnemius muscle. The mass has heterogeneous signal depth starting from isointense to barely hyperintense to skeletal muscle. Ahlawat S et al: Schwannoma in neurofibromatosis sort 1: a pitfall for detecting malignancy by metabolic imaging. Beaulieu S et al: Positron emission tomography of schwannomas: emphasizing its potential in preoperative planning. The mass is isointense to barely hypointense to the adjacent muscle, making it tough to delineate. Schwannoma enhancement varies from absent to intense and could additionally be homogeneous or inhomogeneous. Given the situation, large cell tumor or neurofibroma are likely diagnoses, although schwannoma and chordoma ought to be thought-about as properly. The lesion also entails the neural foramen, growing the probability of nerve sheath tumor; schwannoma was confirmed. Although this could be seen in any delicate tissue tumor, it happens most often in synovial sarcoma, the more than likely working prognosis. It is significant that the lesion is in the path of a branch of the femoral nerve. Longstanding schwannomas are more likely to have heterogeneous signal from calcification and different degenerative change. The mass is heterogeneously isointense to skeletal muscle with a small central focus of decreased signal. Regions of very high sign may be due to hemorrhage, cyst, or necrosis, each of which are common. There is chronic denervation of the proper gluteus muscle tissue with fatty infiltration. Nonenhancing regions likely characterize a combination of necrosis, old hemorrhage, or calcification. This mass is slightly inhomogeneous, with sign intensity much like and barely higher than skeletal muscle. The left neurofibroma additionally enhances, in addition to other further intrathecal neurofibromas. The mass incorporates scattered foci of debris that have slightly decreased sign intensity. Internal enhancement is tough to assess as a result of the intrinsic T1 hyperintensity of the lesion. Melamud K et al: Diagnostic imaging of benign and malignant osseous tumors of the fingers. Location alongside the extensor surface of the rest of the upper extremity is the 2nd commonest website; extra nodules are shown involving the dorsal wrist, and dorsal finger. The agency, fleshy superficial nodules could also be adherent to underlying constructions or freely mobile. Imaging of these lesions can mimic a delicate tissue neoplasm, abscess, crystal disease, and overseas physique granuloma.
Terramycin 250 mg discount free shipping
Before these medicine are prescribed antibiotic resistance not finishing prescription buy terramycin 250 mg on line, it is important to antibiotics for acne in south africa terramycin 250 mg buy generic on-line exclude ischemic heart illness. These drugs are completely contraindicated in patients being handled with nitroglycerine or other nitrate-containing medicine as a outcome of severe hypotension and deadly cardiac occasions can happen. The inflatable kind is three times costlier and subject to mechanical failure, however it avoids the embarrassment caused by other units. In diabetic autonomic neuropathy, the motor perform of the bladder is unimpaired, but afferent fiber damage results in diminished bladder sensation. Patients are seen with bladders crammed to their umbilicus, yet they really feel no discomfort. Loss of bladder sensation occurs with diminished voiding frequency, and the affected person is no longer capable of void fully. The principal goal of the remedy should be to improve bladder emptying and to reduce the risk of urinary tract an infection. Extended sphincter rest can be achieved with an 1-blocker, such as doxazosin. Sweating Disturbances Hyperhidrosis of the higher physique, often associated to eating (gustatory sweating), is a characteristic feature of autonomic neuropathy. Gustatory sweating accompanies the ingestion of sure meals, significantly spicy foods and cheeses. Gustatory sweating is extra widespread than previously believed; topically applied-and probably oral- glycopyrrolate (an antimuscarinic compound) is a really effective remedy in reducing each severity and frequency. Loss of decrease body sweating could cause dry, brittle skin that cracks easily, predisposing the affected person to ulcer formation that can lead to loss of a limb. The launch of catecholamine alerts the affected person to take the required measures to stop coma as a result of low blood glucose. The incapability to acknowledge the warning indicators of impending neuroglycopenia is called hypoglycemic unawareness. The failure of glucose counterregulation could be confirmed by the absence of glucagon and epinephrine responses to hypoglycemia induced by a regular managed dose of insulin. However, a syndrome of hypoglycemic autonomic failure occurs with intensification of diabetes control and repeated episodes of hypoglycemia. In the absence of severe autonomic dysfunction, hypoglycemic unawareness associated with hypoglycemia is a minimal of partially reversible. Patients with hypoglycemia unawareness and unresponsiveness pose a big management problem for the physician. It is our advice that, if a pump is used, boluses of smaller than calculated amounts should be used. If intensive standard remedy is used, long-acting insulin with very small boluses ought to be given. Further complicating management in some diabetic patients is the development of a functional autonomic insufficiency related to intensive insulin therapy, which resembles autonomic neuropathy in all related elements. Avoidance of hypoglycemia for a number of days ends in recovery of the adrenergic response. These information help recommendations from the American Diabetes Association to treat diabetic subjects as in the occasion that they already have established coronary artery disease. These incidence charges presumably reflect sufferers of their late 30s, 10 years beyond baseline age in the studies. It additionally seems that diabetes interacts synergistically with different threat components to extra sharply increase threat as the variety of complete risk factors will increase. In the presence of diabetes, the cardiovascular demise rate steeply rises at any degree of concomitant risk elements. Other studies have additionally concluded that impaired insulin sensitivity through the prediabetic state contributes to atherogenic threat. Therefore, a proinflammatory state can contribute to the atherogenic risk profile in prediabetic sufferers with elevated insulin resistance. Many aspects of the proatherogenic and proinflammatory state of prediabetes might derive from elevated adiposity and specifically visceral fats. The greater diploma of improvement in danger factors with intensive therapy was also mirrored in outcomes. Cardiovascular mortality and all-cause mortality charges improve all through the range of fasting plasma glucose in a graded trend. This association appears to be graded and continuous, with no clear threshold below which the relationship ends. Tominaga and colleagues examined survival rates in a cohort of members in a diabetes prevalence trial in Japan877 and concluded that the danger of cardiovascular fatality is predicated on impaired glucose tolerance rather than impaired fasting glucose. The outcomes indicated that the oral glucose tolerance take a look at provides the most effective index of risk of mortality associated with impaired glucose tolerance. There had been also differences in prevalence based mostly on ethnicity, with the highest general prevalence among Mexican Americans (31. Similar degrees of improve in danger with the metabolic syndrome were also seen when different diagnostic criteria had been used. The query stays, nonetheless, whether intensive glycemic control can modify the cardiovascular danger profile of patients with diabetes. Patients in the conventional treatment group had more albuminuria and microalbuminuria than intensively treated patients, but the variations in threat remained important after adjustment for these components. Because these drugs work by growing insulin sensitivity quite than by growing insulin levels, this finding is in preserving with information displaying that insulin resistance is positively correlated with cardiovascular outcomes (described earlier). According to the investigators, this broad primary finish point, which prolonged beyond the extra commonplace, objective major finish point often employed in cardiovascular trials, was accomplished to enhance the possibilities of seeing benefit. In fact, enhancements in peripheral vascular disease end points have been tough to show, even in the presence of potent cardiovascular risk-reducing agents like statins. Compared with placebo, pioglitazone also significantly reduced the necessity to add insulin to glucose-lowering regimens. Intravascular coronary ultrasound studies have also shown important decreases in coronary atherosclerosis in response to pioglitazone. In contrast, one other meta-analysis, carried out by Lago and associates, examined solely randomized scientific trials by which cardiovascular finish factors had been prespecified as occasions of interest or by which such events had been adjudicated. Enthusiasm for the use of these agents has also been tempered by elevated bone fractures and questions relating to bladder most cancers. As a outcome, a appreciable quantity of new knowledge concerning cardiovascular results of oral antidiabetic brokers is now rising or forthcoming. Two landmark trials testing the effects of saxagliptin and alogliptin on cardiovascular occasions have now been revealed. The difficulties in establishing this seemingly straightforward proposition has been attributed to various elements: trial points (too quick, too small, poor design), offsetting results of brokers, pursuit of targets unlikely to yield benefit, or intervening in patients too late in their pure history. The latter notion is supported by indicators in trials suggesting that subgroups with the shorter length of diabetes do manifest cardiovascular profit via tighter glucose management, whereas other work suggests these with less coronary calcification, which can also replicate a illness means of shorter duration, might benefit. A number of options of dyslipidemia are uniquely associated with diabetes and appear to improve the predisposition to atherogenesis. Several research have additional verified the usage of statins in patients with diabetes and related situations. Such issues could stem from various components, corresponding to totally different sorts of strokes (hemorrhagic vs.