
Rumalaya forte dosages: 30 pills
Rumalaya forte packs: 1 packs, 2 packs, 3 packs, 4 packs, 5 packs, 6 packs, 7 packs, 8 packs, 9 packs, 10 packs

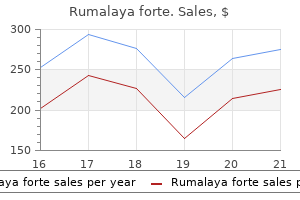
Rumalaya forte 30 pills on line
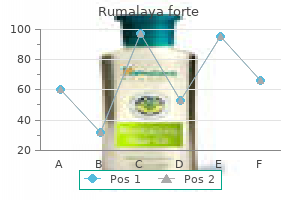
Calculation of the urine anion hole (as an oblique measure of urinary ammonium excretion) may be helpful in identifying a diarrhoea-induced (with elevated urinary ammonium and adverse anion gap) aetiology of hypokalaemic metabolic acidosis spasms sleep cheap rumalaya forte 30 pills overnight delivery. Renal potassium loss the most common reason for hypokalaemia is increased renal potassium excretion muscle relaxant kidney stones trusted 30 pills rumalaya forte, often from drugs or, in uncommon situations, intrinsic renal defects. Drugs Many medicines enhance renal potassium excretion, together with diuretics, sure antibiotics, and anti-neoplastic agents, and toxins. Both thiazide and loop diuretics improve urinary potassium excretion; (Siegel et al. All diuretics, besides the potassium-sparing diuretics, improve potassium excretion increasing amassing duct luminal move price and luminal sodium delivery and high dietary sodium chloride consumption exacerbates the kaliuretic results of diuretics. Some antibiotics, anti-neoplastic medication, and toxins can enhance urinary potassium excretion by a number of mechanisms. High-dose penicillin and some penicillin analogues, such as carbenicillin, oxacillin and ampicillin, enhance distal tubular supply of a non-reabsorbable anion, which will increase urinary potassium excretion (Gill et al. Polyene antibiotics, significantly amphotericin B, create cation channels within the apical membrane of accumulating duct cells, which will increase potassium secretion and leads to impaired potassium conservation (Kamel et al. Cisplatin may induce hypokalaemia through an increase in renal potassium excretion (Jones and Chesney, 1995), and ifosfamide causes a Fanconi-like syndrome with hypokalaemia in up to 4% of sufferers who receive this drug (Ho et al. Aminoglycoside antibiotics may cause hypokalaemia both in the presence or absence of overt nephrotoxicity. Potassium supplementation protects in opposition to experimental aminoglycoside nephrotoxicity (Thompson et al. Aldosterone is a crucial hormone that regulates total physique potassium homeostasis, and extra aldosterone exercise frequently leads to hypokalaemia. Primary hyperaldosteronism results in hypertension (Holland, 1995), partially due to the sodium-retaining results of aldosterone and partly by way of direct effects of aldosterone on vascular endothelium and on vascular easy muscle cells, and thru central nervous system-induced mechanisms. In addition, the related hypokalaemia may contribute by sensitizing the vasculature to neurohumoral regulators of blood stress. An aldosterone-producing Magnesium depletion Magnesium depletion is discovered in many medical circumstances associated with potassium depletion (see Chapter 27). The compulsory loss of cations, to preserve electroneutrality, ends in renal potassium wasting. In each case, elevated distal tubular luminal bicarbonate delivery increases potassium secretion (Malnic et al. This is also true in certain instances of aminoglycoside toxicity and cisplatin toxicity, hypokalaemia related to lysozymuria in acute leukaemia, and in people with Gitelman syndrome (see below). Hypomagnesaemia is frequently observed with hypokalaemia and may contribute to its improvement. In humans, magnesium depletion is associated with hypokalaemia (Kelepouris and Agus, 1998) and will induce renal potassium wasting (Shils, 1969). In addition, dietary magnesium depletion causes a selective potassium loss from cardiac as properly as skeletal muscle, and intracellular potassium deficiency will not be restored by potassium administration alone within the presence of magnesium deficiency (Whang, 1987; Rodriguez et al. These observations suggest co-administration of magnesium might additional improve potassium handling when each are poor. Potassium loss in magnesium deficiency may be associated to a relative enhance in the exercise of renal potassium channels and, therefore, continued urinary potassium excretion (Hille, 1992). Magnesium oxide 250�500 mg by mouth four occasions daily is the preferred methodology of replacement. Diagnosis of hypokalaemia Evaluation of the patient with hypokalaemia ought to begin with a radical historical past and physical examination. One ought to first contemplate and exclude pseudohypokalaemia due to potassium uptake by abnormal leucocytes and consider hormones, drugs or conditions that end in redistribution of potassium from the extra- to the intracellular area. If none of these potentialities is current, then the hypokalaemia probably represents whole body potassium depletion resulting from potassium loss through the kidney, gastrointestinal tract, or skin. Hypomagnesaemia-induced hypokalaemia might causes renal potassium wasting, and may happen with aggressive diuresis. Gastrointestinal potassium loss happens from diarrhoea, vomiting, nasogastric suction, or a gastrointestinal fistula. Many instances are obvious from the history and the medical setting, however less obvious causes embody surreptitious vomiting and laxative abuse, which are frequently diagnostic challenges. Erosion of the dental enamel, metabolic alkalosis, and low urinary chloride content are all options of chronic vomiting and clues to its prognosis. In patients with self-induced diarrhoea from catharctics, the historical past of laxative use could additionally be tough to obtain. Habitual use of anthracene laxatives, similar to senna, cascara, and aloe, results in melanosis coli (Wittoesch et al. Phenolphthalein is a cathartic and has been previously used in laxatives that turns pink or purple within the presence of a powerful alkali. Excessive potassium loss from the skin may result from extended exposure in scorching environments the place sweat loss is excessive, and this prognosis must be obvious from the historical past. Bartter and Gitelman syndromes are uncommon genetic problems that exhibit hypokalaemia and normally exhibit metabolic alkalosis with a normal or low blood strain. However, a much more frequent trigger for this constellation of findings is surreptitious diuretic abuse. A urine display screen for diuretics is a vital part of the analysis of the affected person with potential Bartter or Gitelman syndrome to find a way to exclude surreptitious diuretic use. Bartter and Gitelman syndrome can be differentiated from each other by evaluation of urinary calcium excretion, which is excessive with Bartter syndrome and suppressed in Gitelman syndrome. Renal transport defects Genetic illnesses of hypokalaemia are uncommon, but have superior our understanding of renal physiology. In 1962, Bartter described the affiliation of hypokalaemia, hypomagnesaemia, hyper-reninaemia, and metabolic alkalosis (Bartter et al. Further phenotypic refinement led to the popularity of two syndromes: Bartter syndrome and Gitelman syndrome (Gitelman et al. These three proteins are needed for sodium reabsorption within the thick ascending limb of the loop of Henle (Simon et al. Gitelman syndrome features hypocalciuria, hypomagnesaemia, milder scientific manifestations, and it generally presents at a later age. This syndrome most commonly is due to mutations affecting the thiazide-sensitive NaCl cotransporter (Simon et al. Hypotension and intravascular volume depletion because of renal sodium-wasting are widespread features in both. Concomitant intravascular quantity depletion and secondary hyperaldosteronism further exacerbates the hypokalaemia. Treatment of the hypokalaemia incessantly includes oral administration of enormous amounts of potassium chloride, however some degree of hypokalaemia regularly persists. Liddle syndrome is related to hypertension, hypokalaemia, metabolic alkalosis, and suppressed renin and aldosterone levels (Liddle et al. Less frequent causes embrace hyperaldosteronism, acute anabolic stimulus or history suggestive of hypokalemic periodic paralysis Presence of cathartics or osmotic agents (high magnesium or phosphate concentration) in stool No Yes Hyomagnesemia-induced hypokalemia Probable secondary hyperaldosteronism No Serum bicarbonate
Diseases
- Syndrome of inappropraite antidiuretic hormone
- Keratosis palmoplantaris esophageal colon cancer
- Forney Robinson Pascoe syndrome
- Hallervorden Spatz disease
- Platelet disorder
- Enteropathica
- 18-Hydroxylase deficiency, rare (NIH)
- Roberts syndrome
- Albinism oculocutaneous, Hermansky Pudlak type
- Richards Rundle syndrome
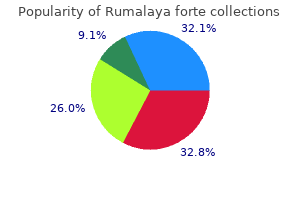
Purchase rumalaya forte 30 pills on-line
Due to increased international recognition spasms near ribs discount rumalaya forte 30 pills amex, prevalence charges seem to be rising and vary between 2 muscle relaxant before exercise order 30 pills rumalaya forte visa. Neuropsychological status has been noticed in some cases to progressively decline impartial of different neuro logical episodes [128]. Neuroimaging findings show inflammatory lesions with a predilection for the diencephalon, midbrain, and brainstem [128]. The lesions have additionally been observed to resolve after administration of corticosteroids [128]. Corticosteroids and different immunosuppressive brokers have been essentially the most effec tive remedies for these manifestations in uncontrolled studies, case collection, and case stories. The external carotid system is most vulnerable, and involvement of the optic nerve can result in visual loss. The most typical neurologic features are head ache, amaurosis fugax, and neuroophthalmologic signs, and many sufferers also current with systemic symptoms together with weight reduction, fatigue, fever, and polymyalgia rheumatica. Two thirds of sufferers with medium vessel involvement current with newonset severe complications, generally situated in temporal areas [138]. Large vessel involvement usually manifests as claudication in the arms, absent or asymmetrical pulses and blood stress readings, and occasional tissue gangrene [139]. Aortic involvement is commonly not clinically detectable, but can result in severe arterial dilation and aneurysm [140]. Thirty p.c of patients present with neurological manifes tations, including neuropathies (14%) and fewer generally tran sient ischemic attacks and strokes (3�4%) that result from extreme occlusion of carotid or vertebral arteries [141]. The clinical course of cognitive impairment is variable, and cognitive dysfunction has been noticed to be conscious of corticosteroid remedy. Comparable to the opposite vasculitides, therapy is basically empirical but sometimes includes highdose intravenous or oral corticosteroids [145]. Anticoagulation has also been used in some instances, typically after proof documents the formation of thrombi in the infected arteries [146]. Systemic sclerosis (scleroderma) Systemic sclerosis is a multisystem autoimmune disease that confers severe dangers for morbidity and mortality [148]. Neurological symptoms are relatively unusual however can embody cranial and peripheral neuropathies. In another study, 52% of patients had lesions within the corticomedul lary junction, 56% within the periventricular regions, 40% in the basal ganglia, and 40% within the pons [122]. Studies using neuropsychological assessment show govt dysfunction, and it has been posited that cardiovascular reactivity performs a job in cognitive alterations of these patients [152]. Sarcoidosis Sarcoidosis is a granulomatous multisystem disorder of unknown etiology, though autoimmunity has been strongly implicated. Sarcoidosis can affect any a half of the body, although lung, pores and skin, and eye manifestations are the most typical. The disease sometimes presents within the 30s and 40s and is more com mon among folks of West African descent and North European Caucasians [153]. The prevalence in the United States is esti mated at 40 per one hundred 000 [154], with annual incidence rates of sixty five. Noncaseating granulomata, consisting of centrally organ ized macrophages and epithelioid cells encircled by lympho cytes, are the basic pathological features of sarcoidosis. Cranial neuropathy appears to be the most common manifestation, affecting 50�75% of patients, followed by cognitive or behavio ral manifestations in 20%, meningeal involvement in 10�20%, and seizures in 5�10% [157]. For example, 10�15% of neurosarcoidosis patients develop neuroendocrine associated symptoms because of hypothalamic and pituitary involvement [160]. With respect to cognitive dysfunction and dementia, case reports of sufferers with neurosarcoidosis describe extreme psychiatric manifestations together with psychosis and delirium [161�163]. Although the procedure entails important danger, the gold normal for the diagnosis of neurosarcoidosis is brain biopsy to search proof of noncaseating granulomata. In the absence of biopsy, other diagnostic criteria have been suggested, although a definite prognosis could also be difficult to reach. Probable neurosar coidosis may be recognized when the medical presentation is con sistent with neurosarcoidosis, other mimickers have been excluded, and a therapeutic response has been observed to immunotherapy for 12 months [166]. As in different illnesses for controlled trial proof of remedy is missing, therapy is largely empirical and employs the usage of corticosteroids and other immunosuppressive drugs. Celiac illness Celiac disease is an autoimmune dysfunction brought on by an opposed reaction to gliadin, a protein present in wheat, along with a simi lar reaction to associated proteins in barley and rye. An inflamma tory response within the intestine is triggered when tissue transglutaminase enzyme modifies the triggered gliadin protein as it reacts with small bowel tissue. This course of inhibits the absorption of nutri ents, and small bowel involvement leads to symptoms together with continual diarrhea, failure to thrive (in children), and fatigue. The prevalence of neurologi cal dysfunction resulting from celiac disease is unclear, however some stories suggest neurological dysfunction occurs in 10 to 23% of sufferers [169, 170]. Several research have noticed substantial cognitive deficits in small cohorts of patients with celiac illness [173]. Diagnostically, the affiliation between autoantibody produc tion and neurologic dysfunction is unclear, with some sufferers showing serum antibody reactivity to a number of ganglio sides, while other patients present no reactivity [169]. A proposed diagnostic schedule by Hadjivassiliou and colleagues included testing for gliadin, deamidated gliadin, and antitissue transglu taminase IgA and IgG antibodies, adopted by duodenal biopsy to detect enteropathy or, in the absence of enteropathy, the iden tification of IgA deposits towards tissue transglutaminase on the biopsy [174]. Other treat ments underneath energetic exploration and development embrace enzyme supplements, engineered grains and pretreatment of flours, and neutralizing gluten antibodies [176]. The relationship among depres sion, subjective cognitive impairment, and neuropsychological efficiency in a number of sclerosis. Evidencebased guidelines for the usage of immunologic checks: antinuclear antibody testing. Estimates of the preva lence of arthritis and selected musculoskeletal issues in the United States. Epidemiological research in incidence, prevalence, mortality, and comorbidity of the rheumatic diseases. Estimating the incidence of systemic lupus erythematosus in a tropical region (Natal, Brazil). Part 1: Renal, neuropsychiatric, cardiovascular, pulmonary, and hemato logic illness. Prospective clinical and computed tomographic classification of eighty two occasions in seventy one patients. The inci dence and prognosis of central nervous system disease in systemic lupus erythematosus. The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Summary and conclusions Each of the illnesses and syndromes described beforehand is characterised by a broad range of clinical displays and dis parate neurological and cognitive sequelae, however all of them share the presence of autoimmunity and a propensity to trigger important cognitive dysfunction and associated disability in chosen sufferers. It is clear that the cognitive manifestations of those rheumato logic circumstances influence the development of disability by impacting actions of daily residing, accelerating departure from the work pressure, and negatively impacting overall wellbeing. Neuropsychological testing in these sufferers may facilitate the identification of particular patterns of cognitive impairment, aiding patient care and offering clues to patho physiology.
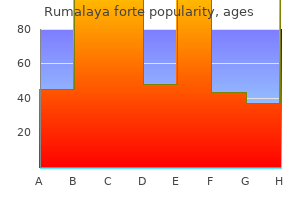
Discount rumalaya forte 30 pills
Perirolandic spasms that cause coughing rumalaya forte 30 pills generic, supplementary motor space muscle relaxant definition rumalaya forte 30 pills online buy cheap, striatal and insular atrophy are associated with the executive�motor syndrome [8]. Case 2 Nonfluent variant primary progressive aphasia A 54yearold righthanded lady first famous difficulty with speaking three years previous to analysis. Initially, she had bother finding phrases in conversation, and pauses in her speech developed into stuttering. Her speech was slurred; she made frequent phonemic paraphasic errors, and she or he sometimes careworn the incorrect syllable in pronouncing phrases. Six months prior, she developed issue utilizing her right hand and began to use her left hand to decide up objects. There was gentle cogwheel rigidity in the right higher extremity, but no axial rigidity. Neuropsychological testing revealed important deficits in language testing, together with naming and repetition. Verbal reminiscence and govt perform were impaired, however the prominence of her language impairments rendered the interpretation of other cognitive testing less clear. She had involuntary actions in her proper hand and foot, which additionally intermittently assumed dystonic postures, and finally had bother utilizing utensils in her left hand. On examination, her eye movements had been extraordinarily limited, and she or he had rightsided visible neglect. Case three Behavioral variant frontotemporal dementia A 64yearold gentleman started to develop character modifications 7 years prior to analysis. He developed a newfound interest in painting, and commenced to put on bizarre, brightly colored outfits. Over the subsequent a number of years, his obsession with portray burgeoned, and he created lots of of items of artwork. Previously conservative with cash, he developed an curiosity in playing, both successful and dropping giant amounts of cash in casinos. He became a "bornagain" Christian 5 years prior to analysis and started praying a quantity of instances a day. Four years after his character adjustments started, he developed shortterm reminiscence difficulty. In the few months previous to analysis, his family noted that his gait grew slower and that he had a hand tremor. Neuropsychological testing revealed important deficits in memory, language, and government operate. He stopped initiating conversations and needed to be monitored and encouraged to perform primary activities of day by day residing, corresponding to toileting and grooming. Often, behavioral modifications are misdiagnosed as psychiatric disease early within the disease course. Clinical options of progressive supranuclear palsy syndrome Progressive supranuclear palsy was first outlined as a neurode generative syndrome consisting of supranuclear vertical gaze palsy, axial dystonia with a hypererect posture, bradykinesia, rigidity, and early falls [9]. Case research: A 63yearold man developed problems with focus 5 years prior to evaluation. Previously excellent with multitasking, he described vital issue maintaining track of a couple of exercise concurrently. He grew more outspoken, began telling his coworkers exactly what he thought of them, and have become less aware of putting himself and others in uncomfortable situations. Three years previous to evalua tion, he fell when trying to rise up from a reclining chair. Two years previous to evaluation, he walked more slowly and he developed a shuffling gait. Mild emotional triggers caused him to snicker and cry easily and grew extra disinhibited in social situations. Vertical saccadic velocity was reduced, with downgaze more affected than upgaze; horizontal saccades appeared regular. Deep tendon reflexes have been 2+ within the extremities, and plantar responses have been flexor. Neuropsychological testing revealed deficits only in executive operate and indicated that his responses were error inclined and impulsive. He developed extreme dysarthria and dysphagia, which required a modified food regimen to stop aspiration. Prominent behavioral modifications often emerge, with apathy and disinhibition being the most common [67]. With supranuclear gaze palsy, the oculocephalic reflex is undamaged early within the illness course but disappears in later illness levels. Other ocular abnormalities usually embody square wave jerks, blepharospasm, eyelid opening apraxia, and decreased blink fee [71]. The procerus signal, brought on by contraction of the corrugator and orbicularis oculi muscles leading to wrinkles within the glabellar region and the bridge of the nostril, may give a furrowedbrow look [72, 73]. As motor symptoms progress, nonetheless, falls may be unpredictable, with no known provocation. The etiology of the falls is multifactorial; impaired downgaze, poor postural reflexes and instability, and impulsivity all contribute to fall danger. Tau protein has six isoforms which harbor either three or four tubulinbinding repeats, referred to as 3R and 4R isoforms, respectively. Tau protein assists in microtubule meeting and stability and is very expressed in axons. Hyperphosphorylation of tau alters its binding affinity for microtubules and will increase its aggregation into multimers [89b, c]. The cerebellar dentate nucleus and superior cerebellar peduncle present neuronal loss [95]. Mild neuronal loss and gliosis happen within the thalamus and striatum and the nucleus basalis of Meynert [96]. Neurofibrillary tangles are composed of paired helical fila ments and straight filaments of tau protein [97]. In oligodendro cytes, taupositive, argyrophilic, perinuclear fibers appear as coiled bodies [102]. Across all subtypes, the subthalamic nucleus, substantia nigra, and globus pallidus are most severely affected by tau pathology [103, 104, 106]. Nearly all of those studies were performed with clinically diagnosed sufferers with out post-mortem studies, limiting the scope and energy of these analyses. Summary Corticobasal degeneration and progressive supranuclear palsy are 4R tauopathies with heterogeneous shows and appreciable medical and pathological overlap. A heterogeneous degeneration involving the mind stem, basal ganglia and cerebellum with vertical gaze and pseudobulbar palsy, Nuchal Dystonia and Dementia.
Buy 30 pills rumalaya forte overnight delivery
This chapter will concentrate on renal mechanisms of diuretic action and diuretic remedy of oedema muscle relaxant pills over the counter order rumalaya forte 30 pills without prescription. The molecular targets of diuretic medication are predominantly Na+ transport pathways on the apical (luminal) floor of kidney tubule cells spasms 1983 dvd rumalaya forte 30 pills generic otc. Mannitol is freely filtered at the glomerulus and its presence in tubule fluid minimizes passive water reabsorption. When an osmotic diuretic is administered, the osmotic force of the non-reabsorbable solute in the lumen opposes the osmotic pressure produced by sodium reabsorption, and sodium reabsorption eventually stops. Perhaps surprisingly, mannitol has a greater impact on inhibiting Na and water reabsorption in the loop of Henle than within the proximal tubule. Further downstream, in the collecting duct, mannitol can also scale back sodium and water reabsorption (Buerkert et al. During the administration of mannitol, its molecules diffuse from the blood stream into the interstitial house. Renal cortical and medullary blood flow rates improve following mannitol infusion (Buerkert et al. Experimental research point out that the osmotic effect of mannitol to improve water motion from intracellular to extracellular house leads to a decrease in haematocrit and in blood viscosity. Of the filtered load, < 10% is reabsorbed by the renal tubule, and a similar quantity is metabolized, in all probability in the liver. Osmotic diuretics Osmotic diuretics are substances which might be freely filtered on the glomerulus, but are poorly reabsorbed. Inhibition of NaCl reabsorption by these drugs depends on the osmotic strain exerted by the drug molecules in answer, not on interplay with specific transport proteins. Because the connection between the magnitude of diuretic effect and focus of osmotic diuretic in answer is linear, all osmotic diuretics are small molecules. Following mannitol infusion, sodium, potassium, calcium, magnesium, bicarbonate and chloride excretion rates increase (Table 33. Sodium and water reabsorption charges are decreased by 27% and 12%, respectively (Seely and Dirks, 1969). Magnesium and calcium reabsorption can additionally be reduced along the proximal tubule and loop of Henle. Carbonic anhydrase inhibitors additionally enhance potassium excretion, likely indirectly. The impact of carbonic anhydrase inhibitors on the proximal tubule ion transport facilitates an increase in tubular fluid circulate price and sodium and bicarbonate delivery to the distal nephron, the place the lumen unfavorable voltage (Malnic et al. The biochemical, morphological, and useful properties of carbonic anhydrase have been reviewed (Pastorekova et al. Carbonic anhydrase inhibitors act primarily on this segment, but their natriuretic efficiency is relatively weak. First, proximal sodium reabsorption is mediated by carbonic anhydrase-independent as properly as carbonic anhydrase-dependent pathways. Second, the elevated sodium delivered to distal nephron segments is essentially reabsorbed. Third, carbonic anhydrase inhibitors generate a hyperchloraemic metabolic acidosis, further decreasing the results of subsequent doses of carbonic anhydrase inhibitor. Finally, metabolic acidosis increases the Ki for bicarbonate absorption by membrane impermeant carbonic anhydrase inhibitors by an element of 100 to 500, suggesting that metabolic acidosis is associated with modifications in the physical properties of the carbonic anhydrase protein (Shuichi and Schwartz. For these reasons, carbonic anhydrase inhibitors alone are hardly ever used as diuretic agents chronically; they do, nevertheless, play an necessary function in short-term treatment of diuretic resistance. The highest concentrations are present in tissues that comprise massive amounts of carbonic anhydrase. Renal effects are noticeable inside half-hour and are normally maximal at 2 hours. The half-life is approximately 5 hours and renal excretion is actually complete in 24 hours (Weiner, 1990). Generally, carbonic anhydrase inhibitors are well tolerated with rare serious adverse results. Side results of carbonic anhydrase inhibitors might arise from the continued excretion of electrolytes. In elderly patients with glaucoma treated with acetazolamide (250�1000 mg/day), metabolic acidosis was a frequent finding (Heller et al. Premature infants treated with furosemide and acetazolamide are particularly susceptible to nephrocalcinosis, presumably as a end result of the combined effect of an alkaline urine and hypercalciuria (Stafstrom et al. Although these medicine additionally impair ion transport by proximal and distal tubules under some conditions, these effects in all probability contribute little to their action clinically. The loop diuretics obtainable embrace furosemide, bumetanide, torsemide, and ethacrynic acid. Loop diuretics improve water, Na+, K+, Cl-, phosphate, magnesium, and calcium excretion rates (Table 33. During maximal loop diuretic motion, the urinary + concentration is normally between seventy five and one hundred mmol/L (Puschett Na and Goldberg, 1968). This impact of loop diuretics has been exploited to treat hyponatraemia, when combined with normal or hypertonic saline (Hantman et al. This transporter is a member of the cation chloride cotransporter family (Hebert et al. This protein uses the electrochemical gradient favouring Na+ entry across the apical membrane to move Cl- into the cell together with K+, whereas K+ diffuses back into the luminal fluid by way of a K+ channel; thus, web reabsorption throughout this section is primarily NaCl. The mixture of K+ movement across the apical membrane and Cl- movement across the basolateral cell membrane generates a transepithelial voltage oriented in the lumen-positive course (Greger and Schlatter, 1983), which drives absorption of Na+, Ca2+ and Mg2+ via the paracellular pathway. It should be noted, nevertheless, that both the transcellular and the paracellular components of Na+ transport are inhibited by loop diuretics, the previous instantly and the latter not directly. The mixture of solute absorption and water impermeability determines the role of the thick ascending limb as the primary diluting section of the kidney. Thick ascending limb cells have been proven to produce prostaglandin E2 following stimulation with furosemide (Miyanoshita et al. Blockade of cyclooxygenase reduces the results of furosemide to inhibit loop section chloride transport in rats (Kirchner, 1985; Kirchner et al. When given intravenously, peak diuretic concentrations are reached rapidly, but levels may decline extra quickly than throughout oral administration. As natriuresis is decided by the time above the natriuretic threshold, and because the threshold is impacted by illness (A), the relationship between oral and intravenous efficacy is complicated. Increases in renal prostaglandins can also contribute to the haemodynamic results of loop diuretics described beneath. Ca2+ and Mg2+ transport Loop diuretics enhance the excretion of the divalent cations, calcium and magnesium, owing to their effects to scale back the transepithelial voltage.
Triacontanol (Policosanol). Rumalaya forte.
- How does Policosanol work?
- Are there any interactions with medications?
- Dosing considerations for Policosanol.
- Are there safety concerns?
- What is Policosanol?
- High cholesterol, inherited high cholesterol (familial hypercholesterolemia), intermittent claudication, increasing blood flow to the heart in people with coronary heart disease, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96177
Rumalaya forte 30 pills order
The recip rocal dangers of stroke and cognitive impairment in an aged popula tion muscle relaxant tizanidine rumalaya forte 30 pills low cost. Lacunar infarcts defined by magnetic resonance imaging of 3660 aged folks: the Cardiovascular Health Study spasms during mri rumalaya forte 30 pills purchase without a prescription. Clinical correlates of white matter findings on cranial magnetic resonance imaging of 3301 elderly people. Prevalence and risk factors of silent mind infarcts in the inhabitants primarily based Rotterdam Scan Study. Incidence and risk elements of silent brain infarcts in the populationbased Rotterdam Scan Study. Cerebral microbleeds: a evaluate of clinical, genetic, and neuroimaging associations. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy maps to chromosome 19q12. Genetics and molecular pathogenesis of sporadic and hereditary cer ebral amyloid angiopathies. Apolipoprotein E epsilon 4 and cerebral hemorrhage related to amyloid angiopathy. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the american heart association/american stroke association. Confusion and memory loss from capsular genu infarction: a thalamocortical disconnection syndrome Dementia after ischemic stroke: a populationbased research in Rochester, Minnesota (1960�1984). Long time period cognitive transitions, rates of cognitive change, and predictors 50 51 52 53 54 fifty five fifty six 57 58 fifty nine 60 61 sixty two sixty three sixty four sixty five 66 67 of incident dementia in a populationbased firstever stroke cohort. Clinical and radiological determinants of prestroke cognitive decline in a stroke cohort. The contribution of medial temporal lobe atrophy and vascular pathology to cognitive impairment in vascular dementia. An post-mortem examine of the incidence of lacunes in relation to age, hypertension, and arterio sclerosis. Periventricular lesions in the white matter on mag netic resonance imaging within the elderly. A morphometric correlation with arteriolosclerosis and dilated perivascular areas. Pathophysiologic mechanisms in the growth of agerelated white matter adjustments of the mind. Incidence, manifestations, and pre dictors of worsening white matter on serial cranial magnetic reso nance imaging within the aged: the Cardiovascular Health Study. Progression of cerebral small vessel illness in relation to risk elements and cognitive consequences: Rotterdam Scan examine. Subcortical lacunes are related to government dysfunction in cognitively normal elderly. Multiple or combined cerebral microbleeds and dementia in sufferers with vascular threat elements. Recognition memory and verbal fluency differentiate possible Alzheimer illness from subcortical ischemic vascular dementia. National institute of neurological disorders and strokecanadian stroke network vascular cognitive impairment harmonization requirements. Multimodal markers of inflam mation in the subcortical ischemic vascular disease sort of vascular cognitive impairment. Clinicopathological validation examine of four units of clinical standards for vascular dementia. Understanding hippocampal sclero sis in the elderly: epidemiology, characterization, and diagnostic issues. Prevention of dementia in randomised double blind placebocontrolled systolic hypertension in Europe (SystEur) trial. The prevention of dementia with antihypertensive treatment: new evidence from the systolic hypertension in Europe (SystEur) study. Effects of blood stress decreasing with perindo pril and indapamide remedy on dementia and cognitive decline in sufferers with cerebrovascular disease. Plasma n3 fatty acids and the chance of cognitive decline in older adults: the atherosclerosis danger in communities study. Physical activity, cognitive activity, and cognitive decline in a biracial group population. Physical exercise and dementia threat within the aged: findings from a prospective Italian examine. Long time period effects of secondary prevention on cognitive perform in stroke sufferers. Efficacy and opposed effects of cho linesterase inhibitors and memantine in vascular dementia: a metaanalysis of randomised controlled trials. Visual evaluation of medial temporal lobe atrophy on magnetic resonance imaging: interobserver reliability. Prevalence estimates have various, however in a single research in the Netherlands, it was estimated at 2. Onset is most commonly in the sixth decade however has been described as early as the third decade and as late as the ninth [5]. Two years earlier than presentation, her personality gradually modified, and she or he began to swear more incessantly, would burp in public, and would speak to strangers about her sex life. She watched more television and when she was unable to work out the distant management would sit and stare at the clean display. She started craving candy foods and consuming complete luggage of cookies in a sitting and gained 30 kilos. She recognized that she had lost her job but mentioned it was because of unreasonable demands from her boss. On examination, she had elevated speech output and would use the identical phrases repetitively, however her speech was fluent and smart, and she or he followed advanced commands accurately. She would stare on the examiner for lengthy intervals of time and repeatedly interrupted the examination to inform jokes. Frequently, these are felt to be both psychiatric in nature or to symbolize a "midlife crisis" [9]. Typical early symptoms embrace disinhibition, apathy, lack of empathy, modifications in eating behaviors, and compulsive behaviors. A distinction between a disinhibited subtype and an apathetic subtype has been proposed [10], though these options are inclined to be coexistent.
Rumalaya forte 30 pills discount online
Post-surgical Disturbances in water excretion are a common explanation for morbidity following trans-sphenoidal surgical procedure muscle relaxant metabolism rumalaya forte 30 pills order. Although hypokalaemia is incessantly present in such patients and may contribute spasms trapezius rumalaya forte 30 pills buy low cost, the concentration defect additionally happens when plasma potassium focus is regular. When hyperglycaemia causes the quantity of filtered glucose to exceed the reabsorptive capability of the proximal tubule, important glycosuria results. As glucose acts as an effective osmole in the tubular fluid, it prevents the reabsorption of water within the collecting duct. This reabsorption is additional impaired by a comparatively low osmolality of the renal medulla (which usually acts as the driving pressure for water reabsorption). This may result from hyperalimentation, elevated catabolism, gastrointestinal bleeding, or recovery from transient renal failure (Lindner et al. Diuretics In rare circumstances, loop diuretics can result in hypernatraemia by interfering with the renal concentrating mechanism. Hypokalaemia In rats, hypokalaemia has been proven to scale back the variety of aquaporin water channels in the luminal membrane of the amassing duct (Marples et al. Although hypokalaemia is incessantly associated with polyuria, it rarely leads to hypernatraemia. Gastrointestinal water loss Prolonged diarrhoea and/or vomiting can result in the loss of water from the physique (Hartling et al. In osmotic diarrhoeas, however, the primary osmoles misplaced are natural compounds corresponding to lactulose. During extended vomiting, as happens in oncology patients throughout chemotherapy, oral water consumption is impaired, whereas insensible water loss continues, resulting in hypernatraemia (Berk and Rana, 2006). In vitro data have proven that water permeability decreases at higher luminal calcium concentrations (Earm et al. Cutaneous water loss Excessive sweating could trigger the body to lose large amounts of water that, if not changed, would lead to hypernatraemia. Usually, nonetheless, this water loss results in thirst and replenishment of lost fluids. Indeed, in collapsed marathon runners hyponatraemia is no less than as likely to happen as hypernatraemia (Kratz et al. Burn harm affects the skin integrity and its protection against fluid loss is lost (Pruitt, 1978). Therefore, severely burned sufferers need cautious and intensive fluid resuscitation. This is much more necessary, as a result of the presence of hypernatraemia in sufferers with burns adversely affects pores and skin grafts (Namdar et al. All states that increase the insensible loss of water through the pores and skin (and from the respiratory tract) put the affected person at threat of growing a hyperosmolar state. In all these circumstances hypernatraemia will solely develop if the patient is unable to drink freely. As vasopressinase is produced within the placenta, hypernatraemia is transient in this disorder (Aleksandrov et al. Osmotic diuresis If plasma osmolality is bigger than urine osmolality and the day by day osmole excretion rate is > one thousand mOsmol/day an osmotic diuresis is current. The subsequent step is to decide which solute is answerable for the noticed increase in osmole excretion. Hyperglycaemic hyperosmolarity is the best clinical example of a disorder in which osmotic diuresis causes hypernatraemia Gain of sodium In sufferers incapable of regulating their very own fluid intake, hypernatraemia can develop for quite a lot of causes (Lindner et al. Frequently, water depletion is accompanied by the lack of sodium and or potassium salts, resulting in true volume depletion. If considerable sodium acquire is current and the patient is fluid overloaded, remedy with giant quantities of hypotonic fluid could lead to pulmonary oedema. In such patients, natriuresis should be induced with (loop) diuretics, as discussed below. In patients with hypernatraemia because of water loss, urine output ought to be measured to determine if (persistent) polyuria is current. As the expected urine move could be low, in these patients (inappropriate) polyuria could be defined as a urine output > 30 mL/hour. It is important to take the effect of osmolytes other than sodium on plasma tonicity into account. Especially, the contribution of glucose to measured osmolality ought to be assessed, for the explanation that treatment of hypernatraemia with concurrent hyperglycaemia poses particular challenges. These patients generally receive isotonic intravenous fluids, but pass comparatively hypotonic urine. Treatment and end result In basic, inducing a positive web water balance treats hypernatraemia. In sufferers in whom the gastrointestinal tract is useful, this is greatest achieved with oral water intake. Intravenous water administration with glucose 5% options (dextrose; D5W) is proscribed by the quantity of glucose that can be metabolized. The therapeutic method to the sufferers ought to include the steps listed in Table 29. At presentation there are several questions one should ask earlier than embarking on a particular treatment. In acute hypertonicity, the mind has a lower osmolality than plasma, which finally ends up in shrinkage and in the end (in rare cases) cerebral haemorrhage. In acute hypernatraemia the mind has not had the time to respond to the hypertonic state by growing the quantity of intracellular osmoles. Most sufferers with hypernatraemia present within the emergency division and the time-course is normally uncertain. The main therapeutic implication of the distinction between acute and continual is that in acute/symptomatic hypernatraemia plasma osmolality ought to be lowered rapidly to avoid cerebral issues. In chronic hypernatraemia, nevertheless, overly bold reducing of plasma osmolality would result in cerebral oedema and demise due to mind herniation. Similar to suggestions in hyponatraemia, sufferers with hypernatraemia must be treated quickly only if severely symptomatic due to the rapid (< forty eight hours) improvement of hypernatraemia. Set the [Na] target In symptomatic sufferers, the first purpose is to induce a shift of water in the path of the brain, by rapidly reducing plasma osmolality. Start remedy to achieve the goal Replace water loss Calculating the water deficit can provide an estimate of the amount of water that has been lost: Water deficit = zero. The impact a litre of a given infusate could have on plasma sodium focus may be calculated using the formula developed by Adrogu� and Madias (2000): Table 29. In cachectic and/or elderly sufferers, this proportion can easily be as little as 40%. Using these calculations might result in over-estimation of water deficit with the subsequent hazard of over-correction. When estimating the correction charges with these formulae, no correction is made for ongoing (renal) water loss. The impact a given infusate will have on plasma [Na] can be estimated by calculating a tonicity steadiness, where each enter and output of sodium, potassium and water are calculated. When glycaemia is corrected, plasma sodium concentration should rise, as water returns to the intracellular compartment.
Purchase 30 pills rumalaya forte overnight delivery
Pulmonary manifestations essentially the most frequent extrarenal presentation is pulmonary involvement muscle relaxant definition 30 pills rumalaya forte purchase. Patients current with cough muscle relaxant generic names 30 pills rumalaya forte quality, dyspnoea, shortness of breath, and haemoptysis, though the severity can range widely-ranging from mild to life-threatening and requiring mechanical ventilation. The prevalence of pulmonary haemorrhage is reported from 50% to 90%, varying on different criteria for prognosis of pulmonary haemorrhage. Pulmonary haemorrhage presents sometimes as haemoptysis that might be episodic, varies from the trivial to torrential and is a poor reflection of the particular amount of pulmonary bleeding. In distinction with renal harm, lung illness exhibits a really poor correlation with antibody titre, although the autoantigen is present in alveolar in addition to glomerular basement membrane. This may mirror the dearth of direct contact between circulating antibodies and alveolar basement membrane (Jennings et al. It is consistent with the clear affiliation between pulmonary haemorrhage and cigarette smoking or exposure to other inhaled toxins, notably gasoline or different hydrocarbons (discussed additional in Chapter 74). Isolated lung illness is reported frequently, though haematuria is probably always current. Symmetrical parenchymal patchy shadows are proven with some confluent consolidation. The diagnosis of pulmonary haemorrhage presents few problems within the majority of patients, and difficulties only come up in the minority whose haemoptysis is absent. Other indicators include a sudden in any other case unexplained drop in haemoglobin and new shadows on the chest radiograph. This is probably the most sensitive and particular take a look at for fresh pulmonary haemorrhage (Ewan et al. Signs Physical examination can be normal in sufferers with gentle to average pulmonary haemorrhage, but the more severely affected are usually tachypnoeic and may be cyanosed. They might expectorate fresh blood and have rather dry-sounding inspiratory crackles on auscultation which may be most distinguished over the decrease lung fields and could also be accompanied by areas of bronchial respiration. Pulmonary pathology At autopsy of sufferers with pulmonary haemorrhage, the lungs are characteristically heavy, showing patchy congestion or haemorrhage. Histologically, intra-alveolar haemorrhage is accompanied by haemosiderin-containing macrophages, deposits of fibrin, and alveolar cell hyperplasia. Electron microscopy reveals thickening of the alveolar basement membrane, often with defects. Thickened alveolar partitions might present oedema, fibrosis, and modest inflammatory cell infiltration, primarily with polymorphs and lymphocytes. Immunofluorescence investigations are more difficult in the lung, however linear fixation of immunoglobulin could be detected at autopsy in patients with lung haemorrhage. Usually the shadows involve the central lung fields, with peripheral and upper-lobe sparing. Changes range from ill-defined nodules of dimension 1�4 mm to confluent consolidation with an air bronchogram. Indirect immunofluorescence assay utilizing sections of regular kidney is particular however not delicate and has been replaced by strong part immunoassays. False-negative immunoassay outcomes are most probably in sufferers with isolated pulmonary or low-grade/early renal illness. Rare non-IgG antibodies are recognized by direct immunofluorescence research of the renal biopsy. False-positive assays might sometimes be seen in states of polyclonal activation including other autoimmune situations. Other serologic checks corresponding to anti-streptolysin O, antinuclear antibodies, serum immunoglobulin and complement ranges, rheumatoid issue, cryoglobulins, and circulating immune complex are both adverse or regular. In such condition, the immunofluorescence might display segmental linear deposits or completely adverse. Role of endothelial injury and repair, induction of autologous section, and kinetics of antibody deposition in Lewis rats. Anti-glomerular basement membrane glomerulonephritis: a morphologic examine of eighty cases. Anti-glomerular basement membrane antibody disease in Japan: part of the nationwide quickly progressive glomerulonephritis survey in Japan. Comparison of 4 enzyme immunoassays for the detection of immunoglobulin G antibody towards glomerular basement membrane. Therapy of anti-glomerular basement membrane antibody disease: evaluation of prognostic significance of clinical, pathologic and therapy elements. Antiglomerular basement membrane antibody-mediated nephritis with regular pulmonary and renal function. Alveolar hemorrhage syndromes: diffuse microvascular lung hemorrhage in immune and idiopathic disorders. Long-term outcome of anti-glomerular basement membrane antibody illness treated with plasma change and immunosuppression. The clinical data and light-weight microscopic findings should assist make this distinction. Fibrillary glomerulonephritis: an entity with unusual immunofluorescence options. Rapidly progressive glomerulonephritis: analysis of prevalence and medical course. Antibasement membrane antibody disease with out scientific evidence of renal illness. Characteristics and prognosis of Chinese patients with anti-glomerular basement membrane disease. Characteristics and outcome of anti-glomerular basement membrane disease: a single-center expertise. The immunopathological spectrum of crescentic glomerulonephritis: a survey of 106 sufferers in a single Chinese middle. Anti-glomerular basement membrane disease: position of enzyme-linked immunosorbent assays in prognosis. IgA antiglomerular basement membrane illness related to bronchial carcinoma and monoclonal gammopathy. Glomerulonephritis with coexistent immune deposits and antibasement membrane exercise. Henoch-Schonlein purpura and pulmonary hemorrhage: a report and literature evaluate. Binding of anti-basement membrane antibody to alveolar basement membrane after intratracheal gasoline instillation in rabbits. However, it appeared that less severely affected individuals did relatively properly without plasma change. Retrospective analyses based on a massive quantity of patients provide useful data (Couser, 1988; Cui et al. The kidney consequence for this cohort was strongly influenced by kidney function at presentation. However, amongst patients who wanted dialysis at presentation, patient and kidney survival had been decreased to 65% and 8% at 1 year, respectively. Compared to nearly 100% mortality from pulmonary haemorrhage and kidney failure in historic collection, this treatment technique represent a major improvement and is broadly adopted in multiple centres.
Purchase rumalaya forte 30 pills with mastercard
Comparison of various measures of urinary protein excretion for prediction of renal events spasms just before falling asleep best 30 pills rumalaya forte. Creatinine clearance following cimetidine for estimation of glomerular filtration fee xiphoid spasms rumalaya forte 30 pills order on-line. Turbidimetric determination of proteins with sulfosalicylic and trichloracetic acids. Measurement of muscle mass in humans: validity of the 24-hour urinary creatinine method. Increased urinary neutrophil gelatinase related lipocalin levels in a rat mannequin of upper urinary tract infection. New micro-turbidimetric method for dedication of protein in cerebrospinal fluid and urine. Ueber den Niederschlag welchen Pikrinsa�ure in normalen Harn erzeugt und �ber eine neue response des Kreatinins. Urinary proteins enzymes as early indicators of renal dysfunction in persistent publicity to cadmium. Determination of reference intervals for serum creatinine, creatinine excretion and creatinine clearance with an enzymatic and a modified Jaffe method. Biological variation of cystatin C: implications for the evaluation of glomerular filtration fee. Defective urinary-concentrating ability due to a complete deficiency of aquaporin-1. Clinical utility of trace proteinuria for microalbuminuria screening within the general inhabitants. Circadian rhythm of proteinuria: penalties of the utilization of urinary protein: creatinine ratios. A simplified equation to predict glomerular filtration rate from serum creatinine [Abstract]. Modification of Diet in Renal Disease Study Group and the Diabetes Control and Complications Trial Research Group. Effect of food plan on creatinine clearance and excretion in young and aged healthy topics and in patients with renal disease. Urinary N-acetyl-beta-(D)-glucosaminidase activity and kidney damage molecule-1 degree are related to antagonistic outcomes in acute renal failure, J Am Soc Nephrol, 18, 904�12. Thyroid function in another way impacts serum cystatin C and creatinine concentrations. Microalbuminuria or micro-alpha-1-microglobulinuria: which one is healthier predictor of the development of the secondary nephropathy Liver fatty acid-binding protein as a biomarker of acute kidney harm after cardiac surgical procedure. Modified food regimen in renal disease technique overestimates renal function in selected elderly sufferers. The urine protein to creatinine ratio as a predictor of 24-hour urine protein excretion in sort 1 diabetic patients with nephropathy. Protective results of fosfomycin on cisplatin-induced nephrotoxicity in sufferers with lung most cancers. Cross sectional longitudinal research of spot morning urine protein: creatinine ratio, 24 urine protein excretion rate, glomerular filtration price, and finish stage renal failure in persistent renal disease in patients with out diabetes. A easy estimate of glomerular filtration rate in full-term infants through the first year of life. Glomerular filtration price through plasma iohexol disappearance: pilot research for persistent kidney disease in children. A simple estimate of glomerular filtration rate in youngsters derived from body size and plasma creatinine. N-acetyl-glucosaminidase and 2-microglobulin: their urinary excretion in sufferers with parenchymatous renal illnesses. A explanation for discrepancy between values for urinary protein as assayed by the Coomassie Brilliant Blue G-250 method and the sulphosalycilic acid technique. Effects of 5 completely different antisera on the immunoturbidimetric willpower of urinary albumin. Evaluation of urinary enzyme patterns in sufferers with kidney ailments and primary benign hypertension. Estimating equations for glomerular filtration fee in youngsters: laboratory concerns. Difference of carboplatin clearance estimated by the Cockroft-Gault, Jelliffe, Modified-Jelliffe, Wright or Chatelut method. A comparison of simplified and standard methods for the measurement of glomerular filtration fee and renal tubular perform. The Lund-Malm� creatinine-based glomerular filtration price prediction equation for adults also performs nicely in kids. An improved pyrogallol red-molybdate methodology for figuring out complete urinary protein. Activity and isoenzyme profile of N-acetyl-beta-d-glucosaminidase in urine from employees exposed to cadmium. An automated dry-slide enzymatic method evaluated for measurement of creatinine in serum. Follow-up of steroid-resistant nephrotic syndrome: tubular proteinuria and enzymuria. An accurate and fast technique for the willpower of proteins in small amounts of blood serum and plasma. Diagnostic accuracy of urine dipsticks for detection of albuminuria in the general group. Reevaluation of formulas for predicting creatinine clearance in adults and kids, utilizing compensated creatinine methods. Early prediction of urinary tract an infection with urinary neutrophil gelatinase associated lipocalin. The loop of Henle creates the countercurrent multiplication course of and the corticomedullary osmotic gradient (Morello and Bichet, 2001). In the distal convoluted tubule, the lumen osmolality decreases to 60 mOsm/kg H2O. The accumulating duct has extremely low water permeability in the absence of the antidiuretic hormone vasopressin. Under this situation, no water transport is noticed along the accumulating duct and the final urine is maximally diluted. In the presence of vasopressin, transepithelial actions of water occur throughout the principal cells. Aquaporin 2 is expressed on the apical plasma membrane exclusively within the presence of vasopressin, thus growing water permeability. The transepithelial distinction in osmolality drives water from the lumen to the interstitium.

Rumalaya forte 30 pills order mastercard
Volume expansion Extracellular fluid volume growth or contraction induces phosphaturia or decreases excretion of Pi muscle relaxant blood pressure purchase 30 pills rumalaya forte fast delivery. Genetic alterations resulting in spasms spinal cord buy discount rumalaya forte 30 pills on-line altered renal dealing with of Pi Genetic defects that alter renal Pi handling could be localized either in NaPi cotransporter genes or in genes coding for factors/cofactors that regulate proximal tubular reabsorption of Pi. Renal phosphate dealing with in human-what can we study from hereditary hypophosphataemias Secreted frizzled-related protein-4 reduces sodium-phosphate co-transporter abundance and exercise in proximal tubule cells. Characterization of transport mechanisms and determinants critical for Na+-dependent Pi symport of the PiT family paralogs human PiT1 and PiT2. Tumors related to oncogenic osteomalacia express genes essential in bone and mineral metabolism. Deciphering PiT transport kinetics and substrate specificity using electrophysiology and flux measurements. Differential expression, abundance, and regulation of Na-phosphate cotransporter genes in murine kidney. Inhibition by volume enlargement of phosphate uptake by the renal proximal tubule brush border membrane. Ablation of the Galnt3 gene results in low-circulating intact fibroblast development factor 23 (Fgf23) concentrations and hyperphosphatemia regardless of increased Fgf23 expression. Sodium-dependent phosphate cotransporters: classes from gene knockout and mutation studies. Renal phosphaturia throughout metabolic acidosis revisited: molecular mechanisms for decreased renal phosphate reabsorption. It plays an important role in skeletal mineralization and in all kinds of organic functions. Recommended dietary Ca2+ intake is 1000�1500 mg/day, depending on age (McCabe et al. Ca2+ homeostasis is regulated by three key mechanisms: intestinal and renal reabsorption, and bone turnover. This built-in hormonal response re-establishes serum Ca2+ and shuts off the negative suggestions loop; in contrast, a rise in Ca2+ level will increase Ca2+ excretion and bone storage (Peacock, 2010). Every day, roughly eight g of Ca2+ is filtered at the glomerulus, of which < 2% is excreted into the urine. Calcium distribution Most of the whole body Ca2+ (about 99%) is confined to the skeleton as Ca2+-phosphate complexes, primarily as hydroxyapatite, where it guarantees skeletal energy and, on the identical time, a continuously exchangeable store for the physique (Wang et al. Ca2+ regulates a spread of essential functions, together with extra- and intracellular signalling, muscle contraction, and nerve impulse conduction (Bootman et al. It comprises free ions (51%), protein-bound complexes (40%), and ionic complexes (9%). To stop Ca2+ toxicity, the concentration of serum ionized Ca2+ is intently maintained within the physiological range of 1. Non-ionized Ca2+ is bound to an array of various proteins and anions in both the extra- and intracellular swimming pools. The major Ca2+ binding proteins are albumin and globulin in serum, and calmodulin and different Ca2+-binding proteins in the cell. The major ionic complexes in serum are calcium phosphate, calcium carbonate, and calcium oxalate. The proximal tubule Along the proximal tubule Ca2+ transport is, in essence, an iso-osmotic process, energetically passive, proceeding via the paracellular pathway. Nevertheless, renal micropuncture experiments, carried out under experimental circumstances in which the driving drive for passive Ca2+ motion has been eradicated, demonstrate that 10�15% of the reabsorption is active, implicating a cellular pathway for this course of (Ullrich et al. Total proximal tubule reabsorption accounts for about 65% of total Ca2+ filtered at the glomerulus. Evidence has been offered indicating that Ca2+ transport is driven by the electrochemical gradient as a result of the recycling of potassium ions via the luminal membrane, appropriate with a passive absorptive process (Bourdeau and Burg, 1979). Serum Ca2+ homeostasis is set to keep extracellular ionized Ca2+ levels in the physiological vary. However, the contribution of energetic Ca2+ transport deserves further investigation (Hoenderop et al. Co-administration of chlorothiazide decreases furosemide-induced hypercalciuria, given acutely or chronically. About 65% of the filtered quantity of Ca2+ takes a paracellular route alongside the proximal tubule. This transport is especially paracellular, but some evidences suggest additionally a transcellular part. Finally some research report about 1% of filtered Ca2+ is reabsorbed along the collecting duct. After Ca2+ binding, calbindin-D28k facilitates the transport of Ca2+ to the basolateral membrane and operates as a dynamic Ca2+ buffer. The role of renal calbindin-D9k in compensating for impaired calbindin-D28k perform (and vice versa) needs additional investigations (Schlatter, 2006). The thiazide-induced calcium-sparing effect Thiazide diuretics, coupled with their natriuretic impact, are in a place to cut back urinary Ca2+ excretion. Thiazide-induced Ca2+ reabsorption takes place mainly along the proximal tubule and is driven by the rise in proximal Na+ reabsorption as a end result of thiazide-induced contraction of the extracellular circulating quantity (Bindels, 2010). A vesicular-mediated transcellular route for Ca2+ absorption has been recognized in chick enterocytes after stimulation with energetic vitamin D. Intracellular vesicles containing calbindin-D28k appear to shuttle Ca2+ through the cell. In duodenal chick enterocytes a fast Ca2+ efflux pathway has been described in response to acute stimulation with vitamin D. Intestinal calcium absorption Dietary Ca2+ consumption is important for systemic Ca2+ homeostasis. Ca2+ absorption occurs in the small gut by energetic (low dietary intake) and passive (high dietary intake) transport mechanisms. Active transcellular Ca2+ absorption is positioned largely within the duodenum and upper jejunum, whereas passive paracellular Ca2+ absorption happens throughout the entire length of the gut (Bronner et al. The effectiveness of this pathway is dependent upon the lumen-to-interstitium electrochemical gradient and the integrity of the intercellular tight junction complexes, and may be regulated by vitamin D (Fujita et al. However, how this mechanism directly contributes to serum Ca2+ homeostasis has not been fully clarified. Calcium absorption along the intestine requires both an lively (transcelluar) and passive (paracellular) transport. During physiological feeding situation, lively transport takes place, mainly, in the duodenum and within the first part of the jejunum, while passive transport occurs along the whole intestine (left side of the picture). Ca2+ release within the mineralizing space and proton removal are key steps for bone mineralization.