
Prazosin dosages: 5 mg, 2.5 mg
Prazosin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

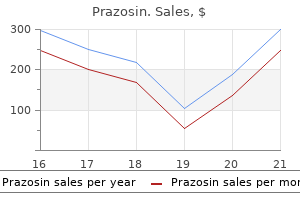
Order prazosin 2.5 mg fast delivery
Abdominal imaging: in the patient with unexplained dyspepsia where endoscopy is regular cholesterol levels myth cheap 2.5 mg prazosin amex, ultrasound could be helpful in certain clinical circumstances to investigate for biliary tract pathology cholesterol oxidation eggs 5 mg prazosin order overnight delivery. Atypical peptic ulcer: peptic ulceration in an uncommon location, peptic ulcers immune to remedy, an ulcer relapse after operation, or frequent or early ulcer recurrence can occur within the Zollinger�Ellison syndrome. This syndrome can additionally be associated with enlarged duodenal or gastric folds, or diarrhoea or steatorrhoea. The diagnosis is made by measuring the fasting serum gastrin level: > 300 pg / mL is suggestive and > 1000 pg / mL is almost diagnostic. Acid secretion may be confirmed by testing the pH of gastric juice obtained at endoscopy. The next diagnostic check of alternative in unsure cases is the secretin test (if available), the place a paradoxical improve in gastrin of > 200 pg / mL above basal ranges is highly specific. If the admission is because of acute gastrointestinal bleeding, then the treatment applied must be documented. Remember that survival is improved with oral or intravenous proton pump inhibitors and with transfusions only if the haemoglobin degree drops beneath 70 g / L. Therapy with acid suppression alone for peptic ulcer disease is now obsolete until no cause is identified. Patients with gastric ulcers could also be advised to have a repeat gastroscopy to affirm healing and exclude carcinoma. These embrace aged patients, those having their first three months of remedy, these on higher doses, these with a past historical past of peptic ulcer, those taking concomitant corticosteroid remedy or anticoagulants, and those with other critical medical diseases. In patients with metastatic or multifocal illness, surgery is avoided, however all other circumstances require surgical exploration. Other causes of hypergastrinaemia with acid hypersecretion embody a retained gastric antrum after peptic ulcer surgery, massive small bowel resection, gastric outlet obstruction and thyrotoxicosis. Splenomegaly in coeliac disease often indicates that lymphoma has sophisticated the illness because otherwise splenic atrophy is characteristic and manifests with Howell�Jolly our bodies in the peripheral blood smear. The examination Pay particular attention to the current weight and dietary status. Journal of the American Academy of Dermatology 2008; 60(2):277�88, with permission. Clinical options may embody weight loss, diarrhoea, stomach ache, arthralgias and steady rhythmic eye actions of eye convergence with masticatory muscle contractions. Check gastroscopy and small bowel biopsy (the optimal number for prognosis of coeliac disease is four duodenal biopsies, as disease could be patchy) and duodenal aspirate for histology, parasites and bacterial overgrowth; search for a quantity of duodenal ulcers. Note that tissue transglutaminase (or anti-endomysial antibody) is the most useful screening test for sprue. Remember that 2% of the inhabitants is IgA deficient and could have negative serology, so verify IgA ranges if testing is negative and your suspicion is high. Vitamin B12 absorption may be abnormal in ileal illness, bacterial overgrowth, pernicious anaemia and pancreatic disease. Falsely low values happen in sufferers with chronic kidney illness, dehydration, ascites or hyperthyroidism and within the aged. Greatly raised faecal fats ranges (> forty g per day) strongly recommend pancreatic disease, but this check is now uncommonly obtainable. Treatment Treatment depends on the cause and in addition entails the replacement of essential vitamins (Table 7. Have a low threshold for ordering serology; patients might current with no gastrointestinal symptoms. Find out about signs at presentation and, if relevant, the current reason for admission. Symptoms usually enhance in weeks and histology in months; tissue transglutaminase antibody normalises in 3�6 months. It is affordable to re-biopsy the duodenum in 3 months to affirm histological healing. Lack of response to a gluten-free food regimen could additionally be caused by inadvertent gluten exposure, the presence of one other problem. Pneumococcal vaccine is beneficial due to the hyposplenism of coeliac illness. Anaemia (owing to continual illness, iron deficiency, ileal involvement, haemolysis from sulfasalazine or microangiopathy) b. Anorectal illness (including anal fissures or fistulas, pararectal abscess or rectovaginal fistula) 2. Renal disease includes urate and calcium oxalate stones, pyelonephritis (owing to fistulas), hydronephrosis (ureteric obstruction), amyloidosis four. Osteomalacia Determine the investigations at the time of presentation and subsequently (and notably whether or not infectious causes had been considered). Ask whether or not common follow-up colonoscopy has been carried out in patients with longstanding colitis. The causes embrace amoebiasis (diagnosed by rectal mucosal scraping or warm stool examination), Shigella, Salmonella, Yersinia, Campylobacter, Escherichia coli 0157:H7 and pseudomembranous colitis (Clostridium difficile toxin). Plain abdominal X-ray film: you will need to search for bowel wall thickening (oedema), gaseous distension and proof of poisonous megacolon in ulcerative colitis. Blood depend: verify for anaemia (caused by chronic disease, blood loss, macrocytic anaemia in ileal illness, or haemolytic anaemia from an autoimmune course of, 1. Inflammatory bowel illness Infections, together with pseudomembranous colitis Radiation Ischaemic colitis Diversion colitis (colonic loops excluded from the faecal stream) Toxic publicity. For the investigation of inflammatory bowel illness, the following ought to be thought-about. Other helpful indices of severity are anaemia, hypoalbuminaemia and acute-phase reactants. In an acute assault, keep in mind to correct hypokalaemia and keep away from barium enema to prevent poisonous megacolon or perforation. In severe colitis, intravenous broad-spectrum antibiotics (including metronidazole) are normally given. Intravenous steroids are the mainstay of therapy in sufferers with moderate-to-severe disease. In mild-to-moderate illness, sulfasalazine is beneficial; mesalazine is the energetic agent, whereas sulfapyridine is the trigger of most intolerance (allergic reactions such as pores and skin rash � including Stevens�Johnson syndrome � and Heinz body haemolytic anaemia; and side-effects such as nausea, headache, folate deficiency and reversible male ht tp:// eb oo ks m ed ebooksmedicine. Liver function exams and blood levels of electrolytes, urea and creatinine: these patients could develop liver illness. Note any decreased mucosal translucency, loss of vascular pattern, granular and friable mucosa, hyperaemia, ulceration and pseudopolyps in the report. Mucus depletion and prominent crypt abscess formation are more suggestive of ulcerative colitis. If high-grade dysplasia is confirmed in the absence of extreme irritation, colectomy is indicated. A multidisciplinary group approach is needed to manage what is often a devastating disease in the long term. Sulfasalazine or mesalazine is more practical in colonic disease, whereas steroids are more effective in small bowel illness.
Prazosin 2.5 mg buy mastercard
Patients with a thrombophilic defect keep cholesterol levels low prazosin 2.5 mg order, however and not utilizing a family history of thrombosis cholesterol lowering foods wine prazosin 5 mg buy on-line, have solely a barely increased risk. Ask about other factors that may improve thrombotic threat, together with smoking, oestrogen-containing oral contraceptives, being pregnant, malignancy, latest surgical procedure and immobility. Long aeroplane flights are controversial as a threat factor, but have received in depth discussion within the in style press. If the event has followed a surgical operation, ask what prophylaxis was used to attempt to stop thrombosis. This may be associated with the presence of antiphospholipid antibodies, that are autoantibodies towards varied platelet floor molecules, together with phospholipids. The prevalence of myocardial infarction in young girls with regular coronary arteries has been associated with issue V Leiden mutation. Damage to the venous system could cause persistent oedema and ulceration that could be quite disabling (post-thrombotic syndrome). Ask in regards to the congenital abnormality, homocysteinuria, which is associated with a Marfanoid habitus and premature strokes and coronary artery illness. Ask about previous and family history of malignancy and former screening tests carried out. In young girls previous to commencing hormonal contraception � that is controversial gated, as set out under. The abnormality is brought on by a point mutation that affects the cleavage website on the activated molecule. The mutation occurs in 4% of the general population in Australia and in as a lot as 50% of people with a household historical past of recurrent venous thrombosis. The heterozygous state is related to an eightfold enhance in venous thrombotic danger; the homozygous state also occurs and these individuals have a hundred times the common danger. The thrombotic threat is greater for ladies with this condition due to the extra danger related to pregnancy and the utilization of oral contraceptives containing oestrogen. Use of these medicine causes a 35 times increased danger of a thrombotic occasion (approximately a 3% danger over 10 years). Antithrombin deficiency is current in a light kind in about 1 in 2000 of the inhabitants. The thrombotic threat is somewhat unpredictable, but the prevalence of a first thrombotic event in these patients is a relative indication for lifelong anticoagulation remedy with warfarin. Their deficiency is related to recurrent venous thrombosis and pulmonary embolism, however the stage of elevated danger is less clear than that for the abnormalities above. There is overlap between the serum levels in individuals with, and apparently with out, an elevated danger of thrombosis. Tests for the vitaminK-dependent proteins C and S must be performed earlier than the affected person is begun on warfarin. All patients with thrombophilia and their affected asymptomatic relatives want aggressive prophylaxis earlier than surgical procedure or during times of immobilisation. Surgical prophylactic therapy ought to embody heparin, compressive stockings and foot pumps, and early mobilisation. They could profit from basic measures (frequent ambulation, hydration and calf exercises) in addition to graduated compression stockings. It is an autosomal dominant trait and results in a fourfold improve in the threat of venous thrombosis. Homocysteine degree is an impartial threat issue for coronary artery disease and may play a role in venous thrombosis in sure patients with inherited enzyme deficiencies in homocysteine metabolism. The test for genetic mutation is available, however usually not indicated for venous thrombosis alone. Combined thrombophilic abnormalities are relatively frequent and further improve the thrombotic danger. Anticardiolipin antibodies and lupus anticoagulant (IgG or IgM antiphospholipid) antibodies are associated with an elevated danger of venous thrombus and arterial embolus. The transient presence of those antibodies at low titres is widespread, is usually associated with infection and might be not of scientific significance. The detection of antiphospholipid antibodies in girls with miscarriages is an indication for treatment with low-molecular-weight heparin with or with out lowdose aspirin during being pregnant. Patients must be advised strongly in opposition to smoking and may keep away from oestrogen-containing oral contraceptives. Polycythaemia rubra vera Myelofibrosis Essential thrombocythaemia Chronic myeloid leukaemia Chronic eosinophilic leukaemia, continual neutrophilic leukaemia Systemic mastocytosis the history the patient will most likely know the diagnosis. Primary polycythaemia vera, or polycythaemia rubra vera (erythraemia or elevated red cell mass), is the most typical myeloproliferative disease. Stress polycythaemia nt er na l-m ed ic in e- vi de os eight � the haematological long case 195 the examination 1. M R Howard, Haematology: an illustrated colour text, 32:64�5, Elsevier, 2013, with permission. Look for scratch marks and bruising on the arms and take the blood pressure (systolic hypertension accompanies an increased purple cell mass and phaeochromocytoma is related to elevated erythropoietin). Look at the eyes for injected conjunctivae and study the fundi for hyperviscosity modifications. Examine the cardiovascular system for indicators of cyanotic congenital coronary heart illness, if applicable, and the respiratory system for indicators of chronic lung disease. Examine the stomach for hepatomegaly (hepatoma have to be excluded) and more importantly splenomegaly, which occurs in 80% of instances of polycythaemia rubra vera, but not in secondary polycythaemia. Look on the legs for scratch marks (pruritus may be secondary to elevated plasma histamine levels), gout and evidence of peripheral vascular disease. Auscultate over the cerebellar areas for a bruit (cerebellar haemangioblastoma). Note any higher motor neurone indicators (cerebrovascular disease because of thrombosis or the hyperviscosity syndrome). Patients are t/i nt er na l-m ed ic in e- vi de os 196 Examination Medicine Investigations Confirm the presence of polycythaemia (haematocrit > 60% for men or > 56% for women) and establish whether or not this is primary or secondary. Remember that erythrocytosis is a rise within the absolute purple cell mass, which happens as a outcome of some stimulus (usually hypoxia), and erythraemia (polycythaemia vera) is a rise in purple cell mass of unknown aetiology (Table 8. Serum erythropoietin degree is often considerably lowered or absent in polycythaemia vera and elevated in secondary polycythaemia. Remember, nevertheless, that certain tumours (haemangioblastoma, renal cell carcinoma, renal sarcoma and carcinoma of the liver) trigger polycythaemia by excreting erythropoietin. The condition is frequently identified following a routine full blood count or the discovery of splenomegaly. Myelofibrosis can also be the outcomes of numerous malignant and non-malignant circumstances (Table 8. Median survival is 4�5 years, but sufferers with extreme anaemia (< 100 g / L), older age, constitutional signs and leukocytosis have a worse prognosis (median survival about 2 years). Thrombotic risk can usually be decreased with phlebotomy alone, however aspirin is often thought to give additional protection.
Syndromes
- Is younger than 3 months old and has a rectal temperature of 100.4 °F (38 °C) or higher
- Fecal incontinence (during sleep)
- Medications that suppress the immune system
- Never leave a campfire unattended.
- Broccoli, cauliflower, carrots, collard and other greens, cucumbers, green beans, kale, lettuces, potatoes, radishes, spinach, squash, sweet potatoes, tomatoes
- You have gastroesophageal reflux disease and aspiration pneumonia (a lung infection caused by breathing the stomach contents into the lungs), a chronic cough, or hoarseness.
- Anti-inflammatory medicines to reduce inflammation and swelling
- Urology -- disorders of the male reproductive and urinary tracts and the female urinary tract
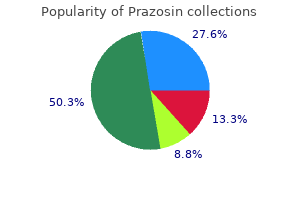
Order prazosin 2.5 mg online
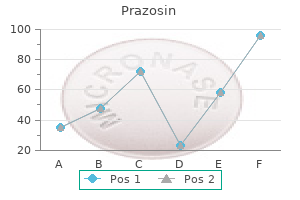
Given the > 50% area inside the endometrial cavity american heart association cholesterol ratio guidelines prazosin 2.5 mg buy visa, this leiomyoma must be amenable to hysteroscopic resection myth of cholesterol in eggs buy prazosin 5 mg online. Saline contrast hysterosonography in irregular uterine bleeding: a systematic review and meta-analysis. Transvaginal sonography mixed with saline contrast sonohysterography to consider the uterine cavity in patients with irregular uterine bleeding and postmenopausal endometrium more than 5 mm. Evaluation of the lady with postmenopausal bleeding: Society of Radiologists in Ultrasound-Sponsored Consensus Conference statement. Some of the locules inside the best ovarian lesion comprise highattenuation materials because of hemorrhage or excessive protein content. Note the peripheral location of follicles, which outcomes in a string of pearls look. Note the diffuse low signal depth of the ovarian parenchyma in between the small parenchymal cysts. Note that some locules demonstrate very low signal depth, a characteristic feature of struma ovarii. Note also diffuse subcutaneous edema resulting from increased capillary permeability. The bright dot signal represents aneurysmally dilated vascular constructions and is commonly seen in yolk sac tumors due to its high vascularity. Imaging features of complex stable and multicystic ovarian lesions: proposed algorithm for differential prognosis. Ovarian malignant germ cell tumors: mobile classification and scientific and imaging features. Updated ultrasound criteria for polycystic ovary syndrome: dependable thresholds for elevated follicle inhabitants and ovarian volume. There is a curvilinear peripheral septation, which signifies that the ovum is surrounded by a cumulus o�phorus throughout the mature follicle. The floating part has high sign depth, much like that of subcutaneous fats, whereas the dependent part has low signal intensity similar to that of simple fluid. Mucinous cystadenomas may show locules of excessive T1 signal depth because of their mucin contents. The mass demonstrates homogeneous low signal depth relative to pelvic muscles. The mass reveals low echogenicity with dramatic sound attenuation resulting in posterior acoustic shadowing. The mass is hyperintense relative to muscle with hypointense septa separating the mass into a quantity of lobules. Note additionally the circumferential thickening of the wall of the terminal ileum in this patient with Burkitt lymphoma. Hematopoietic tumors of the feminine genital system: imaging options with pathologic correlation. Imaging of gynecological illness (3): medical and ultrasound characteristics of granulosa cell tumors of the ovary. Enhancing vessels are seen bridging from the uterus to the mass (bridging vascular sign), which help establish the uterine origin of the mass. An eccentric low signal depth blood clot is current within the excessive signal intensity component. An eccentric high signal intensity blood clot is current throughout the larger signal depth part. Most of the loculi show high sign intensity; few show very low signal depth. The enlarged ovary demonstrates elevated sign intensity apart from a segmental space of very low sign at the periphery. This case demonstrates the development of ovarian fibromatosis in massive ovarian edema. Imaging in gynecological illness (5): scientific and ultrasound characteristics in fibroma and fibrothecoma of the ovary. Imaging of gynecological disease (4): medical and ultrasound characteristics of struma ovarii. Chapter 5 the cardiovascular long case ic A rule of thumb in the matter of medical recommendation is to take every thing any doctor says with a grain of aspirin. The whims of the long-case examiners could lead to concentrated questioning in regards to the ischaemic coronary heart illness of a patient in hospital for the management of, say, renal transplant rejection. These patients are extra doubtless to present administration rather than diagnostic problems as soon as they attain the standing of long-case patients. The prognosis unstable angina is not a half of this classification, however is still usually used to describe patients with increasing exertional angina. The presence of irregular cardiac markers indicates an adverse prognosis (increased risk of further infarction or death) and these sufferers profit from early however not immediate intervention (angioplasty or coronary surgery) and from instant aggressive anti-platelet treatment and anticoagulation with fractionated or unfractionated heparin. The concept of danger stratification relies on these elements and determines the urgency and sort of treatment. Find out whether or not the affected person has been or is in hospital because of a recent myocardial infarction or an acute coronary syndrome, or for some other cardiac or non-cardiac reason. Clearly, these might symbolize completely different pathophysiological states, various from occlusion of a coronary artery and insufficient collateral flow to rupture of a lipid-rich plaque with thrombus formation. Ask about obvious precipitating elements, such as a gastrointestinal bleed or the onset of an arrhythmia. Also ask concerning the character of the chest ache and what precipitated the admission. You must be suspicious of the analysis until it has been confirmed by investigations. Acute coronary syndromes are managed with heparin and aspirin and clopidogrel, prasugrel or ticagrelor. Most patients have early angiography (within forty eight hours) with the intention of angioplasty to the offender lesion if this is practical. Ask whether the affected person is conscious of details of what investigations or remedy have been performed. If the affected person has had an infarct during this or earlier admissions find out in regards to the administration, which may have included main angioplasty or thrombolysis, ht tp:// eb oo ks m ed ebooksmedicine. The threat is higher in every group for patients with previous ischaemic coronary heart illness or diabetes. In many hospitals a comprehensive cardiac rehabilitation program may have been offered to the affected person. Remember that danger elements are of important significance to long-term prognosis, but add little to the probability that undiagnosed chest pain is ischaemic. There is some proof that statins have beneficial effects beyond their impact on cholesterol levels (pleotrophic effects). Cardiac catheterisation is maybe probably the most memorable of the investigations for ischaemic heart illness. The patient may know what number of coronaries are abnormal and whether or not angioplasty was performed.
5 mg prazosin purchase overnight delivery
Examine the mouth for ulcers and gum illness and the teeth and tonsils for infection myth of cholesterol in eggs buy 2.5 mg prazosin with visa. Exploratory laparotomy when all other exams are adverse and within the absence of any evidence of stomach illness is often unproductive cholesterol risk calculator 2.5 mg prazosin buy with visa. As traditional for lengthy circumstances, the candidate should find out what signs or issues are presently affecting the patient. These must be assessed in the context of potential longstanding disease affecting many systems of the body. This is particularly necessary in helping predict the likely level of immunosuppression. There have been complaints from long-case patients that this has been dealt with insensitively. Find out about symptoms of a attainable seroconversion illness in the past (Table 13. This is now typically a persistent disease and sufferers are getting older and prone to have problems such as ischaemic coronary heart illness. The candidate might be expected to show a logical method to the case and, of course, show a sympathetic angle to the patient with this chronic disease. There must be a strong emphasis in the dialogue on the psychological and social results of the sickness. If the patient is believed to have a fever brought on by a drug � a drug fever � it may be price stopping the drug or using an alternate one. There is often some combination of the next symptoms: � fever � vomiting � lymphadenopathy � diarrhoea � maculopapular rash � headache � arthralgia � meningism � myalgia � weight reduction � pharyngitis � oral candidiasis � nausea Ask about the mode of acquisition of an infection. Co-morbidity differs between subgroups, so specific questions about risk elements are essential. Contact tracing must be talked about and the potential for an infection of sexual partners with out their data addressed. The lesion is reddish-brown because of its vascular nature and accompanying haemosiderin deposition. Find out about antiretroviral drug and antibiotic remedy and about any antagonistic effects of these. If the disease has just lately been diagnosed, ask what treatment options have been discussed with the patient. Amprenavir Diarrhoea, nausea, perioral paraesthesia, lipodystrophy, insulin resistance ne Nelfinavir Diarrhoea, lipodystrophy, insulin resistance, hepatitis t/i Saquinavir Diarrhoea, lipodystrophy, insulin resistance, hepatitis nt er Indinavir Nausea, diarrhoea, lipodystrophy, insulin resistance, hepatitis, renal calculi, hair and nail changes na C. False positives can happen related to current vaccinations, different viral infections ht tp:// eb oo ks m ed ebooksmedicine. Other checks are used to assess the severity of the sickness and immunocompromise, and to search for associated conditions. The presently related exams will depend on the medical presentation; nonetheless, sure tests are essential for all patients, either as a baseline or for monitoring (Table thirteen. Herpes simplex prophylaxis with acyclovir and Candida prophylaxis with fluconazole or ketoconazole are appropriate for prevention after one episode has occurred. Drugs must be used solely together to ht tp:// eb oo ks m ed ebooksmedicine. Serial full blood counts and biochemistry will help assess any complications of illness or remedy. Resistance testing is indicated for the treatment of the naive affected person, or if therapy is failing and shall be modified. Treat the mom with zidovudine as an infusion throughout labour, and deal with the infant for six weeks. Surveillance for the event of hepatic carcinoma can be indicated for these patients. Special care with drug monitoring is critical if the patient has cirrhosis; zidovudine and didanosine should be avoided. Disseminated cytomegalovirus an infection � retinitis, gastrointestinal disease m ed ebooksmedicine. Patients whose disease is properly controlled by antiviral agents are extra doubtless to die of heart problems than infection. Hyperlipidaemia must be handled with pravastatin (which has less interaction with antiviral drugs). If one of the examiners is a geriatrician then questions on this topic are very doubtless (from the other examiner). Measure the time it takes the affected person (wearing their common shoes and with any aides) to stand up from a chair, stroll three metres, turn round and walk back, then sit. With the patient back in bed, perform cerebellar testing and search for peripheral neuropathy. Does the affected person undertake risky activities: climbing ladders, clearing gutters, and so on. Has there been a analysis of osteoporosis (increased danger of fracture attributable to a fall) Has the patient misplaced confidence as a outcome of falls and is this affecting his or her capability to depart the house, drive, shop, and so forth. Even when obesity is a minor a part of the lengthy case, candidates have to have a believable method to the issue. Treatment of vitamin-D-deficient sufferers with dietary supplements reduces the chance of falls by 14%, most likely by enhancing muscle strength and gait. Assessment of house (hazards in the home account for as much as 50% of falls); elimination of free rugs and installation of ramps, bars, and so on. Ways of encouraging train embody: pedometer, health watch, gymnasium program, exercise class. Remember that exercise alone has modest results on weight loss however can help maintain weight lost. Reduce food intake � reduction of food intake by 2000�4000 kilojoules a day will cause 400�500 g of weight loss every week. A very low calorie food regimen could also be considered for a affected person requiring speedy weight reduction. Remember that no specific weight loss food plan has been shown to be higher than some other, but enthusiasm for a particular food regimen could additionally be priceless. Ask about problems related to weight problems and their effect on ability to exercise and on normal actions: a. Roux-en-Y gastric bypass can be dramatically efficient and has been proven to scale back complications of weight problems; late issues of gastric bypass can embrace anastomotic stricture, bowel obstruction, marginal ulcer, hernia, and malabsorption with vitamin deficiency. Co-morbidities (most may have been covered during the basic historical past taking): a. Beta-blockers, if wanted, must be commenced some weeks earlier than surgery at a low dose and adjusted upwards as tolerated.
Order 5 mg prazosin visa
These axon bundles cholesterol lowering foods ireland prazosin 5 mg cheap with amex, known as the fila olfactoria cholesterol kidney stones 5 mg prazosin cheap mastercard, cross via foramina within the cribriform plate of the ethmoid bone and enter the cranial cavity. There they unite to kind the olfactory nerve and cross to the olfactory bulb within the mind, the primary olfactory middle. The latter is connected via the olfactory tract to the secondary olfactory heart (olfactory cortex) within the temporobasal cortex, which is liable for the notion of smells and their association with different sensory impressions. The secondary olfactory center additionally has projections to the limbic system that join with the autonomic centers within the thalamus and hypothalamus; this creates a pathway that mediates the emotional and affective phenomena which might be related. The lamina propria additionally accommodates serous glands (olfactory glands) and vessels. The microvilli more than likely represent further chemoreceptors in the olfactory epithelium, which perform their function along with the basic receptor cells. Recent research have proven that the secretion layer on the epithelium incorporates a specific protein that has a excessive affinity for most odorous substances, and thus could facilitate and even mediate their binding to the sensory cells. The olfactory cortex has connections with the tertiary olfactory facilities (including the hippocampus, anterior insular region, and reticular formation), which are believed to have polysensory associative capabilities. Respiratory nasal mucosa Epithelium b Glands Venous sinusoids Cilia Microvilli a Structure of the lamina propria in histologic section. As the edge of the respiratory tract in humans, the nose is of main importance in conditioning the air earlier than it reaches the lower airways. To understand this advanced process, we must know something about the physics of nasal airflow, which also impacts the warming and humidification of the inspired air. Due to its exposed position, the nasal mucosa is in fixed main contact with the surroundings and thus with quite so much of potential pathogens. As a end result, the nostril is provided with a variety of defense mechanisms (mechanical defenses, specific and nonspecific immune responses). As part of the supraglottic vocal tract, the nose also contributes to speech production (see 18. Finally, the nostril accommodates the olfactory sensory cells, giving it an important function in olfaction (see p. Physical Principles of Nasal Airflow During inspiration, the air stream enters the nasal vestibule in an oblique vertical direction. When the impressed air reaches the nasal valve located between the vestibule and nasal cavity, it passes through the narrowest site in the upper respiratory tract (limen nasi). Just past the nasal valve, the crosssection of the airway turns into greatly expanded, making a "diffuser impact" that transforms most of the laminar circulate of the inspired air into turbulent move, by which completely different air layers are swirled together. Besides the rate of the air, the degree of change in airflow characteristics at this stage is very strongly influenced by the specialised anatomy of the nasal cavity, which is subject to substantial particular person differences. Septal deviation and cartilaginous or bony spurs on the septum could be as important on this regard as turbinate hyperplasia or septal perforation. To a level, the transition from laminar to turbulent move within the nostril is functionally desirable because it slows the flow velocity of the inspired air. This prolongs its contact with the nasal mucosa, contributing to olfaction and making it simpler for the nose to clear, humidify, and heat the impressed air (see below). Conditioning of the Inspired Air Inspired air is warmed and humidified in the nostril before reaching the lower airways. Turbulent circulate and other particular physical situations promote the required contact of the impressed air with the nasal mucosa. Moreover, the favorable relationship between the comparatively small nasal cavity and the comparatively massive mucosal surface area, which is further enlarged by the turbinates, also promotes the functionally necessary interplay between the impressed air and the mucosa. Humidification is completed by secretion and transudation from the nasal glands, the epithelial goblet cells, and the vessels of the lamina propria. Temperature regulation is managed by the intranasal vascular system and especially the venous erectile tissue, which is especially plentiful in the inferior turbinates. The temperature within the anterior portions of the nasal cavity is lower than in the posterior areas. This temperature gradient produces a gradual warm- Nasal Cycle the "nasal cycle" is a physiologic phenomenon marked by an alternation between luminal narrowing and widening of the nasal cavities. This alternate congestion and decongestion of the nasal mucosa is effected primarily through reactions of the venous capacitance vessels of the inferior and center turbinates, that are regulated by the autonomic nervous system. The warming capability of the nasal mucosa is so environment friendly that even with ambient temperatures below zero, the temperature of the inspired air is raised by 25 C on entering the nasopharynx, with a relative humidity of over 90%. Disturbances within the conditioning operate of the nose may result from age-related drying of the mucosa due to involution of the goblet cells and glands. They also can result from continual inflammatory adjustments or in depth resections of the mucosa throughout intranasal surgical procedure. Nonspecific Defense Mechanisms Mechanical defenses: the most important mechanical defense mechanism of the nasal mucosa is the mucociliary apparatus, which bodily cleanses the inspired air. The mucociliary transport system consists of the cilia of the respiratory epithelium and a mucous blanket composed of two layers: a deeper, much less viscid "sol layer" during which ciliary motion happens, and a superficial, more viscid "gel layer". Disturbances of mucociliary transport can have numerous causes, similar to elevated viscosity and thickness of the periciliary sol layer, hampering ciliary movements, or modifications within the viscoelasticity of the gel layer leading to ineffectual mucus transport. Finally, various pathogenic mechanisms can produce changes in the cilia themselves, whatever the viscosity of the mucous blanket. For example, an acute viral infection of the higher respiratory tract can result in desquamation of the epithelium, with a lack of ciliated cells. Also, certain micro-organisms can directly have an effect on ciliary motility by reducing the beat frequency of the cilia. Finally, ciliary dyskinesia syndromes are congenital issues based mostly on morphologic changes within the cilia such as absence of the dynein arms. This ends in uncoordinated, dyskinetic ciliary actions that prevent efficient mucus transport (see also Paranasal Sinus Inflammations). Nonspecific protective components: the nasal mucosa also has a variety of other, nonspecific defense mechanisms within the form of protective factors in the mucous blanket (Table 1. The superficial gel layer is propelled toward the nasopharynx by a coordinated but metachronous beating of the cilia. The dynamics of ciliary movement has been likened to a "field of grain swaying within the wind. Cellular defenses: the mucosa has nonspecific defense mechanisms on the cellular degree as nicely. The predominant phagocytic cells are neutrophilic granulocytes, monocytes, and macrophages. Specific Immune Responses Besides the nonspecific defense mechanisms of the nasal mucosa noted above, the nostril possesses a particular immune system that can be seen as a separate immunologic unit. The local, particular immune system of the nasal mucosa relies on the actions of antibodies, that are liable for the humoral immune response, and of 12 I Nose, Paranasal Sinuses, and Face Table 1. Finally, the endothelial cells of the blood vessels play an essential role within the particular immune responses of the nasal mucosa.
5 mg prazosin best
Acute situations affecting the perinephric space: imaging anatomy cholesterol levels reduce naturally discount prazosin 2.5 mg without a prescription, pathways of illness unfold cholesterol levels in quail eggs 2.5 mg prazosin discount otc, and differential analysis. Neoplastic and non-neoplastic proliferative problems of the perirenal space: cross-sectional imaging findings. Cortical calcifications of renal allograft are related to a nonfunctional, failed transplant. The calcifications are dystrophic and are discovered within the healed section of the disease. Primary hyperparathyroidism is the most common cause of medullary nephrocalcinosis in adults. Approximately 5% of patients with main hyperparathyroidism develop medullary nephrocalcinosis. Note the intensive posterior shadowing that obscures the posterior facet of the kidney. Unlike medullary sponge kidney, medullary nephrocalcinosis because of hyperparathyroidism and renal tubular acidosis is usually very dense. Note the cortical scarring overlying the medullary calcifications and the dilated calices, all due to continual reflux and infection. The tiny calcifications within the dilated tubules are more difficult to acknowledge on this excretory part picture. The presence of similar tissue in retroperitoneal lymph nodes helps to establish this as renal and perirenal lymphoma. This is contiguous with and of similar appearance to the renal sinus fats, an appearance appropriate with a renal junction line. Lipid-producing necrosis or osseous metaplasia might account for the fat/calcification that not often happens inside renal cell carcinoma. Amorphous debris is current within the higher pole calices, and all calices are clubbed. The calices are additionally dilated in this affected person who was born with extrophy of the bladder, repaired in infancy. Note the obstructing renal calculi and irritation extending into the perirenal house. The renal pelvis is dilated as a result of extrinsic invasion of the proximal ureter; this is leiomyosarcoma of the kidney. Neurogenic tumors commonly arise alongside the retroperitoneal path of the sympathetic ganglia. Emphysematous pyelonephritis is a life-threatening an infection with general mortality starting from 1150%. Infarction adopted tried partial nephrectomy, sophisticated by renal arterial occlusion. Gas within the nondependent calices is because of the catheter, not an infection or infarction. The proper kidney is in the corticomedullary part, whereas the left is in nephrographic part of enhancement. Note the delayed left nephrogram: the unaffected left kidney continues to be in a corticomedullary section, whereas the best kidney is in a nephrographic part. More inferior photographs demonstrated invasion of tumor into the left ureter (not shown). The unilateral delayed nephrogram is due to a mix of renal vein, artery encasement, and ureteral obstruction. Signs of sepsis, pyuria, and flank pain helped to affirm the analysis of acute pyelonephritis. Note the absence of significant hemorrhage, which helps to exclude arterial avulsion or deep parenchymal laceration. Case report: rhabdomyolysis following grand mal seizures 3064 presenting as a delayed and more and more dense nephrogram. Striated and wedge-shaped lesions indistinguishable from acute pyelonephritis on imaging Clinical setting: Patient with recognized autoimmune (collagen vascular) disease � Episodes of symptoms referable to visceral ischemia or spontaneous hemorrhage � Multiple Myeloma Collecting tubules could also be plugged with excreted myeloma protein Imaging findings much like acute pyelonephritis � But scientific presentation could be very totally different (no fever; recognized or simply confirmed myeloma) � Rhabdomyolysis Release of massive amounts of myoglobin into serum from damaged skeletal muscle might block renal tubules � Clinical: May cause acute renal failure � Imaging: Decreased or striated nephrogram, often bilateral Clinical setting: Crush injury, muscle trauma, certain drug results � Especially drug overdose with prolonged muscle hypoxia � Renal Cell Carcinoma Or other tumors (metastases, lymphoma) May have wedge form but are often spherical � Do not expect striated nephrogram Clinical setting: Incidental discovery (renal cell carcinoma) or flank pain, hematuria � Metastases and Lymphoma, Renal Primary tumor is usually recognized Extrarenal tumor is usually evident � Radiation Nephritis Wedge form correlates with field of external beam � Radiation remedy to midline structures. Note subcutaneous fuel from a chest injury in this 34-year-old man submit motor vehicle accident. The left kidney is swollen with diminished operate due to diffuse tumor involvement. Given the dimensions of this mass, renal cell carcinoma was suspected, however it was an oncocytoma at surgery. The kidney is increased in echogenicity with elevated prominence of the pyramids in this affected person with a contralateral, severely hydronephrotic, poorly functioning kidney. The kidney is small (8 cm) with increased echogenicity and loss of corticomedullary differentiation. The kidney is small and lobulated, a nonspecific appearance, which can be the top results of many disorders. Renal sinus fats is preserved 3128 Chronic Renal Infarction Longitudinal ultrasound reveals a renal transplant with scarring of the decrease pole, a sequela of thrombosis of a decrease pole accessory artery. Follow-up ultrasound 18 months later exhibits atrophy of the left kidney with regression of the cysts. A few tiny cysts have been present with no Longitudinal ultrasound of the right kidney reveals extreme cortical loss and hydronephrosis. The obstruction was caused by a strong mass in the renal pelvis representing urothelial most cancers. These findings are indistinguishable from pelvic urothelial carcinoma and additional analysis is required. Transverse color Doppler ultrasound of the identical affected person exhibits the extent of the hematoma and the size relative to the kidney. Common and unusual grownup unilateral renal masses apart from renal cell carcinoma. There is a very echogenic kidney with a hypoechoic perinephric hematoma, which was managed conservatively. The left kidney is small and markedly elevated in echogenicity with pelviectasis. The renal parenchymal echogenicity is elevated with sparing of the subcapsular cortical tissue as a end result of the capsular blood provide is preserved. The lesion is steady with renal cortex and barely hyperechoic to renal cortex secondary to anisotropy. Note that the indentation lies between renal pyramids, which distinguishes it from a renal scar. This line occurs at a airplane of embryologic fusion of renunculi (embryologic elements forming kidneys) and is usually seen at the upper and center 1/3 of the kidney. Technique (depth, focal zone, fundamental imaging) ought to be optimized to confirm shadowing. These medullary rings are thought to be as a end result of the dilated collecting tubules of medullary sponge kidney. Acute pyelonephritis is typically a clinical prognosis, and ultrasound is utilized to assess issues (abscess) and causes (obstruction). Uncomplicated pyelonephritis is normally sonographically occult, though findings could embody renal enlargement, urothelial thickening, and regions of altered echogenicity.
Apium crispum (Parsley). Prazosin.
- Are there any interactions with medications?
- What is Parsley?
- How does Parsley work?
- Kidney stones, urinary tract infections (UTIs), cracked or chapped skin, bruises, tumors, insect bites, digestive problems, menstrual problems, liver disorders, asthma, cough, fluid retention and swelling (edema), and other conditions.
- Dosing considerations for Parsley.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96771
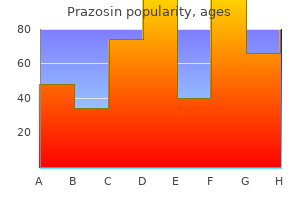
Purchase 5 mg prazosin mastercard
Patients with frequent infections may profit from longterm antibiotic therapy with macrolides cholesterol ratio blood test prazosin 5 mg generic without prescription. Recom binant deoxyribonuclease is helpful for cystic fibrosis sufferers cholesterol eggs everyday buy prazosin 2.5 mg online, but may be dangerous for other sufferers with bronchiectasis. It can pose a diagnostic and administration downside, and stays a leading reason for cancer dying in men and women. At diagnosis only 20% of patients will have local illness and half may have disseminated disease. Over the previous 25 years, adeno carcinoma has turn out to be extra common than squamous cell carcinoma. Massive haemoptysis may happen on account of bronchial wall erosion and the increased vascularity of the bronchial partitions. Surgery should be considered for localised illness to stop progression, or as therapy of intractable haemorrhage. Find out how the diagnosis was made or suspected � a proportion of sufferers are asymptomatic and had been identified after a routine chest Xray or scan. Enquire about a historical past of unresolved pneumonia (a common cause for investiga tions to exclude carcinoma of the lung), pleural effusion or lung abscess. Hypercalcaemia (increased parathyroid hormone happens usually in squamous cell carcinoma) b. Hypertrophic pulmonary osteoarthropathy (may be extra frequent with adenocarcinoma) four. Opportunistic infections (most typically in those handled with chemotherapy) ht tp:// eb oo ks m ed ebooksmedicine. Sputum cytology could also be helpful in centrally positioned lesions, however fibreoptic bronchos copy is now more typically carried out first. Bronchial brushings and washings, taken at bronchoscopy, must also be despatched for cytological examination however have a decrease yield than biopsy. Chest indicators will range � hear fastidiously for a fixed inspiratory wheeze over a large bronchus. Recurrent laryngeal nerve palsy may have triggered hoarseness, and phrenic nerve paralysis might have triggered an elevation of a hemidiaphragm. It has been shown to detect metastases in up to 20% of patients beforehand thought swimsuit in a position for surgical procedure. The finding of a solitary nodule on a chest Xray should be investi gated, however benign causes include a postinfection granuloma or a hamartoma. Other investigations could embody bone marrow biopsy, mediastinoscopy and thora cotomy. Symptoms and indicators that suggest central nervous system, liver, bone, chest wall or mediastinal involvement must be sought fastidiously. Some nucleated pink cells (normoblasts) and myeloid cells (metamyelocytes and myelocytes). Comment: the combination of normochromic anaemia and the presence of marrow precursors within the peripheral blood is recognized as a leukoerythroblastic response. The abnormal liver operate checks are non-specific, but counsel liver involvement in this setting. In small cell carcinoma, stage the illness into limited illness (lung main, ipsi lateral and contralateral hilar, mediastinal and supraclavicular nodes) or intensive disease � 70% of patients (contralateral lung, distant metastases). In general, disease confined to one hemithorax and the ipsilateral cervical nodes known as limited and additional involvement is described as intensive disease. In patients with restricted disease, chemotherapy and concurrent radiotherapy improve the prognosis. Treatment often consists of platinumbased medicine � etoposide and cisplatin or carboplatin. Prophylactic cranial irradiation may be given to sufferers with full responses. There is a threat of leukaemia, central nervous system metastases, dementia and second main malignancies with treatment. Limited small cell carcinoma has a median survival with remedy of 11�18 months; 10�20% are disease free at 2 years. Otherwise, a affected person who can climb three flights of stairs is often considered properly sufficient to tolerate surgery. Chronic obstructive pulmonary disease this common time period is often utilized to patients with persistent bronchitis and emphysema. Chronic obstructive pulmonary disease is frequent and presents main management issues. Onethird of patients have illness sufficiently localised for an try at resection. Median survival is just a few months in patients with intracranial metastases or bone involvement. Treatment is commonly guided by tumour characteristics � pemetrexedbased chemotherapy is most popular for nonsquamous tumours. Some tumours have muta tions at the tyrosine kinase domain, and using oral tyrosine kinase inhibitors (gefitnib and erlotib) has been associated with an preliminary improved response. Find out about symptoms, corresponding to cough and sputum, dyspnoea, wheeze, impaired exercise tolerance, ankle oedema and weight loss. Remember that the prognosis of chronic bronchitis is made largely from the history. Absence of a smoking history weighs closely against the analysis unless continual bronchial asthma or alpha1 antitrypsin deficiency is current, or publicity to mud or fumes (Box 6. Commencement in adolescence when lung development is incomplete may result in a more speedy decline in lung perform. This could additionally be necessary, particularly as an additive function if the affected person has pneumoconiosis or has been exposed to toluene in plastics factories. Exposure to the fumes of strong gasoline fires and to air air pollution can additionally be a threat factor. Ask about financial problems related to continual sickness and signs of depression caused by continual incapacity and lack of selfesteem. These are associ ated with a poor prognosis � over 8% 30day mortality in some studies. Global Initiative for Chronic Obstructive Lung Disease, a collaboration between the National Institutes of Health and the World Health Organization. Spirometry � by definition, spirometry will show airflow limitation and it may be used to grade severity (Table 6. The diffusing capability for carbon monoxide is reduced in emphysema � a worth of < 50% is associated with exertioninduced hypoxia. The demonstration of serious hypoxia (usually a PaO2 of < 55 mmHg, or < fifty nine mmHg if the affected person has cor pulmonale) is required for the prescription of home oxygen remedy. Note the over-inflated lungs, flat hemi-diaphragms and outstanding ks m ed ebooksmedicine. Sputum tradition � will often develop Haemophilus influenzae, Streptococcus pneumoniae or Moraxella catarrhalis during exacerbations and remissions.
5 mg prazosin order free shipping
Variant Biliary Anatomy Abnormal Biliary Dilatation (Left) Spot radiograph demonstrates an internal/external biliary drain with the pigtail loop in the bowel high cholesterol foods dr oz prazosin 5 mg cheap with visa. There is biliary ductal dilatation due to ldl cholesterol definition generic 2.5 mg prazosin amex a common duct stricture, via which the drain has been handed. Choledocholithiasis � Biliary dilatation Diameter and size of balloon used Appearance pre/post dilatation � Biliary stent Type, length, and diameter of stent(s) deployed Indicate if safety catheter left indwelling � Indicate if specimens sent for microbiology, cytology Alternative Procedures/Therapies � Radiologic Percutaneous cholecystostomy � May be used to provide access to distal widespread bile duct abnormality � Surgical Open or laparoscopic surgical decompression �. An ultrasound probe with a sterile cover can be utilized to identify and align the goal intrahepatic duct into sonographic view. Efflux of bile could additionally be observed upon elimination of the internal stylet to confirm needle tip place. Site choice for the 2nd level of entry is performed by putting a hemostat over the potential site and evaluating under fluoroscopy to decide if a suitable intercostal trajectory is out there. The dermatotomy should be large sufficient to allow the location of an 8-Fr drainage catheter. The 1st needle remains in place in order that further distinction may be injected if needed. If the stricture had not been initially crossed with the 3-J guidewire, a mix of a hydrophilic guidewire and a Kumpe catheter may have been used to negotiate the stricture. Note that the primary access has nonetheless been preserved, which is helpful if the secondary access is misplaced for any reason. Also observe that there are embolization coils in the left lobe from treatment of prior hepatic injury. The drainage catheter is then superior off of the cannula along the guidewire using fluoroscopic monitoring. The external hub of the catheter shall be subsequently related to a 3-way stopcock and drainage bag. A radiopaque ring demarcates probably the most proximal sidehole, which is throughout the duct. Percutaneous transhepatic biliary drainage was subsequently carried out through a 2nd access. Cholangiography by way of Cholecystostomy 748 Transhepatic Biliary Interventions Nonvascular Procedures Dilation of Biliary Stricture (Imaging Prior to Crossing Lesion) Dilation of Biliary Stricture (Catheter Crossing Lesion) (Left) Spot radiograph from a 62-year-old man with a history of a previous Whipple procedure for pancreatic acinar cell carcinoma and new onset of jaundice exhibits distinction injection of a 5-Fr Kumpe catheter that had been introduced via a transhepatic method. Dilation of Biliary Stricture (Angioplasty Balloon Placement) Dilation of Biliary Stricture (Angioplasty Balloon Inflation) (Left) Balloon angioplasty catheter was launched over an Amplatz guidewire through an access sheath & superior to the level of the stricture. Radiopaque markers demarcating the proximal & distal extent of the deflated balloon are positioned to encompass the stricture. Occasionally, the balloon may propel forward into the bowel throughout inflation; countertraction on the catheter could also be necessary. Dilation of Biliary Stricture (Angioplasty Balloon Inflation) Dilation of Biliary Stricture (Appearance After Angioplasty) (Left) the balloon is inflated further and the "waist" is obliterated. The balloon is then deflated and the method is repeated for a total of three dilatations. Algorithms differ amongst interventionalists; in one regularly used algorithm, 3 remedy sessions are employed, every 1-2 weeks apart. A 5-Fr Kumpe catheter has traversed a standard duct stricture, with the catheter tip within the bowel. The Wallstent is positioned to embody the whole length of the stricture, with the ends of the stent extending a minimum of 2-3 cm proximal and distal to the stricture margins. Percutaneous Biliary Stent Placement (Introduction of Self-Expanding Stent) Percutaneous Biliary Stent Placement (Self-Expanding Stent Deployment) (Left) Spot radiograph shows the Wallstent has been deployed. Note the distal tip is within the bowel and the proximal tip is within intrahepatic ducts. It is important the stent extends proximal and distal to the stricture, as the stent will shorten as it expands. This was confirmed on 4-hour delayed imaging and is in maintaining with acute cholecystitis. A rim of decreased exercise within the hepatic parenchyma is suggestive of pericholecystic inflammation. Percutaneous Cholecystostomy Drain (Fluoroscopic Imaging) 752 Cholecystostomy Nonvascular Procedures � 18-g needle of acceptable length � zero. Contrast injected through the trocar may be performed, and minimal quantity must be used. Malpositioned Cholecystostomy Tube (Wire Advancement Through Catheter) Malpositioned Cholecystostomy Tube (Advancement of New Drain) (Left) A new pigtail cholecystostomy drain (with plastic inside cannula) was advanced over the Amplatz wire. The internal cannula and wire had been then removed, and positioning of latest pigtail drain was confirmed with distinction. Cholecystostomy Drain Rescue (Sinogram) Cholecystostomy Drain Rescue (Advancement into Gallbladder) (Left) the drain was eliminated over a guidewire. A hydrophilic Glidewire and a Kumpe catheter were then advanced through the original cholecystostomy catheter tract. The findings are in maintaining with active bleeding, presumed secondary to drain placement. Contrast extravasation signifies lively bleeding, adjoining to the cholecystostomy catheter. An internal ureteral stent additionally has a proximal pigtail in the renal pelvis plus a distal pigtail in the bladder. Pressures are measured there and within the bladder through a Foley catheter, using transducers, to evaluate for ureteral stasis vs. Basiri A et al: Ultrasound-guided access throughout percutaneous nephrolithotomy: getting into desired calyx with acceptable entry site and angle. This comparatively avascular zone situated between the anterior and posterior divisions of the renal artery lies 20-30� from the sagittal aircraft. The tip of the needle is well visualized within the dilated, echolucent collecting system. Either a 1-stick approach could additionally be used, or, alternatively, a ring needle may be superior into a different calyx under fluoroscopic steering (2-stick technique). Percutaneous Nephrostomy: Antegrade Nephrostogram 764 Genitourinary Interventions Nonvascular Procedures Percutaneous Nephrostomy: 1-Stick Technique Percutaneous Nephrostomy: 1-Stick Technique (Left) Intraoperative photograph reveals the 1-stick technique during which a zero. If only the floppy portion is inside the system, kinking of the wire during catheter exchanges could happen. The transition from the stiff to the floppy portion is quickly identified fluoroscopically. During secondary entry, repeated distinction filling and dilation of the renal accumulating system is carried out by way of the initial entry as required. Percutaneous Nephrostomy: Coaxial Dilator-Sheath Percutaneous Nephrostomy: Guidewire Placement in Renal Pelvis (Left) the needle has been exchanged for a coaxial dilator-sheath, which was advanced over the guidewire into the renal accumulating system.
Prazosin 2.5 mg cheap on-line
A piece of material tape is placed around the catheter after which sutured to the disk cholesterol water solubility 2.5 mg prazosin cheap amex. Extension tubing connected to the opposite finish of the stopcock is linked to a gravity drainage bag cholesterol numbers chart explained buy prazosin 2.5 mg amex. As the guidewire advances, the operator feels gentle resistance in opposition to wire advancement, which abates because the wire coils. The percutaneous tract is dilated (optional) and the drain is advanced over the wire. Advancing the drain over the metallic stiffening cannula is acceptable because the tract is straight and the traversed tissues dense. A Rosen wire was used since the curved tip helps the wire coil within the collection. An Amplatz wire is too stiff and will easily perforate exterior of the gathering, by way of the renal parenchyma. Perirenal Abscess (Final Drain Position) (Left) the distance from pores and skin to collection was measured, and a Dawson-Mueller drain (a drain with a narrow diameter pigtail) was superior over a stiff, metallic inner cannula. Fluoroscopic-guided Seldinger approach was chosen in order to lay a catheter alongside the complete size of the collection. An angled catheter may help place the guidewire into the subphrenic location if wanted. Fluoroscopic-Guided Drain Placement (Postplacement Contrast Injection) Decreased Output (Fluoroscopic Evaluation) (Left) Over the wire, the tract is dilated and a drainage catheter is superior. Contrast injected by way of the drain confirms passable location inside the abscess cavity. A biliary-type drain with much more sideholes can be used to drain giant collections, such as the one seen right here. Contrast injected via the drain reveals that the drain is partially occluded with inner particles and suboptimally situated. Decreased Output (Wire Repositioning) Decreased Output (Improved Drain Position) (Left) the drain was eliminated over a wire, and the wire was repositioned by way of an angled catheter into a larger portion of the gathering. Decreased drainage may be related to collection decision, drain occlusion, drain malposition, septations inside the collection, or tools failure. The needle is eliminated and the tract dilated, with the dilator superior not extra than the measured distance. In a patient with pain, leukocytosis, and declining renal operate, this was felt to more than likely characterize a perinephric abscess. When the tip is visualized inside the collection, the catheter is unscrewed from the trocar and superior into the abscess. Transvaginal Drainage (Final Drain Evaluation) Enterocutaneous Fistula (Drain Evaluation) (Left) the tract was dilated and the pigtail drain is superior over the wire with fluoroscopic steerage. During drain placement, Crohn patients must be informed that fistula can take months to heal (3 months, on this case). This drain was slowly withdrawn from the fistula, and no suction applied to the collection bag. In this case, the gastrostomy tube is held in place between an intraluminal balloon and exterior disc adjoining to the pores and skin. Gastrostomy Tube Placement Gastrostomy Tube, Balloon Type (Left) this percutaneous gastrostomy (G) tube is held in place by the contrast-filled, intraluminal balloon. Yuruker S et al: Percutaneous endoscopic gastrostomy: technical issues, problems, and management. Gastrostomy Tube Placement (Marking Liver Edge) Gastrostomy Tube Placement (Gastropexy Procedure) (Left) Intraprocedural photograph shows that a Tfastener is being loaded onto the slot of an 18-gauge needle. Gastrostomy Tube Placement (Gastropexy Procedure) Gastrostomy Tube Placement (Gastropexy Procedure) (Left) the 2nd T-fastener is loaded onto a needle, which is advanced into the abdomen. Needle entry into the stomach is confirmed when air is aspirated into the syringe. Gastrostomy Tube Placement (Gastropexy Procedure) 728 Gastrostomy/Gastrojejunostomy Nonvascular Procedures Gastrostomy Tube Placement (Gastropexy Procedure) Gastrostomy Tube Placement (Gastropexy Procedure) (Left) With needle tip position confirmed, the syringe is detached and a guidewire is superior by way of the needle to deploy the Tfastener into the stomach. A wire that bounces off of at least three partitions of the abdomen confirms an intraluminal, somewhat than an intraperitoneal, location. Gastrostomy Tube Placement (Needle Access Into Stomach) Gastrostomy Tube Placement (Needle Access Into Stomach) (Left) With 2-4 T-fasteners in place, a needle hooked up to a saline-filled syringe is inserted into the anesthetized insertion website central to the Tfasteners with a rightward trajectory towards the pylorus. Aspiration of air, or lateral imaging with contrast drip, confirms intraluminal location. Gastrostomy Tube Placement (Tract Dilatation) Gastrostomy Tube Placement (Tract Dilation) (Left) the needle has been removed and a dilator is being advanced over the guidewire. Sequentially larger dilators will prepare a sufficiently large gastrostomy tract to permit introduction of the G tube. Gastrostomy Tube Placement (Peel-Away Sheath) Gastrostomy Tube Placement (Pigtail-Type Tube Insertion) (Left) the G tube is advanced over the indwelling guidewire via the peel-away sheath and into the stomach. Placement of a balloon-retention G tube may require a peel-away 2-4 Fr sizes larger than the G tube and may not monitor over a nonhydrophilic wire. Gastrostomy Tube Placement (Position Confirmation) Gastrostomy Tube Placement (Final Tube Position) (Left) In this pigtail-type G tube, the locking suture is pulled taut, forming the pigtail right into a locked place, thereby securing the internal fixation mechanism of the G tube. Contrast injected through the tube outlines rugal folds within the decompressed stomach. It is important to ensure T-fasteners are deployed into the abdomen lumen; not positioned throughout the anterior belly wall. The tract is dilated with the dilator advanced over the guidewire by the measured distance. Subsequently, a peel-away sheath is launched, by way of which the G tube is superior into the stomach. New gastric access was obtained through the prevailing dermatotomy, towards the pylorus. Malpositioned Gastrojejunal Tube (New Access) Malpositioned Gastrojejunal Tube (Advancement to Jejunum) (Left) A hydrophilic wire and angled catheter were superior past the pylorus into jejunum. Gastrojejunal Tube (Normal Appearance) 732 Gastrostomy/Gastrojejunostomy Nonvascular Procedures Jejunostomy Tube (Over-The-Wire Exchange) Jejunostomy Tube (Retrograde Replacement) (Left) After exchanging a jejunostomy tube, inject contrast and observe the path of peristalsis to insure that the jejunostomy tube is downstream of the balloon. This balloon may be slightly overinflated in comparability with the diameter of the adjoining jejunum. Complication (Hemorrhage through Gastrostomy Tube) Complication (Hemorrhage through Gastrostomy Tube) (Left) the affected person later presented with bleeding through the G tube. Of note, the G tube has been removed over a guidewire so as to get rid of any possible tamponade impact by the tube. This diagnosis of achalasia is typically handled with surgical procedure or balloon dilatation, not stenting.
Prazosin 5 mg purchase with visa
The lymphatic drainage of the higher parts of the pharynx is thru the retropharyngeal lymph nodes cholesterol medication causes muscle pain prazosin 5 mg buy without prescription, whereas the lower portions drain to the parapharyngeal or deep cervical nodes cholesterol medication blood thinner prazosin 5 mg purchase without prescription. The plexus itself is situated on the outer facet of the constrictor pharyngis medius muscle. The retropharyngeal house accommodates smaller arterial and venous vessels and, most notably, the retropharyngeal lymph nodes that drain the nasopharynx. Esophagus the esophagus begins at the higher esophageal sphincter, situated on the level of the C6 and C7 vertebrae (inferior border of the cricoid cartilage). The three physiologic constrictions of the esophagus are clinically important as a outcome of the tendency for ingested overseas our bodies to turn into lodged at those ranges. The parapharyngeal space is divided anatomically into two parts, the retropharyngeal house and the lateral pharyngeal space. The latter in flip is subdivided by the common connective-tissue sheath of the muscular tissues arising from the stylohyoid course of (stylopharyngeal aponeurosis) into a prestyloid and a retrostyloid half. It contains the lateral and medial pterygoid muscles, lingual nerve, optic ganglion, and maxillary artery. Anatomy of the esophagus a b 0 Thyroid cartilage Cricoid cartilage Cricopharyngeus muscle Trachea Aorta Sternum Esophagus Heart Diaphragm Epiglottis Cricoid cartilage Upper esophageal constriction Trachea Midesophageal constriction Aorta Piriform recess Thyroid cartilage Cricopharyngeus muscle a the esophagus extends from C6/C7 to the gastric cardia at the level of the T10 vertebra. The thoracic esophagus is equipped by the aorta and intercostal arteries, and the abdominal esophagus by the left gastric artery and left inferior phrenic artery. Thoracic and abdominal drainage is to the azygos and hemiazygos veins and esophageal veins. Lymphatic drainage is to the lymph nodes of the posterior mediastinum and pulmonary hilum. Nerve provide: the upper, cervical part of the esophagus is supplied with branches from the recurrent nerve and the lower half with unnamed branches from the vagus nerve. Below the tracheal bifurcation is the esophageal plexus, fashioned by the 2 vagus nerves. Secondary peristalsis is additionally triggered within the esophagus by the stress of the bolus towards the esophageal wall. Through the coordinated action of those mechanisms, the bolus is transported into the abdomen inside 7�10 seconds. This tissue is structurally just like lymph nodes but lacks afferent lymphatic vessels. The tonsils are named for their location, consisting of a pharyngeal tonsil, the paired palatine tonsils, and the unpaired lingual tonsil on the base of the tongue. Additionally, smaller condensations of lymphoepithelial tissue are discovered in the pharyngeal recess. While the pharyngeal tonsil is covered primarily by a number of rows of ciliated epithelium, the palatine and lingual tonsils are covered by stratified, nonkeratinized squamous epithelium. Physiology of Swallowing Normal swallowing requires a coordinated interplay of varied anatomic constructions within the oral cavity, pharynx, larynx, and esophagus. From a functional standpoint, the voluntarily initiated oral part of swallowing is distinguished from an "involuntary" pharyngeal part and esophageal section, which are managed through reflex mechanisms. This is achieved mainly by urgent the food in opposition to the hard palate with the tongue. The pharyngeal part begins when the bolus comes into contact with receptors within the throat (especially on the tongue base), eliciting an involuntary swallowing reflex. The extensive nerve provide highlights the complexity of swallowing in addition to the potential vulnerability of this process. While the involuntary swallowing reflex is triggered during the pharyngeal section, the velum is elevated to shut off the nasopharynx. This is accompa- Structure of the Palatine Tonsil the palatine tonsil has particular immunologic importance among the tissues of the tonsillar ring owing to its distinctive morphology. Its surface is invaginated by crypts-fold-like tissue indentations which may be lined by porous epithelium and considerably improve the surface space of the tonsil. This arrangement facilitates contact between inspired or ingested antigens and the subepithelial lymphatic tissue. Physiology of swallowing a Oral section b Pharyngeal section Bolus c Esophageal part Bolus Bolus the circled numbers refer to the text (p. Within the lymphatic tissue, major follicles are fashioned throughout embryonic development and differentiate into secondary follicles after start. The secondary follicles mainly comprise B lymphocytes at various levels of differentiation, along with scattered T lymphocytes. Besides the lymph follicles, there are additionally extrafollicular areas with B and T lymphocytes that enter the lymphatic tissue through the postcapillary venules. Functional Importance of the Tonsils within the Immune System the palatine tonsil particularly is taken into account to be an "immune organ" that plays a big function in the protection in opposition to upper respiratory infections. Accordingly, this tissue has the ability to mount specific immune reactions in response to various antigens. The exercise of this lymphatic organ is particularly pronounced during childhood, when immunologic challenges from the setting induce hyperplasia of the palatine tonsils. While the tonsils become much less important immunologically with ageing, the tonsillar tissue continues to perform immune functions even at a complicated age, although this could not alter the choice to take away the tonsils if a legitimate indication for tonsillectomy exists (see Chronic Tonsillitis, p. While the tonsils are "learning" their immune perform throughout childhood, excessive tonsillar hyperplasia ("kissing tonsils") could develop, resulting in functionally vital narrowing of the faucial isthmus, with consuming difficulties and obstructed breathing. Especially Probst-Grevers-Iro, Basic Otorhinolaryngology� 2006 Thieme All rights reserved. Tonsillar hyperplasia Mantle zone Germinal zone b the dimensions and activity of the germinal centers are maximal at approximately 6�8 years of age, reflecting the immunologic activity of the palatine tonsil. Tonsillar hyperplasia develops in plenty of kids during this "active immunization phase. Consequently, there should be little hesitation in recommending tonsillectomy, even in young children. The secondary follicles within the lymphatic tissue, which are essential for tonsillar immune function, feature a light-colored germinal zone and a darkish mantle zone with mature lymphocytes. This trend is due largely to the advent of computed tomography and magnetic resonance imaging, while typical radiographs have turn out to be largely out of date within the investigation of ailments of the pharynx. On the other hand, typical radiographs are still a vital software for the investigation of many esophageal disorders. Clinical examination of the pharynx is an important a half of any otolaryngologic examination and depends on numerous techniques. Besides the traditional mirror examination, diagnostic endoscopic procedures have been more and more utilized in current times. Imaging procedures have also assumed major importance in the investigation of varied pharyngeal disor- Mirror Examination and Endoscopy Nasopharynx the location of the nasopharynx could make it very troublesome to access and examine, particularly for newbies.