
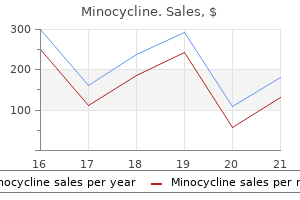
Minocycline dosages: 50 mg
Minocycline packs: 15 pills, 30 pills, 45 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Order minocycline 50 mg line
Why should anesthesia providers give attention to the effects of analgesia on the method of vaginal delivery Lack of effective maternal effort related to insufficient progress of labor (descent of the fetus) is a sign for operative vaginal supply infection rates for hospitals 50 mg minocycline cheap with amex. In contrast antibiotics loss of taste minocycline 50 mg generic line, several massive observational research counsel that epidural analgesia is related to a decreased danger for anal sphincter laceration in nulliparous women. Of concern is a decline within the variety of obstetricians expert at operative vaginal supply. Duration of Labor First Stage of Labor the effect of neuraxial labor analgesia on the length of the first stage of labor was addressed as a secondary end result variable in many of the randomized controlled trials. A 2011 meta-analysis3 of 11 research found no distinction in the length of the first stage of labor between girls who were randomly assigned to obtain epidural analgesia and people assigned to obtain systemic opioid analgesia, although the confidence interval was broad, indicating important heterogeneity among research (Table 23. There was significant heterogeneity in the end result due to the combined parity of the patient populations and variations among studies in the definition of the duration of the first stage of labor. Labor analgesia and cesarean delivery: a person meta-analysis of nulliparous girls. Both teams of investigators decided that the period of the primary stage of labor, and thus consequently the overall period of labor, had been significantly shorter in ladies randomly assigned to receive early labor neuraxial analgesia than in these assigned to obtain systemic opioid analgesia. Determining the period of labor requires that investigators document begin and finish instances. The definition of the start time varies among research however is often consistent between groups within a study. The end of the first stage of labor is outlined as the time of full (10 cm) cervical dilation. Clinically, full cervical dilation is recognized when a cervical examination is carried out as a end result of the affected person complains of rectal pressure. It is likely that girls with effective epidural analgesia will complain of rectal stress at a later time (and lower fetal station) than girls with systemic opioid analgesia. In other words, the affected person could additionally be fully dilated for a major time earlier than cervical examination verifies full cervical dilation. This distinction serves to artificially extend the length of the primary stage of labor in the epidural group, although it shortens the apparent length of the second stage of labor. Some clinicians have noted enhanced uterine activity in some patients for roughly 30 minutes after the initiation of neuraxial analgesia, whereas uterine exercise appears to be decreased in other patients. Schellenberg466 advised that aortocaval compression is answerable for the transient lower in uterine exercise that occurs after the administration of epidural analgesia in some sufferers. Because this organ additionally releases oxytocin, the production of that hormone might also be transiently suppressed; this possible decrease in oxytocin launch might partially clarify the transient adjustments in uterine contractility noticed in association with epidural analgesia. No important difference within the variety of contractions earlier than and after epidural analgesia was noticed. There was greater intrauterine strain in the higher uterine phase than in the lower section (consistent with fundal dominance) each earlier than and after initiation of epidural analgesia. Further, fundal dominance was larger after epidural analgesia than in the preanalgesia period. Increased uterine activity after the initiation of neuraxial analgesia has been hypothesized to be an oblique effect of neuraxial analgesia (see later discussion). Some physicians have expressed concern that the epinephrine might exert a systemic beta-adrenergic tocolytic effect and gradual labor. Early research, which used large doses of epinephrine, advised that the caudal epidural administration of native anesthetic with epinephrine extended the primary stage of labor and increased the number of sufferers who required oxytocin augmentation of labor. In abstract, neuraxial analgesia appears to have a variable impact on the duration of the primary stage of labor. Second Stage of Labor There is little doubt that effective neuraxial analgesia prolongs the second stage of labor. Meta-analyses of randomized controlled trials that compared neuraxial with systemic opioid analgesia assist this medical observation (see Table 23. Data have been abstracted for term parturients in spontaneous labor with a singleton gestation in the vertex presentation and with regular perinatal outcome. The rate of spontaneous vaginal delivery declined because the duration of the second stage of labor elevated; however, greater than 55% of ladies whose second-stage duration was 3 hours or longer still went on to ship vaginally. Extending the duration of the second stage will permit a significant number of ladies to deliver vaginally. Summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, and American College of Obstetricians and Gynecologists Workshop. Data are median (95th percentile) period of the second stage of labor in spontaneous laboring ladies. Many ladies are asked to begin "pushing" as soon as full cervical dilation has been confirmed, regardless of the fetal station. Some practitioners have advised that "delayed" pushing may lead to much less maternal exhaustion and higher maternal and fetal outcomes. Several randomized studies have sought to determine whether immediate or delayed pushing for women with epidural analgesia through the second stage of labor impacts labor duration and consequence. In a 2017 meta-analysis including 13 research that compared early and delayed pushing in women with epidural analgesia, the authors judged that the proof ranged from moderate to very low high quality. There was no distinction in perineal trauma, neonatal intensive care unit admissions, or 5-minute Apgar scores. The authors concluded that the current evidence is inadequate and inconclusive to support any specific timing and sort of pushing; further high-quality studies are essential. The length of the third stage of labor was shorter in women who acquired epidural analgesia and subsequently required manual removal of the placenta. The researchers instructed that epidural analgesia Review: Pushing/bearing down strategies for the second stage of labor Comparison: 2 Analysis 2. The diamond represents the purpose estimate of the pooled danger ratio, and the size of the diamond is proportional to the arrogance interval. Other Factors and Progress of Labor Oxytocin Active management of labor is an idea that consists of a disciplined, standardized labor administration protocol that features early amniotomy and oxytocin augmentation if the cervix fails to dilate at a minimal price (usually 1 cm/hour in nulliparous women). Early research suggested that this kind of labor administration decreased the speed of cesarean supply. In a search of the medical literature, they recognized sixteen randomized managed trials; 8 of the 16 trials included descriptions of labor administration, and these trials have been included within the evaluation. Seven of the eight trials described energetic management of labor and located no distinction within the mode of supply between teams. Only certainly one of eight trials described using low-dose oxytocin and reported a markedly higher rate of cesarean supply in the neuraxial analgesia group. The researchers had been right in stating that the function of oxytocin in neuraxial analgesia consequence studies has not been well managed. In randomized controlled trials that compared the effects of neuraxial and systemic opioid analgesia on the finish result of labor, women who received neuraxial opioids had the next rate of oxytocin augmentation. Ambulation Observational studies counsel that ambulation could additionally be associated with less ache and a shorter length of labor. There was no distinction between groups within the mode of supply or period of labor. These results agree with these of a meta-analysis of five randomized managed trials involving 1161 women.
Minocycline 50 mg purchase with mastercard
The prevalence is 240 per million antibiotic zithromax and alcohol minocycline 50 mg cheap, which is 4 to 9 instances greater than the reported world prevalence antibiotic wound ointment minocycline 50 mg discount otc. Scleroderma is almost 5 occasions extra common in girls than in men and occurs primarily between 30 and 50 years of age. Although the stimulus for fibroblasts to produce excessive collagen and different matrix constituents is unknown, their accumulation leads to microvascular obliteration and fibrosis within the skin and different target organs. Endothelial cells bear vasomotor and permeability changes, producing cyclic vasoconstriction-vasodilation and edema. Patients with scleroderma produce autoantibodies in opposition to nuclear and centromere structures, although their significance is unclear. Scleroderma exhibits a powerful feminine predilection, a steep rise in incidence after the childbearing years, and features which may be much like graft-versus-host illness after bone marrow transplantation, prompting some to postulate that microchimerism may be involved in its pathogenesis. Fetal cells acquire entry to the maternal circulation throughout gestation and may be detected in maternal blood for many years after delivery. After some unknown stimulus however possibly including environmental elements,107 they could differentiate and initiate a reaction similar to graft-versus-host illness. Skin involvement is proscribed to the arms, face, and feet in this type of the illness. The extra in depth medical manifestations of diffuse cutaneous scleroderma are summarized in Box 40. Effect on Pregnancy and the Fetus the frequency of preterm births and small-for-dates infants is higher in pregnant women with scleroderma. No disease modification advantages have been proven by administration of penicillamine, methotrexate, or other immunosuppressive agents (other than the utilization of glucocorticoids for inflammatory myositis). Nitric oxide donors and presumably heparin may provide some safety in opposition to placental dysfunction in pregnant ladies with scleroderma. Preterm delivery or termination of being pregnant may be required in the presence of advanced or rapidly progressive illness. Frequent assessment of renal perform and intensive observation for the onset of systemic or pulmonary hypertension, cardiac dysfunction, and fetal compromise, mixed with enhancements in monitoring and treatment, enable most mothers to deliver wholesome infants. Although the prevalence of left ventricular diastolic dysfunction is understood to be higher in sufferers with scleroderma than within the basic population,116 an association with being pregnant has not been famous. Obstructive uropathy could end result from an enlarging uterus trapped within a noncompliant abdomen. Successive critiques by Steen109�111 point out that enhancements in management enable patients with scleroderma to have successful maternal and fetal outcomes. In the other 18% of pregnancies, esophageal reflux, cardiac arrhythmias, arthritis, pores and skin thickening, and/or renal disaster occurred or worsened. History and physical examination must be directed towards detection of underlying systemic dysfunction. Laboratory tests include complete blood cell depend, coagulation display, electrolyte concentrations and creatinine clearance, arterial blood gasoline evaluation, urinalysis, and urine protein willpower. An electrocardiogram and pulmonary function testing should be performed in all patients. Echocardiography is more and more used to assess ventricular dysfunction, pericardial and pleural effusions, and pulmonary hypertension. Severe limitation of mouth opening attributable to hidebound perioral pores and skin might make direct laryngoscopy impossible and mandates careful airway evaluation. The adjustments in airway assessment scores that happen throughout labor should also be borne in mind. Administration of a pulmonary vasodilator may enhance the likelihood of a positive end result. One report of two pregnant women with scleroderma and pulmonary hypertension described administration of neuraxial anesthesia in a single affected person and general anesthesia in the other affected person, highlighting the complexity of administration decisions. Even when severe diffuse cutaneous involvement is current, the pores and skin of the lumbar back is spared. Spinal anesthesia for cesarean supply complicated by precipitous hypotension in a parturient with scleroderma has been reported124; restoration was uneventful with full return of motor perform inside three. Prolonged duration of regional anesthesia has been observed in some sufferers with scleroderma, and may be brought on by reduced uptake of the native anesthetic agent as a consequence of microvasculature adjustments. These instances have included (1) an axillary block performed with 1% lidocaine with epinephrine (reported to have endured for twenty-four hours)125; (2) a digital nerve block carried out with 1% lidocaine without epinephrine (10-hour duration)126; (3) a sciatic nerve block that continued for sixteen hours127; and (4) extended epidural anesthesia with 2% 2-chloroprocaine. Whether this consideration makes epidural (with the flexibility to titrate the dose) rather than spinal anesthesia preferable for cesarean supply is unclear. Diffuse cutaneous involvement could indicate the need for central venous catheterization, and for invasive arterial monitoring if noninvasive blood pressure measurement is inaccurate. Pulmonary artery catheterization could additionally be indicated in the presence of cardiac dysfunction or pulmonary hypertension. Scleroderma reduces tear production, and the eyes must be protected in opposition to corneal abrasions. Polymyositis is characterized by nonsuppurative inflammation of muscle, primarily skeletal muscles of the proximal limbs, neck, and pharynx. This inflammation results in symmetric weak spot, atrophy, and fibrosis of affected muscle groups. These issues are fairly rare, with a prevalence of 10 per million and an annual incidence of 5. The age at onset is bimodal, with peaks before puberty and through the fifth decade. The etiology of inflammatory muscle disease is unknown and possibly multifactorial. An preliminary insult mediated by viral or other infectious agent, or publicity to environmental substances, might lead to preliminary muscle damage in genetically susceptible individuals. This preliminary process might then trigger an autoimmune response involving persistent muscle irritation. Among the 18 patients with previously identified illness, the disease remained inactive in eleven (61%) of the sufferers, and a pair of (11%) had an exacerbation of disease exercise. Consequences may include fetal growth restriction, preterm delivery, and fetal death. Many drugs, including lipid-lowering drugs within the statin group and antiretroviral medication, are related to the development of myopathy. The presence of mobile infiltrates within affected muscle tissue and complement-mediated capillary damage are options of inflammatory muscle illnesses. Underlying malignancy has been related to both situations, though causality is unclear; the affiliation is stronger for dermatomyositis than polymyositis. Pharyngeal muscle involvement results in dysphagia and reflux, and most sufferers exhibit impairment of gastric and esophageal motility. Pulmonary fibrosis is present in 30% of patients and should hardly ever lead to pulmonary hypertension. Cardiac involvement contains nonspecific repolarization abnormalities, conduction disturbances, arrhythmias, coronary artery vasculitis, and, hardly ever, coronary heart failure. The onset of a pregnancy-associated form of dermatomyositis has been described postpartum.
Minocycline 50 mg purchase on line
However antibiotics for acne erythromycin purchase minocycline 50 mg on line, a number of randomized managed trials have shown that the incidence of hypotension after preload with zero antibiotics for uti in adults discount 50 mg minocycline fast delivery. In our apply, my colleagues and I usually administer approximately 500 mL of intravenous crystalloid (co-load) on the time of initiation of neuraxial labor analgesia. Treatment includes the administration of extra intravenous crystalloid, placement of the mother in the full lateral and Trendelenburg place, and administration of an intravenous vasopressor. Traditionally, ephedrine 5 to 10 mg has been administered; nevertheless, studies in girls present process spinal anesthesia for elective cesarean delivery have proven that phenylephrine is equally efficacious in restoring blood strain and is associated with higher umbilical arterial blood pH measurements at birth. Pruritus Pruritus is the most typical aspect effect of epidural or intrathecal opioid administration (see Chapter 13). For moderate to severe pruritus that requires treatment, we usually administer nalbuphine 2. The co-administration of local anesthetic decreases the incidence of pruritus,199 whereas the co-administration of epinephrine might worsen pruritus. The pruritus seems to be mediated via central �-opioid receptors, given that �-opioid receptor antagonists relieve itching. Most studies have addressed pruritus after intrathecal morphine, not lipid-soluble opioids such as fentanyl and sufentanil. However, the usage of these brokers in a bolus or steady infusion might reverse the analgesia. A number of drugs have been investigated for prophylaxis in opposition to neuraxial opioid�induced pruritus, primarily coincident with neuraxial morphine administration. A 2016 metaanalysis included six randomized managed trials of prophylactic ondansetron for prevention of intrathecal fentanyl or sufentanil-induced pruritus in both obstetric and nonobstetric sufferers. However, a single trial in obstetric sufferers who received ondansetron 4 mg or 8 mg before intrathecal fentanyl 25 �g discovered no profit in contrast with placebo. The pruritus is typically self-limiting; the Nausea and vomiting occur regularly throughout labor. It is difficult to decide the incidence of nausea and vomiting directly associated to epidural and intrathecal opioid administration. Nausea and vomiting can also be secondary to neuraxial analgesia�induced hypotension. Maternal blood stress should be measured when the affected person complains of nausea in the presence of neuroblockade. Other causes of nausea and vomiting during labor are pregnancy itself, pain, opioid-induced delay of gastric emptying (see later discussion), and systemic opioids, that are generally administered before intrathecal or epidural opioids. In one examine, the incidences of nausea (7% versus 44%) and vomiting (2% versus 17%) were considerably lower in ladies randomly assigned to receive intrathecal fentanyl than in those assigned to obtain systemic hydromorphone analgesia in early labor. No studies, nonetheless, have specifically addressed the therapy of neuraxial analgesia�associated nausea and vomiting during labor. Fever Both observational and randomized controlled trials have consistently noted a gradual rise in core temperature over a quantity of hours in laboring ladies receiving epidural analgesia that was not observed in women receiving no analgesia, inhaled nitrous oxide, or parenteral opioids. In the small subset of girls who ultimately developed medical fever, core temperature started to rise within 1 hour of initiation of epidural analgesia. The mechanism of temperature elevation in some ladies who receive epidural labor analgesia is incompletely understood however likely reflects a noninfectious inflammatory course of. In an observational examine in girls who self-selected the sort of analgesia, the histologic prognosis of placental inflammation was extra common in girls with epidural analgesia. Maternal fever is related to mode of delivery; the rate of instrumental and cesarean delivery is greater in girls with intrapartum fever. In the pursuits of maternal and fetal safety, intrapartum maternal fever sometimes prompts an intrapartum prognosis of clinical chorioamnionitis. When maternal fever happens, good medical practice dictates that efforts be made to decrease maternal temperature, and identify and treat a presumed maternal an infection. Shivering Several elements, including hormonal components, likely influence thermoregulatory response during labor and delivery. Shivering is frequently observed throughout labor and should happen more commonly after epidural analgesia. Before supply, 18% of girls shivered, and 15% of these episodes were associated with normothermia and vasodilation, suggesting a nonthermoregulatory explanation for the shivering. After delivery, shivering was observed in 16% of women, and in 28% of them, it was nonthermoregulatory. There was no difference within the incidence of shivering between girls who chose epidural (bupivacaine/fentanyl) analgesia and folks who selected systemic meperidine analgesia. The addition of an opioid to the local anesthetic resolution may affect the shivering response. Any distinction in bladder function seems to be shortlived; differences between groups in one study had resolved by postpartum day 1. Parturients must be frequently noticed during labor for proof of bladder distention, particularly in the occasion that they complain of suprapubic pain throughout contractions. The differential prognosis of breakthrough pain throughout neuraxial labor analgesia should include bladder distention. Inability to void and bladder distention ought to immediate catheterization to empty the bladder. Recrudescence of Herpes Simplex Virus the frequent cold sore or fever blister is a manifestation of the reactivation of latent infection. Reactivation can occur after exposure to ultraviolet light, fever, immunosuppression, or trauma. Urinary Retention Urinary retention is a troublesome facet impact of neuraxial anesthesia/analgesia. The bladder and urethral sphincters obtain sympathetic innervation from the low thoracic/high lumbar sympathetic fibers and parasympathetic innervation from sacral fibers. Neuraxial local anesthetics cause urinary retention via blockade of sacral nerve roots. Efferent and afferent nerve traffic via the S2, S3, and S4 nerve roots controls the detrusor muscle (responsible for urine storage and micturition) and inside and external sphincter function. Intrathecal opioids trigger dose-dependent suppression of detrusor muscle contractility and decreased urge sensation via inhibition of sacral parasympathetic nervous system outflow. It is troublesome to determine the magnitude of this downside during labor, as a outcome of parturients often require catheterization for different reasons. Postpartum bladder dysfunction was noticed in 14% of girls who had a traditional spontaneous vaginal supply and in 38% of girls who underwent instrumental vaginal delivery, all with out epidural analgesia. Intravenous or intramuscular opioid administration leads to delayed gastric emptying in laboring girls. In addition, it could end in a larger quantity of gastric contents, which-in theory-might be problematic in patients who require induction of common anesthesia for emergency cesarean supply. Factors such as affected person age and weight, the particular method, the kind of epidural catheter, and the talent of the anesthesia provider are associated with the rate of failure of neuraxial analgesia. The total failure rate of 12% included procedures that resulted in no or inadequate analgesia, unintentional dural puncture with an epidural needle or catheter, intravenous cannulation with the epidural catheter, or alternative of the catheter for any purpose.
Purchase minocycline 50 mg with visa
A case-controlled examine comparing clinical course and outcomes of pregnant and non-pregnant women with severe acute respiratory syndrome virus on macbook air discount minocycline 50 mg with mastercard. Combined high frequency air flow in the administration of respiratory failure in late being pregnant bacteria urine hpf minocycline 50 mg free shipping. Endotracheal intubation, however not laryngeal mask airway insertion, produces reversible bronchoconstriction. Mechanical air flow in an obstetric inhabitants: traits and supply rates. Beneficial impact of epidural anesthesia on oxygen consumption in a parturient with grownup respiratory misery syndrome. Overall, the speed of past-month illicit drug use in pregnant women as reported in the National Survey on Drug Use and Health in 2015 was four. Depending on the actual substance, pregnant girls might experience little to no acute and chronic adverse effects, or alternatively, may manifest one or more of the next: (1) cardiovascular, pulmonary, and neurologic problems or (2) obstetric complications. Although analysis of urine, meconium, and hair are the commonest strategies to test pregnant sufferers and their infants for the presence of illicit drugs, evaluation of saliva, umbilical twine tissue, amniotic fluid, and neonatal gastric aspirate can also be accomplished (Tables fifty three. Caregivers ought to be conscious that the immunoassays mostly used in drug testing can have false-positive or false-negative results in the presence of structurally related drugs or components. Gas chromatography with mass spectrometry ideally should be used to present confirmation of optimistic outcomes. Pharmacology Alcohol is absorbed by way of the gastrointestinal tract, primarily throughout the small intestine, and is then metabolized by alcohol and acetaldehyde dehydrogenases. A small residual amount (2% to 8%) of alcohol is excreted via the lungs, urine, and sweat. Systemic Effects Legally outlined "intoxication" implies a blood alcohol degree of a minimum of 80 to one hundred mg/dL, although behavioral, cognitive, and psychomotor adjustments can occur at ranges of 20 to 30 mg/dL. Endogenous opioids interact with alcohol to "reinforce" further alcohol use; this effect is blunted by opioid antagonists similar to naltrexone, which can be utilized in the treatment of alcohol use dysfunction. Heavy alcohol consumption can end result in hepatic cirrhosis, which, in turn, can lead to encephalopathy, coagulopathy, and esophageal varices (Table 53. Delirium tremens, though rare in pregnant girls, can result in maternal and fetal dying if untreated. These results embody bodily, psychological, behavioral, and/or studying disabilities with potential lifelong implications. Anesthetic Management Alcohol-intoxicated parturients are at elevated danger for behavioral problems, electrolyte abnormalities, greater gastric acid secretion, and co-intoxication with different substances. In addition, these patients could have intravascular volume depletion secondary to vomiting, inadequate oral intake, diuresis, and hypoalbuminemia. Significant alcohol ingestion in the setting of poor oral intake can also manifest as severe hypoglycemia. Evidence from revealed reports is inconclusive about predictable differences in anesthetic necessities in patients with acute and chronic alcohol use. No large inhabitants studies have assessed dose necessities for volatile anesthetic agents or hypnotic agents in patients who chronically use alcohol. Short-term consumption of alcohol inhibits the metabolism of drugs by the liver (through competitors for cytochrome P450), which outcomes in larger plasma concentrations of hepatically metabolized medication. Long-term consumption of alcohol will increase the exercise of cytochrome P450, leading to decreased ranges of medicines corresponding to diazepam and labetalol, and elevated levels of toxic metabolites that happen from hepatic degradation of illicit drugs such as cocaine. Therefore, a balanced anesthetic technique that combines induction with beneficiant doses of a hypnotic agent with succinylcholine, adopted by maintenance with a risky anesthetic agent (limited to zero. Withholding extra muscle leisure after induction and adding a brain function monitor if time and circumstance permit may assist identify patients who could benefit from extra anesthesia. Pharmacology Caffeine (1,three,7-trimethylxanthine) is a naturally occurring alkaloid found in coffee, tea, cocoa, and a few delicate drinks and medicines. Caffeine is readily absorbed through the gastrointestinal tract with maximum blood concentrations 1 to 1. The halflife in the neonate is extended in contrast with that in children and in nonpregnant girls. Habitual use of caffeine at levels higher than 500 to 600 mg/day is outlined in some studies as abuse. In the absence of the inhibitory results of adenosine, the neurotransmitters norepinephrine, dopamine, and serotonin are launched in increased concentrations. Studies of the consequences of caffeine on alertness, vigilance, temper, and reminiscence have produced inconsistent outcomes. Caffeine doses as low as 250 mg have been reported to have a hypertensive effect after acute ingestion (an increase in systolic blood pressure of 5 to 15 mm Hg and a rise in diastolic blood pressure of 5 to 10 mm Hg), significantly in caffeine-na�ve people; nevertheless, epidemiologic studies have produced inconsistent outcomes. Moderate caffeine intake could exacerbate preexisting bladder signs, and excessive intake (greater than four hundred mg/day) increases the danger for bladder dysfunction. Typically, signs start 12 to 24 hours after cessation of use, peak at 20 to forty eight hours, and last as lengthy as 7 days. Moderate first-trimester caffeine intake was discovered to have both no significant effect or to have a protective effect on the development of maternal gestational diabetes mellitus, relying on the population studied. The elimination of theophylline and acetaminophen may be slowed by habitual caffeine consumption, resulting in larger serum drug concentrations. In contrast, serum concentrations of lithium could also be decreased secondary to caffeine-enhanced elimination. Evidence for the efficacy of caffeine in the remedy of post� dural puncture headache is scant (see Chapter 30). Nicotine, the principal element of tobacco, acts at peripheral and central nicotinic (acetylcholine) receptors throughout the body to have an effect on the release of catecholamines. Peripherally, nicotine increases sympathetic tone, thereby rising maternal coronary heart rate, blood pressure, and cardiac work (see Table 53. The pulmonary results of tobacco smoking embody changes in the increased volume of mucus, impaired mucociliary clearance, and an elevated incidence of bronchitis and continual obstructive pulmonary disease (see Table 53. Smoking cessation interventions include counseling and therapy, hypnosis, acupuncture, and pharmacologic remedy. This compromised state can result in decreased uptake of nourishing amino acids by the placenta. In a newer examine, smoking cessation in early being pregnant was associated with a greater discount in risk for fetal development restriction in contrast with cessation later in being pregnant. After controlling for confounders, including adversity and sex, prenatal smoking publicity appeared to have long-term results on neural exercise and development. Anesthetic Management Smoking is a threat factor for a number of perioperative issues, including respiratory sequelae and impaired wound therapeutic. Smokers may be more more likely to cough following emergence from basic anesthesia, however the information are combined and may be associated to the specific volatile agent used.
Minocycline 50 mg cheap with amex
The relationship of blood product ratio to mortality: survival profit or survival bias Postinjury life threatening coagulopathy: is 1:1 fresh frozen plasma:packed purple blood cells the answer Black Hawk down: the evolution of resuscitation strategies in massive traumatic hemorrhage headphones bacteria 700 times 50 mg minocycline purchase amex. Massive transfusion protocols: a survey of educational medical facilities within the United States going back on antibiotics for acne minocycline 50 mg generic amex. Aortoiliac thrombosis following tranexamic acid administration throughout urgent cesarean hysterectomy: a case report. Obstetric neuraxial drug administration errors: a quantitative and qualitative analytical evaluate. Effect of tranexamic acid on surgical bleeding: systematic evaluation and cumulative meta-analysis. Prophylactic tranexamic acid in parturients at low threat for post-partum haemorrhage: systematic evaluate and meta-analysis. Each of these entities varies in its incidence, medical course, and consequences. Embolic events account for nearly one-sixth of all maternal deaths in the United States. The incidence of each factor is increased throughout pregnancy or in the postpartum period. Venous stasis happens as a end result of venocaval compression and presumably decreased mobility later in being pregnant. Separation of the placenta from the uterine wall traumatizes the endometrium, which accelerates the coagulation cascade. Additionally, being pregnant is a comparatively hypercoagulable state, associated with enhanced platelet turnover, coagulation, and fibrinolysis. Fibrinolytic exercise decreases during the 48 hours after supply and enhances clot stability in the early postpartum interval. Intracardiac shunting may develop when elevated proper ventricular pressure forces blood across a probe-patent foramen ovale. The enhance in proper ventricular strain leads to right ventricular dilation, with elevated wall pressure and oxygen demand, and a leftward shift of the interventricular septum. This distribution is completely different from the anatomic distribution in nonpregnant patients, who are extra likely to have thrombi within the distal calf vessels. If the results are adverse or equivocal, and iliac vein thrombosis is suspected, clinicians might go for Doppler ultrasonography of the iliac vein, venography, or magnetic resonance imaging or presumptive anticoagulation. Unfortunately, d-dimer ranges are elevated in pregnancy, making interpretation of elevated ranges troublesome in pregnant girls. In one potential, longitudinal study, serial d-dimer ranges had been evaluated in 89 healthy pregnant ladies; values exceeded the traditional nonpregnant reference vary in all however one woman within the third trimester. Physical examination of the affected person commonly reveals tachypnea, crackles, decreased breath sounds, and tachycardia. Signs of right ventricular failure, together with an accentuated or splitsecond coronary heart sound, jugular venous distention, a parasternal heave, and hepatic enlargement, may be apparent. The use of magnetic resonance pulmonary angiography has not been validated in the pregnant inhabitants. The Society for Obstetric Anesthesia and Perinatology consensus statement on the anesthetic administration of pregnant and postpartum girls receiving thromboprophylaxis or higher dose anticoagulants. The following anticoagulation methods will help to facilitate protected and well timed neuraxial analgesia/anesthesia for parturients40,50: 1. Other anticoagulant drugs sometimes administered to pregnant women embrace aspirin, warfarin, and newer anticoagulant drugs. Treatment with thrombolytics is an absolute contraindication to neuraxial anesthesia. Risks related to general anesthesia within the anticoagulated affected person include airway bleeding. The anesthesia supplier ought to be conscious that placement of nasopharyngeal and oropharyngeal airways, gastric tubes, and other units. Emergency surgical procedure may necessitate the administration of protamine or the transfusion of blood merchandise. The timing of initiation of pharmacologic prophylaxis postpartum varies according to which drug is chosen and the dose. A metaanalysis estimated the incidence of epidural hematoma in obstetric patients (8 studies, pooled n = 1. These embody (1) extreme, unremitting backache; (2) neurologic deficit, together with bowel or bladder dysfunction or radiculopathy; (3) tenderness over the spinous or paraspinous space; and (4) unexplained fever. Neurologic restoration is a perform of the severity of preoperative deficits, the period of most deficit, and the interval between symptom onset and surgery; better outcomes are related to a shorter symptom onset-to-surgery interval. Systems should be developed to establish at-risk women for whom peripartum mechanical or pharmacologic thromboprophylaxis is indicated. Pathologic prognosis of fetal squames or hair within the maternal lungs Society for Maternal-Fetal Medicine and the Amniotic Fluid Foundation Criteria67 1. Sudden onset of cardiorespiratory arrest, or each hypotension and respiratory compromise 2. The coagulopathy must be detected earlier than sufficient blood is lost to account for dilutional or shock-related consumptive coagulopathy. Coagulopathy (laboratory proof or hemorrhage without an alternate explanation) four. Onset of the above throughout labor, cesarean supply, dilation and evacuation, or within 30 minutes postpartum 5. Proposed diagnostic standards for the case definition of amniotic fluid embolism in analysis research. One regional surveillance system in Australia has developed the capacity to systematically evaluation records for all instances identified from administrative data. Steiner and Lushbaugh, two pathologists from the University of Chicago, described a case series of eight autopsies after deadly intrapartum shock. Fetal squamous cells and syncytiotrophoblasts display excessive concentrations of tissue issue and phosphatidylserine. As pregnancy progresses, rising quantities of tissue factor, a potent procoagulant, accumulates within the amniotic fluid. During the preliminary part, acute pulmonary hypertension ends in proper ventricular dilation, a lower in cardiac output, and ventilation-perfusion (V/Q) mismatch resulting in oxygen desaturation. Maternal symptoms began just earlier than the onset of spontaneous uterine tachysystole and fetal bradycardia. A chest radiograph might present diffuse bilateral heterogeneous or homogenous areas of opacity.
Minocycline 50 mg fast delivery
Minimum analgesic doses of fentanyl and sufentanil for epidural analgesia in the first stage of labor best antibiotics for acne uk buy minocycline 50 mg on-line. The addition of pethidine to epidural bupivacaine in labour�effect of adjusting bupivacaine energy bacterial throat infection cheap 50 mg minocycline amex. Shivering associated to epidural blockade with bupivacaine in labour, and the affect of epidural pethidine. Bupivacaine with meperidine versus bupivacaine with fentanyl for continuous epidural labor analgesia. An isobolographic analysis of diamorphine and levobupivacaine for epidural analgesia in early labour. Plasma concentrations of bupivacaine throughout steady epidural analgesia in labour: the impact of adrenaline. Levobupivacaine-sufentanil with or without epinephrine throughout epidural labor analgesia. Extradural pethidine with and with out adrenaline during labour: extensive variation in impact. Minimum analgesic dose of epidural sufentanil for first-stage labor analgesia: a comparison between spontaneous and prostaglandin-induced labors in nulliparous ladies. The development and validation of a dynamic mannequin to account for the progress of labor within the assessment of ache. Pitfalls in chronobiology: a advised evaluation utilizing intrathecal bupivacaine analgesia for example. Epidural infusion of alfentanil or diamorphine with bupivacaine in labour-a dose discovering research. Epidural analgesia for labour using a steady infusion of bupivacaine and alfentanil. A comparability of the native anesthetic results of meperidine, fentanyl, and sufentanil on dorsal root axons. The dose-sparing effect of clonidine added to ropivacaine for labor epidural analgesia. Impact of the addition of sufentanil 5 �g or clonidine 75 �g on the minimum native analgesic focus of ropivacaine for epidural analgesia in labour: a randomized comparison. Patient-controlled epidural analgesia in labor: the addition of clonidine to bupivacaine-fentanyl. Clonidine added to bupivacaine-epinephrine-sufentanil improves epidural analgesia during childbirth. Effects of a continuous low-dose clonidine epidural regimen on pain, satisfaction and opposed occasions during labour: a randomized, double-blind, placebo-controlled trial. Addition of clonidine to a continuous patient-controlled epidural infusion of low-concentration levobupivacaine plus sufentanil in primiparous girls throughout labour. Effects of epidural clonidine and neostigmine following intrathecal labour analgesia: a randomised, double-blind, placebo-controlled trial. The effect of clonidine on the minimum local analgesic concentration of epidural ropivacaine during labor. The effect of epidural neostigmine combined with ropivacaine and sufentanil on neuraxial analgesia during labor. Epidural neostigmine combined with sufentanil supplies balanced and selective analgesia in early labor. Neostigmine decreases bupivacaine use by patient-controlled epidural analgesia throughout labor: a randomized managed research. Antinociceptive results of spinal cholinesterase inhibition and isobolographic analysis of the interplay with mu and alpha 2 receptor systems. Epidural neostigmine and clonidine improves the quality of mixed spinal epidural analgesia in labour: a randomised, double-blind controlled trial. Efficacy and facet effect profile of various doses of intrathecal fentanyl added to bupivacaine for labor analgesia. Synergistic interplay between fentanyl and bupivacaine given intrathecally for labor analgesia. Minimum native analgesic dose of intrathecal bupivacaine in labor and the impact of intrathecal fentanyl. Analgesia, pruritus, and air flow exhibit a dose-response relationship in parturients receiving intrathecal fentanyl throughout labor. Blood strain, but not cerebrospinal fluid fentanyl focus, predicts period of labor analgesia from spinal fentanyl. Determination of the dose-response relationship for intrathecal sufentanil in laboring sufferers. Intrathecal sufentanil and epidural bupivacaine for labor analgesia: dose-response of individual brokers and together. Observational examine of the effect of mu-opioid receptor genetic polymorphism on intrathecal opioid labor analgesia and post-cesarean delivery analgesia. Duration of analgesia and pruritus following intrathecal fentanyl for labour analgesia: no important impact of A118G mu-opioid receptor polymorphism, but a marked effect of ethnically distinct hospital populations. Determination of the total dose-response relation of intrathecal bupivacaine, levobupivacaine, and ropivacaine, combined with sufentanil, for labor analgesia. Intrathecal administration of hyperbaric morphine for the relief of ache in labour. Small dose bupivacaine-fentanyl spinal analgesia mixed with morphine for labor. The addition of morphine prolongs fentanyl-bupivacaine spinal analgesia for the relief of labor pain. Addition of low-dose morphine to intrathecal bupivacaine/sufentanil labour analgesia: a randomised managed study. Comparison amongst intrathecal fentanyl, meperidine, and sufentanil for labor analgesia. Subarachnoid meperidine (Pethidine) causes important nausea and vomiting throughout labor. Analgesia for labour and delivery utilizing incremental diamorphine and bupivacaine via a 32-gauge intrathecal catheter. Choice of opioid for initiation of mixed spinal epidural analgesia in labour�fentanyl or diamorphine. Intrathecal bupivacaine reduces pruritus and prolongs period of fentanyl analgesia during labor: a prospective, randomized managed trial. Minimum native analgesic doses of ropivacaine, levobupivacaine, and bupivacaine for intrathecal labor analgesia. Densities of dextrose-free intrathecal local anesthetics, opioids, and mixtures measured at 37 degrees C. Maternal posture influences the extent of sensory block produced by intrathecal dextrose-free bupivacaine with fentanyl for labor analgesia.
50 mg minocycline cheap fast delivery
Regardless of location antibiotic resistance gene database buy minocycline 50 mg free shipping, the gear can taking antibiotics for acne make it worse minocycline 50 mg order overnight delivery, services, and assist personnel out there in the labor and delivery working room must be comparable to those out there in the primary working room. The instant availability of these sources is particularly important, given the frequency and urgency of anesthesia care. Consideration ought to be given to having a variety of the gear and provides immediately available in one location or in a cart. Securing special-situation gear and provides in a cart with a single-use breakthrough plastic tie helps ensure that the cart is kept in a completely stocked state. Aspiration Prophylaxis the affected person must be asked about oral intake, although inadequate evidence exists regarding the relationship between current ingestion and subsequent aspiration pneumonitis (see Chapter 28). The volume of liquid ingested is less important than the absence of particulate matter. A fasting interval for solids of 6 to eight hours, relying on the fat content of the food, has been beneficial. Antibiotics with efficacy against gram-positive, gramnegative, and some anaerobic bacteria are commonly used for prophylaxis for cesarean supply. Appropriate coverage includes intravenous ampicillin 2 g, cefazolin 1 g, or ceftriaxone 1 g. Appropriate antibiotic coverage ought to final for three to four hours; due to this fact, ampicillin could also be much less acceptable owing to a shorter half-life than the cephalosporins. A 2016 randomized controlled trial addressed whether surgical site infection prophylaxis must be broadened to cowl species generally associated with postcesarean an infection. However, a meta-analysis demonstrated that preincision antibiotic prophylaxis reduces the incidence of postcesarean endometritis and total maternal infectious morbidity, without evidence of opposed neonatal results. Since that time, the apply of hand hygiene has brought on a major reduction in maternal and neonatal infectious morbidity. As a consequence, obstetric anesthesia suppliers should always give cautious attention to aseptic approach, particularly during performance of a neuraxial procedure. Proper sterile technique for neuraxial procedures contains wearing a face mask, performing hand hygiene, and donning sterile gloves (see Chapter 12). An increasing number of establishments are utilizing premixed solutions of native anesthetic and opioid (prepared beneath aseptic situations in a hospital or compounding pharmacy) to limit breaches in aseptic method in the course of the administration of neuraxial anesthesia. Intravenous Access and Fluid Management the institution of functional intravenous entry is of crucial importance to the successful outcome of many medical conditions in obstetric anesthesia practice. Because the dimensions of the catheter, more than the size of the vein, dictates the move price, the usage of a brief, large-diameter catheter. Smaller catheters could also be acceptable in an emergency; quantity and blood resuscitation can be satisfactorily achieved using 20- and 22-gauge catheters (without evidence of higher purple blood cell destruction) with the use of dilution, pressurization, or each. The kind of fluid (crystalloid, colloid) and the amount, rate, and timing of administration are related factors in the prevention and treatment of hypotension. Traditionally, roughly 1 L of crystalloid resolution has been administered intravenously (as "prehydration" or "preload") to stop or scale back the incidence and severity of hypotension during neuraxial anesthesia for cesarean supply. However, prehydration, even with massive volumes (30 mL/kg), is minimally effective in preventing neuraxial anesthesia-induced hypotension. For patients at excessive risk for hypotension or the implications of hypotension, colloid could additionally be administered earlier than or on the time of initiation of neuraxial blockade. Supplemental Medications for Anxiety the administration of benzodiazepines, even low doses. However, every so often, particularly in girls with extreme anxiety or undergoing an emergency cesarean delivery, the utilization of low doses of intravenous midazolam or an opioid may facilitate performance of a neuraxial technique, awake tracheal intubation, or the induction of common anesthesia. The supine hypotension syndrome, which is brought on by compression of the aorta and inferior vena cava by the gravid uterus, can manifest as pallor, tachycardia, sweating, nausea, hypotension, and dizziness. Fifteen degrees of left lateral tilt (left uterine displacement) has been proposed to significantly reduce the antagonistic hemodynamic penalties of the supine place, although both the aorta and inferior vena cava might stay partially compressed. The editors have chosen to retain the use of the abbreviation �g all through this textual content. Lateral tilt ought to be utilized in all ladies in mid- to late being pregnant after the administration of neuraxial or general anesthesia, with larger tilt used when possible if aortocaval compression is suspected because the trigger for maternal or fetal compromise. If blankets are used to create the ramp place, they need to be stacked somewhat than interlaced, to permit for rapid removal and readjustment of the top and neck position if needed. The value of this method in stopping hypotension during neuraxial anesthesia has been questioned. Whether using the lateral or the sitting place is greatest for routine initiation of neuraxial anesthesia is controversial. Theoretically, the lateral position could also be of value during development of an epidural needle as a result of it minimizes the prominence of the dural sac. Bulging of the lumbar dural sac-particularly within the sitting position-may decrease the drive required to create a dural puncture with a Tuohy epidural needle, however this chance is unproven. The sitting place also has some benefits, together with simpler landmark recognition in overweight parturients and ease of positioning sufferers in a symmetrical place (the spine is usually rotated in the lateral position because the underside shoulder is fixed). It grew to become a typical follow following the seminal report by Fox and Houle100 that demonstrated improved oxygenation, higher umbilical twine blood acid-base measurements, and fewer time to sustained respiration within the neonate, when mothers present process cesarean delivery with neuraxial anesthesia breathed one hundred pc oxygen as an alternative of air for at least 10 minutes. However, later evidence instructed that routine oxygen administration could additionally be pointless, ineffective101 and presumably detrimental. Nonetheless, the emergency cesarean supply of the compromised fetus ought to include maternal oxygen administration of excessive Fio2, significantly within the setting of uterine contractions, which may exacerbate fetal compromise; in these situations, supplemental oxygen may cut back the severity of fetal hypoxia with limited oxygen free-radical effects. The activity of those compensatory mechanisms and their relationship to gestational age and labor recommend that the highest risk for ischemia-reperfusion damage occurs in preterm fetuses earlier than the onset of labor. Of curiosity, when asphyxiated infants are instantly resuscitated at start with air as an alternative of 100% oxygen, higher shortterm outcomes have been observed114,115; this discovering could additionally be a result of the shift within the stability between beneficial oxygenation and detrimental free radicals. Although the worth of supplemental oxygen use throughout elective cesarean supply with neuraxial anesthesia of a noncompromised fetus is questionable, some obstetric anesthesia providers place nasal cannulae or a mask to monitor air flow using expired carbon dioxide evaluation. The most applicable anesthetic technique for cesarean supply depends on maternal, fetal, and obstetric elements (Table 26. The urgency and anticipated duration of the operation play an essential role within the choice of an anesthetic approach. A standardized four-grade classification system may be used to communicate the degree of urgency amongst providers (Table 26. Effective communication with the obstetric staff is critical to establish the diploma of urgency, which helps guide decisions relating to anesthetic administration. Further, contemporary standards for affected person security require that each one members of the surgical staff take part in a preoperative "time-out" to verify (1) the correct affected person identification, place, and operative web site; (2) agreement on the procedure to be performed; and (3) the supply of special gear, if needed. In circumstances of emergency cesarean supply, the emotional needs of the mom and father are additionally important. Parental distress generally occurs on this setting, and the anesthesia provider is usually the best particular person to give reassurance. In up to date practice, neuraxial anesthesia is run to some patients who would have acquired common anesthesia up to now. Umbilical cord prolapse, placenta previa, and preeclampsia with extreme options are now not thought-about absolute indications for general anesthesia. For instance, in some cases a prolapsed umbilical cord can be decompressed, and if fetal status is reassuring, a neuraxial approach can be used.
Generic 50 mg minocycline free shipping
Recovery after nulliparous birth: a detailed evaluation of pain analgesia and restoration of function antibiotic resistance scholarly articles purchase minocycline 50 mg on-line. Moving past ache as the fifth vital signal and affected person satisfaction scores to improve ache care within the 21st century infection in finger 50 mg minocycline with amex. Dose response to intrathecal diamorphine for elective caesarean section and compliance with a national audit commonplace. Chronic ache after vaginal and cesarean delivery: a reality questioning our day by day practice of obstetric anesthesia. The short-lasting analgesia and long-term antihyperalgesic effect of intrathecal clonidine in sufferers present process colonic surgical procedure. Intraoperative epidural analgesia mixed with ketamine provides efficient preventive analgesia in sufferers present process main digestive surgery. Patient choice compared with no choice of intrathecal morphine dose for caesarean analgesia: a randomized scientific trial. Principles of Analgesic Use in the Treatment of Acute Pain or Chronic Cancer Pain. Patient controlled opioid analgesia versus non-patient controlled opioid analgesia for postoperative pain. An updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Comparison of patient-controlled epidural analgesia with patient-controlled intravenous analgesia utilizing pethidine or fentanyl. Morphine for post-caesarean section analgesia: intrathecal, epidural or intravenous Epidural narcotic and patient-controlled analgesia for post-cesarean part pain aid. Analgesia after caesarean section: patient-controlled intravenous morphine vs epidural morphine. Respiratory and haemodynamic effects of acute postoperative pain administration: proof from printed information. Respiratory despair in grownup sufferers with intravenous patient-controlled analgesia. Variables of patient-controlled analgesia 4: the relevance of bolus dose size to supplement a background infusion. Analgesic efficacy and potency of two oral controlled-release morphine preparations. Oral analgesia in contrast with intravenous patient-controlled analgesia for pain after cesarean delivery: a randomized controlled trial. Pain management after cesarean: a randomized managed trial of oxycodone versus intravenous piritramide. The worth of "multimodal" or "balanced analgesia" in postoperative ache remedy. Fixed time interval compared with on-demand oral analgesia protocols for post-caesarean ache: a randomised controlled trial. Effects of acetaminophen on morphine side-effects and consumption after major surgery: meta-analysis of randomized managed trials. Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs for the reduction in morphine-related side-effects after major surgery: a systematic evaluate. Does multimodal analgesia with acetaminophen, nonsteroidal antiinflammatory medication, or selective cyclooxygenase-2 inhibitors and patient-controlled analgesia morphine supply advantages over morphine alone Small doses of intrathecal morphine mixed with systemic diclofenac for postoperative pain control after cesarean delivery. A double-blind randomised controlled trial of paracetamol, diclofenac or the mix for pain aid after caesarean section. A randomized, controlled trial to compare ketorolac tromethamine versus placebo after cesarean part to reduce ache and narcotic utilization. A randomised managed trial of parecoxib, celecoxib and paracetamol as adjuncts to patient-controlled epidural analgesia after caesarean supply. The impact of celecoxib on intrathecal morphine-induced pruritus in sufferers present process caesarean section. Transfer of parecoxib and its main lively metabolite valdecoxib by way of transitional breastmilk following intravenous parecoxib use after cesarean supply: a comparability of naive pooled information analysis and nonlinear mixed-effects modeling. Effect of perioperative systemic alpha-2 agonists on postoperative morphine consumption and pain intensity: systematic review and meta-analysis of randomized controlled trials. Intravenous dexmedetomidine as an adjunct for labor analgesia and cesarean supply anesthesia in a parturient with a tethered spinal twine. Intravenous dexmedetomidine for cesarean supply and its concentration in colostrum. Contemporary usage of obstetric magnesium sulfate: indication, contraindication, and relevance of dose. Effect of perioperative gabapentin on postoperative pain decision and opioid cessation in a combined surgical cohort: a randomized scientific trial. Mechanisms of lowering postoperative pain, nausea and vomiting: a scientific evaluate of present techniques. A randomized, managed trial validates a peripheral supra-additive antihyperalgesic effect of a paracetamol-ketorolac combination. Combining paracetamol (acetaminophen) with nonsteroidal antiinflammatory medication: a qualitative systematic evaluation of analgesic efficacy for acute postoperative pain. Normal postoperative gastric emptying after orthopaedic surgical procedure with spinal anaesthesia and that i. Plasma and cerebrospinal fluid pharmacokinetic parameters after single-dose administration of intravenous, oral, or rectal acetaminophen. Effect of administration of ketorolac and native anaesthetic infiltration for pain aid after laparoscopic-assisted vaginal hysterectomy. Nonsteroidal anti-inflammatory medication during being pregnant and the initiation of lactation. High-dose diclofenac for postoperative analgesia after elective caesarean part in regional anaesthesia. Gabapentin improves postcesarean delivery pain administration: a randomized, placebo-controlled trial. Low-dose intravenous ketamine improves postoperative analgesia after caesarean delivery with spinal bupivacaine in African parturients. Low-dose ketamine with multimodal postcesarean supply analgesia: a randomized managed trial. Intravenous ketamine throughout spinal and common anaesthesia for caesarean part: systematic review and meta-analysis. A survey of perioperative and postoperative anesthetic practices for cesarean supply. Analgesia after cesarean supply: affected person evaluations and prices of five opioid strategies. Patient-controlled analgesia following cesarean part: a comparison with epidural and intramuscular narcotics.