
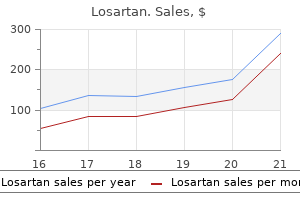
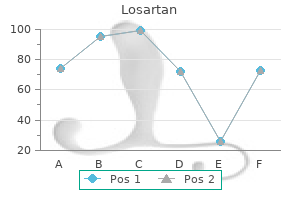
Losartan dosages: 50 mg, 25 mg
Losartan packs: 28 pills, 56 pills, 112 pills, 224 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

50 mg losartan cheap amex
The excess adipose tissue is excised diabetes mellitus definition idf safe 50 mg losartan, and an enough fascial incision is made to accommodate the ileum or neourethra diabetes symptoms when blood sugar is low buy 50 mg losartan visa. Once the fascial opening is discovered to be ample to avoid neourethral narrowing, the pouch is anchored to the anterior belly wall with four to six interrupted 0 permanent sutures to avoid torsion, peristomal hernias, and especially kinking of the pouch-neourethra, which might prevent passage of the Foley catheter throughout self-catheterization. Step eight Large drains (at least 19F Jackson-Pratt or Bard Channel drains) are positioned within the neighborhood of the Miami pouch to permit evacuation of any urinary leak in the pouch or ureteral anastomosis. The authors customarily place an extra drain when a concomitant pelvic exenteration is performed, corresponding to a 16F Malecot drain, as a result of postoperative serous and sanguineous fluid accumulation is excessive. Step 9 the Foley catheter is left within the pouch for 14 days and flushed with one hundred to 200 mL of saline resolution every four hours or until mucus is cleared. The nephroureteral stents are removed on days 14 through 21 along with the Foley catheter after a contrast examine of the urinary reservoir and the ureters has been performed to ensure the absence of any urinary leakage, reflux, or upper tract obstruction. Minimally Invasive Approach to Urinary Diversion Robotic or laparoscopic urinary diversion has been described for some time within the urology literature, from laparoscopic hand-assisted formation of an ileal conduit to complete laparoscopic urinary diversion. Pomel and Castaigne (2004) described the first case of laparoscopic anterior pelvic exenteration with laparoscopic-assisted formation of a Miami pouch in a patient with adenocarcinoma of the cervix with bladder involvement. The estimated blood loss was 200 mL, 294 Section 9 Pelvic Reconstructive Procedures which is much lower than the quantity reported during an open process. The whole time of process including exenteration and reconstruction was 6 hours, and the patient was ambulatory on the following postoperative day; she skilled no postoperative issues. Lim (2009) was the primary to describe the utilization of the da Vinci robotic system (da Vinci Surgical System; Intuitive Surgical, Sunnyvale, California) for whole pelvic exenteration and formation of an ileal loop urinary diversion. The complete time for the whole pelvic exenteration was 225 minutes, and for the formation of the ileal loop urinary diversion, 120 minutes, with an estimated blood loss of 375 mL. Mart�nez and colleagues (2011) had been among the many first to report a retrospective cohort study comparing outcomes of sufferers who had undergone laparoscopic pelvic exenteration (14) for gynecologic malignancy and outcomes in those who had undergone an open pelvic exenteration (29) at one institution between 2000 and 2008. Martinez and colleagues reported no difference in operating time, length of keep, postoperative issues, or mortality, however transfusion rate was significantly greater among the laparotomy group. This process has historically been used less regularly in gynecologic oncology patients after exenteration due to tissue harm to the pelvis from radiation, which will increase the danger for urethra-neobladder anastomosis leak and urinary fistula formation, and due to the high danger of recurrence of gynecologic malignancy in the trigone or urethra, thus limiting candidacy for urethra-sparing surgical procedure. Three patients had a postoperative neobladder anastomotic leak, with one requiring reoperation. Patients have been happy with continence achieved with the neobladder, and all were glad with their determination to endure the procedure. Postoperative Care and Management of Postoperative Complications Immediate Postoperative Care As necessary as the intraoperative surgical technique and knowledge, the quick postoperative care is crucial in minimizing postoperative morbidity and mortality related to pelvic exenterations and urinary reconstruction. Patients present process surgical procedures as radical as pelvic exenteration and vaginal and urinary reconstruction are at excessive danger of postoperative complications on account of the radicality of the process and the patient comorbidities. The common danger of diversion-related complications has been reported to be approximately 30% to 50% within the largest series. This section describes the instant perioperative care and the evaluation and management of postoperative problems. Intensive Care Unit Admission All exenterative and urinary diversion sufferers are admitted to the intensive care unit for shut monitoring of vital indicators, respiratory fluid, and cardiac standing. Many of those patients remain intubated and require blood products because of fluid shift, imply blood lack of 1500 to 2000 mL, and other comorbidities. The median intraoperative transfusion amount was 4 items of packed red blood cells (75% of patients) in a single examine. At this time, the affected person needs to be taught proper irrigation and self-catheterization strategies. In the beginning, the patient will carry out self-catheterization every 2 to four hours and irrigate four occasions a day to keep away from obstruction till all mucus is cleared. The affected person could gradually decrease the frequency of catheterization as continence is achieved however ought to concentrate on signs indicating the necessity for bladder emptying such as stomach ache and fullness. Follow-up renal sonograms for hydronephrosis are paramount for recognizing and avoiding loss of the renal unit from ureteral strictures, which might happen months to years later. Foley Catheter the Foley catheter is left in place for 14 days and flushed with a hundred to 200 mL of saline solution till away from mucoid material each 6 hours for the primary couple of weeks to forestall accumulation of mucus produced by the colonic mucosa, which can result in obstruction, neobladder distention and pain, and even perforation. During discharge planning, the affected person ought to be taught how to self-catheterize and flush the neobladder two or three times per day in order that she can start doing so after she has been cleared to achieve this in the clinic. Drains the Jackson-Pratt or Bard Channel drains are continued for 10 to 14 days to enable evacuation of all intraabdominal blood and fluid, especially extravasated urine, which might result in peritoneal irritation. Management of Postoperative Complications the currently obtainable comparative retrospective studies have dispelled the parable that incontinent urinary diversions are safer for patients, albeit technically simpler to carry out, and should in fact cause larger morbidity on account of the chosen intestinal segment within an irradiated subject. In one of the largest evaluations of incontinent diversion that has addressed this subject, Tabbaa and colleagues (2014) reviewed 166 sufferers who had undergone incontinent urinary diversion creation, comparing only important diversion-related issues in the 30� and 90�postoperative day periods, outlined as the following: ureteral stricture, conduit leak, conduit obstruction, conduit ischemia, ureteral anastomosis leak, stent obstruction requiring intervention by way of interventional radiology process or reoperation, and renal failure. No important variations were found amongst sufferers who had undergone ileal, sigmoid, or transverse colonic conduit formation; however, sigmoid colonic diversions, within the isodose curves, more incessantly resulted in conduit-related issues necessitating intervention and extra procedures. Transverse colon conduits had been related to fewer problems, but a low outcome quantity made statistical evaluation difficult. Significant predictive features of postsurgical problems included sort of exenteration, anterior versus total (P <. Karsenty and colleagues reported comparable rates of both ureterorenal dilation Electrolytes the selection of intestinal phase similar to an ileocolonic neobladder can lead to particular metabolic abnormalities such as hyperchloremic metabolic acidosis from the physiologic excretion of bicarbonate via intestinal losses from the colonic mucosa. Of sufferers who undergo a urinary diversion, 30% to 50% will develop hyperchloremic metabolic acidosis. The chapter authors advocate a basic metabolic panel performed every day for the first few days and then weekly until the outcomes are steady. Electrolyte supplementation corresponding to with potassium and bicarbonate is widespread within the quick postoperative interval. Vitamin B12 is absorbed within the terminal ileum; due to this fact any urinary reservoir process that makes use of the terminal ileum as the reservoir will end in vitamin B12 deficiency because absorption may be compromised as a consequence of radiation fibrosis. It is usually asymptomatic, and it is recommended that vitamin B12 levels be followed in the long-term postoperative interval. Postoperative Antibiotics Antibiotics are used often after pelvic exenteration and urinary diversion in an try to lower the excessive price of postoperative infectious morbidity. A comparability of continent and incontinent urinary diversion after pelvic exenteration: a examine of long-term morbidity and renal function. Total pelvic exenteration: the Albert Einstein College of Medicine/Montefiore Medical Center expertise (1987 to 2003). Angioli and colleagues (1998) discovered that pyelonephritis not related to ureteral stricture or obstruction was found in 13 of seventy seven (16. If no obstruction is recognized, one can consider long-term suppressive therapy with daily antibiotic if greater than four episodes per year are diagnosed. Miami pouch, Salom and colleagues reported that only 3 of 90 sufferers developed stomal skin stricture; this was managed within the outpatient setting. Many of the sufferers who skilled hassle with catheterization within the early postoperative interval were found to have deviation of the ileal phase from overdistention of the reservoir, which shaped an acute angle from the pores and skin to the reservoir. Of the 5 sufferers who skilled issue self-catheterizing during the late postoperative interval, two sufferers were discovered to have stones that obstructed the pouch, and one affected person was discovered to have a deviated ileal stomal outlet that required surgical correction.
Diseases
- Trigeminal neuralgia
- Choledochal cyst, hand malformation
- Urophathy distal obstructive polydactyly
- Thyrocerebrorenal syndrome
- Myoclonus progressive epilepsy of Unverricht and Lundborg
- Neuropathy, hereditary sensory, type II
- Familial dilated cardiomyopathy
Losartan 25 mg generic visa
Furthermore metabolic disease ga-1 buy generic losartan 50 mg on line, low- and intermediate-risk sufferers who choose medical remedy should undergo symptom-limited managing diabetes food buy 25 mg losartan fast delivery, non-invasive stress testing to identify the cohort of sufferers with an i threat of antagonistic end result. Patients managed with an early conservative technique are likely to have an i would like for antianginal remedy and rehospitalization for angina, and many endure coronary angiography within the year. The strategy to sufferers with arrhythmias relies upon upon: � the effects of the rhythm on the affected person. Effects of the rhythm on the patient Patients with indicators of severe haemodynamic compromise � Impending cardiac arrest. Diagnosing the arrhythmia the main distinctions to make are: � Tachy- (>120/min) versus brady- (<60/min) arrhythmia. Ask specifically about situations identified to be related to sure cardiac arrhythmias. In haemodynamically unstable patients, some of these investigations might have to be accomplished after restoration of steady rhythm. Beware respiratory despair and have an anaesthetist, flumazenil, and naloxone to hand, and at all times ask for anaesthetic assistance if not experienced in this. If this is unsuccessful, they can be electrically cardioverted under sedation/ anaesthesia. Once the acute episode is over, contemplate referral to a heart specialist for: � Holter monitoring. Most sufferers will be haemodynamically unstable and should endure exterior defibrillation. The necessary distinction to make is between common and irregular tachyarrhythmias (see Table 1. Higher doses are required in sufferers on theophyllines, lower in patients on dipyridamole. Less commonly, it may present with an embolic event (stroke, peripheral embolus) or be asymptomatic. Investigations these ought to be directed at on the lookout for a precipitant and underlying heart disease. Immediate management Stabilize the patient � General measures (E Tachyarrhythmias coronary heart fee >120bpm, pp. This is especially helpful in patients with a fee of one hundred fifty bpm where atrial flutter should at all times be considered. If potential, goal to optimize the scientific image before cardioversion: � Hypokalaemia could also be rapidly corrected by giving 20mmol over 1h in 100mL of regular saline through a central line. Haemodynamically secure patients � the initial purpose ought to be speedy pharmacological fee management, followed by a choice concerning restoration of sinus rhythm if acceptable. Ventricular price might increase and fibrillatory waves coarsen earlier than reverting to sinus rhythm, so load with digoxin/-blocker/verapamil before giving this. Dosing requires a central line, and it might take 24�48h for sinus rhythm to be achieved. Amiodarone has relatively poor fee control properties and will need to be combined with a -blocker or verapamil initially. Digoxin, with or without amiodarone, is an effective mixture (amiodarone will improve the plasma digoxin level, so halve the maintenance digoxin dose). The present trend is to hold patients at average or excessive danger of thromboembolism on anticoagulation life-long, except there are concerns. Discuss with a cardiac electrophysiologist, as with increasing success of the process and lowered danger, this must be thought-about for all patients with resistant or recurrent flutter. Management � the one true effective remedy is to treat the underlying illness. Management Haemodynamically unstable patients � Give O2 through face masks if the patient is hypoxic on air. Look for a supply of blood loss, and start aggressive resuscitation with fluids and inotropes. It could also be of worth to have appropriate central venous access (femoral or inner jugular vein) in place in case of want for emergency momentary wire insertion. However, when related to haemodynamic disturbance or progression to larger levels of block (even if intermittent), insertion of a transvenous pacing wire have to be thought-about. The want for longer-term pacing relies on the persistence of symptoms and underlying cause. Causes � � � � � � � � � � � � � � � � � Associated with acute infarction or ischaemia. Management � Principles are listed beneath E Bradyarrhythmias: common strategy, pp. It could additionally be difficult to differentiate the two clinically, and indeed sometimes they might coexist. Further management Subsequent management of the affected person is geared toward guaranteeing adequate ventilation/gas exchange, making certain haemodynamic stability, and correcting any reversible precipitants of acute pulmonary oedema. However, it could worsen tachycardia, and it might be arrhythmogenic and decrease potassium levels (K+) (supplement to ensure K+ ranges are 4�5mmol/L). The most common aetiology is cardiogenic shock, but keep in mind non-cardiogenic causes. The alternative of inotropic agent is determined by the clinical condition of the patient and, to some extent, the underlying analysis. However, tachycardia and/or hypotension secondary to peripheral vasodilatation may restrict its effectiveness. However, it tends to increase the pulmonary capillary filling stress further and ought to be mixed with vasodilators. Arterial strain should be monitored constantly via an arterial line to forestall inadvertent hypotension. Anaemia � Cardiac failure could additionally be worsened or precipitated by the presence of serious anaemia. Presentation could be insidious, as in streptococcal infections, with putting constitutional symptoms, corresponding to with Staphylococcus aureus. Presenting features can embrace the next: � Symptoms and indicators of the an infection: these embrace malaise, anorexia, weight reduction, fever, rigors, and night time sweats. Complications of the an infection � Local effects: � Valve destruction ends in a new or changing murmur. A excessive index of suspicion have to be maintained if patients present with unexplained fever, a predisposing cardiac lesion, bacteraemia, and an embolic phenomenon. The Duke classification has been devised to assist with the analysis: � Definite endocarditis: two main standards, or one major and three minor criteria, or 5 minor criteria. Evidence of endocardial involvement � Positive echocardiogram: � Oscillating intracardiac mass (vegetation). In steady patients on antibiotic therapy, doses have to be delayed to permit culture on successive days.
Safe losartan 25 mg
Anterior to these nodes type 1 diabetes simple definition losartan 50 mg order amex, the superior hypogastric plexus offers origin to the hypogastric nerves definition of diabetes mellitus type 2 losartan 25 mg cheap mastercard. Technique After correct exploration of the abdomen and pelvis, one should acquire any fluid within the belly or pelvic cavity and submit this for cytologic analysis. The medial leaf of the peritoneum is opened, making a "window" to help avoid ureteral injury. If the surgeon prefers to not make the window, the ureter should be checked earlier than this step. This choice is helpful with mucinous tumors as a result of time to evacuate the cyst contents may be prolonged because of the cyst content material being very viscous. A good choice for evacuation of the cyst is to exteriorize the bag by way of the trocar within the stomach wall and to aspirate it underneath direct visualization. This step can additionally be done through the vagina if a hysterectomy has been carried out. The umbilical port can be used because the extraction web site if after cyst aspiration the bag can be easily extracted without enlarging the umbilical incision. For very giant cysts (>20 cm), we perform a small suprapubic incision to evacuate the cyst and extract it from the abdomen with a wound protector. We use the Applied Medical Laparoscopic Surgery for Ovarian Neoplasms Adnexectomy for Suspected Ovarian Cysts (Video 25. This method is associated with reductions in fever, urinary tract an infection, postoperative complications, postoperative ache, variety of days within the hospital, and total value. In cases of mucinous tumors, rupture throughout surgical manipulation may cause secondary tumors with prominent pseudomyxoma ovarii. The surgeon is slicing the omentum alongside the transverse colon while holding it with the left hand; the assistant pulls the omentum. While part of the ovary is exterior the stomach, the adnexectomy may be easily performed laparoscopically. The adnexa is extracted and sent for frozen part analysis to determine further intraoperative administration. Placement of Endobags within the Surgical Field Inserting an Endobag into the abdominal cavity may be difficult, significantly when the adnexal cyst is bigger than eight cm. Once the Endobag is inside the cavity, it have to be opened before one tries to place it posteriorly to the ovary. During coagulation or sealing of the omental vessels, you will want to be certain that the vessel-sealing device is kept a secure distance from the colonic serosa to keep away from thermal injury. As the surgeon progresses with the transection of the omental vessels, the assistant retains pressure on the omentum. Usually, the omental attachment to the splenic flexure is simpler to dissect from lateral to medial (left to right). At this point, the surgeon pulls the left border of the omentum medially, and the assistant pushes the descending colon (close to the splenic flexure) laterally whereas the surgeon detaches the omentum by using the sealing gadget with the best hand. The dissection is now from left to proper, up to the second the section areas meet and the omentectomy is accomplished. This method ought to be utilized in choose sufferers, because on the lateral features of the omentum, along the splenic and hepatic flexures of the colon, the resection is tougher and may be incomplete. Key Points � Oncologic outcomes of laparoscopic and open approaches are equivalent in most gynecologic malignancies. The surgeon faces the superior abdomen whereas the second assistant pulls the omentum downward and medially with traction on the hepatic flexure of the colon. Laparoscopic pelvic lymphadenectomy within the staging of early carcinoma of the cervix. Total laparoscopic radical hysterectomy with pelvic lymphadenectomy utilizing the argonbeam coagulator: pilot data and comparability to laparotomy. Laparoscopy versus laparotomy for the surgical management of apparent early stage ovarian most cancers. A comparative examine of 3 surgical strategies for hysterectomy with staging for endometrial most cancers: robotic help, laparoscopy, laparotomy. Total laparoscopic hysterectomy versus abdominal hysterectomy within the remedy of sufferers with early stage endometrial most cancers: a randomized multi middle examine. A comparative element analysis of the educational curve and surgical consequence for robotic hysterectomy with lymphadenectomy versus laparoscopic hysterectomy with lymphadenectomy in therapy of endometrial cancer: a case-matched managed examine of the primary 100 twenty two patients. Updating of a latest meta-analysis of randomized managed trials to assess the protection and the efficacy of the laparoscopic surgical procedure for treating early stage endometrial most cancers. Safety of laparoscopy versus laparotomy in early-stage endometrial cancer: a randomised trial. Minimally invasive surgical administration of early-stage cervical cancer: an evaluation of the risk factors of surgical issues and of oncologic outcomes. Comparison of the prognosis and recurrence of apparent early-stage ovarian tumors handled with laparoscopy and laparotomy: a meta-analysis of scientific studies. Analysis of secondary cytoreduction for recurrent ovarian most cancers by robotics, laparoscopy and laparotomy. Chemotherapy versus surgical procedure for initial treatment in advanced ovarian epithelial cancer. Definition of a dynamic laparoscopic model for the prediction of incomplete cytoreduction in advanced epithelial ovarian cancer: proof of an idea. Anesthetic considerations within the sufferers of persistent obstructive pulmonary illness present process laparoscopic surgical procedures. Impact of smoking on perioperative pulmonary and upper respiratory problems after laparoscopic gynecologic surgical procedure. Anesthetic challenges of patients with cardiac comorbidities present process main urologic surgical procedure. Port site metastasis after diagnostic laparoscopy for upper gastrointestinal tract malignancies: an unusual entity. Risk components contributing to early prevalence of port site metastases of laparoscopic surgical procedure for malignancy. Topical remedies of laparoscopic port websites can decrease the incidence of incision metastasis. Influence of cytotoxic agents on intraperitoneal tumor implantation after laparoscopy. A comparison of three different entry methods in gynecological laparoscopic surgical procedure: a randomized prospective trial. Comparison of complete laparoscopic and stomach radical hysterectomy for sufferers with early-stage cervical most cancers. Laparoscopic total radical hysterectomy by the Pune technique: our expertise of 248 cases. Laparotomy conversion fee of laparoscopic radical hysterectomy for early-stage cervical most cancers in a consecutive collection without case selection.
Cheap losartan 25 mg with amex
Alcoholics incessantly show vitamin D deficiency [35] diabetes test buy online 50 mg losartan mastercard, and subsequently diabetes mellitus vs diabetes insipidus buy cheap losartan 50 mg on-line, a relationship between muscle weak point and low vitamin D levels has been a matter of research. Additionally, among 90 alcoholics, we lately reported a big relationship between decreased lean mass and low vitamin D levels [38]. In any case, alcoholic myopathy and alcohol-induced pseudo-Cushing syndrome seem to be utterly completely different, unrelated, medical photos. However, the deleterious effect of ethanol on muscle mass already impacts muscle cell development. While axial and body wall musculature is generated by elongation of dermomyotome epithelium, limb musculature formation implies migration of progenitors from ventral dermomyotome [43,44]. Rearrangement of myofibrils, distribution of nuclei within the periphery, and reorganization of the cytoskeleton all happen in the course of the differentiation course of. This differential growth seems to happen underneath competitive rules closely influenced by environmental factors, like inflammatory or dietary standing [46]. Ethanol inhibits muscle cell differentiation [47] and skeletal muscle repair, by not solely interfering with myotube formation and MyoD and myogenin expression but additionally activating Notch-target genes, leading to inhibition of the myogenic fusion course of [48]. In addition, ethanol misuse results in continual irritation, which promotes expression of genes concerned in the nuclear issue kappa B pathway, downregulating myogenesis and selling adipogenesis. Inflammation-related oxidative stress additionally reduces ranges of -catenin, enhancing adipogenesis. Indeed, the offspring of mammalians subjected to dietary deprivation throughout pregnancy develop a collagen-rich skeletal muscle [46]. Induction of the muscle reparative transcription issue, ciliary neurotrophic factor, implicated in myotube differentiation, was delayed [9]. Akt phosphorylation promotes S6K-1 phosphorylation, which in turn exerts a unfavorable suggestions impact on Akt phosphorylation. Myostatin upregulation has been documented in alcohol-mediated cardiomyopathy [60], and experimental knowledge also assist a job of myostatin on muscle atrophy in alcoholic models. Elevated levels of myostatin may be related to obesity, suggesting a relationship between weight problems and muscle atrophy [62]. This finding is due to this fact linked with the function played by adiposity on muscle atrophy, a subject largely unknown in alcoholics. Insulin resistance is a common finding in obese patients and altered response to insulin signaling has also been observed in alcoholics [63]. One of the hormones produced in fats tissue is leptin which will increase resting power expenditure. Leptin exerts a positive impact on muscle, increasing fiber size and muscle mass and expression of myogenin. In a research on seventy nine alcoholics, we found low leptin levels in relation with fats mass-that was also reduced [66]. Increased Protein Breakdown Degradation of muscle proteins may theoretically play a role in ethanol-mediated muscle atrophy. In addition to the ubiquitin�proteasome machinery, theoretically inhibited by ethanol [67], there are several mobile mechanisms by which protein breakdown might ensue, together with several forms of regulated cell demise and/or breakdown of organelles. Regulated cell dying involves genetically encoded molecular pathways, distinguishing it from unintentional cell demise, by which a cell is destroyed after being exposed to overwhelming insults [68]. Several forms of regulated cell demise have been described, together with apoptosis, autophagy, necroptosis, pyroptosis, mitotic disaster, or mitoptosis [69], however the primary pathways which happen in alcoholic myopathy are apoptosis and autophagy. This final mechanism ought to be considered as an adaptative, prosurvival mechanism in situations of limited nutrition, by which the cell breaks down pointless organelles, whereas apoptosis is a programmed cell death. Two main pathways may be concerned in apoptosis activation, together with the mitochondrial pathway and dying receptor dependent pathways. This so known as extrinsic pathway, through caspase 8, additionally engages the mitochondrial pathway, leading to amplification of the apoptotic response [15]. Autophagy Another possibility that explains muscle protein loss in alcoholics is autophagy. The authors also showed that this effect was dependent on acetaldehyde somewhat than on ethanol itself. Autophagy could additionally be considered as a prosurvival mechanism, able to remove broken organelles and mitochondria probably capable of triggering apoptosis [72]. Therefore, the online effect of ethanol on autophagy and alcoholic myopathy needs additional research. Altered Carbohydrate Metabolism Data relating to alterations of carbohydrate metabolism in alcoholic myopathy are much less conclusive, and, in some circumstances, contradictory. In any case, the role of altered glucose utilization in the pathogenesis of alcoholic myopathy is unclear [76]. Oxidative damage may be as a end result of an imbalance between decreased exercise of the antioxidant systems and elevated free radical production. The chance that other metabolic pathways were also involved in mitochondrial oxidative injury was explored by Nguyen et al. Moreover, these alterations caused a rise in mitochondrial oxidative harm [88]. The authors also found that acetylcholinesterase expression in skeletal muscle was impaired, presumably in relation to oxidative stress. The most necessary intracellular antioxidant techniques include glutathione peroxidase and superoxide dismutase, and their enzymatic exercise critically is dependent upon the supply of sure hint parts, such as selenium, copper, zinc, and manganese. Ethanol-mediated deficiency of these elements in muscle tissue has been described in animal fashions [90], and serum selenium is lower in alcoholics [91,92]. Extracellular antioxidants, together with, amongst many others, vitamin E, ascorbic acid, and retinol, are additionally low in alcoholics, however information relative to a pathogenetic position on alcoholic myopathy are lacking. Overall, the position of oxidative stress in the pathogenesis of alcoholic myopathy continues to be a matter of debate. Together with well-established, strong information about some processes, there are still many obscure lacunae that want additional analysis. A fascinating new area of research is the analysis of the potential systemic effects brought on by alcoholic myopathy. In distinction with the basic concept that muscle was solely a comparatively inert structural, protein-storing organ, recent analysis has revealed that it can be thought-about an endocrine organ that secretes a quantity of molecules and growth elements which will have an effect on construction or perform of distant organs. The name myokines was coined by Pedersen in 2003 [103] to check with these molecules. Therefore, muscle disease, as is the case of alcoholic myopathy, might play causative damaging roles in distant organs. To our information, that is an open field of analysis that may most likely yield important data in the immediate future. Some examples of the significance of the relationships between myokines and the practical alteration of distant organs are outlined under. Muscle activity undoubtedly affects bone reworking, each by a direct impact of the increased mechanical drive on the Wnt-beta catenin canonical pathway and by oblique effects. In this sense, myostatin not solely increases bone resorption but additionally inhibits bone formation [105].
Shelum (Water Dropwort). Losartan.
- Are there safety concerns?
- Dosing considerations for Water Dropwort.
- Liver disease, high blood pressure, diabetes, abdominal pain, food poisoning, and other conditions.
- How does Water Dropwort work?
- What is Water Dropwort?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97087
Purchase 25 mg losartan with visa
Supportive therapy � Intensive care monitoring is crucial in any shocked patient or if important impairment of consciousness diabetes prevention workshops order losartan 25 mg without prescription. Supportive look after septic shock is mentioned underneath E Sepsis syndrome and septic shock managing diabetes in dogs losartan 25 mg buy low price, pp. Prognosis � Meningitis with out shock: mortality 710%, neurological sequelae uncommon. Remittent temperature progressively rising in the course of the first week to 40�C, with relative bradycardia. Azithromycin is a possible oral different if the isolate is quinolone-resistant. Ampicillin or amoxicillin (4�6g/day + probenecid 2g/day) or ciprofloxacin (750mg bd) for 4 weeks will clear 80�90% of patients, falling to 20�50% if the patient has gallstones. Cholecystectomy may eradicate carriage, however not usually indicated if carriage is asymptomatic. The vary of scientific disease brought on by these viruses is marked, but many cause severe lifethreatening disease. Transmission: human� human; attainable bat reservoir Incubation: 2�21 days Marburg virus Rural districts of Central and South Africa Transmission: animal (most probably bats)�human�human Incubation: 2�21 days Clinical features Fever, pharyngitis, retrosternal pain, proteinuria, headache, joint ache, stomach pain, and vomiting. It is a zoonosis (disease acquired from animals) and infects a range of domestic and wild animals. Outbreaks have just lately been recorded in Russia, Turkey, Iran, Kazakhstan, Mauritania, Kosovo, Albania, Pakistan, and South Africa. Hantavirus Hantaviruses are rodent-borne, zoonotic (acquired from animals) viruses. There are several totally different hantaviruses; some are present in Europe and Asia, whereas others occur in North and South America. Recognition is essential because rickettsial illnesses have significant mortality if left untreated. Macular rash begins at wrists and ankles, spreading to trunk, may be petechial or purpuric. Mortality 30% if untreated Eschar, painful regional lymphadenopathy, fever, headache, malaise, maculopapular rash in 60% Clinical options Murine typhus: Rickettsia typhi Spotted fever group Boutonneuse fever: R. There have been current outbreaks within the Netherlands, Australia, and the Mediterranean and Middle East areas. Complement fixation checks identify antibodies to phase 1 antigens (chronic infection. Treat with oral doxycycline (to attempt to prevent chronic infection), co-trimoxazole, rifampicin, or a quinolone. Aerobic and anaerobic cultures should be taken previous to treatment with antibiotics. Puncture wounds should be cleaned thoroughly and treated with prophylactic antibiotics (as described earlier). Clean the wound, swab for cardio and anaerobic cultures, tetanus prophylaxis as wanted, and prophylactic antibiotics (E Human bites, p. Presenting options are a viral prodrome, followed by paraesthesiae and fasciculations. Agitation, confusion, muscle spasms, localized paralysis, and brainstem dysfunction follow. It can be transmitted by bite and saliva and has brought on fatal disseminated infection in humans. If the bite is from a macaque from a colony not deemed away from the virus, consider starting valaciclovir 1g tds for 14 days, pending additional investigation. Staphylococcus aureus bacteraemia and right-sided endocarditis are severe issues. Patients with murmurs should have echocardiography to examine the potential of endocarditis. Multiple round lung infiltrates (� lysis) are characteristic of tricuspid endocarditis with septic emboli. Chronic swelling of both legs because of venous insufficiency or cardiac failure is usually fairly red in look. Presentations where each legs are purple should be fastidiously assessed for different diagnoses, including dermatitis, vascular phenomena/venous stasis, and haemosiderin deposition. Flucloxacillin 2g qds (barring allergy, renal impairment, or drug interactions) is frequently the preferred choice. Many sufferers may be managed with simply oral antimicrobials, and a total course length of 10�14 days may be warranted. Necrotizing fasciitis � Necrotizing fasciitis is a rare an infection of the subcutaneous tissues that tracks along fascial planes. Samples ought to be despatched for pressing Gram stain, as properly as culture and sensitivity testing. Further imaging previous to theatre merely delays the procedure with out providing further therapeutic data. Controlled decontamination important Melioidosis Antitoxin given on scientific suspicion The threat of growing scientific illness is 5% in the first 5 years after exposure, and an extra 5% over subsequent lifetime. Less generally, erythema nodosum, pericardial disease, or scrofuloderma could also be apparent. Culture could take as a lot as 6 weeks and antimicrobial susceptibility testing usually takes an additional 2 weeks. Public Health � Isolation: a facet room with respiratory precautions for suspected pulmonary illness. It is important to consult with specialists earlier than prescribing any specific therapies. General principles � the use of combination antiretroviral therapy is very successful. Examination of the mouth can reveal a great deal of info concerning the extent of immunity [e. If the patient declines or has further questions, then you will want to dispel any misconceptions and detail the advantages of testing (specifically that early diagnosis has a greater prognosis via access to remedy and that the disease, whereas presently incurable, has an excellent life expectancy, and so forth. However, this is justified within the following settings: � testing of organ transplantation donors. In this situation, testing is justified if the patient is unlikely to regain consciousness for 48h however should only be performed on a blood specimen that has been beforehand taken for one more purpose. Health-care providers for these diagnosed with tB, viral hepatitis B or C, and lymphoma.
25 mg losartan best
Once again metabolic disease 3 ps3 order 50 mg losartan, a self-retaining retractor is used diabetes prevention program outcomes study cheap 50 mg losartan with amex, allowing for maximal upward displacement of the costal margin. This may be carried out solely with an adequate incision at the facet of hepatic mobilization. Reliance on preoperative computed tomography or positron emission tomography imaging alone to establish small-volume diaphragmatic illness is inadequate. As beforehand discussed, liver mobilization begins with identification and transection of the spherical ligament through the use of a bipolar power device, followed by identification and transection of the falciform ligament. The leaves of the falciform are then dissected again toward the diaphragm by using electrosurgical energy, ultimately main the surgeon to the bilateral triangular and coronary ligaments. Any disease deposits involving the spherical ligament or falciform ligament ought to be resected presently. With dissection of the coronary ligaments, care should be taken to avoid damage to the underlying right and left hepatic veins. For adequate exposure of the best diaphragm to be achieved, complete hepatic mobilization is required. Specifically, with dissection of the right hepatic ligaments alone, rotation of the liver medially and inferiorly might end in significant vascular congestion. To allow the liver to rotate on its vascular axis, avoiding the hinge effect, the left triangular and coronary ligaments must also be launched. Division of the hepatogastric ligament may even help in full mobilization of the left hepatic lobe. The right-sided dissection is then continued by cauterizing and transecting the best coronary ligament, working from medial to lateral. The right liver parenchyma can then be mobilized medially, bringing into the operative field the right paracolic gutter and Morison pouch. Progressive dissection and medial mobilization will enable for exposure of the naked space of the liver and visualization of the best kidney and adrenal gland and a panoramic view of the best hemidiaphragm. In some instances, the operating surgeon may favor to start the dissection laterally, working from the best triangular ligament within the course of the falciform ligament medially. If a large adherent tumor plaque ends in agglutination of the liver floor and diaphragm peritoneum, the surgeon has two options. This will permit for entry to the anterior layer of the coronary ligament and completion of the diaphragm peritonectomy in a extra conventional style. Conversely, the surgeon may elect to dissect the tumor off of the adjoining diaphragmatic musculature by incising the diaphragm peritoneal reflection ventral Porta Hepatis Disease Uncommonly, metastatic ovarian most cancers implants may be identified within the porta hepatis. Given the important constructions housed within the hepatoduodenal ligament, an understanding of the anatomy is pivotal to successful resection. Furthermore, attempts at cytoreduction of disease on this location should be carried out when the anticipated surgical outcome is resection to no gross seen residual disease. Once the portal vein, hepatic artery, and customary bile duct have been identified and skeletonized, the metastatic disease may be dissected off of the underlying buildings, because infiltrative development patterns are unusual. Given the serious morbidity related to unintended injury to the porta constructions, hepatobiliary surgeons with expertise in this anatomic area must be consulted for intraoperative help. Similar methods are employed when porta hepatic adenopathy is recognized on preoperative imaging and the plan for resection is made. Surgical resection requires enough publicity, which depends on choice of an acceptable belly incision. We mostly use a vertical midline incision that extends from the pubic bone to instantly beneath the xiphoid course of, particularly when multiquadrant surgical resection is required (both pelvic and higher belly disease). In the much less widespread situation of targeted resection of recurrent diaphragmatic disease, a subcostal incision may be carried out, although this significantly limits exploration of the rest of the stomach cavity and is therefore not advocated. Roboticassisted surgical procedure and laparoscopy have been described for the resection of diaphragmatic disease, although both restrict retrohepatic exploration. The patient can be positioned within the low dorsal lithotomy place or supine on the working room desk. A curvilinear incision is created in the diaphragm peritoneum alongside the costal margin and grasped with clamps for traction. Dissection proceeds within the subperitoneal plane, working from ventral to dorsal and from lateral to medial. The diaphragm muscle is incised with electrocautery and the diseased space circumscribed with a visibly disease-free margin of resection. The dissection is then carried out in a dorsal course till the bare space of the liver is recognized. After liver mobilization, the best lobe of the liver is placed gently behind a self-retaining retractor blade or manually retracted. Subsequently, a curved incision is made alongside the diaphragm peritoneum, following the costal margin. The incised fringe of the diaphragm peritoneum is then elevated and placed on traction through the use of ring forceps or sequential Allis clamps. If the appropriate plane is troublesome to delineate anteriorly, the dissection may be started laterally at the junction of the paracolic gutter and Morison pouch. The dissection proceeds from the ventral to the dorsal path and laterally to medially, till the naked area is reached and the specimen has been resected. Full-Thickness Diaphragm Resection Occasionally, a full-thickness diaphragm resection is required for successful resection of disease that has invaded the diaphragm muscle, rising beyond and obliterating the normal subpleural plane. Liver mobilization is performed as described earlier, and the peritonectomy is began in a traditional trend. The incision ought to be carried parallel to the branching phrenic nerve to keep away from pointless damage and limit diaphragmatic dysfunction after the operation. During resection, branches of the phrenic artery and vein may be encountered and should must be managed with a suture ligature or bipolar vitality device. After removal of the specimen, the stomach and peritoneal surfaces must be recognized for the pathologist. The pleural cavity can additionally be visibly and manually explored to consider for illness. In addition, evaluation for the presence of an enlarged cardiophrenic lymph node can be performed presently. In practically all cases, major closure of the diaphragm could be accomplished with both interrupted figure-of-eight sutures or a operating locked sew through the use of a 1-0 or 2-0 nonabsorbable monofilament suture. Before the final suture is secured, a fenestrated 14F red Robinson catheter is placed into the pleural space, and along side positive-pressure air flow by the anesthesiologist, the catheter is connected to low steady suction evacuating the pneumothorax, and eliminated as the ultimate sew is secured. A postoperative chest radiograph is obtained to consider for a residual pneumothorax. The tip of the chest tube is then directed into the superior facet of the lung manually, avoiding injury to the underlying 168 Section 5 Ovarian Cancer lung parenchyma. The chest tube is then attached to a standard evacuation system (Pleur-evac; Teleflex, Morrisville, North Carolina), sutured in place to the chest wall, and dressed. In an effort to reduce the discomfort related to conventional chest tube placement, variations have been developed and include use of a 15F or 19F Jackson-Pratt drain (Cardinal Health, Dublin, Ohio) within the pleural area. The drain is handed through the diaphragm defect, into the pleural house, exiting the chest wall in the fifth or sixth intercostal house, along the midclavicular line. The drain is then sutured into place and connected to commonplace bulb suction, incorporating a stopcock into the drainage system to keep away from inadvertent introduction of air into the pleural space (pneumothorax) during bulb emptying.
Quality 50 mg losartan
Management Supportive therapy with blood and platelet transfusion and hydration is usually sufficient newcastle university diabetes diet losartan 50 mg generic otc. Discuss with urologists if severe diabetes diet education materials 50 mg losartan cheap mastercard, as more specialist intervention, such as bladder irrigation, may be required. Severely sick patients and people on steroids may not be capable of mount a fever; indicators corresponding to tachypnoea, tachycardia, or hypotension should be thought of serious. Basic microbiological investigations � Blood cultures: taken from Hickman line and by venepuncture. Important factors � Antibiotic therapy should never be delayed to await further assessment of scientific progress or laboratory outcomes. Central traces and urinary catheters must be inserted with platelet cover, and arterial puncture is finest prevented (use pulse oximetry). Antimicrobial routine When in doubt, take haematological recommendation; use the hospital policy. Monotherapy is usually inappropriate, even when an organism has been isolated; the affected person could well have >1 an infection. Duration of neutropenia is an important factor, as fungal infections turn out to be extra doubtless the longer the interval of neutropenia. It is effectively prevented and handled with aciclovir; the principle complication is bacterial super-infection. Have a excessive index of suspicion and deal with aggressively with amphotericin or fluconazole. There is intensive native tissue destruction with cavitating lung lesions or bone destruction of sinuses. Different pathogens are usually implicated in infections, depending on the degree of immunocompetence of the patient: � the neutropenic affected person (E the febrile neutropenic affected person 1, p. Cell-mediated immunity may be impaired for a number of months after bone marrow (and solid organ) transplantation. Immediate administration � Ensure sufficient respiration; seek the assistance of the anaesthetist and think about CpAp/invasive ventilation early if O2 requirements are increasing or the affected person is turning into exhausted. Presentation Most sufferers develop signs when serum viscosity reached 5�6 centipoises (normal <1. Management Arrange pressing intervention (same day), relying on the cause: � polycythaemia: � Venesect 1�2U. It is most likely to occur with bulky, extremely chemosensitive lymphoproliferative illness. Features � Uric acid 476 micromol/L or 25% enhance from baseline � urate nephropathy and oliguric renal failure. Prevention � Start allopurinol 300mg od (or bd) 48h prior to chemotherapy if renal perform is normal. Monitor U&Es, pO43�, Ca2+, and urate a minimal of twice daily for the first few days of therapy. Presentation � nausea, vomiting, drowsiness, confusion, nocturia, polyuria, bone and stomach pains, constipation. Massive mediastinal mass Presentation � Dry cough, stridor, and dyspnoea, especially on mendacity flat. Management Histological analysis (or cytological from pleural effusion if present): � General anaesthetic carries considerable threat. If left untreated, joint destruction is fast-50% of cartilage proteoglycan is lost inside 48h; bone loss is obvious inside 7 days; mortality of Staphylococcus aureus arthritis is 10%. Practice points � Always assume that a monoarthritis is because of sepsis till proven in any other case. Aspirate any cutaneous pustules for Gram stain in sufferers with suspected gonococcal an infection. Prosthetic joints should be aspirated by the orthopaedic group in theatre-liaise with them and contemplate early arthroscopy to facilitate effective joint washout, especially if inflammatory markers are slow to fall. Use cautiously within the aged, sufferers with peptic ulceration, or sufferers with asthma, cardiac failure, or renal or liver disease. In renal impairment, scale back the dose to 500 micrograms every 12h and monitor renal perform. Oral prednisolone (20�30mg/day) may be given for 3�5 days and then tapered over 7�10 days. Investigations � Aspirate a big affected joint and analyse the synovial fluid (E Joint aspiration, p. Signs most common in hands, toes, knees-but remember synovial joints of the backbone (and atlantoaxial joint/ligaments) and larynx (arytenoid joints). Most generally methotrexate, however others corresponding to hydroxychloroquine, sulfasalazine, and leflunomide. Reactive arthritis Clinical features � sometimes younger, sexually lively individual with oro-genital ulcers (painless), conjunctivitis (which could progress to iritis), and rash (soles of feet-keratoderma blenorrhagica). Practice points Marked morning joint pain or stiffness is most likely to be due to inflammatory arthritis. Ankylosing spondylitis Clinical options � Enquire about axial skeleton involvement (lower lumbar back ache, with early morning stiffness, that improves with exercise). Organ involvement varies with the type of vasculitis but generally includes the skin, joints, kidneys, lungs, and the nervous system. Rashes: splinter haemorrhages, nail fold infarcts, purpura, livedo reticularis, nodules. Clinically, one has to determine whether or not their symptoms mirror disease exercise, an underlying infection as a end result of iatrogenic/inherent immunocompromise which can precipitate a flare of the disease, or an unrelated condition. Emergency management � Patients generally die from hypoxia (pulmonary haemorrhage, pulmonary oedema), arrhythmias (due to electrolyte abnormalities), and concomitant an infection. Type 1 monoclonal � kind 1 cryoglobulinaemia, or easy cryoglobulinaemia, is the result of a monoclonal Ig, often IgM or IgG. Type 2 (mixed monoclonal) and type 3 (mixed polyclonal) � sort 2 and sort 3 cryoglobulinaemia (mixed cryoglobulinaemia) contain RhFs (often IgM). Clinical features � � � � � � Renal involvement (haematuria, proteinuria, renal failure). Management � Patients with suspected big cell arteritis must be started on high-dose prednisolone instantly, as delay may result in blindness, and a temporal artery biopsy ought to be organized inside 1 week of beginning steroids, to safe a diagnosis and confidently commit the patient to steroids for 1�2 years. If potentially reversible symptoms persist or worsen, the dose could additionally be i until symptomatic control is achieved. Suggested tapering routine: � proceed with 40�60mg prednisolone until signs and laboratory abnormalities resolve (at least 3�4 weeks); � scale back dose by 10mg every 2 weeks to 20mg; � then scale back by 2. Clinical options � Proximal muscle stiffness and pain with out weakness or losing (see Box 11. Failure to respond should alert the clinician to the potential of an underlying neoplasm or connective tissue disease. L1�L3/4) might have weak thighs and absent knee jerks, and are unlikely to have a disc lesion and may have a tumour. S1 nerve root indicators and signs can be produced by a lesion in the area of the upper lumbar cord (central disc prolapse compressing the S1 nerve root).

Order 25 mg losartan with visa
The appendiceal artery is a department off the ileocolic artery and runs in the mesoappendix diabetic vision losartan 50 mg discount. The ascending colon measures approximately 15 to 20 cm lengthy and runs from the ileocecal valve to the hepatic flexure diabetes type 2 tingling feet 25 mg losartan buy with visa. It ascends as a retroperitoneal structure covered by peritoneum solely on its anterior and lateral surfaces. It lies anterior to the quadratus lumborum, psoas, and transversus abdominis muscular tissues; inferior pole of the best kidney; and descending portion of the duodenum. Lateral to the ascending colon is the white line of Toldt, which represents the fusion of the colonic mesentery with the parietal peritoneum. There may be congenital adhesions between the anterior facet of the ascending colon and the proper abdominal wall (Jackson membrane). The ascending colon and hepatic flexure are equipped by the ileocolic and right colic arteries, and the venous drainage is through the ileocolic and proper colic veins, which drain into the superior mesenteric vein. The lymphatic drainage of the ascending colon is through the paracolic and epicolic lymph nodes, which empty into the superior mesenteric lymph nodes. The transverse colon is the portion of huge bowel that lies between the hepatic and splenic flexures. It is the longest portion of the big bowel and often measures 30 to 60 cm in size. Unlike the ascending and descending colon, the transverse colon has its personal mesentery, which is longest in the center, and is therefore thought of an intraperitoneal structure. The root of the mesentery of the transverse colon covers the descending part of the duodenum, the pancreas, and a portion of the left kidney. At the hepatic and splenic flexures, the mesentery is very brief and should place the transverse colon in contact with the duodenum and the head of the pancreas, which can be injured throughout mobilization of the hepatic flexure. The splenic flexure is linked to the diaphragm by the phrenocolic ligament and to the spleen by the lienocolic ligament. The descending colon is roughly 20 to 25 cm in length; it begins at the splenic flexure and ends on the pelvic brim with the start of the sigmoid colon, which is demarcated by its intraperitoneal mesentery. The proximal part of the descending colon is connected to the peritoneum overlying the left kidney by the phrenicocolic ligament. Lateral to the descending colon is the white line of Toldt, which demarcates the proper plane to enter the retroperitoneal space to mobilize the descending colon. The sigmoid colon begins on the pelvic brim, curves inferiorly along the left pelvic facet wall over the bifurcation of the left common iliac artery, and eventually runs in the midline. The sigmoid mesocolon begins on the pelvic brim and becomes longer to the midpoint of the sigmoid colon and then decreases in dimension as it travels inferiorly. The sigmoid colon becomes the rectum in entrance of the sacrum at the level at which the sigmoid colon mesentery ends and the appendices epiploicae disappear. The taeniae coli become extra diffuse around the rectum and type a whole outer layer of longitudinal muscle. The longitudinal muscles merge with the perineal physique and with muscles of the exterior sphincter. The higher third of the rectum is covered by peritoneum anteriorly and laterally, the center third is roofed only anteriorly, and the decrease third is without peritoneal covering. The peritoneum is tented forward to the upper vagina to type the rectouterine pouch of Douglas. The rectum passes inferiorly via a ligamentous gate formed by the left and proper ligamentum sacrouterinum and travels posterior to the vagina. This surgical plane between the posterior vagina and the rectum is a vital landmark throughout surgical procedures for gynecologic cancer as a outcome of right here the retroperitoneum could be entered under the peritoneal reflection and the perirectal fat and the anterior rectum can be developed in preparation for the resection. Surgical Techniques General Principles of Intestinal Surgery Avoiding tissue trauma, gaining adequate publicity, and utilizing information of anatomy are essential within the performance of any surgical process, and especially with intestinal surgical procedure. Selection of instruments, positioning, suture materials, and stapling strategies are necessary however not as important as the style by which the details are executed. In addition, there are a number of essential rules of profitable intestinal surgery: 1. Chapter 17 Small Bowel and Large Bowel Resection and Anastomosis 235 Maintain an adequate lumen. Consider a diverting ostomy in the setting of an infection, peritonitis, or radiation modifications. Intestinal Anastomosis Techniques of Bowel Anastomosis Intestinal anastomoses can be performed utilizing considered one of two basic strategies: hand-sewn or stapled. Although the introduction of intestinal staplers has simplified and accelerated the creation of a bowel anastomosis, there are occasions when the hand-sewn approach may be indicated or helpful, and the surgeon ought to be familiar with both strategies. Independent of the technique used, there are several basic ideas which are necessary to ensure a profitable anastomosis. Hand-Sewn Anastomoses Hand-sewn anastomosis may be divided into two categories: one-layer and two-layer anastomoses. Variations in method exist, including interrupted versus steady closure, and the selection of absorbable or permanent suture. The small intestine heals very quickly, reaching maximal power in approximately 14 to 21 days. This fee of colonic therapeutic is much like the fast price of healing of the small intestine. The antimesenteric edge is farthest away from the blood supply and is at highest risk for underperfusion. The conventional hand-sewn small bowel anastomosis is carried out by using a one-layer or a two-layer inverting method. The sequence of layer closure depends on the mobility of the portions of gut to be anastomosed. The bowel ends are approximated with bowel clamps and two keep sutures, incorporating the seromuscular layer, positioned halfway between the mesenteric and antimesenteric borders to assist in alignment. The two-layered anastomosis begins with a placement of a single row of imbricating (Lembert) sutures on the posterior wall by way of the seromuscular layer. This is achieved by using a continuous running suture on the posterior mucosal edges and a Connell inverting suture on the anterior mucosal edge. The anastomosis is then completed by putting a row of imbricating (Lembert) sutures on the anterior wall, putting all the sutures before tying them. The one-layer closure has the benefit of decreasing the time required to kind the anastomosis and producing a wider lumen as a result of much less of the bowel edge is inverted. Full-thickness sutures should be placed 5 mm from the edge (out to in), and ideally 1 to 2 mm of mucosa (for hemostasis) ought to be integrated on each ends before exiting 5 mm from the sting on the contralateral facet (in to out). The bowel is turned one hundred eighty levels, and a second mesenteric suture is positioned proper next to the previous one and tied as described earlier; then the suture is run to the antimesenteric facet, where each sutures are tied collectively. The anastomosis is inspected, and interrupted sutures can be placed if necessary to guarantee a watertight anastomosis. Alternatively, a 4-0 double-armed (Monofilament, Vicryl, or silk) suture can be used. The suture is placed on the mesenteric facet (out to in and in to out) in an analogous way as described earlier.
Quality losartan 25 mg
A transverse conduit stoma can be created within the upper quadrant more easily than in the decrease quadrant diabetes symptoms zollinger buy 25 mg losartan fast delivery. As a general rule diabetic quotes losartan 25 mg generic with mastercard, one should try to place the continent diversion stoma in both the right decrease quadrant or the umbilicus. The umbilicus supplies a extra pleasing beauty outcome but does require some preoperative planning, in order that the surgeon is aware of to depart an sufficient quantity of fascia lateral to the umbilical base to enable for a secure fascial closure, as well as to evaluate the periumbilical caliber for hernias that might also complicate its use. A nurse will educate the affected person regarding the forms of home equipment, method and frequency of application, and possible problems. For continent reservoirs, the patient will be educated concerning the proper care and maintenance of the drainage catheter, frequency of catheterization, and frequency of saline flushes of the neobladder. The last is essential because this follow prevents overdistention and perforation of the neobladder by eradicating the mucus that may hinder the outflow. Preoperative Antibiotics Because the danger of surgical website wound infection is roughly 5% to 12% for a clean-contaminated wound, and probably higher amongst high-risk girls with earlier irradiation and poor nutritional status, preoperative use of antibiotics is prudent. Accordingly, intravenous antimicrobial prophylaxis with a second-generation cephalosporin similar to cefoxitin or cefotetan or cefazolin plus metronidazole is warranted. In -lactam�allergic sufferers, the intravenous antibiotics indicated embrace clindamycin plus gentamicin or ciprofloxacin or aztreonam. The antibiotic prophylaxis must be redosed if the surgical time exceeds two halflives of the drug or if blood loss is larger than 1500 mL. The preferred technique of bowel preparation includes neomycin sulfate a thousand mg and erythromycin one thousand mg orally at 1:00 pm, 2:00 pm, and 10:00 pm the day earlier than operation and 8:00 am the day of operation, and begin polyethylene glycol 8 oz each 10 minutes till four L are ingested starting at 6:00 pm the day earlier than surgery. Blood Products the average blood loss throughout an exenterative procedure is about 1000 to 1500 mL, and so preoperative preparation to avoid cardiovascular decompensation is sensible. All sufferers present process exenteration with urinary reconstruction must be typed and cross-matched for at least four to 6 items of packed pink blood cells. Surgical Techniques for Urinary Diversion the choice of urinary diversion is sophisticated and multifactorial. Currently, the surgeon has many more choices at his or her disposal compared with the preliminary description of ureterosigmoidostomy or wet colostomy by Brunschwig (see Table 21. Furthermore, the notion that incontinent conduits are the safer alternative for reconstruction of the urinary bladder in sufferers with recurrent or advanced gynecologic cancers has been evaluated by numerous authors. The subsequent part describes the various urinary diversion techniques, with special emphasis on the Miami pouch or ileocolonic continent urinary reservoir. There remains debate within the gynecologic literature as to which form of conduit is right and has the fewest postoperative complications. They reported no statistically vital difference in rates of conduit-related complications general but did find that sigmoid conduits tended to have an increased fee of intervention and restore. The commonest problems included conduits leaks (ileal, 11%; transverse, 0%; sigmoid, 20%), ureteral anastomotic leak (ileal, 4%; transverse, 0%; sigmoid, 0%), and ureteral stricture (ileal, 3%; transverse, 0%; sigmoid, 0%). In addition, the transverse colon anatomically allows for ease of mobilization because of lack of adhesions, facilitates stomal placement, and permits for larger ureteral anastomosis, particularly with shortened ureteral lengths. The three commonest methods for incontinent urinary diversion including ileal, transverse, and sigmoid conduits are described within the following sections. The left ureter can be tunneled by way of the sigmoid or the descending colon mesentery. The ends of the ureters are trimmed to produce wholesome ends and then spatulated about 0. The small bowel can then be reanastomosed in a side-to-side style through the use of a normal strategy. Mobilization of the intestinal mesentery is minimized to permit a tension-free approximation to the pores and skin for the stoma. Step 4 At the proximal end of the ileal conduit (side reverse to the ostomy end), Metzenbaum scissors are used to create a 5-mm opening on each side of the ileal wall on the antimesenteric finish. The distal end is opened at the staple line to irrigate with betadine and saline till clear to remove all remaining fecal material inside the ileal conduit. Step 5 A 7F or 8F urinary diversion catheter is handed through the ureter over a guidewire into the renal pelvis. The distal end of the stent with the guidewire is then threaded via the opening in the ileal conduit and eventually out the distal or stomal end. Both ureters are sutured through the use of a 4-0 absorbable or delayed absorbable suture incorporating the total thickness of the wall of the ureter and ileum. A variety of stories evaluating direct anastomosis to antireflux anastomosis have proven that the stricture price is highest with the antireflux methodology and not utilizing a significant lower in pyelonephritis, hydronephrosis, or higher stone formation, and so consequently the chapter authors prefer the direct anastomosis or Wallace technique. Reinforcing sutures are positioned on the peritoneal floor of the ureter and the ileum to decrease tension on the anastomosis. Step 6 the distal (stomal) end of the conduit is then introduced through a preselected web site on the abdomen. An approximately 3-cm circular incision is made on the skin and adipose tissue and brought all the way down to the fascia. The stoma is then created with a typical "rosebud" method by putting interrupted 2-0 or 3-0 absorbable sutures via the pores and skin. A portion of the ileal serosa is introduced through about three to 4 cm from the stomal edge and then handed through the total thickness of the stomal wall opening. Step 7 the ileal conduit should be sutured to the peritoneum just below the stomal opening to keep away from peristomal hernia and torsion of the conduit. This catheter, in addition to the ureteral stents, can be secured to the pores and skin with suture. Finally, a big 19F or 21F closed bulb suction drainage catheter is positioned intraperitoneally in the neighborhood of the conduit to allow absorption of any urinary leaks. This section ought to be about 15 cm from the ileocecal valve to enable for ample room for the reanastomosis. If the ileum is found to be compromised, then a phase of jejunum can be utilized to restrict postoperative complications. The length of ileum used depends on the length needed from the ureters to the skin. Step 2 the ureterolysis is performed next to permit a willpower of the length of the conduit, however sparingly to permit just enough Chapter 21 Urinary Diversion in Gynecologic Oncology 291 Step 9 the Foley catheter can be eliminated 2 to 4 weeks postoperatively, and the ureteral stents could be removed 6 to eight weeks postoperatively. Sigmoid and Transverse Conduit Surgical Technique Surgical Steps Step 1 the selection between a transverse or sigmoid conduit will rely upon the ischemic harm from radiation to the sigmoid, the degree of scarring and adhesions, and the size of mesentary needed for stomal placement. The creation of both a transverse colon or sigmoid conduit begins with mobilization of the splenic flexure, which is the idea for a tension-free colostomy. Steps 2 Through 9 Step 2 by way of 9 are the same as for the ileal conduit creation. Of observe, the fascia cruciate incision must be ample due to the dimensions of the colon and to forestall narrowing and ischemia to the colonic section. Continent Urinary Reservoirs Versus Incontinent Diversions Continent urinary diversions include each cutaneous reservoirs and reservoirs which are connected directly to the urethra (orthotopic neobladder). In a continent cutaneous diversion, a bowel phase is related to the pores and skin by a stoma on the stomach wall or umbilicus. In these urinary diversions, the patient should complete periodic self-catheterization to empty the urine.