
Keflex dosages: 750 mg, 500 mg, 250 mg
Keflex packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

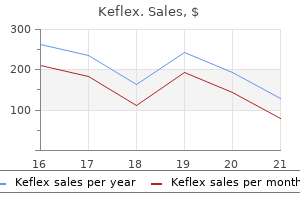
Order keflex 750 mg overnight delivery
Tumors often current within the seventh decade of life infection of the blood discount 750 mg keflex mastercard, with women affected more typically than males (5: 1) antibiotic resistance effects on society keflex 750 mg buy visa. It is essential to notice that there may be severe bleeding at major or metastatic sites which can complicate surgery. Adjuvant radiotherapy, incessantly administered as brachytherapy with a radiation sensitizer may be employed. The total prognosis is poor, with nearly all of patients dying from illness in lower than 6 months. The cut floor is variegated with intensive hemorrhage and necrosis within tumors that are inclined to be giant (up to 12 cm). Freely anastomosing vascular channels are arranged in stable, spindled, papillary, and pseudoglandular patterns. There is plentiful eosinophilic to vacuolated cytoplasm surrounding spherical nuclei with vesicular chromatin and distinguished macronucleoli. The tumors are giant (up to 12 cm), showing a nodular to bosselated outer floor, and vital gentle tissue invasion. Perineural and vascular invasion are regularly current, along with tumor necrosis. The tumors are extremely mobile, organized in bundles or disordered fascicles of spindled cells with centrally positioned, hyperchromatic, blunt-ended, cigar-shaped nuclei. All ages are affected, although patients are normally older at preliminary presentation. Tumors are tan to white and glistening with a "neural" look, typically displaying thyroid gland effacement, cystic change, and necrosis. The tumors arise within the thyroid gland, invading, entrapping, and destroying the parenchyma. The tumors are highly cellular, organized in tightly packed fascicles which are woven right into a obscure herringbone or marbled sample, with solely isolated Antoni B areas. The cells are spindled, with fibrillar cytoplasmic extensions arranged in a loose background. While not coated in this part, it ought to be famous that direct extension into the thyroid from adjoining organs (larynx [squamous cell carcinoma], trachea, esophagus, lymph nodes [lymphoma], soft tissues) could typically must be included in the differential diagnosis of thyroid lots. The thyroid gland is richly vascularized, predisposing to relatively excessive frequency of metastases. In clinical collection, metastatic deposits are identified at a higher frequency in abnormal glands: these with adenomatoid nodules, thyroiditis, and follicular neoplasms. Furthermore, the metastatic deposits may be discovered inside major thyroid tumors. All ages are affected, however metastases are more common in older sufferers (mean, sixty two years), and in females extra typically than males (1. A quickly enlarging thyroid mass will be the presenting signal, although extra typically the underlying thyroid illness could end result within the clinical presentation. Kidney tumors are the most probably to current with an occult major, whereas also having the longest latency interval. Ultrasound can be used to present multifocal disease and bilateral metastases, and to guide biopsy. Close examination of the periphery of the thyroid gland where the vasculature is probably the most dense, will help to determine intravascular metastatic deposits. When the tumor deposits type a mass lesion, they often have an structure and cytomorphology distinct from thyroid primaries. Diffusion artifact and/or entrapment of follicular epithelium inside metastatic tumors should be excluded. The prominent vascularity, glandular lumina full of erythrocytes, lack of colloid, sharp intercellular borders, and small, hyperchromatic nuclei favor a renal cell carcinoma. However, if metastatic disease is restricted to the thyroid, surgery can end result in extended survival, particularly for renal cell carcinoma, a main tumor known for capricious habits. Macro-follicular variant of papillary thyroid carcinoma: a case and control analysis. Follicular variant of papillary thyroid cancer: encapsulated, nonencapsulated, and diffuse: distinct biologic and clinical entities. Familial adenomatous polyposis related thyroid carcinoma: a definite sort of follicular cell neoplasm. Predicting end result in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 sufferers surgically handled at one institution during 1940 via 1989. Papillary thyroid carcinoma managed on the Mayo Clinic throughout six many years (1940-1999): temporal tendencies in initial remedy and longterm outcome in 2444 consecutively treated sufferers. A National Cancer Data Base report on fifty three,856 cases of thyroid carcinoma treated in the U. Prognostic significance of extrathyroid extension of papillary thyroid carcinoma: large but not minimal extension affects the relapse-free survival. Diffuse (or multinodular) follicular variant of papillary thyroid carcinoma: a clinicopathologic and immunohistochemical evaluation of ten instances of an aggressive type of differentiated thyroid carcinoma. Diffuse sclerosing variant of papillary thyroid carcinoma:Major genetic alterations and prognostic implications. Thyroid gland papillary carcinomas with "micropapillary pattern," a recently acknowledged poor prognostic finding: clinicopathologic and survival analysis of seven circumstances. Observer variation within the diagnosis of follicular variant of papillary thyroid carcinoma. Oncocytic papillary carcinoma with lymphoid stroma (Warthin-like tumour) of the thyroid: a distinct entity with beneficial prognosis. Papillary thyroid carcinoma with outstanding hobnail options: a new aggressive variant of reasonably differentiated papillary carcinoma. Thyroid transcription factor1, thyroglobulin, cytokeratin 7, and cytokeratin 20 in thyroid neoplasms. The oncocytic variant of papillary carcinoma of the thyroid: a clinicopathologic examine of 15 cases. Cribriform-morular variant of papillary carcinoma: a distinctive variant representing the sporadic counterpart of familial adenomatous polyposisassociated thyroid carcinoma A clinicopathologic study of 241 instances handled on the University of Florence, Italy. Diffuse sclerosing variant of papillary thyroid carcinoma: clinicopathologic study of 15 circumstances. Systematic evaluation and meta-analysis of the antagonistic results of thyroidectomy combined with central neck dissection as compared with thyroidectomy alone. Diffuse sclerosing variant of papillary thyroid carcinoma�clinical features and consequence.
250 mg keflex buy fast delivery
The tumor cells are plump fusiform cells antibiotic resistance graph purchase keflex 750 mg without prescription, though they are often rounded and epithelioid virus jc discount keflex 750 mg with mastercard. Opacified, dense, eosinophilic cytoplasm gives a touch of squamous differentiation however is difficult to quantify or qualify precisely. When metastatic disease develops (about 20%), cervical lymph nodes and pulmonary involvement is most frequent. There is a worse end result for sufferers with a historical past of radiation, massive tumors, mounted vocal cords, and the presence of epithelial markers immunohistochemically. Surgery, often followed by radiation therapy, seems to yield one of the best long-term affected person outcome. Most tumors show a strongly immunopositive keratin response (A), whereas a unfavorable stain is seen in up to 30% of circumstances (B). As a high-grade lesion, it has a predilection for multifocal presentation and frequent cervical lymph node metastases at presentation. Macroscopically, these tumors are usually agency to exhausting with related central necrosis, occurring as exophytic to nodular lots measuring as much as 6 cm in biggest dimension. Surface ulceration may belie the deeply invasive nature of the tumor, which has frequent lymphovascular invasion, though neurotropism is less frequent. Marked mitotic activity as nicely as comedonecrosis within the center of the neoplastic islands is frequent. The tumor cells are separated by a prominently dense, pink hyaline materials, typically cylindrical or globular, with small cystic areas containing mucoid materials. In metastatic disease, both basaloid and squamous cell parts may be seen, although the basaloid features have predominated. A lack of neuroendocrine nuclear features and immunoreactivity eliminates neuroendocrine carcinoma from consideration. Adenosquamous carcinoma (discussed further on) exhibits a twin composition of true squamous carcinoma and adenocarcinoma. Despite aggressive remedy, the general mortality price is high (60% of sufferers die of their disease). Note the reduplicated basement membrane materials in a linear to globular arrangement. Squamous differentiation is confirmed by pavemented progress with intercellular bridges, keratin pearl formation, dyskeratosis, or particular person cell keratinization. The adenocarcinoma element tends to develop away from the surface (deep), showing tubular, alveolar, and glandular. Both carcinomas might show frequent mitoses, necrosis, and infiltration into the encircling tissue with affiliated perineural invasion. There is usually a sparse inflammatory cell infiltrate on the tumor�stromal interface with minimal to absent desmoplastic fibrosis. Likewise, necrotizing sialometaplasia reveals squamous epithelium lining the scaffolding of preserved duct-gland items that have been infarcted or destroyed. Aggressive surgical procedure with neck dissection and follow-up radiation yields an roughly 15% to 25% 5-year survival. Along with a high lymph node metastatic rate, distant metastases are seen in about 25% of patients (lung most commonly). By definition, this is a heterogeneous group of neoplasms characterised by the presence of epithelial and neuroendocrine differentiation. Systemic manifestations or paraneoplastic syndromes (Cushing, Lambert-Eaton, Schwartz-Bartter) are exceptional. Glandular (with mucin production) or squamous differentiation can be seen in neuroendocrine neoplasms, together with occasional neural-type rosettes. The cells have pale cytoplasm surrounding round nuclei with salt-and-pepper chromatin distribution. The cells can be organized in nests and balls (A), glandular profiles with spherical nuclei and salt-and-pepper chromatin (B), stable sheets of cells with a high nuclear-to-cytoplasmic ratio (C), or fascicles of spindle cells with stippled nuclear chromatin (D). Owing to the fragility of the cells, crush artifact is regularly outstanding in small cell carcinoma. The location of the nucleus is variable (central, eccentric), surrounded by amphophilic to eosinophilic cytoplasm. Crush artifact, mitotic figures, necrosis, and occasional multinucleated neoplastic giant cells are current. Part of the rationale for making a definitive diagnosis relating to neuroendocrine tumors is the distinction in therapy protocols and affected person end result. However, medullary carcinoma of the thyroid may metastasize to or instantly invade into the larynx. Complex intercellular digitation and occasional intercellular junctions are current. Lymphomas, with crush artifact and a submucosal location, can be separated by the dearth of neuroendocrine differentiation (either immunohistochemically or ultrastructurally) and their response with varied lymphoid markers. Death is usually because of metastatic illness, with the dimensions of the tumor an necessary prognostic issue. The proposed etiology for laryngeal chondrosarcomas is disordered ossification of the laryngeal cartilages, specifically the cricoid cartilage (ossification usually develops in areas of muscle insertion and is attributed to the mechanical influence of the contracting muscles). The ossification is found in hyaline cartilages in older grownup sufferers, the height age for presentation of laryngeal chondrosarcoma. Recurrences are common (about 60%), yielding a 50% 5-year survival, with death normally as a end result of metastatic disease (lungs, bone, liver). Interestingly, laryngeal chondromas develop on common about a decade earlier than chondrosarcomas, perhaps suggesting a developmental continuum. By definition, chondrosarcoma is a malignant neoplasm forming neoplastic hyaline cartilage. As the airway is progressively narrowed or obstructed by the endolaryngeal progress, hoarseness, adopted by dyspnea, dysphagia, difficulty respiration, and stridor results. Symptoms are regularly present for a long time (mean, >2 years), supporting the indolent tumor development. After the tumor is identified as "cartilaginous," the remaining features are nonspecific. Most chondrosarcomas appear to involve only a single cartilage with very little tendency to infiltrate adjoining cartilages. There is an total lack of normal architecture and distribution of the chondrocytes ("cluster disarray"). Mitotic figures, including atypical varieties, are solely infrequently famous and solely in high-grade tumors. Tumor necrosis, usually focal and of limited geographic distribution, is usually restricted to highergrade tumors.
Diseases
- Chromosome 3, trisomy 3p25
- Elattoproteus in context of NF
- Ulna metaphyseal dysplasia syndrome
- Nonvenereal endemic syphilis
- Glanzmann thrombasthenia
- Limb dystonia
500 mg keflex amex
A number of components are involved in the development of multinodular goiters; most are associated with some impairment of thyroid hormone production bacterial infection in stomach cheap keflex 750 mg with amex. In iodinedeficient areas of the world antibiotics beer buy keflex 500 mg mastercard, multinodular goiters at one time affected over half of adolescent girls; this was primarily reversed by iodine supplementation. Excess iodine intake, together with iodine-containing medications or different goitrogens, can even induce multinodular goiter by interfering with environment friendly organification of iodine within the production of thyroid hormone. A genetic component can also play a role in the improvement of multinodular goiter. The nodules are usually multiple, but one may be dominant and suggest a solitary nodule. Nodules that attain a big measurement may produce signs due to compression of adjoining constructions (dysphagia, hoarseness, stridor) or trigger cosmetic disfigurement. However, the nodules can be troublesome to distinguish from benign and malignant neoplasms on imaging. As a outcome, there are published guidelines recommending which nodules ought to be biopsied to exclude malignancy. Nodules could reveal hemorrhage in the form of central hematomas or areas of organization, with brown patches representing hemosiderin deposits. Fibrous scars may be seen in some nodules; degenerated nodules are often calcified and may require decalcification prior to histologic processing. Necrosis, if present, is normally central and confluent due to vascular insufficiency. It is always prudent to keep in mind that a multinodular goiter can easily harbor a thyroid neoplasm among its nodules. Therefore tan-white nodules or those with "capsules" ought to be generously sampled, concentrating on the periphery or "capsule of the lesion" to exclude carcinoma. Nodules with a "capsule" must be fastidiously examined histologically to exclude a carcinoma. Sections submitted from the periphery rather than from the center of the nodule are more helpful in yielding a prognosis. The cytologic appearance varies, but the nuclei are sometimes round and hyperchromatic. Hemosiderin-laden macrophages are often seen in the cystic areas and in adjacent parenchyma. A variety of metaplastic modifications could also be seen, together with fatty, squamous, cartilaginous, and osseous metaplasia. They are seen as nodular groupings of variably sized follicles, which stand out among the many regular background follicles. This represents a nodule of thyroid tissue which has become separated from the thyroid gland, often demonstrating either nodular hyperplasia or nodular chronic lymphocytic thyroiditis. The attachment to the thyroid is by an inconspicuous twine of fibrous tissue, usually overlooked intraoperatively. A, Papillary constructions in adenomatoid nodules could also be fairly outstanding and edematous/ bulbous or fantastic and arborizing. C, Hemosiderin-laden macrophages almost completely exchange the colloid in a half of this nodule. This is a common incidence in adenomatoid nodules however very rare in papillary carcinoma. Small fragments of infected thyroid epithelium, detached from the gland, might resemble lymph nodes intraoperatively and histologically. B, Cystic degeneration or hemorrhage ends in the presence of hemosiderin-laden macrophages in plenty of cases (alcohol-fixed, Papanicolaou stain). Because parasitic nodules lack the structures of a lymph node (subcapsular sinus, sinusoids, etc. These are considered to be indeterminate or "suggestive of neoplasm"; surgical elimination of the nodule is usually required in such circumstances. The follicular epithelial cells from the large follicles ruptured by the aspiration course of are normally found as massive flat sheets, with evenly spaced round nuclei in a honeycomb sample. In lesions with degenerative changes, the follicular cells could additionally be somewhat oxyphilic. Once invasion is excluded, the excellence between nodular hyperplasia and a follicular adenoma is of no medical significance and will, actually, be impossible. B, Sheets of follicular epithelium usually have a "honeycomb" appearance due to their polarity and distinct cell borders (alcohol-fixed, Papanicolaou-stained). C, this cellular adenomatoid nodule has scant colloid, excessive cellularity, and oxyphilic change; separation from a neoplasm is commonly unimaginable by fantastic needle aspiration smears alone (alcoholfixed, Papanicolaou stain). The differential analysis of a parasitic nodule and thyroid carcinoma is described in the preceding textual content. Graves illness can be in the differential prognosis when a nodule is hyperfunctioning ("toxic"). Hyperfunctioning nodules could present prominent papillary infoldings and scalloping just like that seen in Graves disease. Hypothyroidism is a danger in any patient handled surgically for multinodular goiter. It has an autosomal recessive inheritance sample and accounts for 15% to 20% of cases of congenital hypothyroidism. It is the second most frequent reason for everlasting congenital hypothyroidism after dysgenesis (abnormal thyroid gland growth and/or migration). However, only sufferers with essentially the most severe impairment in thyroid hormone production present clinically in infancy with cretinism. The common age at presentation is sixteen years, but patients from neonates to adults could also be affected. Approximately two-thirds of sufferers are recognized to have hypothyroidism prior to recognition of the goiter, which tends to develop later in life. The nodules of dyshormonogenetic goiter vary of their look, probably because of the totally different enzyme defects and the duration of the disease (age of patient) at the time of analysis. The commonest finding is the presence of hypercellular nodules with stable or microfollicular patterns. Fibrosis is usually a distinguished finding and could also be so extensive that it distorts the contours of the nodules, suggesting an invasive sample, as seen in follicular carcinoma. B, There is type of no colloid on this low-power view of the thyroid gland, exhibiting a quantity of nodules. B, the nodules may be fairly cellular in dyshormonogenetic goiter, in order to recommend a follicular neoplasm. Diffuse hyperplasia includes clinical hyperthyroidism, usually with lymphoid aggregates and normally has some colloid present. Radiation thyroiditis might demonstrate mobile nodules with cytologic atypia and increased fibrosis inside the gland. An accurate scientific historical past should readily enable the excellence from dyshormonogenetic goiter. The aspirates are remarkably mobile, with little or no colloid and often with prominent nuclear atypia. These findings make exclusion of a follicular neoplasm impossible, even when the historical past of dyshormonogenetic goiter is understood.
Buy cheap keflex 750 mg on line
No clinically significant variations in pharmacokinetics of imipenem antibiotic 875125 buy discount keflex 500 mg on line, cilastatin antibiotic resistance cheap keflex 750 mg without a prescription, and relebactam had been noticed based mostly on age, gender, or race. To guarantee full dissolution, adhere to the following preparation instructions: Step 1. For diluents not available in 100-mL prefilled infusion baggage, withdraw a hundred mL of the specified diluent and switch it to an empty infusion bag, then proceed to Step 2. Withdraw 20 mL (as two 10-mL aliquots) of diluent from the appropriate infusion bag and reconstitute the vial with one 10-mL aliquot of the diluent. After reconstitution, shake vial nicely and transfer ensuing suspension into the remaining 80 mL of the infusion bag. Add the second 10-mL aliquot of infusion diluent to the vial and shake well to ensure full switch of vial contents; repeat transfer of the ensuing suspension to the infusion answer earlier than administering. For sufferers with renal impairment, put together a decreased dose of imipenem, cilastatin, and relebactam by getting ready a 100-mL solution containing 1. Preparation of Reduced Imipenem, Cilastatin, and Relebactam Doses for Intravenous Administration in Patients With Renal Impairment After Preparation as Instructed Above, Remove From the 100-mL Prepared Bag the Volume Indicated Below and Discard 20 mL Resulting Volume That Provides the Indicated Reduced Dose eighty mL 60 mL forty mL Creatinine Clearance (mL/min) 60 to 89 mL/min 30 to fifty nine mL/min Dosage of Imipenem, Cilastatin, and Relebactam 1 Gm (imipenem four hundred mg, cilastatin 400 mg, and relebactam 200 mg) zero. An antibacterial combination product consisting of imipenem (a carbapenem antibacterial drug), cilastatin (a renal dehydropeptidase inhibitor), and relebactam (a diazabicyclooctane beta lactamase inhibitor). When administered alone, imipenem is metabolized within the kidneys by dehydropeptidase. Cilastatin, an inhibitor of this enzyme, effectively prevents renal metabolism of imipenem. Protein binding is roughly 20% for imipenem, 40% for cilastatin, and 22% for relebactam. Approval of these indications relies on restricted medical security and efficacy data. History of known extreme hypersensitivity (severe systemic allergic reaction, similar to anaphylaxis) to any part of imipenem, cilastatin, and relebactam. Check history of earlier hypersensitivity reactions to other carbapenems, penicillins, cephalosporins, different beta lactams, and other allergens. Specific sensitivity research indicated to decide susceptibility of causative organism to imipenem, cilastatin, and relebactam. Cross-resistance with other courses of antibacterial drugs has not been identified; subsequently isolates proof against different carbapenems, together with imipenem, and to cephalosporins may be prone to imipenem, cilastatin, and relebactam. To cut back the event of drug-resistant bacteria and maintain its effectiveness, imipenem, cilastatin, and relebactam must be used to deal with or stop solely those infections proven or strongly suspected to be attributable to micro organism. Anticonvulsant therapy must be continued in patients with identified seizure problems. Concomitant use of imipenem, cilastatin, and relebactam with valproic acid or divalproex sodium could improve the danger of breakthrough seizures; see Drug/Lab Interactions. Consider in sufferers who present with diarrhea throughout or after remedy with imipenem, cilastatin, and relebactam. Monitor CrCl in patients with fluctuating renal operate and modify dosage accordingly; see Dose Adjustments. Patient Education: Review listing of allergies, medications, and medical situations with provider. Avoid concomitant administration except the potential advantages outweigh the risks. Concomitant use of carbapenems, including imipenem/cilastatin (components of imipenem, cilastatin, and relebactam), with valproic acid or divalproex sodium may lower valproic acid concentrations, which may improve the danger of breakthrough seizures. Consider various antibacterials aside from carbapenems to treat infections in patients whose seizures are nicely managed with valproic acid or divalproex sodium. No clinically important differences in the pharmacokinetics of imipenem or relebactam had been observed when imipenem, cilastatin, and relebactam was used concomitantly with probenecid. In vitro research have demonstrated no antagonism between imipenem/relebactam and amikacin, azithromycin, aztreonam, colistin, gentamicin, levofloxacin, linezolid, tigecycline, tobramycin, or vancomycin. No adjustment is needed for sufferers with delicate (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment. No clinically important differences in pharmacokinetics of lefamulin had been observed primarily based on age, gender, race, weight, or renal impairment, together with sufferers receiving hemodialysis. A semi-synthetic systemic pleuromutilin antibacterial that inhibits bacterial protein synthesis through varied interactions with the 50S ribosomal subunit. Lefamulin is bactericidal in vitro in opposition to Streptococcus pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae (including macrolide-resistant strains) and is bacteriostatic towards Staphylococcus aureus and Streptococcus pyogenes at clinically related concentrations. History of identified severe hypersensitivity to lefamulin, pleuromutilin class medication, or to any element of lefamulin. Use with warning in sufferers with renal failure who require dialysis and in sufferers with any degree of hepatic impairment. Specific sensitivity studies indicated to decide susceptibility of causative organism to lefamulin. Some isolates immune to beta-lactams, glycopeptides, macrolides, mupirocin, quinolones, tetracyclines, and trimethoprim-sulfamethoxazole may be vulnerable to lefamulin. To reduce the development of drug-resistant bacteria and keep its effectiveness, lefamulin ought to be used to deal with or prevent solely these infections confirmed or strongly suspected to be attributable to micro organism. Consider in patients who current with diarrhea during or after remedy with lefamulin. Monitor: Monitor patients with hepatic impairment for adverse reactions related to lefamulin. Women of reproductive potential should use effective contraception during treatment and for two days after the final dose. Maternal/Child: Based on animal research, lefamulin may cause fetal hurt when administered to pregnant ladies. In vitro studies have demonstrated no antagonism between lefamulin and amikacin, azithromycin, aztreonam, ceftriaxone, levofloxacin, linezolid, meropenem, penicillin, tigecycline, trimethoprim/sulfamethoxazole, and vancomycin. The most common opposed reactions embrace headache, hepatic enzyme elevation, hypokalemia, injection website reactions, insomnia, and nausea. To scale back the risk of renal toxicity, pa- tients must be nicely hydrated earlier than administration. Use the lowest efficient dose for the shortest duration according to individual affected person therapy goals. Has not been studied in patients with hepatic impairment or in sufferers with reasonable or severe renal impairment. Because meloxicam is an inhibitor of prostaglandin synthesis, its mode of action might outcome from a decrease of prostaglandins in peripheral tissues. To decrease the potential threat, use the bottom efficient dose for the shortest duration potential.
Keflex 500 mg effective
Corticosteroids decrease bone formation treatment for dogs dermatitis keflex 750 mg order with visa, increase bone resorption antibiotic allergy keflex 750 mg buy visa, and reduce protein matrix of the bone. Myopathy is generalized, might contain ocular and respiratory muscles, and may result in quadriparesis. Clinical enchancment following discontinuation of corticosteroids might take weeks to years. Use with warning in sufferers with ocular herpes simplex because of corneal perforation. Report anorexia, diarrhea, dizziness, fatigue, low blood sugar, nausea, weak spot, weight loss, or vomiting; could point out adrenal insufficiency after dose discount or discontinuing therapy. Dose choice should be cautious based on the risk of age-related organ impairment. If possible, anticholinesterase agents must be withdrawn at least 24 hours earlier than initiating corticosteroid remedy. For chronic overdosage in the face of extreme illness requiring steady steroid remedy, the dosage of the corticosteroid could also be reduced only quickly, or alternate day therapy may be introduced. Repeat every 2 hours for two doses, then each three hours for 3 doses; see Dose Adjustments. Consider potential for decreased organ function and concomitant illness or drug remedy. Diluted solutions steady for 24 hours in regular light, 48 hours if protected against mild. Antiemetic properties appear to be the outcomes of antagonism of central and peripheral dopamine receptors. Increases tone and amplitude of gastric contractions, relaxes the decrease pyloric sphincter and duodenal bulb, and increases peristalsis of the duodenum and jejunum, leading to accelerated gastric emptying. May produce sedation, extrapyramidal signs, or Parkinson-like symptoms, much like those seen with phenothiazines. Avoid use for longer than 12 weeks unless profit outweighs threat of tardive dyskinesia. Patient Education: Use caution performing any task that requires alertness, coordination, tions and Drug/Lab Interactions. Treat overdose or extrapyramidal reactions with diphenhydramine (Benadryl) or benztropine (Cogentin). Discontinue remedy in sufferers who develop S/S of tardive dyskinesia; signs could resolve. Well distributed all through the physique, it acts within 1 to 2 minutes and lasts about 3 to four hours. Beta blockade could depress myocardial contractility and precipitate or exacerbate heart failure and cardiogenic shock. Because of its relative beta selectivity, metoprolol may be used with extreme warning in these patients. If metoprolol is required, it ought to be given together with an alpha-blocker. If coronary heart failure or hypotension happens or persists despite applicable remedy, metoprolol ought to be discontinued. Invasive monitoring of central venous, pulmonary capillary wedge, and arterial pressure could also be required. Use digoxin and diuretics at first sign of cardiac failure; dobutamine, isoproterenol, or glucagon could also be required. Anaerobic infections: Begin with an initial loading dose of 15 mg/kg of physique weight (approximately 1 Gm in a 70-kg patient). Infections involving bone and joint, decrease respiratory tract, and endocardium may require longer therapy. Surgical prophylaxis to stop postoperative infection in contaminated or probably contaminated colorectal surgical procedure: 15 mg/kg infused over 30 to 60 minutes and completed 1 hour earlier than surgery. Another source recommends age- and weight-specific doses as follows: Less than 7 days of age weighing less than 1. A bactericidal agent with cytotoxic results, energetic towards particular obligate anaerobic micro organism and protozoa. Does not possess any clinically relevant activity towards facultative anaerobes or obligate aerobes. Is efficient in Bacteroides fragilis infections resistant to clindamycin, chloramphenicol, and penicillin. Hypersensitivity to metronidazole or other nitroimidazole derivatives; use of disulfiram inside the last 2 weeks; use of alcohol or merchandise containing propylene glycol during and for at least three days after remedy with metronidazole. Cerebellar toxicity may manifest as ataxia, dizziness, dysarthria, nystagmus, and saccadic pursuit. Consider in sufferers who present with diarrhea during or after remedy with metronidazole. Patient Education: Avoid alcohol and alcohol-containing preparations during and for no much less than three days after completion of therapy; poisonous reactions will happen. The elimination half-life, measured in the course of the first 3 days of life, was inversely associated to gestational age. Elderly: Pharmacokinetics altered in the elderly; monitor for metronidazole-associated adverse events and adjust dose accordingly. Dose selection ought to be cautious, reflecting the greater frequency of decreased hepatic, renal, or cardiac operate and of concomitant disease or other drug remedy. If concomitant administration is medically necessary, monitor busulfan plasma focus and adjust busulfan dose accordingly. Overdose: Nausea, neurotoxic results (including ataxia, confusion, disorientation, seizures, and peripheral neuropathy), and vomiting. Evaluate danger versus profit of constant remedy in sufferers who develop abnormal neurologic S/S. Discontinue metronidazole in patients with Cockayne syndrome who develop elevated liver function exams. Treatment of candidemia, acute disseminated candidiasis, Candida peritonitis and abscesses: one hundred mg/day as an infusion. Mean period of treatment during medical studies was 15 days (range 10 to 47 days). Mean period of therapy throughout clinical research was 15 days (range 10 to 30 days). Mean duration of remedy in patients who responded successfully during medical studies was 19 days (range 6 to 51 days). For pediatric patients, calculate the dose in milligrams and withdraw the required quantity from the chosen focus (10 mg/mL or 20 mg/mL).
Syndromes
- Canavan Foundation: www.canavanfoundation.org
- You know you are a genetic carrier and are considering having children
- The mucus membrane that covers the wall will be lifted up.
- High-resolution CT scan of the chest
- Hydrogen peroxide
- Nausea and vomiting
- Thinning of eyebrows
- Benign juvenile lordosis (not medically significant)
Keflex 250 mg discount mastercard
Monitor: Obtain baseline plasma carnitine levels before treatment and monitor weekly and then month-to-month based mostly on response (normal range of free carnitine levels is 35 to 60 micromoles/L) virus kingdom keflex 500 mg discount. Certain scientific situations frequent in hemodialysis sufferers similar to malaise antibiotic resistance questions and answers order keflex 750 mg line, muscle weak spot, cardiomyopathy, and cardiac arrhythmias may be related to abnormal carnitine metabolism. Consider dangers of excess carnitine intake to the nursing infant against advantage of levocarnitine supplementation to the mother. Consideration could also be given to discontinuation of breast-feeding or of levocarnitine treatment. The prescribing info lists several other potential adverse occasions without regard to causality. Post-marketing: Hypersensitivity reactions, including anaphylaxis, bronchospasm, and laryngeal edema. An elevated incidence of seizures has been reported in patients with a historical past of seizures. Discontinue levocarnitine if a severe hypersensitivity reaction happens and initiate acceptable medical remedy. Consider risks and advantages of re-administering levocarnitine to particular person patients following a severe response. Single-use vials: Withdraw desired dose from single-use vial (10 mL for 250 mg, 20 mL for 500 mg, 30 mL for 750 mg). When 500-mg (20-mL) vial is used to prepare two 250-mg doses, withdraw whole contents of vial at once using a single-entry procedure. Instructions for entry to and use of premix versatile containers are on its storage carton. Filters: Not required; however, contents of each vials and premixed options had been filtered throughout manufacturing with polyvinyl mixed ester cellulose filters. Store premix at or under 25� C (77� F); shield from freezing, mild, and extreme heat. Solutions diluted from vials are secure at or below 25� C (77� F) for three days and for as much as 14 days if refrigerated. Each 250- or 500-mg dose should be equally distributed over 60 minutes as an infusion. Temporarily discontinue different options infusing on the identical site and flush tubing with compatible options earlier than and after levofloxacin. May be active in opposition to bacteria immune to aminoglycosides, beta-lactam antibiotics, and macrolides. For circumstances during which Pseudomonas aeruginosa is a documented or presumptive organism, combination therapy with an anti-pseudomonal beta-lactam is really helpful. These reactions can happen inside hours to weeks after beginning levofloxacin and have been seen in patients of any age and in patients with none pre-existing risk factors. Discontinue levofloxacin instantly ated with an increased danger of seizures (convulsions), increased intracranial strain (pseudotumor cerebri), tremors, and light-headedness. The majority of deadly hepatotoxicity reports occurred in patients 65 years of age or older; see Patient Education and Antidote. Discontinue levofloxacin immediately if patient experiences ache, swelling, irritation, or rupture of a tendon. Serious opposed occasions, together with a requirement for ventilatory assist and deaths, have been reported in these sufferers. Cases of sensory or sensorimotor axonal polyneuropathy resulting in paresthesias, hypoesthesias, dysesthesias (impairment of sensitivity or touch), or weakness have been reported. Manifestations might embody allergic pneumonitis, arthralgia, myalgia, renal or hepatic impairment/failure, hematologic toxicity, dermatologic toxicity, serum illness, and vasculitis; see Side Effects, Post-Marketing. Immediately discontinue levofloxacin on the first appearance of a skin rash, jaundice, or other signs of hepatotoxicity or hypersensitivity. Consider in sufferers who present with diarrhea throughout or after therapy with levofloxacin. An elevated incidence of musculoskeletal adverse occasions has been observed in pediatric patients. Periodic monitoring of organ methods, including hematopoietic, hepatic, and renal, is really helpful. May trigger anaphylaxis with the first or succeeding doses, even in sufferers with out recognized hypersensitivity. If a hypoglycemia response happens, discontinue levofloxacin and seek the advice of doctor. Maternal/Child: Safety to be used in being pregnant not established; benefits should outweigh risks. Indicated in pediatric sufferers 6 months of age or older only for prevention of inhalation anthrax (postexposure) and prevention and therapy of plague. The risk-benefit assessment signifies that administration of levofloxacin to pediatric sufferers for these indications is appropriate. May erode cartilage of weight-bearing joints or trigger other signs of arthropathy in infants and kids. Abdominal ache, chest ache, crystalluria, cylindruria, dyspepsia, dyspnea, edema, injection web site response, moniliasis, photosensitivity/phototoxicity (sun sensitivity), pruritus, rash, vaginitis, and vomiting have occurred. Levoleucovorin, when substituted for leucovorin calcium, is dosed at one-half the usual dose of the racemic type (leucovorin calcium). Levoleucovorin rescue after high-dose methotrexate remedy: Dose relies on a methotrexate dose of 12 Gm/M2 infused over four hours; see methotrexate monograph. Additional hydration and urinary alkalinization (pH 7 or greater) are indicated and ought to be continued till the methotrexate degree is lower than 0. Twenty-four hours after starting the methotrexate infusion, provoke levoleucovorin rescue at a dose of seven. Administer and/or modify the levoleucovorin dose or extend rescue primarily based on the next guidelines. Guidelines for Levoleucovorin Administration, Adjustment, or Extension of Rescue Clinical Situation Laboratory Findings Serum methotrexate stage approximately 10 micromolar at 24 hours, 1 micromolar at 48 hours, and fewer than 0. Serum methotrexate level of fifty micromolar or more at 24 hours or 5 micromolar or more at forty eight hours after methotrexate administration. Normal methotrexate elimination Delayed late methotrexate elimination Delayed early methotrexate elimination and/or proof of acute renal injury Treatment of folic acid antagonist overdose or impaired methotrexate elimination: 7. The effectiveness of levoleucovorin in diminishing toxicity might decrease as the time interval between methotrexate administration and levoleucovorin rescue increases. This 5-day course is repeated at 4-week intervals for 2 courses after which at 4- to 5-week intervals offered that complete restoration from the toxic results of the previous course has occurred. These abnormalities may or will not be related to vital scientific toxicity. If toxicity is observed, prolong levoleucovorin rescue for a further 24 hours (a total of 14 doses over eighty four hours) in subsequent programs. If lab abnormalities or medical toxicities are noticed, consider the chance that the affected person is taking other medicines that interact with methotrexate. Treatment of folic acid antagonist overdose or impaired methotrexate elimination: Monitor serum creatinine and methotrexate ranges a minimum of each 24 hours. Hydrate with a minimal of 3 liters/day and use sodium bicarbonate for urinary alkalinization (adjust to maintain a urine pH of seven or greater).
Buy keflex 250 mg online
May trigger undesirable cardiopulmonary depression antibiotics yes or no purchase keflex 750 mg amex, including apnea antibiotic powder for wounds keflex 250 mg buy discount on line, airway obstruction, hypotension, and oxygen desaturation. Use warning in sufferers with elevated intracranial stress or impaired cerebral circulation. Major risk factors for the event of these occasions embrace decreased oxygen delivery to tissues; serious neurologic harm and/or sepsis; excessive dosages of one or more of the following pharmacologic agents: vasoconstrictors, steroids, or inotropes; and/or extended, high-dose infusions of propofol (greater than 5 mg/kg/hr for greater than forty eight hours). Has no analgesic properties; provide pain reduction or local anesthetic as indicated. Has been used efficiently with midazolam (Versed), 1 to 3 mg, for preliminary induction. Midazolam offers better amnesia and causes much less ache on injection, whereas propofol sustains sedation and permits more rapid restoration. Abuse of propofol for leisure and different improper functions has resulted in fatalities and different accidents. Intubation tools, controlled ventilation equipment, oxygen, and facilities for resuscitation and life assist have to be obtainable. Adjust if fat is inadequately cleared from physique, and reduce other lipid administration. Dose could also be lowered carefully to enable affected person to awaken to a lighter stage of sedation, permitting neurologic and respiratory evaluation day by day. Avoid speedy awakening; will cause nervousness, agitation, and resistance to mechanical air flow. Monitor urinalysis and urine sediment on alternate days in patients in danger for renal impairment. Discuss with parents or caregivers the risks, advantages, timing, and length of surgery or procedures requiring anesthetic and sedation medication; see Maternal/Child. Not beneficial to be used in obstetric procedures, together with cesarean part; no assurance of safety for fetus. Has been permitted for induction of anesthesia in pediatric sufferers 3 years to 16 years of age. Has been accredited for maintenance of anesthesia in pediatric sufferers 2 months to sixteen years of age. Distribution and clearance in pediatric sufferers three years to 12 years of age is similar to that seen in adults. Published research counsel that repeated or extended exposures to anesthetic agents in utero (third trimester) and early in life (up to three years of age) could have adverse effects on the growing brain, resulting in opposed cognitive or behavioral effects; see prescribing data for additional discussion. A current examine identified a rise in deaths with propofol versus normal sedative brokers. Elderly: Dose necessities decrease after age fifty five because of lowered clearance and volume distribution and higher blood ranges. Minimize undesirable cardiorespiratory depression (hypotension, apnea, airway obstruction, and/or oxygen desaturation) through the use of reduced doses and rates of administration. Anesthetic and sedative results increased; systolic, diastolic, mean arterial pressure, and cardiac output are decreased. No important adverse interactions famous to date with neuromuscular blocking agents. Competition for chemoreceptor binding websites may occur if utilized in mixture with droperidol; use of propofol as a single agent is typically recommended to control nausea and vomiting. In pediatric sufferers, severe bradycardia could outcome with concomitant administration of fentanyl. Apnea; bradycardia (profound); cough; dyspnea; headache; hypotension; hypoventilation; injection web site burning, pain, stinging; nausea; and upper airway obstruction are most common. Pediatric patients: Increased incidences of agitation, bradycardia, and jitteriness have occurred; apnea has been observed frequently. Abrupt discontinuation following extended infusion might result in agitation, flushing of the palms and toes, hyperirritability, and tremulousness. Overdose: Cardiorespiratory depression (hypotension, apnea, airway obstruction, and/or oxygen desaturation). Discontinue the drug for main side effects, paradoxical reactions, or unintentional overdose. A short-acting drug, a patent airway, and steady controlled ventilation with oxygen until normal function assured must be sufficient. Do not give further propranolol if desired change in fee or rhythm is achieved. Best results achieved if administered within 2 to 4 hours of symptom onset or thrombolytic therapy. Reduce dose gradually to keep away from rebound angina, myocardial infarction, or ventricular arrhythmias. Pediatric price: Extend rate of administration of a single dose by injection to a minimum of 5 minutes in pediatric patients. Propranolol is a nonselective beta-adrenergic blocker with antiarrhythmic effects. Decreases the pressure of cardiac contractility, and decreases arterial strain and cardiac output. Well distributed all through the physique, the onset of motion happens inside 1 to 2 minutes and lasts about 4 hours. Short-term treatment to lower ventricular rate in supraventricular tachycardia, together with Wolff-Parkinson-White syndrome and thyrotoxicosis. Use in sufferers with atrial flutter or atrial fibrillation must be reserved for arrhythmias unresponsive to normal remedy or when extra extended control is required. Control of ventricular rate in life-threatening, digoxin-induced arrhythmias (severe bradycardia could occur). Treatment of tachyarrhythmias due to excessive catecholamine action throughout anesthesia when different measures fail. Not the drug of first choice for treatment of ventricular arrhythmias until arrhythmia is induced by catecholamines or digoxin. Has been used for adjunctive remedy of pheochromocytoma following primary treatment with an alpha-adrenergic blocking agent. Cardiogenic shock, sinus bradycardia, greater than first-degree heart block, bronchial bronchial asthma, known hypersensitivity to propranolol. Use with extreme caution in asthmatics or in sufferers with lung disease or bronchospasm; can block bronchodilation produced by endogenous and exogenous catecholamine stimulation of beta receptors. Use with caution in sufferers with diabetes or in sufferers with a history of hypoglycemia. Abrupt withdrawal of propranolol could additionally be adopted by exacerbation of symptoms, including thyroid storm. Discontinue the drug when a rhythm change is noted and wait to note full impact before giving further treatment if indicated.
Cheap keflex 750 mg otc
Recommended starting dose of treprostinil is 10% of the current epoprostenol dose treatment for dogs kidney failure 500 mg keflex buy visa. The treprostinil dose is then increased gradually as the epoprostenol dose is decreased based on constant ob servation of response infection game strategy keflex 750 mg purchase fast delivery. Interruptions for longer periods could require the dose of treprostinil to be retitrated. The desired length of an infusion between changeovers is up to 48 hours, and reservoirs usually have volumes of fifty or 100 mL. Step 1: Calculate the required focus of treprostinil with the following formulation. Diluted solu tions are stable at ambient temperatures when stored for as a lot as 14 days utilizing highpH glycine diluent at concentrations as low as zero. It directly vasodilates pulmonary and systemic arterial vascular beds and inhibits platelet aggregation. Right and left ventricle afterload is reduced, and cardiac output and stroke quantity are in creased. Has a doserelated unfavorable inotropic (contracting) and lusitropic (relaxing) ef fect on the guts. Primarily excreted in urine with a small amount as unchanged drug and a larger amount as metabolites. Initiation of treprostinil should happen in a setting with enough diagnostic and therapy services to monitor the patient and reply to any medical emergency. In patients with low systemic arterial stress, remedy with treprostinil might cause symptomatic hypotension. Monitor: the ambulatory infusion pump must be small and light-weight; have occlusion/ no supply, low battery, programming error, and motor malfunction alarms; have deliv ery accuracy of 66% or higher of the hourly dose; and be positivepressure driven. Patient and/or caregiver should assume re sponsibility for drug reconstitution, drug administration, and care of the permanent central venous catheter. Consider increased potential for impaired organ perform and concomitant disease or drug therapy. Oral bosentan (Tracleer) and sildenafil (Revatio, Viagra) have been used concurrently with oral treprostinil; no pharmacokinetic interactions were noticed. Overdose: Blurred imaginative and prescient; confusion; diarrhea; dizziness; flushing, together with a sense of warmth and redness of the face, neck, arms, and upper chest; headache; hypotension; lightheadedness when getting up from a lying or sitting position; nausea and vomiting; sudden sweating; or uncommon tiredness or weak point could also be signs of overdose. Most might be treated with dose discount; some may require symptomatic deal with ment. Baseline studies indicated; see Precautions and response is usually achieved with doses lower than 60 mg/kg/24 hr. Complex partial seizures (monotherapy [initial]): Begin with an initial dose of 10 to 15 mg/kg/24 hr. Complex partial seizures (conversion to monotherapy): Begin with an initial dose of 10 to 15 mg/kg/24 hr. May be elevated by 5 to 10 mg/kg/week till desired scientific response achieved or until side effects are dose limiting. Complex partial seizures (adjunctive therapy): Begin with an initial dose of 10 to 15 mg/kg/24 hr. Has been used in mixture with either carbamazepine (Tegretol) or phenytoin (Dilantin). Simple and sophisticated absence seizures: Begin with an initial dose of 15 mg/kg/24 hr. May be elevated by 5 to 10 mg/kg/week until seizures are controlled or unwanted effects are dose limiting. Manufacturer has beneficial that a fee of 20 mg/min not be exceeded; however, outcomes of a single research recommend that selected patients tolerated charges from 1. Peak impact occurs on the finish of a 60-minute infusion or four hours after an oral dose. The halflife will be within the lower part of the vary in patients receiving other enzyme-inducing antiepileptic brokers. Patients with a historical past of hepatic illness, sufferers taking multiple anticonvulsants, pediatric sufferers, patients with congenital metabolic disorders, sufferers with extreme seizure problems accompanied by cognitive impairment, and patients with natural brain disease may be at specific risk. If valproate is used in pediatric patients under 2 years of age with or without these increased risk elements, benefits should outweigh dangers; use only as a sole agent and with excessive warning. Incidence of deadly hepatotoxicity decreases in progressively older affected person groups. Some of the circumstances have been described as hemorrhagic with speedy progression from initial signs to demise. Hyperammonemic encephalopathy must be considered in patients who current with lethargy and vomiting or altered psychological status. Hyperammonemia should also be thought of in patients who current with hypothermia (unintentional drop in body temperature to less than 35� C [95� F]). Can also occur in sufferers using concomitant topiramate with valproate after beginning topiramate remedy or after rising the dose of topiramate. The benefit of improved therapeutic impact with greater doses should be weighed towards the possibility of a larger incidence of opposed reactions. Initial S/S include fever, rash, and/or lymphadenopathy related to different organ system involvement. Total plasma concentrations could additionally be regular, but free concentrations could additionally be considerably elevated in these patients. Thrombocytopenia, inhibition of the secondary section of platelet aggregation, and abnormal coagulation parameters. Closely monitor throughout remedy for the event of acute liver damage with common scientific assessments and serum liver testing. One contributing factor is the nonlinear, concentration-dependent protein binding of valproate, which affects the clearance of the drug. If valproate sodium is given two or three times every day, close monitoring of trough plasma levels may be needed to guarantee therapeutic levels are being maintained. Elevations of ammonia may also be asymptomatic; monitor plasma ammonia levels carefully; see Antidote. Patient Education: May cause drowsiness; determine effects before driving or working any machinery. In utero publicity to valproate may end in listening to impairment or hearing loss. The elevated teratogenic danger from valproate in ladies with epilepsy is anticipated to be mirrored in an elevated danger in different indications. Tests to detect neural tube and other defects must be thought of as a part of routine prenatal care in pregnant girls receiving valproate. If clotting parameters are abnormal within the mother, then these parameters also wants to be monitored in the neonate; see Monitor. Monitor the breast-fed infant for indicators of liver injury, together with jaundice and weird bruising or bleeding. Initial dose should be decrease, and dosage Maternal/Child: Valproate can cause fetal hurt when administered to a pregnant girl.
Order keflex 750 mg otc
Do not use in hypotension from blood loss unless an emergency antibiotic 8 weeks pregnant 750 mg keflex free shipping, in mesenteric or peripheral vascular thrombosis virus 1999 movie order keflex 500 mg without prescription, or with cyclopropane or halothane (inhalant) anesthesia. In an emergency, norepinephrine could be efficient in a hypovolemic state before fluid substitute has been completed. Maternal/Child: Category C: use provided that clearly needed; benefits should outweigh risks. Phentolamine causes instant and conspicuous local hyperemic changes if the area is infiltrated inside 12 hours. Should a sudden or uncontrolled hypertensive state occur, discontinue levarterenol, notify the physician, and if essential, deal with with an adrenergic blocking agent. To stop or attenuate extreme hypersensitivity reactions, premedicate in accordance with the next chart earlier than the indicated infusion. Obinutuzumab: Doses have to be administered as an infusion through a dedicated line according to the following two charts. If no infusion response occurred through the previous infusion, administer at 50 mg/hr. The price of the infusion could be increased in increments of 50 mg/hr each half-hour to a most price of 400 mg/hr. If an infusion response occurred in the course of the earlier infusion, administer at 25 mg/hr. If no infusion response occurred during the previous infusion and the final infusion price was one hundred mg/hr or quicker, infusions could be started at a fee of 100 mg/hr and increased by 100-mg/hr increments each 30 minutes to a most of 400 mg/hr. If an infusion reaction occurred during the earlier infusion, administer at 50 mg/hr. If no infusion reaction or an infusion response of Grade 1 occurred through the previous infusion and the ultimate infusion fee was one hundred mg/hr or sooner, infusions can be began at a price of a hundred mg/hr and increased by 100-mg/hr increments each half-hour to a maximum of 400 mg/hr. If an infusion reaction of Grade 2 or larger occurred in the course of the earlier infusion, administer at 50 mg/hr. Patients who obtain steady disease, full response, or partial response to the preliminary 6 cycles should continue obinutuzumab as monotherapy for two years. During obinutuzumab and chemotherapy treatment, adjust the dosing schedule accordingly to maintain the time interval between chemotherapy cycles. Monotherapy should be initiated approximately 2 months after the final dose of obinutuzumab administered during the induction phase. Storage: Refrigerate single-use vials at 2� to 8� C (36� to 46� F) in carton to shield from mild. Grade 1-2 (mild to moderate): Reduce or interrupt infusion and treat as indicated. If no further reactions occur, fee may escalate as indicated for every treatment-cycle dose. With decision of symptoms, consider restarting the infusion at not more than half the speed that brought on the response. Grade 4 (life-threatening): Stop infusion instantly and discontinue remedy completely. Elimination occurs by a linear clearance pathway and a time-dependent nonlinear clearance pathway. Patients with a historical past of recurring or continual infections may be at increased danger for infection. May be delayed (occurring more than 28 days after completion of therapy and/or extended [lasting longer than 28 days]). However, hypersensitivity reactions not often occur with the first infusion and, when observed, typically occur after a previous publicity. S/S of quick reactions could embrace bronchospasm, dyspnea, hypotension, tachycardia, and urticaria. S/S of late-onset reactions (serum-sickness) embrace chest pain, diffuse arthralgia, and fever. S/S could include fast discount in tumor volume, renal insufficiency, hyperkalemia, hypocalcemia, hyperuricemia, or hyperphosphatemia. Correct electrolyte abnormalities and provide supportive care, including dialysis, as indicated. Patients with severe and long-lasting (greater than 1 week) neutropenia are strongly beneficial to obtain antimicrobial prophylaxis till resolution of neutropenia to Grade 1 or 2. In sufferers with Grade three or Grade four thrombocytopenia, monitor platelet count extra regularly till decision and consider subsequent dose delays of obinutuzumab and chemotherapy or dose reductions of chemotherapy; see Antidote. Elderly: In clinical trials, the incidence of great antagonistic events was greater in older patients. Consider withholding antihypertensive drugs for 12 hours earlier than and all through each infusion and for the first hour after administration. May constitute a medical emergency or shall be handled symptomatically as indicated. Interrupt or cut back fee of infusion for Grade 1 or 2 infusion reactions and handle symptoms. Permanently discontinue remedy for any Grade 4 infusion response together with, however not restricted to , anaphylaxis. If a hypersensitivity response is suspected during or after an infusion, the infusion have to be stopped and remedy completely discontinued. Resumption of therapy must be mentioned with physicians with experience in managing hepatitis B. Consider remedy interruption within the occasion of an infection, Grade 3 or 4 cytopenia, or a hematologic toxicity equal to or greater than Grade 2. Dose delays of obinutuzumab and chemotherapy or dose reductions of chemotherapy may be indicated. Obiltoxaximab: A single dose of sixteen mg/kg administered as an infusion over ninety minutes. A clear to opalescent, colorless to pale yellow to pale brownish-yellow resolution that may contain a couple of translucent-to white proteinaceous particulates. Syringe: Using an appropriately sized syringe for the entire quantity of infusion to be ad- calculated quantity in mL of obiltoxaximab. Transfer the required volume (dose) of obiltoxaximab to the chosen infusion bag. Do not See the following chart for recommended dose, complete infusion quantity, and infusion fee by body weight. Steady-state quantity of distribution is larger than plasma volume, suggesting some tissue distribution. Limitations of use: Should be used just for prophylaxis when its profit for prevention of inhalational anthrax outweighs the chance of hypersensitivity and anaphylaxis. Dosing in pediatric patients was derived utilizing a inhabitants pharmacokinetics method designed to match the observed adult publicity to obiltoxaximab at a 16 mg/kg dose. Patient Education: Effectiveness has been studied only in animals with inhalational anthrax. Maternal/Child: No data on the utilization of obiltoxaximab in pregnant ladies to inform on drug-associated risk. Maternal infection with anthrax is related to a excessive danger of maternal, fetal, and neonatal deaths, notably within the absence of treatment.
250 mg keflex purchase
A pure penicillin antibiotics for uti uti keflex 250 mg on-line, bactericidal in opposition to penicillin-sensitive microorganisms during the stage of active multiplication antibiotics hurting stomach keflex 250 mg generic mastercard. Serious infections attributable to penicillin G�sensitive gram-positive, gram-negative, and anaerobic microorganisms. Premixed options containing dextrose may be contraindicated in sufferers with a recognized allergy to corn or corn products. Hypersensitivity reactions, including fatalities, have been reported in patients undergoing penicillin remedy; most probably to happen in sufferers with a history of penicillin hypersensitivity or sensitivity to multiple allergens. Sensitivity studies necessary to determine susceptibility of the causative organism to penicillin. To scale back the event of drug-resistant micro organism and preserve its effectiveness, penicillin should be used to treat or stop solely those infections confirmed or strongly suspected to be brought on by bacteria. To reduce the danger of rheumatic fever, sufferers being handled for Group A beta-hemolytic streptococcal infections ought to be handled for a minimum of 10 days. Consider in patients who present with diarrhea during or after therapy with penicillin. Doses over 10,000,000 units might cause deadly hyperkalemia, particularly in patients with renal insufficiency. Monitor: Periodic analysis of renal, hepatic, and hematopoietic systems is really helpful in prolonged remedy. Probenecid decreases elimination of penicillin, leading to prolonged halflife and increased serum ranges. May lower effectiveness of oral contraceptives; breakthrough bleeding or pregnancy might result. Higher-than-normal doses might cause neurologic opposed effects including convulsions, particularly with impaired renal function. For all unwanted aspect effects, discontinue the drug, deal with hypersensitivity reactions or resuscitate as essential, and notify the doctor. Treatment of Pneumocystis jiroveci: four mg/kg of body weight once every day for 14 days. Leishmania, cutaneous (unlabeled): 2 to 4 mg/kg once or twice a week till lesions heal. One supply recommends 4 mg/kg every 24 hours with a CrCl of 10 to 50 mL/min or four mg/kg every 24 to 36 hours with a CrCl lower than 10 mL/min. A single dose have to be further diluted in 50 to 250 mL of D5W and given as an infusion. Individually titrate to a dose that provides sufficient analgesia and minimizes antagonistic reactions. Manufacturer states, "Do not mix in the same syringe with soluble barbiturates. Pentazocine is a partial agonist at the mu opioid receptor and an agonist on the kappa opioid receptor. Use as a preoperative preanesthetic medicine and as a complement to surgical anesthesia. Limitations of use: Because of the risk for dependancy, abuse, and misuse, even at really helpful doses, reserve pentazocine to be used in sufferers for whom alternative therapy options. Acute or severe bronchial bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment. Overestimating the pentazocine dose when converting patients from one other opioid product can end result in a deadly overdose with the first dose. Use warning in elderly, cachectic, or debilitated sufferers; respiratory despair is extra likely to happen. Cases of serotonin syndrome have been reported during concomitant use of pentazocine with serotonergic drugs. If adrenal insufficiency is diagnosed, treat with physiologic replacement doses of corticosteroids, and wean the patient off the opioid to allow adrenal function to recuperate. Another opioid could additionally be tried because some instances reported use of a special opioid with out recurrence of adrenal insufficiency. May cause severe hypotension, together with orthostatic hypotension and syncope, in ambulatory sufferers. Use warning in sufferers with head harm, brain tumors, or elevated intracranial stress. May enhance the frequency of seizures in sufferers with a convulsive dysfunction and will induce or worsen seizures in some medical settings. Some formulations comprise sulfites; use warning in sufferers with allergic reactions; see Contraindications. May increase systemic and pulmonary arterial pressure and systemic vascular resistance. May be predisposed to an elevated incidence of adverse reactions Mild narcotic antagonist. Monitor: Naloxone (Narcan), oxygen, and controlled respiratory gear should all the time be out there. Monitor for respiratory depression, especially during initiation of therapy (within the primary 24 to 72 hours) or after a dose improve. Keep affected person supine to reduce side effects; orthostatic hypotension and fainting might happen. Monitor sufferers with a history of seizure issues for worsening seizure management. If stage of ache increases after dosage stabilization, try and identify the supply of increased pain before growing the pentazocine dose. Monitor sufferers frequently for the event of opioid dependancy, abuse, and misuse. Maternal/Child: Use during being pregnant (other than labor and delivery) provided that advantages justify risks to the fetus. Closely monitor neonates exposed to pentazocine throughout labor and supply for signs of extreme sedation and respiratory melancholy. Prolonged use of pentazocine during being pregnant can end result in neonatal opioid withdrawal syndrome, which can be life threatening if not acknowledged and handled. Infants born to mothers receiving pentazo cine throughout being pregnant should be monitored intently and handled for neonatal opioid withdrawal syn drome, if indicated. Monitor infants exposed to pentazocine by way of breast milk for extra sedation and respiratory despair. Withdrawal signs can happen in breast-fed infants when maternal administration of an opioid analgesic is stopped or when breast-feeding is stopped. Information on the safety of pentazocine as a postoperative analgesic in pediatric sufferers under sixteen years of age is proscribed. Consider age-related organ impairment; monitoring of renal function may be indicated.