
Flomax dosages: 0.4 mg, 0.2 mg
Flomax packs: 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps
Buy flomax 0.2 mg online
Child Adol"Sc<nt Adult Infant Full time period neonae: Integum entary Developm ent 0 ~ a prostate cancer nih 0.4 mg flomax purchase with mastercard. Developmental modifications in physiologic elements that influence drug disposition in infants prostate cancer family history discount flomax 0.4 mg otc, kids, and adolescents. Panel B illustrates developmental variations in body composition that may influence the apparent volume of distribution for medication. Panel E illustrates the impression of development on aspects of the integumentary system that collectively can modulate the systemic absorption of medication utilized to the pores and skin. Developmental pharmacology-drug disposition, action and remedy in infants and youngsters. An example of therapeutic utility of pharmacokinetic-based optimization of drug therapy has been just lately illustrated in the provision of antiretroviral therapy in children (6). In the next paragraphs, we offer a summary of developmental pharmacokinetics, a lot of which has been excerpted (with permission) from current works (1,7,8) printed by one of many coauthors (G. These publications could be referred to for reference to citations within the main literature upon which the following summaries are based mostly. Given that the majority orally administered medicine have the physicochemical property of being either a weak acid or weak base, pH within the gastrointestinal tract can influence the quantity of doubtless absorbable drug. In the fully mature neonate, the gastric pH ranges from 6 to 8 at delivery and drops to 2 to three inside a few hours of start. However, after the first 24 hours of postnatal life, the gastric pH will increase due to the immaturity of the parietal cells and gradually reaches expected adult values. As a result of these developmental differences, the bioavailability of acid-labile drugs. Drug Absorption Absorption of medication administered by extravascular routes occurs largely through passive diffusion. During early infancy, gastric emptying time is extended, which can delay supply of orally administered drugs to the small gut where the vast majority of absorption takes place. Lastly, immature biliary operate in neonates and young infants within the first few months of life has the potential for lowering the extent of oral bioavailability of lipophilic medication which would possibly be dependent upon bile acids for their solubility within the small gut. In the neonate, muscular blood move is decreased in the first few days of life, as is the relative effectivity of muscular contractions. Furthermore, neonates and younger infants have greatly decreased muscle mass (compared to older infants and children) and elevated percentage of water per unit of muscle mass. In contrast, mucosal (rectal and buccal) and dermal permeability within the neonate and young infant is increased and thus could end in enhanced absorption by these routes. In addition, the ratio of body floor area to physique weight is larger in infants and kids as compared to adults. Normal developmental variations in drug absorption from virtually all extravascular routes of administration can influence the dose-plasma concentration relationship in a fashion enough to alter pharmacodynamics. Finally, with regard to extravascular drug administration, it must be acknowledged that the onset of drug effect is directly dependent upon the route of administration. For example, the onset of impact for most medication given intravenously is, generally, just about instantaneous. This is contrasted with medication given by inhalation (onset - 2 to three minutes), sublingual administration (onset - 3 to 5 minutes), intramuscular injection (onset - 10 to 20 minutes), subcutaneous injection (onset - 15 to 30 minutes), rectal (onset - 30 minutes), oral (onset - 30 to ninety minutes), and trans dermal (onset - minutes to hours) routes. Drug Distribution Drug distribution is influenced by quite so much of factors together with drug-specific physicochemical properties, tissue composition. To a fantastic diploma, adjustments in drug distribution during development are related to adjustments in body composition and the amount of plasma proteins able to drug binding. The discount in relative complete physique water occurs rapidly in the course of the first yr of life, and by 12 years, grownup values. Of the circulating proteins in plasma, albumin (which preferentially binds weak acids) and aj-acid glycoprotein (which preferentially binds weak bases) are quantitatively the most important for drug binding. A comparable sample of maturation is noticed with aj-acid glycoprotein where neonatal plasma concentrations are roughly thrice lower than in maternal plasma and attain adult values by approximately 1 year of age. Binding affinity for acidic medicine can additionally be lowered within the neonate as a consequence of the higher concentrations of fetal albumin (which has a lower binding capacity) and endogenous substances. Drug Metabolism Metabolism displays the biotransformation of an endogenous or exogenous molecule by a quantity of enzymes to moieties that usually are extra polar (hydrophilic) and thereby, more easily eliminated by way of excretion, secretion, and/or exhalation. While in many circumstances, drug metabolism results in pharmacologic inactivation of a drug, there are situations where it could possibly either contribute to or be a determinant of drug motion. The former scenario is illustrated by medicine that have pharmacologically energetic metabolites. Quantitatively, an important organ liable for drug biotransformation is the liver, However, drug-metabolizing enzymes. Drug metabolism has traditionally been conceptualized as occurring through two common lessons of enzymatic processes: Phase I, or nonsynthetic reactions. Finally, the importance of genetic polymorphism on pharmacodynamics is nicely illustrated by the,B-adrenergic receptor blockers where variant alleles of the,B-receptor are associated with both an improved response to remedy or, alternatively, an elevated chance of antagonistic events which are dependent upon a selected genotype. In addition to their significance in removing drugs from the physique, you will need to acknowledge that both drug-metabolizing enzymes and transporters that exist predominantly in the small gut and each their polymorphic and ontogenic expression can alter absolutely the bioavailability of medicine. Given that the activity of most drug-metabolizing enzymes is markedly reduced in the neonate, the extent of bioavailability of medicine that are substrates for drug-metabolizing enzymes. Pre systemic clearance (also described as first-pass effect) would improve because the functional capacity of these proteins will increase, with the potential for lowering the bioavailability of medicine given by the oral route. Unfortunately, only a few bioavailability studies are performed in infants and children; thus, assumptions regarding the impact of ontogeny on presystemic drug clearance must be made primarily based on the known developmental profiles and pharmacogenomics for the drug-metabolizing enzymes and transporters concerned (20). However, the exercise of those oxidizing enzyme methods is reduced, which ends up in sluggish clearance (and extended elimination) of many medicine. The influence of ontogeny on the activity of human drugmetabolizing enzymes has been the subject of a number of reviews (11-13). As illustrated by knowledge for human glucuronosyltransferases (14), the influence of ontogeny on drug-metabolizing enzyme exercise may be isoform specific. Many drug-metabolizing enzymes represent the merchandise of genes that in some situations, are polymorphically expressed, with the variant alleles usually conveying reduced and/or absent exercise. Similarly, polymorphic expression of genes answerable for regulation of particular drug transporter proteins also exists. Together with drug-metabolizing enzymes, their actions are often the rate-limiting event for metabolic clearance of a drug from the body and, in some cases, for drug motion. Pharmacogenetics: level and medical relevance for specific examples are additional metabolizer. The activity of all drug-metabolizing enzymes is generally larger earlier than versus after puberty. From a developmental perspective, renal function is very dependent on gestational age and postnatal diversifications. Developmental modifications that occur in renal perform are better characterised than some other organ system (Table 79.
0.4 mg flomax buy with visa
Our follow has been to carry out ambulatory Holter monitoring annually at a minimum with extra frequent evaluation or different methods such as occasion recorders in patients with signs or issues for ongoing arrhythmia prostate cancer 100 psi 0.4 mg flomax visa. The use of immunosuppressive and immunomodulatory brokers in suspected instances or proven circumstances of viral myocarditis stays controversial man health sa flomax 0.2 mg buy with amex. The Myocarditis Treatment Trial analyzed the use of immunosuppressive and steroid therapy (52). Although the research was performed in grownup sufferers, the results are potentially relevant to kids. There was no difference among patients treated with azathioprine and prednisone, cyclosporine and prednisone, and conventional therapy. Immunosuppressive remedy was not useful in most sufferers with histologically confirmed myocarditis. However, there could additionally be chosen populations with persistent myocarditis that profit from immunosuppression. The prognosis of acute myocarditis in newborns has been poor over time (157-159). The six infants who survived had no obvious sequelae, although long-term follow-up was not reported. It is most likely going that other viral causes of myocarditis such as adenovirus have similar poor outcomes as infants. Older infants and kids have a greater prognosis, with a mortality price between 10% and 25% in clinically recognizable cases. Twenty-five % of the sufferers continued to have an irregular electrocardiogram or chest radiograph even though they were clinically asymptomatic. Abnormalities in the resting electrocardiogram is probably not seen, but could additionally be introduced out with train. Adult patients who recover may be asymptomatic at rest or with gentle exertion however may demonstrate a decreased working capability with train stress testing. With the development of newer and miniaturized units, various options at the moment are obtainable for each short- and long-term help (162). Of these, 75% survived with seven recovering ventricular function with system elimination and 5 went on to uncomplicated cardiac transplant. Their use will improve in the pediatric inhabitants given the increasing availability of units and the potential need for sustained support in select sufferers. Furthermore, these units allow time for myocardial recovery and favorable transforming of key proteins that may be broken in viral myocarditis (165). Respiratory syncytial an infection in a toddler difficult by interstitial myocarditis with deadly outcome. Pancarditis affecting the conducting system and all valves in human African trypanosomiasis. Myocarditis and pericarditis with tamponade related to disseminated tuberculosis. Myocarditis in combined connective tissue illness: medical and pathologic study of three circumstances and evaluate of the literature. A scientific and histopathologic comparison of cardiac sarcoidosis and idiopathic big cell myocarditis. Persistence of ventricular arrhythmia after decision of occult myocarditis in kids and younger adults. Myocardial deformation in acute myocarditis with normal left ventricular wall motion-a cardiac magnetic resonance and 2-dimensional pressure echocardiographic examine. Management and outcomes in pediatric patients presenting with acute fulminant myocarditis. Long-term follow-up of biopsy-proven viral myocarditis: predictors of mortaliry and incomplete restoration. Clinicopathological features of paediatric deaths due to myocarditis: an autopsy collection. Association of parvovirus B19 genome in kids with myocarditis and cardiac allograft rejection: analysis using the polymerase chain reaction. Viral epidemiologic shift in inflammatory coronary heart disease: the growing involvement of parvovirus B19 within the myocardium of pediatric cardiac transplant sufferers. High prevalence of cardiac parvovirus B19 an infection in sufferers with isolated left ventricular diastolic dysfunction. Long-term outcome of sufferers with biopsy-proved myocarditis: comparability with idiopathic dilated cardiomyopathy. Evaluation of postmortem endomyocardial biopsy specimens from 38 sufferers with lymphocytic myocarditis: implications for position of sampling error. Incidence and prevalence of neutralizing antibodies to the widespread adenoviruses in youngsters with cystic fibrosis: implication for gene remedy with adenovirus vectors. Viral endomyocardial an infection is an impartial predictor and doubtlessly treatable danger issue for graft loss and coronary vasculopathy in pediatric cardiac transplant recipients. Viral myocarditis: a paradigm for understanding the pathogenesis and treatment of dilated cardiomyopathy. The development of interstitial myocarditis to idiopathic endocardial fibroelastosis. Characterization of effector cells and demonstration cytotoxicity in opposition to viral-infected myofibersl. Molecular and immune mechanisms within the pathogenesis of cardiomyopathy-role of viruses, cytokines, and nitric oxide. Coxsackievirus-induced myocarditis depends on distinct immunopathogenic responses in numerous strains of mice. Autoantibodies in sera of sufferers with myocarditis: characterization of the corresponding proteins by isoelectric focusing and N-terminal sequence analysis. A mouse mannequin for mitochondrial myopathy and cardiomyopathy resulting from a deficiency within the heart/muscle isoform of the adenine nucleotide trans locator. Novel organ-specific circulating cardiac autoantibodies in dilated cardiomyopathy. Circulating cardiac-specific autoantibodies as markers of autoimmunity in scientific and biopsy-proven myocarditis. Cardiac-specific overexpression of tumor necrosis factoralpha causes deadly myocarditis in transgenic mice. Therapeutic impact of anti-tumor necrosis factor-alpha antibody on the murine mannequin of viral myocarditis induced by encephalomyocarditis virus. Interleukin-2 suppressed myocarditis within the acute stage however enhanced the situation in the subsequent stage. Long-term outcome of fulminant myocarditis as in contrast with acute (nonfulminant) myocarditis. Adenoviruses and enteroviruses as pathogens in myocarditis and dilated cardiomyopathy. Myocarditis and inflammatory cardiomyopathy: microbiological and molecular biological features. Active Coxsackieviral B an infection is related to disruption of dystrophin in endomyocardial tissue of patients who died all of a sudden of acute myocardial infarction.
Flomax 0.4 mg cheap line
Canadian Cardiovascular Society 2009 Consensus Conference on the administration of adults with congenital heart disease: outflow tract obstruction prostate cancer x-ray images quality flomax 0.2 mg, coarctation of the 1507 109 prostate foods to avoid cheap flomax 0.4 mg with visa. Recurrence rates of arrhythmias during pregnancy in ladies with previous tachyarrhyrhmia and impact on fetal and neonatal outcomes. Choosing the most effective contraceptive technique for the grownup with congenital heart illness. Prevention of infective endocarditis: guidelines from the American Heart Association: a tenet from the American Heart Association Rheumatic Fever, Endocarditis, and Kawa- saki Disease Committee, Council on Cardiovascular Disease within the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Awareness of each cardiovascular disease and the chance of sudden cardiac dying has elevated both in media and in national education programs. In reality, >50% of adolescents with a historical past of chest ache report important concern of cardiac pathology (5). The imply age of kids and adolescents who complain of chest ache is eleven to 14 years, however chest pain can happen in kids as younger as 4 years of age (1,6). Chest pain is equally common in women and men, though sure etiologies could have a sex-specific predilection. The most typical source of chest pain in youngsters and adolescents is the musculoskeletal structures of the chest wall (1,2,4-9). It is necessary to apply adequate stress during this palpation, as gentle touch could not reproduce the ache. Treatment consists of reassurance and relaxation from athletic or strenuous actions, and sometimes could require the use of nonsteroidal antiinflammatory medications, at least in the acute phase. Tietze Syndrome Tietze syndrome entails the irritation of a single costochondral junction (12). While this syndrome has been reported in kids and even infants, it stays comparatively uncommon in childhood (12). The affected joint will be swollen and tender to palpation, and could also be heat to the touch. The ache is often self-limited, lasting wherever from a few weeks to a couple of months. Idiopathic Chest-Wall Pain Nonspecific (idiopathic) chest-wall pain is the most common sort of chest pain in children and adolescents (Table 70. Children with idiopathic chest pain are inclined to have longer programs than kids with other etiologies and should have intermittent chest pain for many months (16,14). The ache usually entails two to 4 contiguous costochondral or costosternal junctions, between the second and fifth costal cartilages (1,10). The pain is mostly unilateral and will affect the left facet extra frequently than the proper. The patient will complain of a sharp ache lasting from several seconds to several minutes, which is exacerbated by deep breathing. The pain sometimes is positioned below the left breast or at the lower left sternal border (15,16). The ache may be so sharp that the patient will breathe shallowly for several seconds. When it occurs throughout train, the patient may should stop and breathe shallowly till the pain subsides. Treatment sometimes is unnecessary and ineffective, due to the random nature of the ache (15). Surgical resection of the particular cartilages can be performed but must be reserved only for severe instances (17,18). Hypersensitive Xiphoid Syndrome Hypersensitive xiphoid syndrome is a rare type of chest pain in youngsters (20). In these patients, light digital stress on the xiphoid course of will reproduce the pain. Trauma and Muscle Strain Chest pain typically may be brought on by traumatic damage to the chest wall, particularly in athletes. The history of prior trauma is suggestive, and sometimes the ache is reproducible with palpation of the affected area of the chest. The ache usually is worsened with positioning or activities involving the specific muscle and bony tissues (13). For easy muscle strains, nonsteroidal anti-inflammatory medicines are typically effective. The examiner have to be conscious that vital trauma can produce a myocardial contusion and possibly a hemopericardium (see Chapter 23), both of which might trigger chest ache. Significant trauma requires full analysis for potential bony and visceral accidents. This can lead to rib laxity, pressure on intercostal nerves, and a "popping" sensation (19). Subsequently, any type of exercise that causes these tissues to move (coughing, athletics, stretching) will produce or worsen the attribute intense aching ache (17). The attribute exam finding in slipping-rib syndrome is the "hooking maneuver. This action will reproduce the ache and should produce a clicking or popping sound (17). Pulmonary Asthma and exercise-induced asthma are well-known causes of chest pain in youngsters and adolescents. Laboratory evidence of asthma has been detected in up to 73% of youngsters evaluated for chest pain, though that is probably an overrepresentation (21). Chest ache in sufferers with asthma more than likely is secondary to cough, chestwall muscle strain, or dyspnea/hyperinflation (19). Exertional bronchial asthma can be handled with inhaled bronchodilators prior to initiation of actions. Additionally, pleural effusions or localized empyemas could produce localized chest ache. In addition to pneumonia/pneumonitis, infection of the massive airways could cause chest pain, including bronchitis and tracheitis. These sufferers typically present with other concurrent typical symptoms to help make clear the analysis. Finally, the doctor should ask of any attainable ingestion history, because the presence of a international body within the airway could produce dyspnea and chest ache. The ache is attributable to an intercostal neuralgia and may present earlier than the looks of the characteristic skin eruption. The pain sometimes resolves with healing of the skin lesions; nevertheless, postherpetic neuralgia could persist and be quite painful. Sickle Cell Disease Patients with sickle cell disease can develop a vase-occlusive disaster that includes chest ache ("acute chest syndrome") and an infiltrate on chest radiography. A patient suspected to have acute chest syndrome should be evaluated emergently (23).
Buy flomax 0.4 mg fast delivery
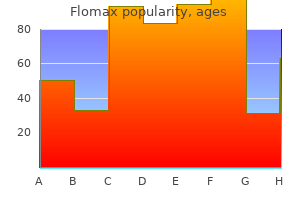
Cumulative frequency distribution of patient age at the time of planned-executed repairs based on androgen hormone migraine 0.2 mg flomax generic visa the kind of repair from a 20-institution cooperative protocol study (Congenital Heart Surgeons Society prostate 2 flomax 0.4 mg discount visa, 1985, 1986). No deaths occurred before repair of sufferers assigned to an arterial swap protocol (median age at surgery, 6 days), whereas 5% of sufferers assigned an atrial change protocol died earlier than repair. However, most significantly, the "reassuring" peripheral oxygen saturation may be associated with paradoxically low oxygen supply, significantly to the brain. Measurements of cerebral venous oxygen saturation have been invasively sampled throughout cardiac catheterization in children who have been both cyanotic and acyanotic (49-51), and noninvasively in children with right-to-left shunt lesions. Consistent with these observations, there are evolving knowledge demonstrating increased central nervous system injury-particularly to the white matter-if an arterial change operation is delayed even by days, particularly if accompanied by hypoxemia (45). In addition, recent follow-up neurodevelopmental consequence research in infancy and beyond counsel that earlier elimination of hypoxemia might contribute to improved motor outcomes and mind development in certain subgroups of sufferers (52). With this approach up to now 2 to 3 years, preliminary information suggest a significant discount in the incidence of preoperatively recognized white matter injury compared with historical controls, but additional work is necessary to confirm these preliminary knowledge and rule out confounding factors all the time inherent when utilizing historical controls. Excluding poor technical efficiency, a number of anatomic and physiologic elements may be liable for unsatisfactory improvement. In common, adequately palliated neonates have an interatrial defect at least 5 to 6 mm in diameter ensuing from the septostomy maneuver. Nevertheless, despite the presence of adequately sized anatomic communications, insufficient circulatory mixing and disappointing scientific improvement have been famous in some infants. It has been postulated that in such instances, a delayed decrease in the pulmonary vascular resistance, with consequent low pulmonary blood circulate and left atrial volumes and pressures, at times might result in inadequate interatrial mixing (see additionally section on "Fetal and Perinatal Physiology"). An interatrial septal defect is created by excising the posterior side of the interatrial septum in a comparatively easy closed heart process that may be performed quickly on even the smallest toddler. Although early within the expertise operative, mortality rates approached 30%, later collection reported mortality risks <3% to 5%. Palliative Blalock-Hanlon or atrial septectomy procedures are rarely performed within the present era as a result of the development toward earlier atrial and neonatal arterial repairs. Partial Venous Return Repair (Baffes) Historically, within the Nineteen Fifties, a partial physiologic repair was proposed and achieved by connecting the inferior vena cava to the left atrium with a homograft or artificial conduit and concurrently detaching the best pulmonary veins and instantly transferring them to the right atrium. This palliative operation then results in an obligate, effective shunt on the atrial stage. Subsequently, a few of these sufferers had a modified Mustard sort of atrial restore to achieve complete physiologic correction. Surgical constriction of the pulmonary artery can present efficient palliation for each these complications in infants and, until the arterial repair era, was generally carried out in early infancy. Operative mortality for banding in the newborn interval traditionally must be within the range of 5% or less. In the atrial change period, the selection between the Senning and Mustard operations was controversial. Proponents of the Senning repair advanced that the operation was simpler to carry out, used minimal (if any) prosthetic materials or nonviable tissue, had less compromised atrial volumes and compliances, and was followed with a decrease frequency of systemic venous obstruction and "late" dysrhythmia. Others demonstrated that modifications to the Mustard process resulted in lowered early mortality, reduced systemic and pulmonary venous obstructions, and less dysrhythmia. Superiority of either surgical approach outdoors of particular person experience has not been convincingly established. Statistics are restricted but presently operative mortality with a Gore-Tex interposition shunt may be as low as 5%. Results and Sequelae of Physiologic Correction Using cardiopulmonary bypass with profound hypothermia (with or without circulatory arrest), these operations have been routinely utilized to neonates and infants typically with a remarkably low early operative mortality by way of the early Nineteen Nineties (56). Combined information more broadly representative of present outcomes recommend 10-year survival rates of 85% to 90% (56,57). A literature evaluate (9) involved with 234 patients operated on largely in the 1970 decade indicated a mean early mortality of 23 %; other reported hospital mortality charges ranged from 10% to 60%, and long-term survival rates stay disappointing, with 5-year survival estimates about 60% to 70%. The issues encountered with this subgroup most likely replicate the increased coexistence of adverse morphologic (associated anomalies) and physiologic (pulmonary hypertension and vascular disease) elements. Persistent and regularly progressive practical cardiac abnormalities have lengthy been acknowledged following physiologic repair and include (a) residual intra-atrial shunts, (b) caval and pulmonary venous obstructions, (c) right ventricular dysfunction, (d) tricuspid valve insufficiency, and (e) arrhythmia. More latest series of both the Mustard or Senning repairs report a significantly lowered incidence of baffle leaks or venous obstruction, however proper ventricular dysfunction to some extent and dysrhythmias in particular stay important late concerns. Residual intra-atrial baffle shunts occur mostly on the superior right atrial-baffle suture line, might cause either systemic-to-pulmonary or pulmonary-to-systemic venous shunting, and are readily detected by colour Doppler echocardiography. Although trivialleaks have been observed at late postoperative angiography in 10% to 20% of patients, significant leaks requiring reoperation have been unusual (1 % to 2%). Systemic and pulmonary venous pathway obstructions are doubtlessly serious complications. The neonate has been considered at larger risk for both kinds of venous obstruction due to the restricted anatomic spaces concerned. The causes of obstruction that have been implicated embrace (a) improper baffle geometry and suture line placement, (b) contraction of the pericardial or synthetic material baffle, and (c) scar tissue or adhesions involving the baffle and excised margins of the atrial septum. Superior vena caval pathway obstruction appears postoperatively in about 5% to 10% of sufferers with a Mustard sort restore. Severe obstruction might current early after surgery with clinical signs of higher extremity plethora or chylothorax, and long-standing obstruction might lead to hydrocephalus. Even anatomically extreme obstruction could stay asymptomatic, nevertheless, because of decompression of the superior vena cava by the azygous or hemiazygos system. Because obstruction can be present without signs or signs, a extra appropriate frequency (about 17%, in Mustard collection; about 14%, in Senning series) could also be mirrored by considering solely sufferers who had late postoperative catheterization examination. The usual location of the obstruction is distal to the superior vena caval entrance, throughout the systemic venous atrium at the site of excision of the superior remnant of the atrial septum. In addition to surgical revision, balloon catheter dilation, stent placement, and an innominate vein to left (physiologic right) atrial appendage shunt all have been used successfully to achieve temporary relief for both acute and continual superior vena cava obstruction. Inferior vena caval obstruction is a severe but infrequent (about 1%) complication of atrial change restore. Operation is carried out using cardiopulmonary bypass with chilly cardioplegic myocardial protection or during profound hypothermia with whole circulatory arrest. A: A proper atriotomy is made in front of and parallel to the caval veins and extended into the atrial appendage. The atrial septum is now incised anteriorly, superiorly, and inferiorly to kind a septal flap (shaded area) as large as potential, which stays mounted posteriorly between the caval entrances. B: the systemic venous chamber and conduit to the mitral valve is fashioned posteriorly by the repositioned septal flap (shaded area), and the conduit then is completed anteriorly by suturing the posterior right atrial free wall flap (z z z) anteriorly to the anterior septal limbus (z z z) as in (C). A left atriotomy is made as lengthy as attainable within the inner atrial groove (exposing the orifices of the right pulmonary veins). C,D: the pulmonary venous chamber and pathway to the tricuspid valve are completed with the suturing of the anterior right free wall atrial flap (asterisk) over the right pulmonary veins to the anterior lip of the left atriotomy (asterisk). D: Black arrows indicate systemic venous caval flow via the newly created atrial tissue conduit and systemic venous chamber (cross-hatched area) towards the mitral valve. Pulmonary venous obstruction, which can be evident immediately after surgery or turn out to be distinguished a few weeks or months later, is a less frequent but extra lethal sort of obstruction than the systemic venous type. A low frequency (about 2 %) of pulmonary venous obstruction has been reported for both the Mustard and Senning forms of atrial restore in two collection representing the original surgical growth groups. Prompt suspicion ought to be aroused by a postoperative chest roentgenogram with pulmonary venous congestion or unexplained arterial desaturation in the postoperative period.
Flomax 0.2 mg without a prescription
Furthermore man health trend flomax 0.2 mg buy cheap line, cardiopulmonary bypass is accompanied by risks of gaseous and particulate embolism dr lam prostate oncology specialists purchase 0.2 mg flomax, macroemboli, and hypoperfusion leading to diffuse ischemia/reperfusion harm (53). Additional mechanisms of hypothermic protection of the mind and different organs throughout ischemia embrace preservation of intracellular shops of high-energy phosphates and of excessive intracellular pH, in addition to safety towards reperfusion injury together with the no-reflew phenomenon, calcium influx, and free radical injury (57). Circulatory arrest has been broadly used because the Nineteen Sixties in centers with expertise in infant open-heart surgery. When evaluated as a continuous variable, longer period of complete circulatory arrest has been related to elevated risk of seizures, choreoathetosis, release of mind isoenzymes, and developmental delay (21,62-71), though in some studies, period of circulatory arrest has not been a big predictor of outcome (60,73). The relationship of duration of circulatory arrest to various developmental outcomes was nonlinear. In addition to period of whole circulation arrest (74), these embody the depth of hypothermia (75), the rate and period of core cooling (76), acid-base management throughout core cooling (77,78), and the degree of hemodilution (79). At the profoundly low temperatures (l5�C to 18�C) used throughout toddler and neonatal cardiac surgical procedure, hypothermia will increase the viscosity of blood and purple Outcomes after Heart Surgery in Children 1581 blood cell aggregation (82), doubtlessly increasing the chance of microvascular occlusion. Hemodilution has been used to counter these dangers (83) and has been shown to improve cerebral blood move (84), but could reduce the oxygen-carrying capacity of blood. Furthermore, as a end result of hypothermia induces a leftward shift of oxyhemoglobin dissociation, hemodilution has the potential to limit oxygen delivery to the central nervous system (83). A subsequent trial confirmed no variations in neurodevelopmental outcome at 1 year with hemodilution within the vary of 25% to 35% (85). For instance, the reduced oxygen-carrying capability of a low hematocrit throughout cardiopulmonary bypass could be compensated for by means of the pH stat technique, or by growing circulate rate, reducing period of circulatory arrest, or decreasing temperature. Preoperative Factors and Host Susceptibility Host susceptibility is prone to have an result on the response of the central nervous system to cardiopulmonary bypass and perioperative events (88). Preoperative affected person characteristics similar to low Apgar scores at 5 minutes, younger gestational age, lower delivery weight, and other attributes have been impartial threat factors for antagonistic neurodevelopmental consequence in scientific trials (79,89). Furthermore, response to cardiac surgery may be mediated by genetic polymorphisms in the pathways affected by exposure to cardiopulmonary bypass, together with irritation, thrombosis, vascular reactivity, and oxidative stress (90). The influence of genetic polymorphisms on postoperative morbidity has been extensively studied amongst adults undergoing open coronary heart surgery (91-94). For instance, among adults, worse postoperative bleeding is extra common among these with polymorphisms in genes coding for coagulation proteins and platelet glycoproteins (95), and postoperative thrombotic complications have been associated with gene polymorphisms in fibrinogen and angiotensin-converting enzyme (96). Low cardiac output syndrome is widespread in the first 24 to 48 hours following restore of advanced congenital heart illness (104,105). Hemodynamic instability and low cardiac output syndrome may be especially damaging to the weak central nervous system of the neonate who has just undergone cardiac surgical procedure using deep hypothermic cardiopulmonary bypass strategies. Hypoxic-ischemic insult associated to hypothermic cardiopulmonary bypass methods disrupts the integrity of cerebral vasoregulatory techniques in the early postoperative period, and autoregulation of cerebral blood circulate is impaired (106-109). General measures of postoperative course complexity even have been associated with later neurodevelopmental consequence. The adverse impact of longer hospitalization on neurodevelopmental consequence reflects multiple contributory components that delay restoration. The hormonal milieu after cardiac surgery may affect the central nervous system. For example, sick euthyroid syndrome is common among infants and kids following open heart surgical procedure, and the diploma of thyroid suppression seems to be biggest after probably the most complicated operations (110-119). In cohort studies, preterm infants with transiently low thyroid levels within the first weeks of life have been found to have later abnormalities of neurologic and developmental operate, including higher risks of cerebral palsy (120) and learning disabilities (121). Furthermore, transient hypothyroxinemia of prematurity has been famous to be an independent danger issue for cerebral white matter damage (120,122). The causes of thyroid hormone suppression after cardiopulmonary bypass, probably multifactorial, might embrace hypothermia, hemodilution, and use of medicines ~e. The affiliation of longer hospital length of stay and worse neurodevelopmental consequence may also be mediated by the inflammatory response. [newline]Inflammation can precipitate autoregulatory disturbance and microvascular ischemia and cause neonatal cerebral white matter injury (127,128). Circulating pro inflammatory cytokines and chemokines, induced by the huge inflammatory effects of cardiopulmonary bypass and subsequently by postoperative occasions, could be related to late brain structural and useful abnormalities. Cardiac catheterization in kids has been associated with neurologic complications at a reported incidence of 0. In addition, distinction toxicity could also be a cause of seizures after cardiac catheterization (130). Catheter interventions could increase the related danger of cerebrovascular harm for some affected person teams. Although procedures corresponding to open coronary heart surgical procedure or cardiac catheterization are mostly associated with embolic stroke in youngsters with congenital coronary heart disease, embolic strokes can also occur from intracardiac thrombi that type within the setting of arrhythmia. Patients with venous hypertension and polycythemia are at elevated risk for cerebral venous thrombosis. Risk of cerebrovascular accidents may also improve within the setting of relative anemia in sufferers with cyanotic coronary heart illness and elevated blood viscosity (135). Infections within the heart or brain could cause neurologic morbidity amongst children with congenital heart disease. Most frequent amongst these is the prevalence of infective endocarditis, with its danger of septic or nonseptic emboli and of mycotic aneurysms (136, 137, 142). Even within the current period, congenital coronary heart disease is the commonest predisposing explanation for brain abscess (138). Brain abscess is very frequent in people with cyanotic coronary heart disease, with the incidence inversely associated to oxygen saturation (139-144). Many require special companies because of their higher frequencies of learning disabilities and of speech, language, and behavioral abnormalities (4,seventy two,145-150). Visual-spatial expertise are an area of relative weak spot amongst youngsters with congenital heart disease (148-151). On a measure of practical independence 1 to 3 years after surgery, Limperopoulos et al. Furthermore, longer period of significant cyanosis is related to a greater decline in cognitive ability (154-160). In common, outcomes after repair of easy lesions, similar to atrial septal defects, are similar to those in the regular population, whereas developmental outcomes appear to be worse after biventricular restore of extra complicated lesions (5,146,159,160-163), although the particular causative elements and the position of cardiopulmonary bypass remain unclear (160). Adverse developmental consequence is most typical among those with numerous types of single ventricle (72,one hundred forty five,166). Outcomes after Heart Surgery in Children 1583 Outcomes in Diagnostic Groups Congenital heart illness contains uncommon and diverse problems, and most studies of growth in youngsters with congenital heart disease include sufferers with heterogeneous lesions. However, children in a few diagnostic groups have been studied in larger detail, and these are briefly reviewed. Risk factors for antagonistic outcomes included establishment, longer circulatory arrest time, postoperative seizures, and use of a restore aside from the arterial switch operation (172). Personality evaluation revealed reduced scores on adaptability and management scales, as well as higher scores on hurt avoidance.
Discount flomax 0.2 mg visa
Using such standards prostate 5lx hair loss buy flomax 0.4 mg with mastercard, a report from the Framington examine demonstrated an incidence of two androgen hormone and hair loss flomax 0.4 mg order amex. A: this parasternal long-axis view demonstrates the 2-D options of mitral valve prolapse, with part of the anterior leaflet being behind the high level of the mitral annulus (black arrow). B: this 3-D picture of mitral valve prolapse was taken utilizing transesophageal echocardiography. The prolapsing segments of the valve may be seen, with the best hand panel displaying the sites of regurgitation. In this setting, myxomatous valves present disorganization in their collagen content and elastin fibers (54-56). Their chordae present a rise in glycosaminoglycans, particularly, chondroitin derma tan 6 sulphate and hyaluronan, which have the ability to bind extra water, ensuing within the gelatinous look of the leaflets and their supporting chordae. In the pediatric population, transthoracic 3-D echocardiography is often sufficient; however, as sufferers move into their teenage and younger grownup years, transesophageal echocardiography is superior. Importantly, it permits a precise identification of the component(s) which are prolapsing, in addition to the relationship to the location and degree of regurgitation. In other circumstances, if the four-chamber view is insufficient, a full-volume knowledge set can be acquired from the parasternal long-axis view; nonetheless, this pictures the leaflets in a lateral plane, which supplies decrease picture decision. Physical findings of M5 embody a middiastolic murmur and a late diastolic murmur during atrial systole. These murmurs are low pitched and higher appreciated with the bell rather than the diaphragm of the stethoscope. Mitral regurgitation leads to a high-pitched pansystolic 51-coincident murmur that will make it difficult to appreciate the primary and second heart sounds. Hepatomegaly and increased work of breathing are different physical findings that may be present in children with both M5 or regurgitation. Clicks could additionally be followed by a high-pitched late systolic murmur of mitral regurgitation, heard finest on the left decrease sternal border or apex. For instance, standing ends in decreased left ventricular preload, leading to prolapse that happens earlier in systole with a click(s) which are close to fifty one. However, squatting will increase preload and delays the prolapse, ensuing in the click on shifting nearer to 52. Oximetry may present delicate desaturation within the setting of pulmonary edema or may indicate the presence of a left-to-right shunt. Hemodynamic evaluation may present pulmonary hypertension, elevated pulmonary capillary wedge pressures, and left atrial hypertension with elevated "A" waves. One exception is with supra-annular prosthetic stenosis, the place the "V" wave is bigger than the "A" wave and the left ventricular end-diastolic pressure is commonly elevated (65). Angiography is related to important risk in patients with pulmonary hypertension and must be averted until balloon valvuloplasty is planned. Findings will include elevated left ventricular end diastolic pressure, elevated left atrial strain with massive "V" waves, and elevated pulmonary capillary wedge stress. However, chest radiography is affordable previous to surgical or catheter interventions. However, hemodynamic evaluation may be valuable in kids with mitral illness related to other lesions. Qs might clarify the relative contribution Balloon versus Surgical Management McElhinney et al. Balloon dilation resulted in a decrease in peak and mean transmitral gradients by a median of 33% and 38%, respectively. Approximately, three-fourths of subjects had the prosthesis placed in the supra-annular position. Surgery could additionally be in the form of chordal fenestration when fusion is an issue, resection of sub annular accent tissue, or splitting of a solitary papillary muscle. Recent retrospective cohorts revealed by large centers show that surgical intervention ends in a 60% to 70% discount in transmitral Doppler gradients and may be achieved with in-hospital mortality of 10% or much less (68,69). However, reasonable or extreme mitral insufficiency remains a postoperative problem. One of the problems with surgical intervention in the infant is that failure to relieve the stenosis is related to increased morbidity and fewer than ideal options. If acknowledged in the neonatal interval, a Norwood/ Hybrid method can be undertaken, thus abandoning the left aspect of the guts. Also, cardiac transplantation is more more probably to result in success prior to developing sustained adjustments in the pulmonary vascular mattress. However, supra-annular placement impairs left atrial compliance and results in pulmonary hypertension, even in the absence of great prosthetic obstruction (65). The limited lifespan of prostheses, particularly bioprostheses, requiring repeated reinterventions later in life (71,72), is an extra disadvantage. Finally, operative mortality, while improving, remains a significant issue, notably in younger children (71,73). Supraannular placement was associated with a decreased chance of needing subsequent pacemaker placement, however within the latter half of the cohort (1991 to 2006) it was associated with worse survival (74). Prostheses which would possibly be too large may contribute to left ventricular outflow tract obstruction, impaired prosthetic valve mobility, and conduction system injury. The use of tissue prostheses in youngsters is proscribed by lack of availability of small sizes, limiting their use in young children, and in addition by extra fast degeneration compared to mechanical prostheses resulting in a very excessive fee of reoperation (78). Pregnancy seems protected with a tissue bioprosthesis and the low price of valve-related complications and good practical class of this patient population is such that bioprosthesis stays an excellent option in some sufferers. Homografts have not often been used in the mitral position and are associated with a higher reoperation threat when compared to other bioprostheses. Among those with an initial mean mitral gradient of <2 mm Hg, none had an intervention or died, whereas among those with an initial mean mitral gradient of >5. Restriction from competitive sports activities is prudent for those with moderate or extreme left ventricular enlargement and people with aortic root dilation. Fortunately, these are very rare in children but could occasionally be noticed in adolescents. Medical administration contains optimizing caloric intake and weight acquire, monitoring for the potential improvement of pulmonary hypertension and atrial arrhythmias, aggressive management of respiratory infections, influenza vaccinations, and prophylaxis against respiratory syncytial virus infection with palivizumab for children <2 years of age. Freedom from reintervention was 80% at 10 years, and survival was approximately 95% at 15 years and roughly 85% at 20 years. These excellent results reveal the feasibility of a conservative surgical method. The relationship of mitral annular form to the prognosis of mitral valve prolapse. A examine of useful anatomy of aortic-mitral valve coupling using 3D matrix trans esophageal echocardiography. Geometric changes of mitral annulus assessed by real-time 3-dimensional echocardiography: changing into enlarged and fewer nonplanar within the anteroposterior course throughout systole in proportion to world left ventricular systolic perform. Restricted diastolic opening of the mitral leaflets in patients with left ventricular dysfunction: proof for elevated valve tethering. Two-dimensional versus transthoracic real-time three-dimensional echocardiography within the evaluation of the mechanisms and sites of atrioventricular valve regurgitation in a congenital heart illness inhabitants. Left ventricular function after resection of the papillary muscle tissue in sufferers with whole mitral valve replacement.
0.2 mg flomax fast delivery
It is essential to do not overlook that these infants are hemodynamically fragile prostate gland enlargement order 0.2 mg flomax amex, tachycardic primary androgen hormone discount 0.2 mg flomax overnight delivery, and infrequently receiving prostaglandin or palliated with a systemic-to-pulmonary artery shunt to increase pulmonary blood move. Therefore, retrograde coronary blood move from the hypertensive proper ventricle occurring during systole and mediated by the ventriculocoronary connections could also be essential to maintain sufficient myocardial perfusion. The administration corollary to this is clear: interference with blood move into the best ventricle or reduction of right ventricular systolic strain in situations by which the coronary circulation is true ventricular dependent may lead to myocardial ischemia, infarction, and demise. It is much more likely to observe ventriculocoronary communications in sufferers whose ventricles have been categorized as unipartite or bipartite. In 9% of the 145 sufferers, the coronary circulation was thought-about wholly right ventricular dependent. Ventriculocoronary connections might involute after profitable right ventncular decompression (whether by pulmonary valvotomy or tricuspid valve excision or avulsion). Such coronary arterial obstructive lesions can occur in fetal tissues, and these lesions have been recognized clinically by each angiography and histopathology in hearts from patients who die in the first few hours and days after delivery. Obviously, some changes could also be acquired late, however clearly obstructive coronary arterial lesions may be recognized within the immediate newborn. In the uncommon patient in whom the interatrial communication is actually restrictive, the cardiac output may be affected as well by proscribing the obligatory right-to-Ieft shunt. A pansystolic murmur often is audible at the left decrease sternal border, according to tricuspid regurgitation. In infants with extreme tricuspid regurgitation, the murmur of tricuspid regurgitation is conspicuous, generally associated with a thrill, and a tricuspid diastolic rumble could additionally be audible. A murmur of the arterial duct could also be distinguished in the second and third left intercostal house, especially after prostaglandin has been administered to promote ductal patency. Unless the atrial septum is profoundly restrictive, affecting cardiac output, the caliber of the arterial pulses is regular. The most hanging and consistent finding earlier than prostaglandins are administered is hypoxemia refractory to elevated inspired oxygen focus and a gentle degree of hypocarbia, reflecting the tachypnea. The differential prognosis of a cyanotic child with a delicate systolic murmur, gentle cardiac enlargement, and oligemic lungs is pretty in depth (Table 41. Echocardiographic Features Although echocardiography has been advocated as the imaging modality for the diagnosis and treatment of many forms of neonatal congenital coronary heart disease, each echocardiography and angiocardiography are often required for a whole evaluation of this dysfunction. Identification of the extent of ventriculocoronary connections may be troublesome by echocardiography. Echocardiographic imaging has not allowed one to establish reliably coronary arterial stenosis or interruption in neonates, As a result of these limitations, angiocardiography could be crucial in infants with severe hypoplasia of the best ventricle, in whom a high incidence of ventriculocoronary artery connections is anticipated. The differential radiographic diagnosis of utmost cardiomegaly within the new child contains the conditions shown in Table 41. Although the noninvasive identification of pulmonary infundibular and valve atresia is acknowledged readily. In the previous, the pulmonary valve is anatomically imperforate, whereas within the latter, the dearth of forward move is because of excessive pulmonary artery strain with poor proper ventricular operate or very severe tricuspid insufficiency. As mentioned previously, it additionally is possible to have anatomic valve atresia with extreme tricuspid regurgitation and a low right ventricular stress, hence the importance of differentiating the 2 situations. Finally, an try to doc coronary artery connections from the proper ventricle must be made, recognizing that this may be difficult. Indeed, the initial therapeutic plan typically is dictated by echocardiographic findings. It is important to verify the functional standing of the interatrial septum because the neonate relies on compulsory right-toleft shunting to maintain cardiac output. The interatrial communication may be assessed readily by the subcostal strategy with a mixture of imaging and Doppler interrogation. The atrial septum hardly ever may assume aneurysmal proportions, with septum primum herniating via the mitral valve. It could additionally be troublesome to detect forward move across an extremely stenotic, obstructive tricuspid valve and patency could also be decided finest by the identifying tricuspid regurgitation. The proper ventricular size, which usually corresponds to the dimension of the tricuspid annulus, may be imaged by a mix of subcostal and precordial views. Significant coronary artery abnormalities with a right ventricle dependence for myocardial flow has been predicted by an analysis of the scale of the tricuspid valve relative to the patient size with a Z-score of < -2. Subcostal echocardiographic view in pulmonary atresia and intact ventricular septum demonstrating an interatrial communication with an aneurysmal flap; shade Doppler (right panel) reveals right-to-left shunting in blue. Subcostal view demonstrating an imperforate valve that was subsequently dilated at cardiac catheterization. Jeffrey Small horn, Director of Echocardiography, Division of Cardiology, University of Alberta, Canada. Furthermore, using echocardiography, it could be troublesome to doc without any doubt these sufferers with tenuous proximal aortocoronary connections (55). The stage of systemic arterial oxygen saturation knowledge displays the magnitude of pulmonary blood move. Before the era of routine administration of prostaglandin, these infants became progressively hypoxemic coincident with functional and anatomic closure of the arterial duct. The administration of prostaglandin, by advantage of its motion on the arterial duct and the pulmonary vascular resistance, augments pulmonary blood flow, and thus arterial saturation increases. The hemodynamic evaluation of the affected person with the hypertensive right ventricle establishes right ventricular stress at or above systemic levels. When dealing with the patient with huge cardiac enlargement, proper ventricular pressure may be substantially lower than systemic. If true restriction to atrial circulate is demonstrated then you will want to think about a balloon atrial septostomy at catheterization to avoid a low cardiac output syndrome, especially if decompression of the right ventricle is not to be included in the therapeutic observe. The proper ventricle is at systemic levels of stress or greater, and the end-diastolic strain could additionally be abnormally high, consistent with a noncompliant ventricular chamber. The finding of a subsystemic proper ventricular stress is consistent with a globally deprived proper ventricle. The right ventricle is usually thinned, and extreme tricuspid regurgitation often is current. The functional disturbance of severe tricuspid regurgitation correlates with an Ebstein-like abnormality of the tricuspid valve or severe tricuspid valve dysplasia. In some patients with ventriculocoronary connections, a balloon catheter inflated in the proper ventricle or catheter-induced tricuspid insufficiency with concurrent observation of the simultaneous electrocardiographic tracing may unmask a proper ventricular-dependent coronary circulation. The angiocardiographic investigation of the patient with the hypertensive right ventricle requires proper ventricular angiocardiography in frontal and lateral projections. The reported surgical survival of 27% previous to the provision of prostaglandins was poor (57). Rarely an pressing balloon atrial septostomy could additionally be required for a restrictive septum as pulmonary move improves and should be considered in any neonate that demonstrates persistent low cardiac output with the similar old therapeutic maneuvers. For the premature infant or the extremely small-for-gestational-age infant, a prolonged course of an E-type prostaglandin could also be essential earlier than surgical procedure is undertaken, though that is uncommon in the current surgical era. Once pulmonary blood flow is established, it may be very important acknowledge that systemic oxygen saturation is expounded to the amount of circulate into the pulmonary circulation.
Flomax 0.4 mg buy with mastercard
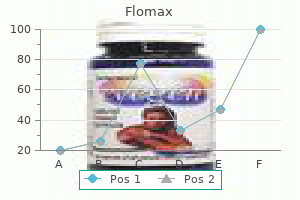
Therefore man health month 0.2 mg flomax buy otc, the procedure ought to be timed such that inotrope-recruitable stroke volume is out there prostate cancer journal of clinical oncology discount 0.2 mg flomax with mastercard. An increase in inflammatory responses together with elevated temperature setpoint is anticipated after sternal closure, with potential need for additional assist. An enhance in oxygen consumption of about 30% can be anticipated with the transition to spontaneous air flow. Excessive work of respiration owing to altered mechanics will shortly destabilize the circulation. Interstage Management and the Timing of Stage 2 Palliation After recovery from stage 1 palliation, acute care is transitioned to chronic therapies that allow preservation of organ operate and somatic development. To detect acute hypoxemia, dehydration, or growth failure between phases 1 and 2 palliation, patients are discharged home with a digital infant scale and pulse oximeter as a half of an interstage monitoring program, and fogeys obtain daily weights and oxygen saturations. Criteria for which parents are instructed to notify a member of the cardiac team are Sa02 < 75% or >90%, weight lack of 30 g, failure to gain 20 g of weight over three days, or enteral consumption <100 mLlkg/ day. Just over half of the monitored sufferers breached surveillance criteria with most sufferers presenting earlier than a hundred days of age. Shunt stenosis, outgrowth of the shunt, and innominate artery narrowing represented the cardiac diagnoses that led to inter stage hypoxemia. Extracardiac causes of desaturation from baseline included viral sickness anemia, and dehydration. Isolated inappropriate weigh~ change or typically poor weight acquire occurred in a 3rd of patients who breached surveillance criteria and was the results of recurrent arch obstruction, sepsis, poor oral consumption necessitating gastrostomy tube placement, failure to adequately regulate gastrostomy tube feeds for weight gain, or progressive heart failure (233). Specifically, preoperative hypoalbuminemia is associated with increased postoperative infection rates, longer hospital stays, and elevated mortality (298). Poor inter stage progress velocity and lower weight-for-age z-score at bidirectional cavopulmonary anastomosis predicts a more advanced postoperative course and longer hospital keep (299,300). Scrutiny of weight change during early infancy offered invaluable somatic growth knowledge for this affected person population. From >1,four hundred patient weight observations, a development curve was generated for infants who survived the interstage interval. Approximately, 25% of our sufferers have undergone open gastrostomy tube placement due to incapability to consume adequate calories with oral feeding alone. Increased attentiveness to dietary intake at our establishment has resulted in improved somatic growth in monitored patients that almost parallels regular infant development with a growth velocity >25 g/day and an increase in weight for age z-score from -1. Attentiveness to nutritional help also offered insight into optimum timing for stage 2 palliation. When comparing mterstage monitored sufferers with those sufferers who have been 10 Normal Infant Growth - 50% eight Cl ~. Interstage progress among survivors of the stage 1 palliation calculated using> 1,four hundred observations of weights. Normal progress is depicted in the shaded area, with the dashed line representing 50% for age. The curve signifies the restricted growth potential of the patient following the first stage of palliation. In this group of patients, growth into later infancy is restricted, not like a standard toddler whose continued development is predicted. Although a extra in depth operation than the bidirectional Glenn shunt, the hemi-Fontan permits for expeditious efficiency of a completion Fontan. A Bidirectional Glenn B Hemi-Fontan not subjected to frequent monitoring of weight and saturation, monitored sufferers had comparable weights to nonmonitored sufferers (5. This observation, along with the demonstrable flattening in progress velocity beyond 4 to 5 months of age call into question the good factor about arbitrarily delaying stage 2 palliation until after 6 months of age. Stage 2: Superior Cavopulmonary Connection Superior cavopulmonary anastomosis prior to completion Fontan improves final survival and is associated with low operative and late mortality (219,302). Anesthetic management usually features a more balanced anesthetic method that avoids prolonged postoperative ventilation, and approaches that include neuraxial opioids may have a favorable impact on early postoperative administration (303). Progression to the cavopulmonary anastomosis reduces each wall stress and atrioventricular valve insufficiency through elimination of the amount load on the one systemic ventricle. It creates a extra environment friendly in-series circulation and will increase diastolic strain with improved coronary artery perfusion (208,221,294). Despitetheyoungerageatstage2 palliationofthemonitored sufferers, weights between teams had been similar: 5. The success of early cavopulmonary anastomosis in these patients deemed at best risk for interstage mortality has modified our overall practice in that stage 2 palliation is electively carried out at four months of age or earlier if essential. The implications of early cavopulmonary anastomosis have been additional reviewed by]aquiss et al. The youthful group, however, required extended mechanical ventilation, had a higher duration of pleural drainage, and had a longer hospital stay. Younger sufferers also had lower oxygen saturations postoperatively compared with the older group, however by hospital discharge, groups had related oxygen saturations (307). Follow-up knowledge on this cohort demonstrated no difference in late issues, preoperative hemodynamics on the time of Fontan palliation, or standing of the patient after completion Fontan (308). These are postulated to be the results of an absence of so-called hepatic issue, which prevents the shunt formation (309). Pulmonary arteriovenous malformations could be reversed by the completion Fontan operation, presumably by restoring hepatic issue to the pulmonary circulation. In each cases, all caval return aside from the coronary sinus is directed to the pulmonary arteries, simulating as carefully as potential the conventional circulatory pattern. This decreases evp and will increase preload to the single ventricle, albeit at the cost of some systemic desaturation. A Lateral tunnel B Extracardiac that is performed within the operating room utilizing certainly one of two techniques; a lateral tunnel or extracardiac conduit. Additional advantages embody a low stage of power loss as decided by computational fluid dynamic studies (310). Although controversial, some research counsel the next incidence of sinus node dysfunction following the lateral tunnel Fontan (311-315). The extracardiac Fontan is constructed by putting a prosthetic conduit between the Iv C and the pulmonary arteries. The benefits include the benefit of the operation and, although somewhat controversial, in all probability a lower incidence of sinus node dysfunction (311-315). To this end, bigger conduits, between 20 and 22 mm in diameter are placed to accommodate development. The use of a fenestration has resulted in excellent survival and shorter hospital stay (206). Additional methods that reduce postoperative hospital stay embrace routine use of the diuretics including spironolactone, an aldosterone antagonist, and furosemide. Supplemental oxygen is used as a pulmonary vasodilator, and afterload discount is given to improve cardiac output and lower single-ventricle filling pressures (316). Outcomes for Staged Palliation Most mortality associated with the staged surgical approach occurs throughout and after stage 1 palliation, with current cumulative early and inter stage mortality within the 5% to 30% range (73,241,317,318).