
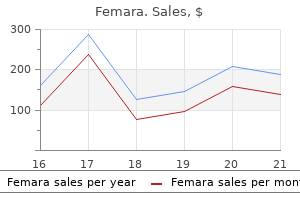
Femara dosages: 2.5 mg
Femara packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Discount 2.5 mg femara visa
Rarely menstrual cup 7 fold 2.5 mg femara order overnight delivery, the signs of thoracic outlet syndrome are attributable to arterial aneurysm menopause involves a decline in 2.5 mg femara cheap fast delivery, and auscultation of the supraclavicular area reveals a bruit. The signs of thoracic outlet syndrome may be elicited by varied maneuvers, together with the Adson test and the elevated arm stress check. The elevated arm stress check is carried out by having the patient hold his or her arms over the top and open and close the arms. Normally, patients without thoracic outlet syndrome can carry out this maneuver for approximately 3 minutes, whereas those affected by thoracic outlet syndrome expertise the onset of symptoms inside 30 seconds. These films must be carefully reviewed for congenital abnormalities such as cervical ribs or overly elongated transverse processes. Paresthesias of the upper extremity radiating into the distribution of the ulnar nerve could also be misdiagnosed as tardy ulnar palsy. If vascular compression exists, edema or discoloration of the arm Brachial plexus Subclavian a. Lateral herniated cervical disk, metastatic tumor, or cervical spondylosis that results TreaTmenT Physical Modalities the primary therapy for sufferers suffering from thoracic outlet syndrome is the rational use of physical remedy to preserve function and palliate pain. Shoulder abnormalities, including subluxation and adhesive capsulitis, have to be aggressively treated. Drug Therapy Gabapentin Gabapentin is first-line pharmacologic treatment for the neuritic pain of thoracic outlet syndrome. The preliminary dose is 300 mg gabapentin at bedtime for two nights, and the patient ought to be cautioned Cervical rib Cervical rib A Subclavian a. The patient underwent surgical removal of the cervical rib, with resulting aid of signs. The drug is usually discontinued owing to laboratory abnormalities erroneously attributed to it. The affected person must be cautioned about unwanted effects, including dizziness, sedation, confusion, and rash. The drug is elevated in 100- to 240-mg increments given in equally divided doses over 2 days, as unwanted facet effects allow, until pain reduction is obtained or a total dosage of 1240 mg/day is reached. Careful monitoring of laboratory parameters is mandatory to keep away from the rare risk of a lifethreatening blood dyscrasia, and on the first sign of blood depend abnormality or rash, the drug must be discontinued. When ache reduction is obtained, the affected person must be stored at that dosage of carbamazepine for a minimum of 6 months before considering tapering of the medicine. Baclofen Baclofen could additionally be of worth in some patients who fail to get hold of aid with gabapentin and carbamazepine. Baseline laboratory exams should be obtained before beginning baclofen, and the patient ought to be cautioned about potential adverse results, which are the same as those related to carbamazepine and gabapentin. Baclofen is began with a 10-mg dose at bedtime for two nights; the drug is then elevated in 10-mg increments given in equally divided doses over 7 days, as side effects enable, until ache reduction is obtained or a total dosage of eighty mg/day is reached. When treating individuals with any of those medication, the doctor should make sure that the affected person knows that premature tapering or discontinuation of the medication might lead to the recurrence of ache, which shall be tougher to management. Invasive Therapy Brachial Plexus Block Brachial plexus block with local anesthetic and steroid is an excellent adjunct to drug therapy of thoracic outlet syndrome. The preliminary block is carried out with preservativefree bupivacaine combined with methylprednisolone. Subsequent every day nerve blocks are carried out in a similar method, by substituting a lower dose of methylprednisolone. CompliCaTionS and piTfallS the pain and dysfunction of thoracic outlet syndrome are troublesome to deal with. Physical therapy should be the first modality in any nicely thought out remedy plan. In basic, the ache of thoracic outlet syndrome responds poorly to opioid analgesics, and these medication should be averted. The cautious use of adjuvant analgesics might assist palliate the pain and permit the affected person to participate in bodily therapy. Correct diagnosis is crucial, as a end result of stretch injuries and contusions of the plexus may reply with time, however plexopathy secondary to tumor or avulsion of the cervical roots requires aggressive therapy. Clinical Pearls Brachial plexus block with local anesthetic and steroid represents an excellent stopgap measure to palliate the pain associated with thoracic outlet syndrome whereas ready for drug remedies to take effect. Correct prognosis is paramount to permit the clinician to design a logical treatment plan. Clinical manifestations, differentiation and therapy pathways, Man Ther 14(6):586�595, 2009. It could occur after seemingly minor trauma or could also be the results of repeated microtrauma. In addition to ache, patients suffering from arthritis of the shoulder joint usually expertise a gradual reduction in useful capacity due to decreasing shoulder range of motion. With continued disuse, muscle wasting may happen, and a frozen shoulder might develop. Magnetic resonance imaging of the shoulder is indicated if a rotator cuff tear is suspected. Radionuclide bone scanning is indicated if metastatic illness or major tumor involving the shoulder is a possibility. Using strict aseptic approach, the practitioner attaches a sterile syringe containing 2 mL of zero. The needle is carefully advanced via the pores and skin and subcutaneous tissues, via the joint capsule, and into the joint. If bone is encountered, the needle is withdrawn into the subcutaneous tissues and is redirected superiorly and slightly more medially. Little resistance to injection is felt; if resistance is encountered, the needle might be in a ligament or tendon and should be advanced slightly into the joint house till the injection can proceed with out significant resistance. The radiograph exhibits all of the attribute features of a hypertrophic type of osteoarthritis of the glenohumeral joint, with joint area narrowing, subchondral sclerosis, large cysts in the glenoid, and massive inferior osteophytosis. Less widespread causes of arthritis-induced shoulder ache include collagen vascular diseases, an infection, villonodular synovitis, and Lyme disease. Collagen vascular illnesses usually manifest as a polyarthropathy quite than a monarthropathy limited to the shoulder joint; nevertheless, shoulder pain secondary to collagen vascular illness responds exceedingly nicely to the intraarticular injection method described here. This injection approach is safe if cautious attention is paid to the clinically related anatomy. The major complication of intraarticular injection of the shoulder is infection, although it should be exceedingly rare if strict aseptic approach is adopted. Approximately 25% of sufferers complain of a transient enhance in ache after intraarticular injection of the shoulder joint, and they need to be warned of this possibility. Clinical Pearls Osteoarthritis of the shoulder is a typical criticism encountered in scientific apply.
Femara 2.5 mg generic fast delivery
Lichenoid dermatitis of the vulva: Diagnosis and differential prognosis for the gynecologic pathologist women's health questions menopause femara 2.5 mg cheap fast delivery. Vulvar lichen sclerosus and neoplastic transformation: A retrospective examine of 976 instances menstrual flow is actually deteriorating buy femara 2.5 mg overnight delivery. Diagnosis of vulval inflammatory dermatoses: A pathologic research with clinical correlation. Allelic imbalance in lichen sclerosus, hyperplasia, and intraepithelial neoplasia of the vulva. Monoclonal -T-cell receptor rearrangement in vulvar lichen sclerosus and squamous cell carcinoma. Claudin and p53 expression in vulvar lichen sclersosus and squamous-cell carcinoma. Immunohistochemical staining for p16 and p53 in premalignant and malignant epithelial lesions of the vulva. Histology of lichen sclerosus varies based on website and proximity to carcinoma. Monoclonal origin of vulvar intraepithelial neoplasia and a few vulvar hyperplasias. Differentiated vulvar intraepithelial neoplasia is often present in lesions, previously recognized as lichen sclerosus, which have progressed to vulvar squamous cell carcinoma. Hypertrophic lichen sclerosus with dyskeratosis and parakeratosis � a standard presentation of vulvar lichen sclerosus not related to a significant risk of malignancy. Histologic and biomolecular features of papillomatosis of the vulvar vestibule in relation to human papillomavirus. Vestibular papillae of the vulva: Lack of proof for human papillomavirus etiology. Vulvar condylomas and squamous vestibular micropapilloma: Differences in look and response to treatment. Evidence of human papillomavirus deoxyribonucleic acid in vulvar squamous papillomatosis. Atypical melanocytic nevi of the genital kind with a discussion of reciprocal parenchymalstromal interactions in the biology of neoplasia. Differentiated squamous intraepithelial lesion-like modifications within the epidermis overlying anogenital melanocytic nevi: A diagnostic pitfall. Epidermal inclusion cyst of the clitoris 30 years after female genital mutilation. Human Bartholin gland, duct, and duct cyst: Histochemical and ultrastructural study. Report of twenty-five sufferers from the United States with distinguished mucocutaneous involvement. Vulvar vestibulitis syndrome: Reliability of analysis and evaluation of present diagnostic standards. Enhanced synthesis of proinflammatory cytokines by vulvar vestibular fibroblasts: Implications for vulvar vestibulitis. Vulvar vestibulitis: A histopathologic research of 36 circumstances, including human papillomavirus in situ hybridization evaluation. Women with main Sj�gren syndrome and with non-Sj�gren sicca syndrome present related vulvar histopathologic and immunohistochemical modifications. Multinucleated atypia of the vulva: Report of a distinct entity not related to human papillomavirus. A clinicopthologic examine of labia minora hypetrophy: Signs of localized lymphedema had been universal. Localized lymphedema of the vulva: A clinicopathologic examine of 2 instances and a evaluation of the literature. Massive localized vulval lymphedema, with lymphangiomas of the labia majora, misdiagnosed as viral warts. Vulval intestinal/enteric heterotopia with a 10-yr follow-up: A case report and review of the literature. Pseudoangiomatous stromal hyperplasia in lesions involving anogenital mammary-like glands. Prostatic-type tissue within the lower female genital tract: A morphologic spectrum, including vaginal tubulosquamous polyp, adenomyomatous hyperplasia of paraurethral Skene glands (female prostate), and ectopic lesion in the vulva. Ectopic salivary gland within the vulva (choristoma): Report of a case and review of the literature. Vulvar endometriosis in a surgical scar after excision of the Bartholin gland: Report of a case. Endometrial stromal sarcoma of the vulva arising in extraovarian endometriosis: A case report and literature evaluation. Localized amyloidosis of the vulva with and without vulvar intraepithelial neoplasia: Report of a sequence. Sebaceous hyperplasia of the vulva: A collection of instances reporting no association with the Muir-Torre syndrome. The nature of atypical multinucleated stromal cells: A examine of 37 circumstances from different websites. Vulvar adenosquamous carcinoma arising in a hidradenoma papilliferum, with quickly deadly consequence: Case report. Pseudoangiomatous stromal hyperplasia of the vulva presenting as a polypoid vulvar lesion: A lesion related to anogenital mammary-like tissue � report of a case and evaluation of the literature. Hidradenoma papilliferum: A clinicopathologic research of 264 tumors from 261 sufferers, with emphasis on mammary-type alterations. Adenocarcinoma in situ arising in vulvar papillary hidradenoma: Report of 2 circumstances. Immunophenotypic and viral (human papillomavirus) correlates of vulvar seborrheic keratosis. Recurrent phyllodes tumor of the vulva: A case report with evaluate of diagnostic standards and differential analysis. Vulval microglandular adenosis-like neoplasm with chondromyxoid stroma: Report of a singular case. Proliferating trichilemmal tumor of the vulva: Case report of evaluation of the literature. Vulvar syringoma: A clinicopathologic and immunologic research of 18 sufferers and outcomes of remedy. Vulvar syringomas with deep extension: A potential histopathologic mimic of microcystic adnexal carcinoma. Trichofolliculoma of the vulva in association with vulvar intraepithelial neoplasia: Report of three circumstances and evaluation of the literature. Inverted follicular keratosis of the vulvar skin: A lesion that can be confused with squamous cell carcinoma.
Generic femara 2.5 mg with mastercard
Sections must also be taken from areas that differ in appearance (fleshy breast cancer awareness shirts order femara 2.5 mg amex, necrotic menstrual effects femara 2.5 mg with amex, hemorrhagic) to exclude serous carcinoma. Blocks of exophytic (surface) tumor and ruptured locules should be separately recognized. The papillae are typically advanced with a hierarchical branching pattern during which progressively smaller fibrous-cored papillae are in flip covered by stratified tumor cells that form cellular tufts or buds. Some cells, typically apical, comprise copious eosinophilic cytoplasm; ciliated cells are also often present and hobnail cells may be seen. Luminal mucin may be conspicuous and cytoplasmic mucin, if current, is confined to the information of the cells. This instance demonstrates the progressive hierarchical branching typical of a serous borderline tumor of the usual sort. This instance has a prominent fibrous stroma with the epithelial element invaginating within it. This example exhibits the typical variation in dimension of papillae with focal small papillary tufts. A higher-power view shows the typical tufted papillae, many of which have apical cells with ample eosinophilic cytoplasm. Another high-power view demonstrates the invagination of epithelium into the stroma. This example demonstrates the typical architectural and cytologic options, the latter being comparatively bland in contrast to serous papillary carcinoma. Dilated tubular glands appear considerably endometrioid in character, a function not uncommon in serous borderline tumors. Cells with plentiful eosinophilic cytoplasm, hardly ever seen in carcinoma, are conspicuous. The nuclear atypia varies from mild to moderate, however uncommon cells with greater atypia may be current. Mitotic figures are usually rare and nucleoli are solely occasionally conspicuous. Infarction of the fibrous-cored papillae may be seen that will elicit a desmoplastic response with entrapment of tumor cells, doubtlessly mimicking an autoimplant (see subsequent heading) or invasion. Small foci of borderline tumor may be a focal or multifocal discovering in an in any other case typical serous cystadenoma. Irrespective of the precise time period elected, communication with the treating doctor is most important. Florid mesothelial hyperplasia in the wall and on the floor of the tumor is occasionally current (Chapter 20). If the latter is more than minimal, caution must be taken to exclude noninvasive serous carcinoma. These mimic the noninvasive desmoplastic implants that happen on the extraovarian peritoneum (see below), appearing as sharply delimited desmoplastic foci that usually occur on the serosal floor but sometimes on the inside (cystic) floor of the tumor. In some circumstances, an look much like that of an autoimplant could also be a result of infarction. The invasive cells may occupy spaces that will outcome from fluid secretion by the tumor cells or might symbolize lymphatics (see last level below). We have seen instances of this kind with extraovarian invasive tumor confirming that the first focus was frank carcinoma. Implants could additionally be grossly visible as small nodules or plaques, but are sometimes microscopic. Only two small nests of neoplastic epithelium are present inside an exuberant desmoplastic stroma. The typical papillary tufts and papillae are well demarcated from the adjacent omental fat with no stromal response. Adjacent benign-appearing glands could characterize endosalpingiosis but could represent maturation of the implant. The implants contain the peritoneal surface together with invaginations between omental fat lobules that might be misinterpreted as invasion. Occasionally, probably as a result of maturation, glands indistinguishable from endosalpingiosis may be seen. Fibrin and acute inflammatory cells could additionally be conspicuous, notably superficially. The epithelial cells and associated reactive stroma increase the septum between two lobules of omental fat. A focal desmoplastic response (left), lymphoid aggregates (right), and many psammoma our bodies are also present. EpithElial Ovarian tumOrs � 399 Invasive implants account for no more than 5% of implants; the frequency is even lower in some research. The epithelial:stromal ratio is often higher than in noninvasive desmoplastic implants. Differential prognosis and/or associated options of implants: � Endosalpingiosis (Chapter 19). The former often immunoreact with epithelial markers (we choose claudin-4; solely membranous staining is taken into account positive) however not for calretinin, whereas the other findings indicate mesothelial cells. An implant will typically elicit a putting peritoneal histiocytic infiltrate (sometimes with admixed hyperplastic mesothelial cells) which will obscure the neoplastic cells of the implant. Left: Most of the tumor entails the nodal parenchyma however some tumor cells are present within subcapsular lymphatics (extreme proper in same image). A focus of tumor (right) is associated with intranodal endosalpingiosis (left) from which it doubtless originated. The left half demonstrates low-grade serous carcinoma with nearly confluent papillae, whereas the proper half exhibits serous borderline neoplasia. Differential analysis M�llerian borderline tumors of blended cell kind (see Chapter 14). Endometrioid papillary tumor of borderline malignancy and endometrioid and clear cell carcinomas (Chapter 14). Both noninvasive and invasive implants had been associated with subsequent carcinoma however the danger was greater within the latter. Overall, 5% of sufferers were dead of illness and one other 6% had persistent illness eventually follow-up. Surprisingly, the only discovering that predicted recurrence was a better 402 � EpithElial Ovarian tumOrs Associated invasive carcinoma in the main tumor. This discovering has not been prognostic in most research with the exception of a particular pattern of involvement noted by McKenney et al. Features of implants, metastases, and recurrences � In the examine by Longacre et al. The recurrences may be discovered soon after initial remedy or years later, in some cases after a quantity of low-grade recurrences. Definitional features: � Destructive stromal invasion, often with a desmoplastic stroma, with the 2 most typical patterns (often admixed) being micropapillae and small nests (often inside a nonepithelial-lined house or cleft). Less widespread patterns embody macropapillae (fibrous-cored papillae, usually lying within an area � so-called inverted pattern); cribriform; glands and/ or cysts; sheets (that might have slit-like spaces); and single cells. Other findings: � Psammoma bodies, which may be numerous and are hardly ever large (see below).
Cheap 2.5 mg femara with amex
Thorough sampling is essential to uncover inclusionary or exclusionary findings; immunostains can also be helpful pregnancy 3d week by week buy generic femara 2.5 mg. Rare sufferers with high-stage tumors have survived over 4 years after intensive chemotherapy menopause the musical reviews buy 2.5 mg femara amex, radiation remedy, or both. In addition to stage I illness, doubtlessly favorable prognostic options embody age >30 years, a normal preoperative calcium degree, a tumor size <10 cm, an absence of enormous cells, treatment by bilateral oophorectomy, and postoperative multiagent chemotherapy and radiotherapy. The ovarian tumors have the same histologic options as these in the broad ligament (Chapter 11). The ovarian tumors usually occur in adults, and are related to the same old signs of an ovarian tumor. The tumors are virtually invariably unilateral, encapsulated, common 12 cm in diameter, and are strong or solid and cystic. The solid tissue is usually lobulated and gray�white to tan or yellow, and rubbery to firm. The microscopic appearance is identical to that of the broad ligament tumors (Chapter 11), together with frequent positivity for inhibin. Hollow tubules lined by cells with considerable pale cytoplasm mimic a Sertoli cell tumor. Typical appearance of the stable areas of such neoplasms shows a refined tubular sample and cells with oval to fusiform nuclei. Differential diagnosis Sex cord tumors, notably Sertoli cell tumors (Chapter 16). Rare wolffian tumors have a distinguished growth of fusiform to spindle cells, however different distinctive patterns, such as sieve-like, might be diagnostic. The uncommon sufferers with high-stage tumors died of disease or had been alive with illness finally follow-up. Elevated testosterone levels as a outcome of adjoining hilus cell hyperplasia may cause androgenic manifestations. Because rete cystadenomas are sometimes misdiagnosed as serous cystadenoma, their frequency is likely a lot greater than instructed by the small variety of reported circumstances. Rete adenomas usually occur in middle-aged or aged patients; most are incidental microscopic findings. The one well-documented rete adenocarcinoma occurred in a 52-year-old woman with ascites. Rete cysts and rete cystadenomas are hilar but might increase into the medulla and infrequently the cortex. Rete cystadenomas have partitions of fibrovascular tissue and smooth muscle and little or no stroma of ovarian kind, and most have an irregular lining with irregularly spaced shallow crevices. Rete cysts and cystadenomas are lined by cuboidal, columnar, or most often flattened cells with bland nuclear features. In half the reported cases, the cyst walls contained hilus cells that were usually hyperplastic. Rete adenomas are well-circumscribed hilar proliferations of carefully packed elongated small tubules; some tubules may be dilated and contain easy papillae. The tubules and papillae are lined by a single layer of cuboidal to columnar cells resembling these of the normal rete. The rete adenocarcinoma consisted of branching hollow or stable tubules and cysts containing papillae with fibrovascular or hyalinized cores. The tubules and papillae were lined by atypical cuboidal nonciliated cells, and focally, transitional-like cells; mitotic figures had been numerous. The wall accommodates bundles of easy muscle (lower left) and Leydig cells in a band-like association (lower heart and right). Differential prognosis Rete cysts and cystadenomas are distinguished from different benign ovarian and paraovarian cysts on the idea of a mixture of their hilar location (not all the time clearly establishable in giant tumors), mural smooth muscle and/or hilus cells, their attribute crevices, and an absence or rarity of ciliated cells. Rare examples of rete hyperplasia (Chapter 12), in contrast to adenomas, have merged virtually imperceptibly with the conventional rete and their margins have been poorly circumscribed. The retiform look of the tubules aids within the differential with a transitional cell carcinoma. Leiomyomas occur from the second to eighth decades of life; 80% arise in premenopausal women. The tumors are often incidental findings, but if larger, may current as an adnexal mass. Differential diagnosis Fibroma (vs typical leiomyoma) and cellular fibroma (vs cellular leiomyoma). Fibromas are rather more widespread than leiomyomas and are composed of fibroblastic cells typically arranged in a storiform sample. The differential analysis of ovarian leiomyomas with uncommon options consists of all kinds of ovarian tumors. Tortuous arteries and veins fed and drained mobile proliferations of anastomosing sinusoidal capillary channels. The differential diagnosis of hemangiomas of every kind includes the closely packed vessels within the ovarian medulla which are usually a conspicuous normal finding in older ladies, a steroid cell tumor with distinguished pseudovascular areas (Chapter 16), and angiosarcoma (distinguishable utilizing criteria similar to these used in soft tissues). Miscellaneous PriMary ovarian TuMors � 549 Neural tumors have together with ganglioneuroma and plexiform neurofibromatosis that might be associated with synchronous involvement of other sites within the feminine genital tract. Rare sarcomas of assorted sorts have been related to floor epithelial�stromal tumors, notably serous, mucinous, and clear cell carcinomas, typically as mural nodules. One case of ovarian involvement by soft-tissue sort of fibromatosis has been reported. Diffuse and pseudopapillary patterns predominate, with occasional nests and small cysts full of colloid-like material. Distinctive options embrace eosinophilic globules, myxohyaline stroma, vacuolated cells, and foamy cells. Large aggregates of cells with plentiful pale cytoplasm impart a resemblance to a steroid cell tumor of the lipid-rich sort. Left: Gland-like spaces are separated by stroma containing quite a few hyaline bodies. Left middle: Higher-power view of pseudopapillary pattern; observe eosinophilic cells with bland nuclear features and cytoplasmic hyaline our bodies. The differential includes sex cord�stromal tumors, steroid cell tumors, and struma ovarii. Because of the oxyphilic tumor cells, a steroid cell tumor and oxyphilic struma could additionally be considerations. However, there are lots of routine microscopic differences between well-sampled examples of these numerous tumors. Microcystic stromal tumors (see Chapter 16) have an identical Miscellaneous PriMary ovarian TuMors � 551 tumors additionally stained for inhibin, considered one of which co-expressed calretinin. The differential analysis is mainly with different tumors containing oxyphil cells (Appendix 14), particularly tumors in the intercourse cord�stromal and steroid cell class because of their typical positivity for inhibin and calretinin. If the analysis is suspected by the nested (zellballen) pattern, which can be only focal or subtle, it can be confirmed by staining for chromogranin and S100. The differential also consists of metastatic strong pseudopapillary tumor of pancreatic origin, considered one of which has been reported (see Chapter 18).
2.5 mg femara generic
Moderate to high-grade mucinous adenocarcinomas may have nonspecific gross options or in some cases have a gelatinous consistency menstrual cramps 9dpo 2.5 mg femara buy fast delivery. Intestinal-type adenocarcinomas have the everyday pseudoendometrioid morphology of colorectal metastases womens health 06484 2.5 mg femara buy visa. Signet-ring cell tumors have the spectrum of Krukenberg tumors, including its tubular variant. This neoplasm had a conspicuous tubular sample, potentially mimicking a Sertoli�Leydig cell tumor. Although not evident on this image, signet-ring cells were present elsewhere (so-called tubular Krukenberg tumor). There is a conspicuous infiltrate of signet-ring cells; the first tumor within the appendix was resected six years beforehand. Small aggregates of mucinous cells have a sample harking again to the formations seen in mucinous carcinoid tumors. Mucinous carcinomas not of signet-ring-cell-type resemble those originating elsewhere in the intestinal tract, or even more so, the pancreas. Distinction from morphologically comparable metastases originating elsewhere is basically or completely depending on medical analysis. Distinction from main endometrioid and mucinous carcinoma is as thought-about underneath the heading of intestinal carcinomas. Most of the primary tumors are small intestinal (usually ileum); less widespread websites include colon, appendix, abdomen, pancreas, and bronchus. Forty % of girls in whom metastases are discovered at operation have carcinoid syndrome; some also have indicators and symptoms referable to intestinal or ovarian involvement. As many as 25% of patients, nonetheless, could stay asymptomatic for years postoperatively, with reduction of the carcinoid syndrome. Well-differentiated appendiceal neuroendocrine (carcinoid) tumors of typical sort hardly ever spread to the ovary. The ovarian tumors, most of which are bilateral, are sometimes predominantly solid, with easy or bosselated surfaces. Scattered cysts, typically full of watery fluid, could create an appearance much like that of a cystadenofibroma; uncommon tumors are predominantly cystic. Microscopic features the patterns are just like those of main ovarian carcinoids (Chapter 15), most commonly insular, however trabecular, combined, and barely, solid tubular patterns are found. Small spherical acini are widespread, usually containing a homogeneous eosinophilic secretion which will endure calcification, which is typically psammomatous. Occasionally, nests of tumor cells disintegrate, with the cells separating from one another. Carcinoid is the metastatic tumor that most usually elicits an extensive fibromatous stromal proliferation; often, the stroma is extensively hyalinized. The cytologic features of the tumors are as seen elsewhere; exceptionally the cells have ample eosinophilic cytoplasm. An related dermoid cyst, mucinous tumor, or struma ovarii nearly by definition excludes metastatic carcinoid permitting for the uncommon chance of a collision tumor. The epithelial nests of those tumors include transitional cells with oval, pale, grooved nuclei rather than the round nuclei with stippled chromatin of carcinoids. Benign and borderline adenofibromas and endometrioid adenocarcinomas with small glands. These are distinguished from carcinoids by their differing patterns and cytologic options. In tough instances in the foregoing differential diagnostic considerations, further sampling and immunostaining for chromogranin, synaptophysin, peptide hormones, and serotonin will normally be diagnostic. In most cases, the primary pancreatic tumor is an adenocarcinoma of ordinary ductal sort. Ductal-type carcinomas vary from stable with a number of nodules to a large multiloculated mass mimicking a primary ovarian mucinous tumor. Metastatic ductal carcinomas frequently include cysts resembling these of major ovarian mucinous tumors with cyst linings that may range in appearance from benign, to borderline, to carcinomatous. Acini, some of them dilated, and rounded cells with conspicuous eosinophilic cytoplasm are outstanding. Metastatic acinar-type pancreatic adenocarcinomas are usually highly mobile with only scanty fibrous stroma and usually have both a small acinar sample or a solid-cribriform pattern with comedonecrosis. The tumor cells have eosinophilic granular cytoplasm and uniform nuclei with distinguished nucleoli. Neuroendocrine tumors are also often extremely cellular, being composed of oxyphilic cells with nuclear features that are relatively uniform in some cases however overtly malignant in others. The one reported metastatic strong pseudopapillary neoplasm had the everyday features of that tumor (Chapter 17), but notably the ovarian illness was bilateral in contrast to all main ovarian tumors of this kind. Differential diagnosis: � Ductal-type carcinomas are usually confused with primary ovarian mucinous carcinomas. High-stage, bilaterality, a quantity of tumor nodules separated by regular ovarian stroma, floor implants, lymphovascular invasion throughout the ovary, and the findings noted above point out their doubtless metastatic nature. Immunoreactivity for chymotrypsin and/or trypsin and unfavorable staining for neuroendocrine markers facilitate the analysis. Occasional inhibin immunoreactivity in acinar-type carcinomas can lead to potential confusion with a sex cord�stromal tumor; positivity for the aforementioned enzymes will point out the proper prognosis. Metastatic tuMors to the ovary � 573 � Neuroendocrine carcinomas vs main ovarian neuroendocrine tumors (Chapter 14). The latter usually are associated with an obvious surface epithelial tumor and lack the standard options of a metastatic tumor (bilaterality, multinodularity, surface implants). The final of those are significantly widespread in some areas of the world, corresponding to Thailand, but may be seen in different parts of the world. Differential prognosis: � Metastatic adenocarcinomas of biliary tract origin are distinguished from primary mucinous tumors using the criteria listed for metastatic pancreatic adenocarcinomas. Although 75% of sufferers are asymptomatic, the clinical picture can occasionally simulate that of a primary ovarian tumor. Rarely, ovarian metastases are evident before the first tumor is detected, notably in circumstances of lobular carcinoma. Although ovarian metastases of breast cancer are usually accompanied by different intra-abdominal metastases, involvement is restricted to the ovary in 15% of instances. Lobular carcinomas, together with these of signet-ring cell sort, unfold to the ovary extra frequently than ductal carcinomas, and yet 75% of ovarian metastases from breast cancer are of the ductal sort because of their greater frequency. The metastatic tumors are usually <5 cm in dimension and bilateral in two-thirds of instances. Cysts are prominent in 20% of tumors and barely the tumor is totally cystic; not often, papillae are seen.
Buy discount femara 2.5 mg line
Rare blended carcinomas are comprised of variable proportions of endocervical-like and serous-like epithelium and infrequently different cell types menstrual knitting femara 2.5 mg generic mastercard. Surface epithelial�Stromal tumorS � 463 borderline tumor of blended cell type from which they probably arose breast cancer 3 day walk michigan femara 2.5 mg purchase amex. They have been composed entirely or nearly completely of endocervical-like epithelium; polygonal eosinophilic cells and/or foci of endometrioid and squamous differentiation have been also sometimes seen. Hobnail, eosinophilic, squamous, clear, and signet-ring cells had been also present in varying proportions. The admixture of considered one of these elements inside an endometrioid carcinoma adversely affects the prognosis. Surface epithelial tumors (serous, mucinous, endometrioid, clear cell) are not often blended with an uncommon high-grade part similar to hepatoid carcinoma, pulmonary-type small cell carcinoma, neuroendocrine carcinoma, or choriocarcinoma. Atypical and borderline endometrioid adenofibromas of the ovary: A report of 27 circumstances. A clinicopathologic analysis of atypical proliferative (borderline) tumors and well-differentiated endometrioid adenocarcinomas of the ovary. Invasive patterns in stage I endometrioid and mucinous ovarian carcinomas: A clinicopathologic analysis emphasizing favorable outcomes in carcinomas without harmful stromal invasion and the occasional malignant course of carcinomas with limited damaging stromal invasion. Unravelling the 2 entities of endometrioid ovarian cancer: A single heart clinical experience. Ovarian endometrioid tumors of low malignant potential: A clinicopathologic study of 30 circumstances with comparability to well-differentiated endometrioid adenocarcinoma. Endometrioid proliferative and low malignant potential tumors of the ovary: A clinicopathologic study of 46 circumstances. Sertoliform endometrioid carcinomas of the ovary: A clinicopathological and immunohistochemical research of thirteen cases. Oxyphilic endometrioid carcinoma of the ovary and endometrium: A report of 9 circumstances. Ovarian endometrioid tumors mimicking Sertoli and Sertoli�Leydig cell tumors: Sertoliform variant of endometrioid carcinoma. Endometrioid carcinoma of the ovary with a prominent spindle-cell part, a source of diagnostic confusion: A report of 14 cases. Ovarian endometrioid carcinomas resembling sex-cord stromal tumors: A clinicopathological evaluation of thirteen cases. Endometrioid epithelial tumors: immunohistochemical and molecular findings Aysal A, Karnezis A, Medhi I, et al. Ovarian endometrioid adenocarcinoma: Incidence and clinical significance of the morphologic and immunohistochemical markers of mismatch restore protein defects and tumor microsatellite instability. Mismatch repair protein expression in endometrioid carcinoma of the ovary: Incidence and clinicopathologic associations in 77 cases. Differential vimentin expression in ovarian and uterine corpus endometrioid adenocarcinomas: Diagnostic utility in distinguishing double primaries from metastatic tumors. Polymerase epsilon exonuclease domain mutations in ovarian endometrioid carcinoma. Utility of hepatocyte nuclear factor-1 as a diagnostic marker in ovarian carcinomas with clear cells. Molecular-based classification algorithm for endometrial carcinoma categorizes ovarian endometrioid carcinoma into prognostically important teams. Ovarian endometrioid carcinomas resembling sex cord�stromal tumors: An immunohistochemical study. Ovarian endometrioid carcinomas simulating intercourse cord-stromal tumors: A study utilizing inhibin and cytokeratin. Transitional cell-like morphology in ovarian endometrioid carcinoma: Morphologic, immunohistochemical, and behavioral features distinguishing it from high-grade serous carcinoma. Endometrioid adenocarcinoma of the ovary mimicking serous borderline tumor: Report of a sequence of circumstances. Hormone receptor-negative, thyroid transcription issue 1-positive uterine and ovarian 463. Malignant mullerian mixed tumor arising from ovarian serous carcinoma: A clinicopathologic and molecular research of two cases. Malignant mullerian mixed tumor of the ovary associated with yolk sac tumor, neuroepithelial and trophoblastic differentiation (teratoid carcinosarcoma). Presence of a sarcomatous component outside the ovary is an adverse prognostic factor for primary ovarian malignant combined mesodermal/mullerian tumors: A clinicopathologic examine of forty seven cases. Comparative mutational profiling of multifocal low grade endometrioid adenocarcinomas utilizing oncogene point mutation and loss of heterozygosity evaluation. Discordant genetic modifications in ovarian and endometrial endometrioid carcinomas: a possible pitfall in molecular diagnosis. Implication of genomic characterization in synchronous endometrial and ovarian cancers of endometrioid histology. Use of gene expression profiles to stage concurrent endometrioid tumors of the endometrium and ovary. Frequent microsatellite instability in synchronous ovarian and endometrial adenocarcinoma and its usefulness for differential prognosis. Synchronous major cancers of the endometrium and ovary: A single establishment evaluation of 84 cases. Simultaneously detected endometrial and ovarian carcinomas � a potential clinicopathologic examine of 74 circumstances: A Gynecologic Oncology Group examine. Juvenile granulosa cell tumor arising in ovarian adenosarcoma: An uncommon form of sarcomatous overgrowth. Mesodermal (mullerian) adenosarcoma of the ovary: A clinicopathological evaluation of 40 cases and evaluation of the literature. Benign and low grade variants of blended mesodermal tumor (adenosarcoma) of the ovary and adnexal region. Mullerian adenosarcoma with a neuroectodermal element associated with an endometriotic cyst of the ovary: A case report. Primary extrauterine endometrial stromal neoplasms: A clinicopathological study of 20 instances and a review of the literature. Primary endometrioid stromal sarcoma of the ovary: A clinicopathologic research of 27 circumstances with morphologic and behavioral options just like those of uterine low-grade endometrial stromal sarcoma. Prognostic favors in ovarian carcinosarcoma: a clinicopathological and immunohistochemical analysis of 23 cases. Two cases of carcinosarcomas of the ovary concerned in hereditary cancer syndromes. Endometrioid stromal sarcomas of the ovary: A clinicopathologic analysis of 23 circumstances. Histological grading of ovarian clear cell adenocarcinoma: Proposal for a easy and reproducible grouping system primarily based on tumor growth structure. Clear cell carcinoma of the ovary: A report from the primary Ovarian Clear Cell Symposium, June 24, 2010. Clear cell carcinoma of the ovary: Evaluation of prognostic parameters primarily based on a clinicopathologic evaluation of one hundred circumstances. Do clear cell ovarian carcinomas have poorer prognosis compared to different epithelial cell types
Order femara 2.5 mg line
In addition to ache menstrual belt order 2.5 mg femara with visa, patients with arthritis of the midtarsal joint typically experience a gradual decrease in functional capability because of lowered midtarsal range of motion that makes simple on an everyday basis tasks such as strolling and climbing stairs quite troublesome women's health group rocky hill ct femara 2.5 mg buy on line. Magnetic resonance imaging of the midtarsal joint is indicated if aseptic necrosis, an occult mass, or a tumor is suspected. Primary and metastatic tumors of the foot may also manifest in a way much like arthritis of the midtarsal joint. TreaTmenT Initial treatment of the ache and practical disability related to arthritis of the midtarsal joint includes a mixture of nonsteroidal antiinflammatory medication or cyclooxygenase-2 inhibitors and physical therapy. The main complication of intraarticular injection of the midtarsal joint is infection, although this should be exceedingly uncommon if strict aseptic method is adopted. At this point, the needle is rigorously superior at a right angle to the dorsal aspect of the ankle via the pores and skin, subcutaneous tissues, and joint capsule and into the joint. The injection method described is extremely efficient in treating the pain of arthritis of the midtarsal joint. However, the deltoid ligament is vulnerable to pressure from acute harm ensuing from sudden overpronation of the ankle or repetitive microtrauma to the ligament from overuse or misuse, corresponding to long-distance operating on gentle or uneven surfaces. The deep layer attaches below to the medial physique of the talus, and the superficial fibers connect to the medial talus, the sustentaculum tali of the calcaneus, and the navicular tuberosity. SignS and SympTomS Patients with deltoid ligament pressure complain of pain just under the medial malleolus. Coexistent bursitis and arthritis of the ankle and subtalar joint may be present and may confuse the medical image. The extra superficial tibiocalcaneal ligament (arrowhead) may have vertical striations as well. The skinny, vertical, low-signal structure superficial to the tibiocalcaneal ligament is the flexor retinaculum (solid arrow). Bursitis, tendinitis, and gout of the midtarsal joints might coexist with deltoid ligament pressure, thus complicated the diagnosis. With the decrease extremity barely kidnapped, the decrease margin of the medial malleolus is identified. At this point, the needle is fastidiously superior at a 30-degree angle to the ankle through the pores and skin and subcutaneous tissues to impinge on the lower margin of the medial malleolus. The needle is then withdrawn slightly, and the contents of the syringe are gently injected. If vital resistance is encountered, the needle is probably in the ligament and must be withdrawn barely until the injection can proceed with out important resistance. The main complication of injection is an infection, though this should be exceedingly rare if strict aseptic approach is adopted. A mild technique ought to always be used when injecting around strained ligaments, to avoid further injury to the already compromised ligament. Although the general public typically views this damage as minor, ankle sprains can end result in vital everlasting ache and incapacity. The injection method described is extraordinarily effective in treating the ache of deltoid ligament pressure. Coexistent arthritis, bursitis, and tendinitis may contribute to medial ankle ache, thus necessitating additional treatment with more localized injection of native anesthetic and methylprednisolone. SuggeSteD reaDingS Collins Ms: Imaging evaluation of continual ankle and hindfoot pain in athletes, Magn Reson Imaging Clin N Am 16(1):39�58, 2008. In Atlas of pain administration injection techniques, ed 2, Philadelphia, 2007, saunders, pp 497�500. Anterior tarsal tunnel syndrome is far less frequent than is posterior tarsal tunnel syndrome. Patients might report that holding the foot within the everted position decreases the ache and paresthesias. Physical findings embody tenderness over the deep peroneal nerve on the dorsum of the foot. Active plantar flexion often reproduces the symptoms of anterior tarsal tunnel syndrome. Weakness of the extensor digitorum brevis could also be present if the lateral department of the deep peroneal nerve is affected. Plain radiographs are indicated in all patients who present with foot or ankle ache, to rule out occult bony illness. SignS and SympTomS this entrapment neuropathy manifests primarily as pain, numbness, and paresthesias in the dorsum of the foot that radiate into the primary dorsal net space; these symptoms may also radiate proximal to the entrapment, into the anterior ankle. No motor involvement occurs unless the distal lateral division of the deep peroneal nerve Extensor hallucis longus m. Tendo calcaneus 356 113 � Anterior Tarsal Tunnel Syndrome 357 differenTial diagnoSiS Anterior tarsal tunnel syndrome is usually misdiagnosed as arthritis of the ankle joint, lumbar radiculopathy, or diabetic polyneuropathy. However, lumbar radiculopathy and deep peroneal nerve entrapment might coexist as the double-crush syndrome. Diabetic polyneuropathy generally manifests as a symmetrical sensory deficit involving the complete foot, somewhat than a dysfunction restricted to the distribution of the deep peroneal nerve. When anterior tarsal tunnel syndrome occurs in diabetic sufferers, diabetic polyneuropathy is often additionally present. TreaTmenT Mild cases of tarsal tunnel syndrome usually respond to conservative therapy; surgery must be reserved for severe instances. Avoidance of repetitive actions that could be liable for the event of tarsal tunnel syndrome, corresponding to prolonged squatting or wearing footwear which might be too tight, also can ameliorate the signs. If sufferers fail to respond to these conservative measures, injection of the tarsal tunnel with local anesthetic and steroid is an affordable next step. Tarsal tunnel injection is performed by placing the patient in the supine place with the leg prolonged. A point just medial to the tendon at the skin crease of the ankle is identified and prepared with antiseptic solution. A 11/2-inch, 25-gauge needle is advanced through this point very slowly towards the tibia until a paresthesia is elicited in the internet area between the first and second toes, usually at a needle depth of 1/4 to half of inch. The patient must be warned to count on this paresthesia and instructed to say "There! If no paresthesia is elicited, the needle is withdrawn and is redirected barely more posteriorly until a paresthesia is induced. After cautious aspiration, a complete of 6 mL of 1% preservative-free lidocaine and forty mg ethylprednisolone is slowly injected. After injection, strain is applied to the injection site to decrease the incidence of ecchymosis and hematoma formation. The primary complications of deep peroneal nerve block are ecchymosis and hematoma, which can be averted by making use of pressure to the injection website. Because a paresthesia is elicited with this method, needle-induced trauma to the frequent peroneal nerve is a risk. By advancing the needle slowly and then withdrawing it slightly away from the nerve, needle-induced trauma can be averted.
Buy generic femara 2.5 mg line
Sympathetic nerve block is believed to obtain these targets by blocking the profound sympathetic stimulation caused by viral irritation of the nerve and gasserian ganglion women health center 2.5 mg femara purchase with visa. If untreated pregnancy pillow buy generic femara 2.5 mg online, this sympathetic hyperactivity may cause ischemia secondary to decreased blood flow of the intraneural capillary bed. If this ischemia is allowed to persist, endoneural edema types, thus growing endoneural pressure and causing a further reduction in endoneural blood circulate, with irreversible nerve injury. These sympathetic blocks ought to be continued aggressively until the patient is pain free and ought to be reimplemented if the ache returns. Failure to use sympathetic neural blockade instantly and aggressively, especially in older sufferers, could sentence the patient to a lifetime of affected by postherpetic neuralgia. Because many patients affected by acute herpes zoster are older or have extreme multisystem illness, shut monitoring for the potential unwanted effects of potent opioid analgesics. Adjuvant Analgesics the anticonvulsant gabapentin represents a first-line remedy for the neuritic ache of acute herpes zoster of the trigeminal nerve. Gabapentin is started at a bedtime dose of 300 mg and is titrated upward in 300-mg increments to a most of 3600 mg given in divided doses, as unwanted effects permit. Pregabalin is began at 50 mg thrice a day and may be titrated upward to 100 mg 3 times a day as unwanted facet effects enable. Carbamazepine should be thought of in sufferers affected by extreme neuritic pain who fail to reply to nerve blocks and gabapentin. If this drug is used, strict monitoring of hematologic parameters is indicated, especially in patients receiving chemotherapy or radiation remedy. Antidepressants may be helpful adjuncts in the preliminary therapy of patients affected by acute herpes zoster. After a quantity of weeks of remedy, antidepressants might exert a moodelevating impact, which can be desirable in some patients. Care should be taken to observe intently for central nervous system unwanted effects on this patient inhabitants. In addition, these drugs may trigger urinary retention and constipation, which can mistakenly be attributed to herpes zoster myelitis. Antiviral Agents A few antiviral brokers, together with valacyclovir, famciclovir, and acyclovir, can shorten the course of acute herpes zoster and will even help forestall the event of postherpetic neuralgia. Topical utility of aluminum sulfate as a tepid soak provides wonderful drying of the crusting and weeping lesions of acute herpes zoster, and most sufferers discover these soaks soothing. Zinc oxide ointment may be used as a protective agent, particularly during the therapeutic section, when temperature sensitivity is a problem. Disposable diapers can be utilized as absorbent padding to protect therapeutic lesions from contact with clothes and sheets. CompliCaTionS and piTfallS In most sufferers, acute herpes zoster of the trigeminal nerve is a self-limited disease. In older sufferers and in immunosuppressed patients, nevertheless, issues may happen. Cutaneous and visceral dissemination could vary from a light rash resembling chickenpox to an amazing, life-threatening an infection in these already suffering from extreme multisystem disease. Clinical Pearls Because the ache of herpes zoster normally precedes the eruption of pores and skin lesions by three to 7 days, another painful condition. In this case, ache within the distribution of the primary division of the trigeminal nerve with out an related rash is identified as zoster sine herpete and is, by necessity, a diagnosis of exclusion. Therefore, other causes of head ache should be ruled out before this diagnosis is invoked. Attacks occur with variable frequency, starting from each few days to once each a number of months. More frequent migraine complications are often related to a phenomenon known as analgesic rebound. Between 60% and 70% of sufferers who are suffering from migraine are female, and tons of report a household historical past of migraine headache. The persona sort of migraineurs has been described as meticulous, neat, compulsive, and infrequently inflexible. They are probably to be obsessive of their every day routines and infrequently find it hard to address the stresses of everyday life. Migraine headache could also be triggered by modifications in sleep patterns or diet or by the ingestion of tyramine-containing foods, monosodium glutamate, nitrates, chocolate, or citrus fruits. Changes in endogenous and exogenous hormones, corresponding to with the utilization of birth control tablets, can even trigger migraine headache. Approximately 20% of sufferers affected by migraine headache also experience a neurologic occasion earlier than the onset of pain referred to as an aura. The aura most frequently takes the form of a visual disturbance, however it may also manifest as an alteration in scent or hearing; these are referred to as olfactory and auditory auras, respectively. Migraine that manifests with out other neurologic symptoms known as migraine without aura. Rarely, patients that suffer from migraine experience extended neurologic dysfunction related to the headache pain. Such neurologic dysfunction could final for more than 24 hours and is termed migraine with prolonged aura. These patients are in danger for the event of everlasting neurologic deficit, and risk factors similar to hypertension, smoking, and oral contraceptives have to be addressed. Patients suffering from migraine with complex aura experience significant neurologic dysfunction that will include aphasia or hemiplegia. As with migraine with prolonged aura, sufferers suffering from migraine with advanced aura might develop permanent neurologic deficits. Pallor, tremulousness, diaphoresis, and SignS and SympTomS Migraine headache is, by definition, a unilateral headache. The time from onset to peak of migraine ache is short, ranging from 20 minutes to 1 hour. In contradistinction to tension-type headache, migraine headache is usually related to systemic symptoms, together with nausea and vomiting, photophobia, and sonophobia, in addition to alterations in appetite, mood, and libido. As mentioned, in roughly 20% of sufferers, migraine headache is preceded by an aura (called migraine with aura). The aura is thought to be the results of ischemia of particular areas of the cerebral cortex. A visual aura often happens 30 to 60 minutes before the onset of headache pain; this will likely take the form of blind spots, known as scotoma, or a zigzag disruption of the visible area, called fortification spectrum. If an aura is present, outcomes of the neurologic examination shall be abnormal; the neurologic examination is usually inside regular limits earlier than, during, and after migraine with out aura. Testing is aimed primarily at figuring out occult pathologic processes or different ailments that will mimic migraine headache (see "Differential Diagnosis"). Screening laboratory checks, including an erythrocyte sedimentation fee, complete blood depend, and automatic blood chemistry, should be carried out if the diagnosis of migraine is in question. The focused historical past and physical examination, combined with applicable testing, should allow the clinician to establish and correctly treat any underlying diseases of those organ techniques.