
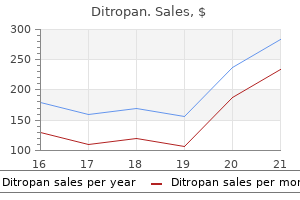
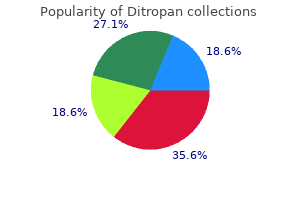
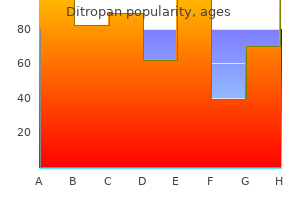
Ditropan dosages: 5 mg, 2.5 mg
Ditropan packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Trusted 2.5 mg ditropan
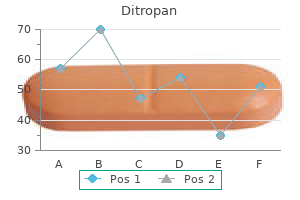
A small-gauge needle slows the speed of injection and reduces the speed and ache of tissue distention gastritis urination order 5 mg ditropan. A 10-mL syringe is really helpful both for its ease of handling and for the relatively gradual rate of injection that it allows gastritis diet 8 jam cheap ditropan 2.5 mg on line. Technique Once an agent has been chosen, proper administration technique minimizes pain, prevents unfold of micro organism, and avoids intravascular injection. Buffering, temperature manipulation, and cautious infiltration additionally scale back the pain of injection. Buffering Raising the pH of an anesthetic by adding sodium bicarbonate decreases pain dramatically, whereas decreasing the pH by adding epinephrine increases ache. Buffering is probably the best way to cut back the ache of native anesthetic injections, and its routine use is very beneficial. Sodium bicarbonate most likely works by growing the ratio of nonionized to ionized molecules, which both renders the ache receptors much less sensitive or causes extra fast diffusion of solution into the nerve and a shorter time to the onset of anesthesia. As the pH of the answer is raised, the anesthetic turns into unstable and has a decreased shelf life. It was initially recommended that buffered lidocaine be prepared just before use to avoid precipitation and degradation, however buffered lidocaine retains its effectiveness for 1 week and refrigeration might additional increase its shelf life. However, ache usually occurs with distention of tissue by the anesthetic, and hence injection should be slow and deliberate. B, If a wound is grossly contaminated, the anesthetic may be launched via the intact pores and skin. The needle is first launched at a degree consistent with the wound and past the wound edge (1), and whereas the anesthetic is slowly injected, the needle is superior to include one complete aspect of the wound (if possible) to some extent well past the other end of the wound. The different facet could also be anesthetized by passing the needle by way of the area already infiltrated by the primary injection (3) to make the pores and skin puncture painless. Some clinicians select to inject the anesthetic by way of intact pores and skin in patients with a grossly contaminated wound. Inject 1% lidocaine via intact pores and skin with the needle bevel dealing with upward as a result of that is less painful than injecting with the needle bevel dealing with downward. For infiltration anesthesia with a smallgauge needle, nonetheless, aspiration is normally pointless except the injection is deeper than the subcutaneous space or the area to be injected incorporates many massive vessels. Its recognition has waned considerably because of the fear (unproven and theoretical) of introducing an infection at the fracture web site and its limited efficacy. This technique is useful for reducing fractures of the distal finish of the forearm and hand. To perform the block, slowly inject 5 to 15 mL of plain 1% lidocaine into the fracture cavity and around the adjoining periosteum. A hematoma block is particularly helpful when a Bier block and basic anesthesia are contraindicated. Prepare the pores and skin over the fracture web site with antiseptic resolution and insert the needle into the hematoma, as confirmed by aspirating blood. Slowly inject 5 to 15 mL of plain 1% lidocaine or 5 to 10 mL of plain 2% lidocaine into the fracture cavity and across the adjacent periosteum. Adequate anesthesia happens in roughly 5 to 10 minutes and should last for a number of hours. The technique can provide aid for several conditions, primarily postthoracotomy pain, postcholecystectomy ache, and most significantly for emergency clinicians, posttraumatic chest pain. Several studies have demonstrated improved respiratory mechanics when intrapleural anesthesia is used. Angle the needle 30 to forty degrees with respect to the skin and purpose medially, with the bevel up and directed just above the rib. After perforating the posterior intercostal membrane (felt as a definite resistance), take away the stylet and connect a well-wetted, air-filled glass syringe to the Tuohy needle. Advance the needle until it enters the pleural space, which is denoted by the plunger being drawn down the syringe as a end result of the adverse stress created throughout inspiration. Remove the syringe and introduce an epidural catheter 5 to 6 cm into the pleural area. Remove the Tuohy needle, acquire a chest radiograph to affirm correct position, and safe the catheter. The level of anesthesia can prolong from T2 to T12 and involve the skin, chest, belly wall, and doubtlessly the viscera if the visceral afferent fibers are blocked on the sympathetic chain in the paravertebral gutter. Though not yet a constantly proven or a completely standardized method, intrapleural anesthesia presents promise for sufferers and is a useful process for the emergency clinician to master. Intraarticular Anesthesia and Analgesia Findings from the history and bodily examination of an acutely traumatized joint, such as the knee, usually underestimate the severity of the injury. Intraarticular anesthesia of the knee has no effect on gait sample or joint proprioception. Intraarticular anesthesia might improve elbow use after aspiration of a hemarthrosis associated with a radial head fracture. Intraarticular lidocaine has been efficient in facilitating discount of a shoulder dislocation. Animal experiments have demonstrated chondrotoxicity when native anesthetics are constantly infused into a joint. Morphine could additionally be injected immediately into joints for postoperative pain reduction and probably provide extended analgesia after discount of fractures. Theoretically, there are native opioid receptors in joints which would possibly be able to being stimulated by rather small doses of morphine to provide aid for up to 24 hours with a single dose. A interval of three to 6 hours may be required for analgesia to reach its maximum effect. In a systematic review, gupta and colleagues concluded that postoperative intraarticular morphine injected into the knee joint at doses of two to 4 mg offers analgesia for as much as 24 hours. Though studied primarily for postoperative use after knee surgery, an analogous concept may be intuitively applied to traumatic joint ache, but this has not been studied adequately. These effects, at doses properly below those used clinically, involve fibroblasts more than nervous tissue. Local anesthetics impair mitochondrial perform and fibroblast proliferation and hasten apoptosis in Intrapleural Anesthesia Indications Intrapleural anesthesia introduces a local anesthetic into the pleural area. Epinephrine added to 1% and 2% concentrations of lidocaine further reduced tensile strength, however when epinephrine was added to distilled water or to zero. Eriksson and associates107 found that lidocaine reduces the inflammatory response in wounds by reducing the number of white cells and their metabolic exercise. Although an inflammatory response may be beneficial in a contaminated wound, it can be detrimental in a sterile wound due to tissue toxicity created by the release of superoxide anions, lysosomal enzymes, thromboxanes, leukotrienes, and interleukins. None of the concerns mentioned earlier should prohibit using commonplace anesthetics or epinephrine when their use is otherwise indicated. Wound Infection Though not usually appreciated, it has long been known that local anesthetics possess antimicrobial activity in vitro. Lidocaine and procaine demonstrate concentration-dependent inhibition of tradition growth of most gram-negative organisms.
5 mg ditropan amex
D gastritis esophagitis 5 mg ditropan discount fast delivery, If the tube tract has matured (at least 2 weeks after placement) gastritis tratamiento generic ditropan 5 mg with amex, it could be eliminated by traction/countertraction. Significant force could additionally be required; be ready for a pop and splattering of gastric contents. Allow a minute for the balloon to deflate earlier than making another attempt at removing by traction. Large, nondeflating balloons ought to probably be punctured, whereas small balloons could additionally be eliminated with traction. Rigid or large inner mushrooms and bolsters, the very type that cause the most difficulty with percutaneous removing, are additionally more prone to trigger problem with rectal passage. In no case ought to a device be released into the intestine with an extended length of tubing attached. Remember that doublepart tubes might have an additional length of tubing for duodenal or jejunal feeding that extends far past the inside bolster. A bolster will stop migration of the tube, which might trigger gastric obstruction. Insert a hemostat by way of the holes in the new bolster and grasp the feeding tube. Surrounding scars may suggest that the tube is in fact an implanted jejunal tube, not a easy G tube. If the tape is replaced at residence, it could be placed under too much pressure and cause thinning of the belly wall at the stoma. Strong tape can even harm the tube throughout tape changes if it adheres too strongly to the tube. The editors of this text, and most clinicians, confirm position routinely with a contrast-enhanced radiograph, whereas others use the medical criteria outlined earlier. Routine use of postplacement contrastenhanced radiography to verify correct placement must be necessary when the tube tract is immature. The place of the G tube could also be checked by air insufflation and aspiration of gastric fluid, as is completed with nasoenteric tubes. Air should enter the abdomen with out resistance and should produce instant borborygmi. Good tube placement is indicated when more fluid returns with aspiration than was initially placed into the catheter. Correct tube placement is simple and readily verified radiographically with a small quantity of distinction materials handed into the tube. Inject 20 to 30 mL of water-soluble solution to document the intraluminal tube place. Take a supine abdominal film 1 to 2 minutes after instillation of dye to optimize visualization of the gut. With correct positioning, distinction material will define the a half of the gut containing the tube. An irregular or rounded blotch with wispy edges or streamers suggests peritoneal leakage. The tube had merely migrated distally (note the comparability of the new tube and positioning of the indwelling one) because the bolster was too far proximal. In most circumstances, passage of the tube was documented by sequential radiographs, with a mean interval of 24 days until passage (range, four to 181 days). Some clinicians and surgeons strongly condemn chopping off the tube on the skin, even when the dangers posed by the process are very low. Some clinicians tape tubes to the pores and skin quite than using a bolster, or use particular adhesive gadgets designed to control the tube and stop ingress, such as the Drain/Tube Attachment Device (Hollister, Inc. It was accomplished beneath fluoroscopic steering, always the most suitable choice in questionable circumstances. B, the stoma opening and direction of the tract could be investigated by gently probing the location and tract with a Q-tip; in this case, it simply entered the abdomen. D, To give a Foley catheter enough rigidity to assist in passage, the tip of a Q-tip was inserted in the side port of the distal end of the catheter, and traction was applied to the catheter. E, If a de Pezzer catheter is used, an endotracheal tube stylet distends the flange for passage, and the tip reforms as soon as within the abdomen. F, this affected person removed her recently changed feeding tube, with the balloon inflated, whereas still in the emergency division awaiting switch. Complications of gastrostomy embody wound infection across the catheter, performance of an pointless laparotomy for suspected leakage, gastrocolic fistula, pneumatosis cystoides intestinalis, bowel obstruction, peritonitis, and hemorrhage. Modest drive could also be required; be ready for a sudden pop and splattering of gastric contents. If wanted, this is a easy however much less secure approach for securing a gastrostomy tube to the skin. Gently pass a small needle alongside the course of the catheter whereas puncturing the balloon as many instances as needed. Note the encrusted condition of this long-standing Foley catheter used as a percutaneous endoscopic gastrostomy tube. C, Occasionally, the wire from a central line kit can clear the inflation lumen and permit deflation. D, If the valve mechanism malfunctions, reduce the catheter and attempt to drain the balloon by putting a needle in the inflation channel and flushing and withdrawing fluid. B, Note the free flow of contrast materials throughout the stomach, particularly outlining the liver (arrows). It is prudent to routinely get hold of a contrast-enhanced research after substitute of a percutaneous endoscopic gastrostomy tube in the emergency department. Note the outline of the gastric rugae and the characteristic mucosal folds of the small intestine. Uncooperative sufferers must be restrained and mittens are sometimes notably helpful. Local leakage of gastric juices could macerate and irritate the pores and skin, which might predispose the site to local infections and abscesses and encourage the event of small granulomas. Any dressing used across the entry web site of an enteral vitamin tube should absorb fluid and never encourage persistent moisture. Although insertion of a larger tube or firmer traction on the tube might be transiently efficient, these measures often end in further enlargement of the stoma. Insertion of a gentle, pliant feeding tube via the widened stoma is usually easy and permits later contraction of the stoma. Large quantities of drainage across the stoma site could happen with excessive residual volumes. Feeding residuals ought to be checked each four hours when a affected person is receiving continuousdrip feeding.
2.5 mg ditropan buy overnight delivery
However gastritis diet ��� ditropan 2.5 mg purchase online, the presence of postprocedural stomach ache gastritis diet ���� ditropan 2.5 mg buy online, fever, sustained or profuse rectal bleeding, or discharge warrants surgical consultation. B Balloon inflated distal to the foreign physique Similar process utilizing an anoscope and a Foley catheter. Patients might complain of ache on defecation, itching, incomplete evacuation, incontinence, or bloody mucosal discharge and mistake the situation for "hemorrhoids. The differential analysis includes hemorrhoids, polyps, cystocele, and carcinoma. Complete and partial prolapse could be distinguished from one another by digital palpation. To reduce the prolapse, place the affected person in the susceptible or lateral decubitus position. Tape the buttocks aside (or enlist the assistance of an assistant to unfold the buttocks) to aid in reduction. With partial or mucosal prolapse, radial rectal folds could also be seen protruding via the rectum. It often affects youngsters youthful than three years and is commonly related to cystic fibrosis, parasitic an infection, chronic diarrhea, malnutrition, or as a sequela of chronic neurologic disease. Prolapse is normally self-limited; outpatient administration (after handbook reduction) includes correcting constipation, avoiding straining, and referring for testing to exclude cystic fibrosis. Moreover, the possibility of lack of anal sphincter tone and incontinence increases with delays in reduction of rectal prolapse. Though showing trivial on examination, fissures could be extraordinarily painful, even hours after a bowel movement, due to persistent spasm. The situation is type of difficult to eradicate, is debilitating, and may final for months. Anal fissures are usually related to constipation, a tough or strained stool, or persistent diarrhea, but the precise trigger is unknown. The prognosis is relatively easy to make, and the fissure is readily seen by spreading the buttocks. The overwhelming majority of anal fissures happen in the posterior midline, 10% to 15% occur within the anterior midline, and fewer than 1% occur in lateral positions. Fissures occurring in atypical locations should immediate consideration of different ailments. Most sufferers with acute anal fissures and almost half of sufferers with chronic fissures will expertise therapeutic with medical therapy. Therapy is geared toward breaking the cycle of ache, spasm, and ischemia, elements thought to be answerable for the development of the fissure. Therapies embrace relaxation of the internal sphincter, establishment and upkeep of atraumatic passage of stool, and aid of ache. Definitive surgery may be tried, but occasional prolapses in debilitated sufferers are usually treated conservatively. Patients must be referred for outpatient proctoscopy to search for a polyp or malignancy that will have acted as a lead point. Procedure Reduce a mucosal prolapse by applying mild, constant strain on the mass for a couple of minutes. After discount, ship the kid house with a pressure dressing and stool softeners. Counsel the dad and mom on the usage of dietary fiber and increased fluid consumption to stop constipation and straining. Parenteral sedation should be provided if the patient is anxious or has issue stress-free the sphincteric muscles. Apply fixed, gentle circumferential pressure to the prolapsed space, starting with the portion closest to the lumen (the most distal segment). Place the thumbs on either side of the lumen whereas greedy the outside walls with the fingers. Apply stress with the thumbs while rolling the partitions inward to pressure the prolapse again by way of the anus. If substantial tissue edema has developed, software of gauze soaked in sugar water might promote shrinkage and subsequent guide reduction. Although some topical preparations could additionally be helpful (see text), these lesions are painful and difficult to heal. Botulinum toxin causes momentary muscle paralysis by stopping the discharge of acetylcholine from presynaptic nerve terminals, thereby lowering stress within the inside sphincter. Surgical remedy is usually reserved for fissures that have failed medical remedy and is usually healing. This chapter reviews basic prehospital immobilization strategies and equipment, together with spinal movement restriction, pelvic stabilization, extremity splinting, and removal of protective tools. During the Nineteen Eighties and 1990s, indications for spinal immobilization were based primarily on the mechanism of injury, regardless of the presence or absence of signs or physical findings suggestive of a spinal injury. The authors concluded that out-of-hospital immobilization has little or no impact on neurologic end result in sufferers with blunt spinal accidents. Nevertheless, obtainable knowledge suggests that we should always cut back or get rid of routine prehospital spinal immobilization in favor of using validated scientific guidelines to decide which patients might have sustained a spinal column damage and making use of spinal motion restriction strategies only to these patients. Until then, emergency physicians have to be educated about prehospital spinal immobilization. Therefore the remainder of this part offers an in depth evaluate of immobilization devices and techniques. Furthermore, the backboard can lower tissue perfusion at pressure points, resulting in the event of strain ulcers. Generally speaking, the fundamental forces that could be exerted on the backbone are flexion, extension, rotation, lateral bending, distraction (stretching), and compression (axial loading). For instance, high-speed rollover motor vehicle collisions might easily exert all of the aforementioned forces. A common state of affairs for this type of damage is an elderly woman who falls from a standing top. In addition, the free space between the thoracic spinal twine and the borders of the spinal canal is relatively small, and the blood supply is less strong. These elements increase the susceptibility of the spinal cord to accidents at this level. Disk dimension and form also change, thus making this part of the backbone notably vulnerable to damage. There can also be a better prevalence of compression and burst fractures within the lumbar backbone. These fractures commonly happen when axial loading forces straighten the natural lordosis in the meanwhile of impression. Such fractures are often caused by direct trauma or falls from a peak, or happen as a outcome of sacral insufficiency secondary to osteopenia, persistent steroid use, or earlier pelvic irradiation.
Buy ditropan 5 mg amex
Even if all foreign materials has been eliminated gastritis diet zucchini ditropan 5 mg order otc, stings from marine animals may initiate a prolonged native irritation that simulates cellulitis gastritis yeast infection purchase ditropan 5 mg free shipping. B, After contact with the pores and skin, a dartlike tail is extended and penetrates the dermis, and C, venom is injected. Further stimulation of the hooked up nematocyst can expel more venom (see text for the decontamination and elimination technique). Other advised, but unproven, treatments embody meat tenderizer, ammonia, baking soda, urine, olive oil, sugar, and papaya latex. To take away the remaining nematocysts, scrape the pores and skin with a hard edge, similar to a bank card held perpendicular to the skin. An alternative is to apply shaving cream and shave the world gently to remove the remaining fragments. If the ache persists, it must be assumed that organelles still stay and further cleansing is required. The application of heat or chilly packs to the realm has not been proven to reduce pain. In abstract, a 2013 Cochrane evaluation found inconclusive evidence defining the most effective therapy for jellyfish envenomation, but a 2016 article advised a quantity of interventions could additionally be efficient for nemocyst inhibition. These authors wrote that topical vinegar for no less than 30 seconds for some species whereas seawater, baking soda slurry and water warmed to 42�C to 45�C can help, along with oral analgesics. Fire coral, a specific kind of coral, is one other type of coelenterate that produces toxicity with stinging nematocysts. After contact, a burning and intense pruritus might happen along with a collection of skin eruptions. Within minutes of contact, pruritus, erythema, and urticaria-like lesions may seem, and blister formation could result within hours. Eventually, the lesions will become lichenoid, however full resolution may not happen for 15 weeks after contact. Immediate care with oral antihistamines and topical steroids tends to scale back, however not stop, the symptoms. With these wounds, delayed therapeutic may happen with the secondary growth of cellulitis or ulceration, maybe because of contamination of the wound with bacteria or microparticles of coral. Hydrogen peroxide could additionally be used to help take away small coral particles from the wound. Reactions may be native or systemic, and the pain may be extreme and is often described as "shocklike," "itching," "burning," or "throbbing. Systemic reactions normally encompass fever, chills, and muscle spasm, but extreme reactions might result in neurologic sequelae ranging from malaise and headache to paralysis and coma. Potential cardiopulmonary manifestations embrace dysrhythmias, hypotension, syncope, bronchospasm, laryngeal edema, and cardiorespiratory failure. Sea Urchins and Starfish Sea urchins and starfish are free-living echinoderms covered with venomous, sharp, brittle spines and with venom-secreting pincers located close to the mouth. If sea urchins or starfish are dealt with or inadvertently stepped on, these spines might turn into embedded within the patient and a extreme native reaction could end result from venom in the spines. Systemic signs happen and embrace muscle weak point; paralysis of the lips, tongue, and face; hypotension; abdominal ache; and respiratory distress. Echinoderm spines might discharge a purple dye that may be mistaken for a retained backbone. If spines are positioned in a joint or close to a nerve, surgical extraction utilizing an operative microscope could additionally be needed. If acceptable, open the wound and drain it to allow it to close by secondary intention. This is believed to present relief of signs by reducing vascular and muscle spasm. Lack of discoloration indicates absorption of dye from the ocean urchin spines and probable absence of retained fragments. Some authors suggest empirical antibiotic remedy to cover gram-negative bacilli. This causes the stingray to lash out its whiplike caudal appendage, or tail, which accommodates one to 4 venom-containing serrated spines. Each backbone is roofed with a sheath containing venom glands, and along with immediate toxin-induced ache, items of the spine or sheath might stay embedded in the wound. Immediate local and systemic reactions develop because of injection of a fancy toxin. Systemic reactions may be severe and may embody muscle cramps, vomiting, seizures, hypotension, arrhythmias, and (rarely) demise. Local digital blocks with out vasoconstrictors present efficient analgesia for hand wounds. Explore and d�bride all wounds, and remove all remnants of the spine and integumentary sheath. The venom could cause important native tissue necrosis, and surgical d�bridement may be required. Unlike different gentle tissue infections, marine injuries turn out to be contaminated with uncommon gram-negative organisms, particularly Vibrio species. Although few studies have evaluated the results of particular antibiotics, it is strongly recommended that quinolones, trimethoprim-sulfamethoxazole, tetracyclines, third-generation cephalosporins, or aminoglycosides be used in lieu of penicillin, ampicillin, erythromycin, or first-generation cephalosporins. B, An unsuspecting sufferer steps on the stingray, and the whiplike tail impales the foot (even through a heavy boot) with a number of spines. C, the spine has backward-facing barbs coated by a sheath with venom-containing cells, which causes a toxic envenomation and the potential for a quantity of international our bodies. Tetanus and Antibiotic Therapy true infection, and surgical exploration is often required in persistent cases. A, To take away them, professional facial gel is unfold with a fan brush, thin at the edges. Deeply embedded cactus spines generally produce granulomatous reactions, however infections are rare. Hence, make an effort to remove deeply embedded spines after rigorously weighing the profit and potential harm related to deep exploration, particularly in a delicate location. Ring Removal Frequently, a hoop should be eliminated to stop laceration of tissue or vascular compromise. However, the stringwrap technique or physically cutting the ring off could additionally be necessary. Preferably, take away all rings before the edema is intensive enough to cause ache or vascular compromise. An occasional patient can stay calm during this process, but if the swelling is important or the digit has been traumatized, anesthesia is important. Perform a proximal digital or metacarpal block to present sufficient anesthesia and to minimize tissue distention on the ring site. Before elimination of the ring, wrap a large Penrose drain circumferentially in a distal-toproximal direction to cut back the delicate tissue swelling. Some nonanesthetized patients panic through the procedure due to growing ache from compression and unwinding. Shorter lengths are discouraged as a end result of one could have to repeat the wrapping procedure halfway.
Best 5 mg ditropan
Splinting and follow-up in a couple of days are prudent primarily based on the injury mechanism and location gastritis diet 7 up cake ditropan 2.5 mg discount overnight delivery. C gastritis ulcer diet 2.5 mg ditropan cheap mastercard, the flexor digitorum profundus tendon is examined by immobilizing the digit in question and asking the patient to flex the distal interphalangeal joint towards resistance. D, the flexor digitorum superficialis tendon is examined by immobilizing the digits not being tested and asking the affected person to flex the proximal interphalangeal joint in opposition to resistance. Pain and weak spot related to flexion against resistance could suggest a partial tendon laceration, but this is typically a very delicate or inaccurate evaluation that must be repeated when the pain and swelling have subsided. Point-of-care ultrasound has emerged as a helpful gizmo to diagnose each complete and partial tendon ruptures. The sensitivity and specificity of ultrasound for Achilles tendon rupture, as reported within the radiology literature, are 96% to 100% and 83% to 100%, respectively. A defect within the Achilles tendon may be appreciated in some circumstances of Achilles tendon rupture, but not on this case. The Achilles tendon is assessed, proximally to distally, for synchronous motion, utilizing dynamic sonography during passive dorsiflexion and plantar flexion of the ankle with the probe over the realm of interest. Splinting the foot in mild plantar flexion (gravity equinus) can shield the tendon till follow-up in 1 to 5 days. Both the quadriceps and patellar tendons are subject to rupture, and the condition happens predominantly in males. Quadriceps tendon rupture is extra widespread in the elderly and in these with systemic degenerative illness, arthritis, and steroid use, and is associated with important morbidity no matter treatment. It can also be seen in youthful patients, corresponding to after taking a basketball leap shot. Patellar tendon rupture is also a severe harm but occurs more generally in healthy sufferers, youthful than 40 years, participating in sporting occasions. The trauma could also be seemingly minor, similar to missing a step or jumping from a low peak. An apparent suprapatellar soft tissue defect and an incapability to perform a straight-leg increase while supine made the prognosis of an entire quadriceps tendon rupture obvious. Diffuse soft tissue swelling, bilateral knee effusions, normal radiographic findings, and the ability to stroll with bilateral knee immobilizers delayed the prognosis of bilateral quadriceps tendon rupture until follow-up. C, A step-off above the knee readily identified an entire quadriceps tendon rupture. The affected person was unable to lift the leg off the stretcher, an exercise that made the gentle tissue defect obvious. Quadriceps tendon rupture normally occurs transversely, just proximal to the patellar insertion, with or without an avulsion fracture of the superior pole of the patella. The mechanism of patellar tendon rupture is often an extreme load on the flexed knee throughout athletic activities. Bilateral full rupture has been described, but the situation is mostly unilateral. With either kind of rupture, a large hemarthrosis is usually produced and sometimes prompts the incorrect prognosis of a ligamentous injury corresponding to an anterior cruciate ligament rupture. A palpable defect superior or inferior to the patella could also be appreciated, however diffuse swelling can mask this finding. Lack of the anticipated defect may be misleading in the presence of a large hemarthrosis. When the historical past consists of only minor trauma, and the findings on bodily examination are subtle, the provider could incorrectly suspect malingering or noncooperation with the examination. With complete rupture, a supine patient is unable to actively lengthen the knee or raise a straightened leg off the stretcher, and the knee flexes when posterior thigh help is removed from the raised leg. Weak extension, particularly within the sitting position, could also be possible if portions of the medial and lateral retinaculae are intact, even with a whole rupture of the central rectus femoris. As one would intuit, however, a knee immobilizer allows the patient to apparently walk normally. Partial tears might allow the patient to stroll with a peculiar forward-leaning gait that helps help the knee in extension. With quadriceps tendon ruptures, a low-riding patella (patella baja) could additionally be current because the patella falls inferiorly. Conversely, a high-riding patella (patella alta) is usually seen with patella tendon ruptures as the quadriceps tendon and patella retract superiorly. The use of dynamic ultrasound will reveal the separated tendon ends shifting away from each other with intervening echogenic or echolucent fluid. Complete tears require surgical restore, usually as quickly as attainable after the diagnosis is made. Blaivas M, Lyon M, Brannam L, et al: Water bathtub analysis approach for emergency ultrasound of painful superficial constructions. Broder J, Jerrard D, Olshaker J, et al: Low risk of an infection in chosen human bites handled without antibiotics. Paavola M, Paakkala T, kannus P, et al: Ultrasonography in the differential diagnosis of Achilles tendon injuries and related problems. Ufberg fast aid of affected person discomfort and facilitates repetitive dosing for titration to the specified effect (see Chapter 33). Alternatives to procedural sedation and analgesia include intraarticular injection of local anesthetics, hematoma blocks, peripheral nerve blocks, and regional anesthesia (see Chapters 29, 31, and 32). This is most essential for hip, knee, and posterior sternoclavicular dislocations. For all dislocations, perform a detailed neurovascular examination of the extremity earlier than focusing consideration on the injured joint. Although many dislocations are clinically apparent, some could escape detection for some time as other injuries or points dominate the medical image. A knee dislocation may be quite apparent in a 170-lb man who shows a deformity of the knee, but in a 400-lb affected person, the knee might look deceivingly normal on first glance. The history and mechanism of injury may be fairly useful in certain circumstances. For instance, a painful shoulder joint in a seizure patient ought to prompt evaluation for a posterior shoulder dislocation, whereas a history of the knee putting the dashboard is a clue to a possible hip dislocation. Carpal dislocations within the wrist may be delicate, however are clinically suggested by extreme pain and swelling. Similarly, superior dislocation of the patella could also be mistaken for high riding patella typical of patellar tendon rupture. Unlike anterior shoulder dislocations, which are sometimes simply detected on plain movies, posterior shoulder dislocations may be missed on preliminary radiographs. A cautious history will uncover these accidents and prompt the necessary assessment of the ligamentous integrity and the potential for an related vascular injury and guide proper immobilization and follow-up care.
Ditropan 5 mg generic with mastercard
Seizures are typically not recurrent and are treated with oxygen and anticonvulsant drugs gastritis diet natural ditropan 5 mg cheap without prescription. Transient cardiovascular reactions gastritis vitamin d deficiency ditropan 5 mg cheap without a prescription, corresponding to bradycardia and hypotension, are attainable with giant doses of lidocaine. One case of cardiac arrest 15 seconds after the use of 200 mg lidocaine has been reported, but the precise medical state of affairs may have been a vasovagal reaction quite than a real cardiac arrest. Bupivacaine offers no profit over lidocaine, has been associated with deaths, and should be prevented. In addition, some leakage of anesthetic can occur after the infusion needle has been removed. Both problems might end in poor anesthesia but could additionally be minimized if a small, well-secured plastic infusion needle is used as a substitute of a metallic scalp vein ("butterfly") needle and if the puncture web site is tightly taped after withdrawal of the catheter. It should be used with caution till the ischemic impact of the tourniquet on the red blood cells of such sufferers has been clarified. Anesthetic Agent Serious issues seldom occur if correct consideration is paid to approach. Other reactions to lidocaine are uncommon and are normally systemic reactions from excessive blood levels. Auroy Y, Narchi P, Messiah A, et al: Serious issues associated to regional anesthesia: results of a prospective survey in France. Emergency clinicians must make sure that all sufferers obtain ache relief and sedation commensurate with their particular person wants throughout any procedure. Though historically well-liked, the extensively misinterpreted and misused time period "conscious sedation" has fallen into disfavor12; it has been labeled as "complicated,"thirteen "imprecise,"12 and an "oxymoron"12,13 and has been changed with the time period "reasonable sedation. Levels of responsiveness stay at finest crude surrogate markers of respiratory drive and retention of protecting airway reflexes. Data are currently insufficient to determine whether or not deep sedation is related to impairment of protecting reflexes or whether such hazard is encountered solely when "pushing" deep sedation to the point at which it approaches or reaches general anesthesia. These hospital-wide sedation insurance policies will differ from site to site based mostly on the specific wants and expertise available inside each establishment. In 2001, the Joint Commission launched new standards for ache management, sedation, and anesthesia care. Low doses of opioids or benzodiazepines induce gentle analgesia or sedation, respectively, with little danger of antagonistic occasions. If, nonetheless, clinicians proceed administering extra medicine past this initial stage, progressively altered consciousness ensues with a proportionately increased danger for respiratory and airway complications. If further medications are administered, the affected person will advance along this continuum till protecting airway reflexes are lost and basic anesthesia is finally reached. An altered mental state could additionally be a secondary impact of medicines administered for this function. Although cognitive perform and coordination may be impaired, ventilatory and cardiovascular function is unaffected. Patients incessantly want help in maintaining a patent airway, and positive strain ventilation could also be required due to depressed spontaneous air flow or drug-induced melancholy of neuromuscular operate. Unduly restrictive policies do a disservice to patients by discouraging appropriate levels of analgesia and sedation. Most hospitals pattern their sedation insurance policies after the Joint Commission standards and definitions. Deep sedation can facilitate such procedures, but with greater danger for cardiorespiratory melancholy than is the case with average sedation. Moderate sedation is frequently insufficient for effective anxiolysis and immobilization in younger, frightened kids, and deep or dissociative sedation is an acceptable different. Health care institutions wishing to bill Medicare should adhere to these tips and provide supporting documentation when requested. Therefore these practitioners are uniquely qualified to present all ranges of analgesia/sedation and anesthesia (moderate to deep to general). If this analysis suggests further risk, rethink the advisability of sedation. High-risk circumstances could additionally be higher managed within the extra managed surroundings of the operating room. Presedation evaluation is a Joint Commission requirement, and most hospitals have developed specific forms to facilitate consistent documentation of the required objects. Consider assessments corresponding to Mallampati scoring or the gap between the chin and hyoid bone (see Chapter four;. Cardiovascular Perform cardiac auscultation to assess for disturbances in rhythm or different abnormalities. Respiratory Perform lung auscultation to assess for active pulmonary disease, especially obstructive lung disease and higher respiratory infections which will predispose the patient to airway reactivity. Gastrointestinal Assess the time and nature of the last oral intake as a result of pulmonary aspiration of gastric contents might occur if the affected person vomits when protecting airway reflexes are impaired. Though uncommon, there may be events during which nonfasting patients require urgent procedures with a substantial depth of sedation that could be extra safely managed within the working room with endotracheal intubation to defend the airway. Selecting agents which are less more likely to produce vomiting, similar to fentanyl as a substitute of morphine or meperidine, could decrease the potential for aspiration. Higher-risk sufferers are those with a quantity of of the following present to a degree individually or cumulatively judged clinically necessary by the treating clinician: � Potential for difficult or prolonged assisted ventilation ought to an airway complication develop. If the affected person is breathing room air (21% oxygen), pulse oximetry will detect a lower in alveolar ventilation somewhat quickly. With preoxygenation or the continued use of supplemental oxygenation throughout a procedure, the heart beat oximetry will take considerably longer to drop despite the entire absence of air flow. With preoxygenation it could take 4 to 5 minutes of apnea before the coronary heart beat oximetry will drop considerably. Such careful observation permits immediate detection of opposed events such as respiratory depression, apnea, partial airway obstruction, emesis, and hypersalivation. They have to be proficient in sustaining airway patency and assisting air flow if wanted. The clinician usually oversees drug administration and performs the procedure, whereas the nurse or respiratory therapist constantly monitors the patient for potential complications. The nurse or respiratory therapist should also document the medications administered and the response to sedation and measure very important signs periodically. During deep sedation, the person dedicated to patient monitoring ought to have expertise with this depth of sedation and no other duties that may interfere with the superior degree of monitoring and documentation acceptable for this diploma of sedation. This is more accurate than impedance-based respiratory monitoring, especially in patients with obstructive apnea or laryngospasm, in whom impedance-based monitoring will interpret chest wall motion with out ventilation as a valid breath. Moreover, several additional research have demonstrated that the usage of capnography reduces the incidence of hypoxic occasions in each children47 and adults. Apply supplemental oxygen, particularly for patients undergoing deep sedation with agents such as propofol. In addition to pulse oximetry, observe the rise and fall of the chest, for the earliest indication of apnea. Ideally, capnography ought to be used in all situations during which high-flow oxygen is run. Before discharge, be sure that the patient is alert and oriented with steady important signs.
Diseases
- Gougerot Blum syndrome
- Sirenomelia
- Cerebral palsy
- Bradykinesia
- Generalized torsion dystonia
- King Denborough syndrome
- Gingival fibrosis
- Molluscum contagiosum
- Posterior valve urethra
- Leukomalacia
Buy ditropan 5 mg mastercard
However lymphocytic gastritis symptoms treatment 5 mg ditropan order otc, present studies show that the height of autologous donations represented less than 2% of the total blood collections and this quantity is declining gastritis onions generic 5 mg ditropan amex. Because blood may be stored for as much as 35 days, donations normally start 5 weeks before wanted. The blood donor will require iron dietary supplements and should keep a hemoglobin stage larger than eleven g/dL. Perfluorocarbons are completely artificial, essentially limitless in supply, chemically steady, and harbor no risk for an infection. Trials to date have centered primarily on their adjunctive use with normal transfusion therapy. A abstract of the dosages and traits of every component is provided in Table 28. Platelet Concentrates Platelet concentrates are ready by fast centrifugation of platelet-rich plasma. Platelets are obtained by single-donor apheresis or from pooled random-donor whole blood models. Platelets obtained by single-donor apheresis have the advantage of exposing the recipient to only one donor. This reduces the danger for exposure to many different donors and confers a lower threat for transfusion-transmitted disease and other problems. Platelet concentrates contain most of the platelets from 1 unit of blood in 30 to 50 mL of plasma. Fresh frozen plasma 15 mL/kg or 1000 mL or 4 items in a 70-kg affected person Each unit raises all coagulation elements by 2%�3% in averagesized adults. Cryoprecipitate 10�20 bags, depending on the indication With fibrinolytic-induced bleeding, recommended doses might help correct bleeding. A 4- to 6-pack of random-donor items delivers approximately the same amount of platelets as a single-donor apheresis unit. It is important to turn out to be acquainted with the blood financial institution terminology at your hospital. For this discussion, the time period unit is used to describe individual models and not a 4- or 6-pack. One individual unit of random-donor platelet concentrate raises the platelet rely by 5000 to 10,000/mm3. In a mean grownup, this works out as approximately 6 to 8 items of platelet focus. Assuming a zero platelet level, 6 items (or one 6-pack) or one single-donor apheresis unit given to a normal-sized grownup should increase the platelet rely to roughly 50,000/mm3. In cases of severe platelet consumption, transfusion could additionally be required each 6 to 24 hours. Some hospital blood banks prepare platelet concentrates frequently; in some cities a central blood bank service, such as the American Red Cross, prepares platelet concentrates frequently and delivers units on an as-needed basis inside 1 to 2 hours of the request. Platelet concentrates are viable for five days when stored at room temperature and gently agitated at intermittent intervals or when kept in motion. Spontaneous bleeding hardly ever happens if the platelet count is larger than 10,000 to 20,000/mm3. Even within the occasion of surgical procedure or trauma, excessive bleeding is rare in patients whose platelet depend exceeds 50,000/mm3. It is usually beneficial that active hemorrhage be treated by platelet transfusion if the platelet rely is lower than 50,000/ mm3, however prophylactic transfusion may be withheld safely till the depend is decrease than 20,000/mm3, and more recent data recommend that this threshold could be lowered to lower than 10,000 and even 5000/mm3. Because of the presence of antiplatelet antibodies in these patients, transfused platelets may last only a quick while (minutes to hours) before being faraway from the circulation. Laboratory affirmation includes the identification of intravascular hemolysis on a peripheral blood smear. In this examine, the administration of a larger quantity of platelets (up to 10 random-donor units) was in a place to reverse a few of the antiplatelet effects of this three-drug combination. Most institutions have a coverage that limits the quantity of incompatible platelets that can be given. When greater than 10 units of blood are transfused, the platelet count should be routinely evaluated and platelets must be changed accordingly. Clinically significant platelet depletion not often occurs if less than 15 units of blood (or 1. Platelets could also be infused rapidly (1 unit/10 min) with the use of specialized platelet filters. However, pathologic hemorrhage after huge transfusions is usually brought on by thrombocytopenia quite than by a depletion of clotting components. It is believed to be an immune-mediated process and may occur in as a lot as 1 in 5000 transfusions containing plasma. The quantity of cryoprecipitate required to right coagulation defects ranges from 10 to 20 units/kg for minor bleeding, such as hemarthrosis, to 50 units/kg for management of bleeding in surgical procedure or trauma. The giant variety of items that should be given increases the chance of exposure to blood-borne illnesses. Cryoprecipitate could also be required to right vital hypofibrinogenemia (<100 mg/dL). A typical adult dose of approximately 10 luggage of cryoprecipitate raises the fibrinogen stage by up to 1 g/L (60 to one hundred mg/dL). In instances of severe bleeding after the utilization of a fibrinolytic agent such as tissue plasminogen activator, cryoprecipitate can be utilized to assist management the bleeding. A consensus on dosing has not been reached, however many sources recommend between 10 and 12 luggage. It works by binding to the floor of activated platelets, which then activate factor X by utilizing the tissue factor pathway (formerly known as the extrinsic pathway). Activated issue X then complexes with issue Va, which leads to thrombin burst and clot formation. At an average cost per dose of $5000 (80 �g/kg), this can be a limiting issue, especially when some studies use protocols consisting of eight sequential doses. Study dosages in these patients have been generally larger than for off-label use (100 to 300 �g), however the drug was effective in controlling bleeding episodes, with an acceptably low rate of thromboembolic events. The threat for hemorrhage expansion inside the first 24 hours is between 20% and 40% in these sufferers. The threat of hematoma growth is doubled in patients on vitamin K antagonists (warfarin). Interestingly, no single technique to reverse warfarin has been conclusively proven to improve clinical outcome better than any other technique. The major outcome measured was the whole transfusion requirement and subgroup analysis was carried out for blunt and penetrating trauma.
Order 5 mg ditropan mastercard
C gastritis diet nuts 5 mg ditropan discount mastercard, this intravenous drug consumer had an "abscess" of the chest wall drained in various emergency departments a quantity of times over a 2-month interval gastritis symptoms vs. heart attack ditropan 5 mg buy with mastercard, and it seemed to initially respond to drainage and antibiotics. He nonetheless had an space of cellulitis, minor fluctuance, and continued drainage close to the center of the chest. Magnetic resonance imaging demonstrated osteomyelitis and an abscess of the sternoclavicular joint that was draining to the pores and skin and simulating a recurrent cutaneous abscess. D, this affected person underwent a sternotomy for bypass surgery a couple of months beforehand. She had been handled sporadically for a minor wound infection, but then a draining fluctuant mass developed on the inferior border of the sternum. The spread of this organism is taken into account an epidemic and it is extremely virulent and aggressive. Panton-Valentine leukocidin enhances tissue necrosis, and phenol-soluble modulin is poisonous to neutrophils. B, the characteristic circular skin lesion from "skin popping" discovered on the arms (arrows) confirmed the medical suspicion. Even though a drug display was optimistic for opioids, the affected person denied drug use and attributed the leg lesions to frequent trauma on the job. Drug customers with abscesses are in danger for quite a few infections, together with mind abscess, endocarditis, and occult osteomyelitis. The patient incessantly describes a small pustule that becomes an abscess in 24 to 48 hours. More recently, community-acquired infections have occurred more frequently, even in individuals with out recognized threat elements. Such lesions are sometimes mistaken for a spider bite or drug use due to their fast progression and seemingly spontaneous onset in an otherwise wholesome individual. However, these organisms fortunately are likely to be susceptible to a broader array of antibiotics. It is usually associated with skin and soft tissue infections in young, otherwise healthy individuals. The presence of a fluctuant mass in an space of induration, erythema, and tenderness is clinical proof that an abscess exists. An abscess might appear initially as a particular, tender, delicate tissue mass, but in some instances a distinct abscess is most likely not readily evident. If the abscess is deep, as is true of many perirectal, pilonidal, and breast abscesses, the clinician may be misled by the presence of a firm, tender, indurated space without a definite mass. If the findings on bodily examination are equivocal, needle aspiration or ultrasound examination may be performed to assist within the diagnosis. Parenteral injection of illicit medication can produce simple cutaneous abscesses that unpredictably advance to extensive necrotizing delicate tissue infections. The emergency clinician should keep a high index of suspicion to avoid missing this probably life-threatening condition. In most instances, a formal I&D procedure shall be essential to successfully manage the situation, despite the precise fact that copious drainage will not be encountered. Although no formal drainage may be required after the spontaneous rupture of a easy cutaneous abscess, conditions similar to a perirectal abscess, Bartholin gland abscess, and breast abscess are usually finest managed with additional applicable drainage and packing. For ultrasound-guided drainage of a cutaneous abscess, use a high-resolution probe (7. Place the sterile transducer over the main body of the abscess and insert the needle via the skin adjoining to the transducer. Adjust their relative relationships consistent with the depth and placement of the abscess cavity. Scan the entire space of the suspected abscess and beyond to capture unexpected extensions of the abscess. Traditionally, culturing the contents of a readily drainable cutaneous abscess was not indicated, nor commonplace. It merely supplied no further helpful data to the clinician beneath most circumstances. Culture may also permit identification of antibiotic susceptibility and assist in customization of antibiotic therapy. Cohort results also provide a framework for local epidemiology and resistance patterns. This data could probably be helpful if the patient responds poorly to initial surgical drainage, if secondary spread of the an infection occurs, or if bacteremia develops. However, the degree of surrounding cellulitis qualifying as "extensive" is ill outlined. When obtaining a specimen for tradition, essentially the most correct and full tradition outcomes might be obtained if one aspirates pus with a needle and syringe earlier than I&D. Most clinicians, nonetheless, still culture free-flowing purulent material obtained with a cotton swab throughout I&D. A "sterile" tradition from a specimen collected with a regular cotton swab after incision is regularly the outcomes of improper anaerobic tradition technique. This foul odor is actually attributable to the presence of anaerobes; the pus associated with E. The discovery of solid or suspicious materials in an abscess ought to immediate histologic evaluation as a end result of a malignancy might mimic cutaneous abscesses. An abscess could produce leukocytosis, depending on the severity and duration of the purulent process; however, the presence or absence of leukocytosis has just about no diagnostic or therapeutic implications. Bacteremia could occasionally be manifested as a peripheral abscess resulting from septic emboli, and it often produces medical traits dissimilar to these related to easy cutaneous abscesses. Gram stain is neither indicated nor commonplace within the care of uncomplicated simple abscesses. However, patients who seem "toxic" or immunocompromised and these that require prophylactic antibiotics (see the part on Prophylactic Antibiotics later on this chapter) might benefit from Gram stain in addition to cultures. Gram stain outcomes have been proven to correlate properly with subsequent tradition outcomes, so in compromised hosts the test can be used to direct the selection of antibiotic remedy. Anaerobic infections should be suspected when multiple organisms are noted on Gram stain, when a foul odor is associated with the purulence, when free air is famous on radiographs of the delicate tissue, and when no progress is reported on cultures. A recent examine from Academic Emergency Medicine by Tayal and colleagues evaluated the impact of soppy tissue ultrasound on the administration of cellulitis within the emergency department. Peritonsillar abscesses are tough to diagnose from the bodily examination alone, and some clinicians might feel hesitant to try blind drainage. Ultrasound of suspected peritonsillar abscesses has been discovered to be reliable in making the analysis. The general dimension of the abscess, in addition to its proximity to the carotid artery, may be evaluated with ultrasound, which can maybe enhance the arrogance of the clinician in attempting drainage. When a significant amount of edema is current throughout the tissue, bands of hypoechoic (dark gray) or anechoic (black) fluid may be seen inside the space of thickened tissue. Cobblestoning seems as thin bands of fluid throughout the tissue and may be distinguished from an abscess by the dearth of a discrete fluid collection. Abscess An abscess is seen as a focal, discrete fluid collection within an area of cellulitis. The presence of surrounding cellulitis is the key to distinguishing an abscess from other fluid collections corresponding to cysts.
Discount 2.5 mg ditropan with mastercard
Instruct sufferers to put on much less constricting footwear and to trim the nail straight across gastritis diet quick generic 2.5 mg ditropan amex. Diabetic patients and those with peripheral vascular illness require closer follow-up gastritis diet treatment 2.5 mg ditropan cheap free shipping. When the ingrown toenail is caused by a nail deformity, a podiatrist or main clinician can carry out definitive removal during follow-up evaluation. Toenail Removal for Complex or Extensive Ingrown Toenails When irritation, infection, or both are more widespread or embody the entire toe, removal of a portion of the nail and d�bridement of the infected tissue may be required. B, An oblique wedge of nail is trimmed from the lateral margin of the nail to free it from the hyperkeratotic area. First separate the nail from the nail mattress by advancing and separating scissors held parallel to the nail mattress. Cover the wound with antibiotic ointment, a nonadherent dressing, and a dry sterile wrap. Antibiotics efficient towards gram-positive organisms are prescribed for significant related infection but are probably not required for this localized process. Partial nail removing accomplishes two things: elimination of the offending portion of nail and destruction of the underlying nail matrix to forestall regrowth of the nail. Phenol, probably the most commonly utilized chemical, causes neurolysis of the nerve endings and necrosis of the nail matrix in a process referred to as matricectomy. Several research have demonstrated that 10% sodium hydroxide resolution is as efficient as phenol and may be associated with less postprocedural pain and faster restoration. After a digital block, exsanguinate the toe by squeezing or wrapping, and apply a tourniquet on the base of the toe. Separate the lateral third of the nail from the nail bed by advancing and separating scissors held parallel to the nail mattress. Arrow identifies the method described in the figure concerning placing the phenol soaked applicator under the eponychium. An English anvil nail splitter is desirable to begin the process, but sharp scissors or a No. Take care to perform a managed division along the longitudinal strains of the nail for several millimeters past the proximal nail fold (cuticle). Inspect the remnant to make sure that the entire piece of nail has been removed as desired. Sharply take away any remaining or swollen/heaped-up skin and all hyperkeratotic particles. After removal of the nail, most clinicians apply a silver nitrate stick with the nail bed and to granulation tissue for two to 3 minutes. Apply a 10% sodium hydroxide resolution to the nail mattress with a cottontipped applicator for 1 to 2 minutes to present efficient ablation of the nail matrix. A 1% phenol solution could be ready by diluting a 70% to 90% aqueous phenol solution in an eighty: 1 ratio. Granulation tissue is curetted (B and C), and the nail matrix is cauterized with hydrogen peroxide or phenol (D) (see text). B Insert a chunk of small tubing break up lengthwise proximally along the lateral nail edge until the nail edge and nail spicule are encircled by the tube. Apply totally moistened (but not saturated) applicators for 3 30-second functions. Avoid forcing phenol under the remaining nail by rolling the applicator so that it rolls over the matrix and over the nail surface quite than in opposition to the cut up edge of the nail. Thoroughly irrigate the cauterized nail bed with water and rub the realm with a gloved finger to remove all traces of phenol. Apply antibiotic ointment (not containing neomycin) and a nonadherent dressing to the wound, adopted by a dry sterile wrap. Instruct the affected person to wash the wound twice day by day adopted by dry dressing changes. The wound will heal in 2 to 4 weeks and could also be accompanied by serous drainage for 2 weeks. Complications embrace nail regrowth, an infection, development of an inclusion cyst, or delayed therapeutic. If the condition returns, podiatric referral is recommended for more in depth ablation of the nail mattress. Nail-Splinting Technique Splinting of the nail spicule on the lateral edge of the affected nail may allow the toenail to grow out without affecting the infected gentle tissue. This technique supplies time for the periungual tissue to heal while the nail continues to develop till it could be trimmed straight across. When the diploma of irritation is minimal, elevation of the nail spicule is definitely accomplished with forceps or a hemostat. A cotton pledget inserted beneath the lateral edge to keep elevation is commonly sufficient in minor cases. Alternatively, a wound closure strip can be used to elevate the corner of the offending nail. Instruct the patient to soak the toe in heat water daily, take away the tape closure, and reinsert a brand new tape strip. This process is repeated until the nook of the nail or the nail spicule has grown out and cleared the periungual gentle tissue, at which time it can be reduce straight throughout. When the degree of inflammation is moderate, nail splinting is completed by utilizing the flexible tube procedure. Perform a digital block and elevate the lateral fringe of the nail with forceps or a hemostat. Gonococcemia, for example, is one cause of tenosynovitis that must be thought of within the acceptable setting. B ursitis and tendinitis are phrases incessantly used to describe quite so much of frequent and often ill-defined regional musculoskeletal circumstances characterised mainly by ache and incapacity at the involved site. They are both periarticular or contained within particular delicate tissue buildings. Use of injection therapy with local anesthetics and corticosteroids for bursitis and tendinitis can relieve pain, cut back inflammation, and improve mobility. Injection therapy could present definitive treatment of a situation or function an adjunct to facilitate rehabilitation therapy. Several invasive and noninvasive strategies can be utilized for the remedy of trigger factors and myofascial ache syndromes. Successful remedy of any these musculoskeletal conditions relies upon extremely on an correct diagnosis and the use of applicable methods. Hence, myofascial ache originating from set off factors is commonly attributed to a plethora of other conditions.
5 mg ditropan discount mastercard
Therefore all knee injuries with significant swelling gastritis weight gain order 2.5 mg ditropan amex, hemarthrosis chronic gastritis mayo 2.5 mg ditropan otc, or a dislocating mechanism of damage ought to be evaluated with the particular intent of ruling out vascular damage. Early consultation must be looked for knee dislocations because of the excessive incidence of problems and the frequent want for operative intervention. The decision to pursue angiography in a affected person with a dislocated knee is greatest made in session with an orthopedic surgeon. The basic initial approach for every type of knee dislocation is to apply traction to the extremity. This Knee Dislocation Reduction three 1 2 Additional maneuvers could also be required, relying on the kind of dislocation. Often this maneuver alone will scale back the joint because of the extreme ligamentous disruption related to the dislocation. The interosseous distance is widened and the proximal finish of the fibula is displaced laterally. For posterior dislocations, carry the proximal finish of the tibia to full the reduction. It is accompanied by obvious prominence of the fibular head anteriorly; no associated neurovascular problems are noted. The less common posterior dislocation could additionally be accompanied by peroneal nerve injury. These injuries cause extreme ligamentous and other derangements in the knee and usually require operative stabilization with an extended interval of restoration and physical remedy. Reduction Technique To scale back an anterior fibular head dislocation, place the patient supine and flex the affected knee to ninety levels to loosen up the biceps femoris tendon. Dorsiflex and externally rotate the foot and apply direct stress to the fibular head; discount is often signified by a snap. When the knee is flexed, the stability of this joint is decreased due to relaxation of the fibular collateral ligament. The usual mechanism is a strong quadriceps contraction combined with a strong valgus and external rotation element. The patient will report that the leg "went out" and will describe really seeing the lateral deformity caused by the displaced patella. Clinical clues to a spontaneously reduced patella embody the presence of a knee effusion and tenderness along the medial edge of the patella. Osteochondral fractures are detectable in approximately half the sufferers with patellar dislocations, but many of those fractures are visible solely on arthroscopy. The scientific prognosis of patellar dislocation in an older affected person should be made with caution as a end result of these are primarily accidents involving the younger. C Superior dislocation Lateral view D Intercondylar dislocation Lateral view Reduction Technique and Post-Reduction Care Reduction of a lateral patellar dislocation is normally quite easy. If the affected person is anxious or in great discomfort, premedication ought to be thought-about (see Chapter 33). The two fundamental maneuvers for patellar relocation are extension of the knee and mild medial stress applied to the patella while lifting the most lateral fringe of the patella over the femoral condyle. Orthopedic follow-up is important due to the necessity for physical therapy and the excessive price of persistent instability. Recurrent dislocations and people associated with an osteochondral fracture may require operative restore. Patellar dislocations in different locations are often irreducible, and orthopedic consultation ought to be sought. Intracondylar, superior, and vertical axis (dorsal fin) dislocations are extremely rare and require operative discount. The uncommon horizontal dislocation may relocate with closed reduction, but surgical reduction is often essential. The knee is held in flexion, and the patella (arrow) may be seen and palpated along the lateral side of the knee. Posterior dislocations of the ankle are more widespread than anterior dislocations, they usually usually result from a fall on a plantar-flexed foot. Patients with posterior dislocations often Clinical Assessment lateral dislocation of the patella is mostly clinically apparent. The knee is held in some degree of flexion and the patella can easily be seen and palpated on the lateral facet of the knee. Tenting of the patella is often detectable unless vital soft tissue swelling is current. Anterior dislocations typically end result from forced dorsiflexion or a blow directed posteriorly onto the distal end of the tibia while the foot is fastened. The talus is prominent anteriorly, and the dorsalis pedis pulse could additionally be misplaced secondary to pressure from the talus. Superior dislocations are unusual and lead to diastasis of the tibiofibular joint. These accidents are often the outcomes of a big axial drive, similar to a fall from a major peak. Therefore clinicians should search for concomitant calcaneal or low spine fractures. Radiographic Examination Because of the high rate of associated fractures and the clinical problem in assessing for the presence or the precise nature of a dislocation, it is recommended that pre-reduction radiographs be obtained for all suspected ankle dislocations. The emergency clinician will typically must scale back these accidents because of the acute lateral deformity and occasional compromise of the dorsalis pedis artery by stretch. Open dislocations (in the absence of vascular compromise) may be higher handled by working room washout earlier than making an attempt discount. Application of a stirrup splint along with the posterior splint will provide additional stability (see Chapter 50). The necessity of admission to the hospital must be determined in session with an orthopedic surgeon. Many patients with these accidents have associated fractures that require surgical intervention. For purposes of this dialogue, dislocation accidents of the foot may be divided into these of the hindfoot and people of the forefoot. It may be inconceivable to accurately determine the exact type of dislocation until pre-reduction films are obtained. The main dislocations are subtalar and talar dislocations and midtarsal fracture-dislocations (lisfranc injury). Although x-ray findings are often refined and easily missed, a lisfranc injury is complex and all the time a fracturedislocation due to the rigid nature of the region. Reduction is at all times painful in an awake patient, and sufficient premedication must be administered. For posterior dislocations, place the patient supine and flex the knee slightly to relax the Achilles tendon. An assistant can do this, or the patient may be positioned such that the knee hangs over the top of the mattress. Grasp the foot with both arms; place one hand on the heel and the opposite on the forefoot. Have a second assistant apply downward strain on the distal finish of the tibia and transfer the heel anteriorly to have an result on discount.