
Brahmi dosages: 60 caps
Brahmi packs: 1 packs, 2 packs, 3 packs, 4 packs, 5 packs, 6 packs, 7 packs, 8 packs, 9 packs, 10 packs

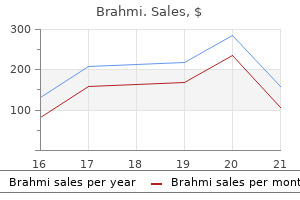
Brahmi 60 caps cheap on line
Other pathologies related to constipation Constipation could additionally be brought on by any stricturing lesion and carcinoma of the colon is a particular concern treatment 1 degree burn brahmi 60 caps order otc. Painful anal lesions similar to fissure treatment gout 60 caps brahmi best, abscess or prolapsed haemorrhoids may also give rise to constipation by inhibiting the want to defecate. Solitary rectal ulcer the time period solitary rectal ulcer is strictly a misnomer, because the lesions could also be multiple and ulceration may not essentially be current. The macroscopic appearance is of a pink thickened space of rectal mucosa usually with a shallow ulcer in the centre. Clinically, all sufferers have problem in defecation which entails going to the toilet a quantity of instances a day however only actually defecating a couple of times. If a inflexible Aganglionosis and/or myenteric plexus lesions Other than medication, constipation could also be caused by malfunction of the intrinsic nervous system of the big gut and this in turn can be subdivided into Hirschsprung disease and idiopathic megacolon and megarectum. These are handled as separate issues within the following sections of this chapter. Constipation because of extracolonic elements Extracolonic components which will give rise to constipation include: �illness causing immobility. However, the only accurate means of demonstrating an intussusception is through the use of defecating proctography. Treatment may be tough and a conservative strategy ought to be taken within the first occasion. A high-fibre food regimen and the use of suppositories might forestall extreme straining and alleviate the symptoms. Complications the primary complication of pseudo-obstruction is faecal peritonitis secondary to perforation of the caecum. Treatment In the first instance, management consists of intravenous fluids, nasogastric aspiration and decompression with a flatus tube inserted at rigid sigmoidoscopy. Concomitantly, it is important to right any metabolic disturbances, treat infections and stop any medicines which will affect colonic motility. This reduces the diameter of the caecum in about 70% of cases, but in about 40% repeated colonoscopy might be required. Recurrence of the pseudo-obstruction may be decreased by inserting a drainage tube into the right aspect of the colon on the time of the primary colonoscopy. Surgery for acute colonic pseudo-obstruction is indicated if all these conservative measures fail to bring about a reduction in the measurement of the caecum. In the absence of indicators suggesting ischaemia or perforation of the bowel, the operation of choice is a tube caecostomy via a restricted right iliac fossa incision to expose the caecum. A massive Foley catheter can then be used to intubate the caecum and this should be retained for about three weeks. However, if there are indicators of ischaemia or perforation, a midline laparotomy ought to be used. Under most circumstances, a direct anastomosis must be deferred and an ileostomy and mucus fistula customary. It must be remembered that colonic pseudo-obstruction is associated with a significant mortality, largely owing to the underlying illnesses that are associated with this situation. Colonic pseudo-obstruction Acute colonic pseudo-obstruction or Ogilvie syndrome is characterized by marked dilation of the colon in the absence of mechanical obstruction. It practically always happens in hospitalized sufferers and the overwhelming majority have an related condition corresponding to infection, widespread malignancy, recent surgical procedure or trauma significantly to the backbone. Clinical options the scientific features of acute colonic pseudo-obstruction intently mimic acute massive bowel obstruction. The affected person usually has colicky abdominal pain and progressive distension of the abdomen is the rule. Constipation is common, though not absolute, as some patients will proceed to move a small amount of flatus or liquid stool. Diagnosis the diagnosis is generally made on plain stomach radiograph, which shows the typical look of a distal colonic obstruction typically with the cut-off within the descending colon. Measurement of the diameter of the caecum on the radiograph is necessary as perforation is common as soon as this exceeds 12 cm. It may be outlined as belly discomfort or ache related to defecation or a change in bowel behavior and with an element of disordered defecation. They encompass an irregular stool frequency (more than thrice a day or lower than thrice a week), irregular stool consistency (hard, loose or watery), abnormal passage of stool (urgency, straining or tenesmus), the passage of mucus and abdominal bloating or distension. The disease presents variably, starting from mildly symptomatic fluctuation in bowel habit and left lower quadrant stomach pain, via haemorrhage and localized sepsis to colonic fistulation, perforation and life-threatening peritonitis. In addition, signs might present as an isolated incidence, or develop right into a persistent criticism. Considered a disease of Western society and of elderly sufferers, its incidence is rising along with associated episodes of hospitalization. Despite the numerous related healthcare burden, the aetiology, natural historical past and optimum management of this illness remains controversial. The terminology utilized to describe the completely different medical displays and illness stages related to diverticular disease could be variable. The time period mychosis is used within the context of diverticular disease to describe muscular shortening and thickening of the colonic wall, commonly seen at surgery. The first noted reference to colonic diverticula as a pathological entity was made by the French surgeon Alexis Littre within the 1700s, though this was not in relation to diverticular disease per se. The pathology we recognize right now as diverticular illness was first described by Jean Cruvehiler in 1849. Its absence from early surgical textbooks at this time suggests the illness was not as prevalent, or not as recognized, as right now. Mayo reported the primary surgical resection for classy diverticulitis in 1907, advocating major resection, though the disease remained uncommon. Although this case collection promoted major resection, staged resection consisting of drainage and stoma, interval resection and subsequent stoma reversal remained routine till the development of alternative remedy paradigms in the trendy era. Similarly, elective surgical procedure for recurrent illness has seen a step-change in recent years. Normally this can take the form of barium enema and sigmoidoscopy or colonoscopy. Certainly, if a affected person has irritable bowel-type symptoms related to rectal bleeding, weight loss or different suspicious symptoms, they need to be thoroughly investigated. The diagnosis, nevertheless, rests on scientific features and the diagnostic criteria agreed on the multinational consensus assembly on practical gastrointestinal disorders held in Rome in 1999 are as follows. If constipation is a big characteristic then dietary fibre ought to be increased by using wheat, bran or bulking brokers. For belly pain, anticholinergic or antispasmodic brokers corresponding to mebeverine may be of worth.
Diseases
- Cleft lip palate pituitary deficiency
- Crystal deposit disease
- Genito palatocardiac syndrome
- Fibular aplasia ectrodactyly
- Turcot syndrome
- Epilepsy, partial, familial
- Boil
- Choroideremia
- Congenital afibrinogenemia
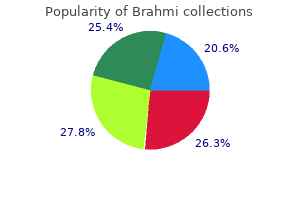
Discount 60 caps brahmi with mastercard
Mutations in the p16 gene are found in approximately 60% of pancreatic adenocarcinomas and may be associated with brief affected person survival medications xl buy discount brahmi 60 caps. When recent diabetes was eradicated medicine for sore throat order 60 caps brahmi amex, some studies found as high as a sixfold danger for pancreatic most cancers in diabetic women but not in diabetic males. In addition, there have been varying definitions of diabetes in all reported research. We due to this fact do not know if all diabetics or a special subset are at risk from pancreatic most cancers. It could be that diabetics have so many different problems that few actually stay long sufficient to develop pancreatic cancer. The second hypothesis is that the presence of pancreatic cancer ultimately induces glucose intolerance. This is supported by the reality that in many instances the diabetes is identified within 2 years before the cancer is discovered. Thus, there could additionally be two types of diabetes mellitus in pancreatic most cancers sufferers: (1) people in whom the hereditary kind is present with its possible increased threat of pancreatic cancer and (2) sufferers in whom the hyperglycaemia is of shorter duration and is a results of the pancreatic cancer. There is a definite suggestion of a bimodality of length of scientific diabetes mellitus in several collection of pancreatic cancer sufferers (40% of patients with duration of higher than 2 years, and 50% with length of less than 1 year). Alcoholism and persistent pancreatitis Retrospective epidemiological knowledge concerning an affiliation between alcoholism and pancreatic cancer are inconclusive. As with diabetics, alcoholics have so many different issues that pancreatic most cancers is considered one of their lesser worries. The primary cause for considering an alcohol�pancreatic cancer association is that pancreatitis (which can be induced by alcohol) has been associated with pancreatic cancer. Cancer of the head of the pancreas this has to be differentiated from most cancers of the ampulla, decrease common bile duct and/or duodenum since these latter tumours could current with similar features. Progressive jaundice occurs in over 75% of sufferers with carcinoma of the head of the pancreas and the incidence of jaundice decreases as the situation of the lesion progresses to the left in path of the tail of the pancreas. Nausea, epigastric bloating, change in bowel habits and vomiting are often present. Haematemesis and melaena sometimes happen in late instances on account of direct invasion of the duodenal or gastric mucosa by tumour or superior mesenteric�splenic vein compression by the tumour. Chills and fever due to cholangitis can occur in longstanding biliary obstruction. These are the very sufferers in whom most profit may be gained by applying the extra refined investigative strategies. It has turn out to be obvious that the prognosis of advanced pancreatic cancer may be made after a careful historical past and routine physical examination. This logic pertains especially to most cancers of the body and tail of the pancreas which is never, if ever, curable in a symptomatic affected person. Percutaneous needle biopsy of any accessible lesion, including the pancreatic mass, can obtain the analysis in many circumstances and the length of hospitalization can be appreciably shortened. The frail elderly affected person with clinically apparent most cancers of the physique or tail of the pancreas ought to be spared the mortality and morbidity of a diagnostic laparotomy. Another method of obviating laparotomy in these significantly sick people is to carry out laparoscopy and direct vision biopsy. The ache could initially be uninteresting and imprecise, localized to the epigastrium or to the again, or it might transfer to either upper quadrant. In late instances, the affected person learns to acquire partial aid by flexing the trunk ahead. Severe pain invariably indicates extension of tumour into the perineural lymphatics and the posterior parietes. Again, haematemesis and melaena could additionally be late features due to mucosal invasion or portal hypertension. Physical examination in the early stages could reveal surprisingly few irregular bodily signs. Centralization or regionalization of the management of adverse pancreatic issues is lengthy overdue due to the dependence on refined diagnostic and therapeutic methods. Positive bodily signs in a affected person with pancreatic cancer typically reflect incurability. The prognosis subsequently must be made earlier than the looks of irregular physical indicators. Surgical therapy of pancreatic cancer Emphasis must be positioned on preoperative analysis and enough preparation of the affected person with pancreatic cancer. The aspirated material is smeared on glass slides and fixed and stained by the Papanicolaou or Giemsa methodology for microscopic examination. Preoperative preparation All jaundiced sufferers must be kept in a great state of diet and hydration with supplemental intravenous fluids, elemental food regimen and multivitamins as deemed necessary. If the patient is grossly malnourished, a interval of parenteral hyperalimentation both earlier than and after operation may be beneficial. Daily injections of vitamin K are administered, preferably for 4�5 days prior to operation. Six models of fresh frozen plasma, six items of platelets and no much less than six units of blood must be made obtainable. It should be emphasized that pancreaticoduodenectomy can now be safely carried out without blood transfusion in lots of cases. Intensive pulmonary physiotherapy, energetic mobilization and leg workout routines are strongly inspired preoperatively. The question of prophylactic digitalization and diuretic therapy is taken into account in particular person sufferers to achieve most cardiovascular compensation. Also, simpler administration of pancreatic anastomotic leakage with hyperalimentation, percutaneous drainage and somatostatin analogue has lowered the magnitude of this problem. A pyloruspreserving Whipple operation is an affordable various but could result in transient gastric stasis. The concept of extended resection for pancreatic most cancers with resections of one or more of the major vessels (regional pancreatectomy) is uniformly attended by an elevated morbidity and mortality and not using a concomitant enchancment in treatment fee. When such extensive procedures are wanted to resect the local tumour, occult metastatic disease is usually present and the illness is incurable. Several authors have advocated a selective strategy to venous resection when the lesion has been deemed resectable, the pancreatic neck is divided, and whereas dissecting the uncinate process from the superior mesenteric vein the tumour is found to be adherent to the posterolateral portion of the vein. The venous segment could be replaced with an inside jugular vein interposition graft. It have to be emphasized that resection of the portal�superior mesenteric venous axis is just beneficial whether it is relatively minor (less than 1 cm in size and less than half of the venous circumference) and it helps in reaching adequate clearance of sentimental tissue margins. Selection of patients for pancreatic resection Except in uncommon circumstances, a significant pancreatic resection is inadvisable in (1) aged folks (older than 80 years), (2) frail patients with a quantity of systemic disorders and (3) those with an estimated life expectancy of lower than three years. The operation must be reserved for the relatively match patient under essentially the most beneficial circumstances. The surgeon should use clinical judgement within the dedication of the relative indications and contraindications for each procedure. A frank dialogue should happen between the surgeon, the patient and his or her relatives prior to embarking on a probably hazardous operation. Surgical choices For curative surgical treatment of a most cancers within the head of the pancreas, four options can be found.
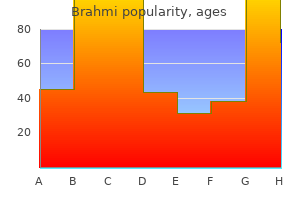
Buy brahmi 60 caps on-line
The congenital adhesions between the sigmoid colon on the left lateral wall are divided with using coagulation diathermy exposing the peritoneal reflection treatment 001 discount brahmi 60 caps online. The peritoneal reflection is then incised to reveal the embryonic aircraft of dissection (white line) medicine dictionary pill identification purchase 60 caps brahmi with mastercard, which should now be developed using countertraction and coagulation diathermy. The ureter is a whitish, non-pulsatile twine and reveals peristaltic activity when gently pinched with forceps. The aircraft anterior to the hypogastric nerves is adopted down into the pelvis until the airplane between the mesorectum and the sacral fascia has been identified. The rest of the left colon is mobilized by extending the aircraft of dissection superiorly as a lot as the splenic flexure. Any obvious adhesions between the omentum and the splenic capsule are divided to prevent haemorrhage from tearing the splenic capsule when traction is positioned on the omentum. Diathermy is used to divide the peritoneal connections between the lateral stomach wall and splenic flexure. The aircraft between the omentum and the transverse mesocolon is identified and entered, by applying traction on the transverse colon and the connected larger omentum. This aircraft is developed and followed to the extent of the splenic flexure providing enough and quick mobilization of the splenic flexure. With the division of the splenic flexure accomplished, the dissection of the peritoneum continues till the level of the aorta, the place the origin of the inferior mesenteric artery may be found. The inferior mesenteric vein is found superiorly on the inferior border of the pancreas and can additionally be dissected and ligated close to its origin. This will full the mobilization of the massive bowel from the transverse colon to the distal sigmoid. The colon is normally divided at the apex of the sigmoid colon (for low rectal cancers) unless this is significantly affected by diverticulosis, when a better division at the descending colon could additionally be more appropriate. The sigmoid mesentery is split up to the colonic wall, including the ligated trunks of both the inferior mesenteric artery and vein. The software of ahead traction to the rectum will reveal the airplane between the mesorectum and sacral fascia with the hypogastric nerves lying on it. However, these results could be partly because of case choice bias, as decrease danger tumours of the higher rectum had been included in the examine. Similar rates have been reported for native excision, with native recurrence charges reaching up to 40% for patients with T1 tumours and as much as 60% for sufferers with T2 tumours. When the tumour involves or is close to the anal sphincter advanced, abdominoperineal resection is indicated. This initiated the organization of grasp classes globally to educate colorectal surgeons the approach. A urinary catheter is advised, because it drains the bladder and due to this fact reduces its measurement and consequently increases the working subject. Preserving the nerves reduces the risk of damaging the parasympathetic nerves on the lower lateral wall of the pelvis and therefore the danger of impairing the bowel, sexual and urinary function. In females, the preliminary plane of dissection lies between the uterus and the mesorectum. The division of the peritoneum is performed at the airplane above and anterior to the apex of the rectovesical (males) or the rectouterine pouch (females). In males, the plane continues between the anterior mesorectum and the seminal vesicles and in females between the anterior mesorectum and the vagina. With the completion of the anterior dissection, the posterior and lateral features are reviewed to ensure adequacy of the entire dissection. Lloyd-Davies scissors or vessel-sealing diathermy gadget can be utilized to divide any posterior strands. When the dissection is completed the lowest a part of the rectum is viewed as a muscle tube. A linear stapler is positioned into the pelvis and the bottom part of the rectum is fastidiously positioned into its jaws. This must be positioned low enough to obtain complete tumour resection, however high sufficient to permit an additional line of staples to be placed beneath it. The hypothesis is that it may kill any intraluminal tumour cells however the evidence is at present controversial. The round stapler is inserted through the anal canal and the centre rod is advanced by way of the centre of the staple line. The resected donuts are additionally checked and despatched for histopathology examination to take a look at for tumour at the margins. Where value is an issue, hand-sewn anastomosis is more cost-effective but increases the intraoperative time. Gastrografin enema is carried out 6�8 weeks following the operation to assess the integrity of the anastomosis. Reversal of the anastomosis is carried out 6�8 weeks following the first operation or the completion of adjuvant chemotherapy. In addition some surgeons could carry out a colopouch, aiming to improve bowel functione outcomes. Sphincter preservation ultra-low anterior resection In very low rectal cancers, an ultra-low anterior resection could be carried out and due to this fact preserve the sphincter. It could be reversed at a later stage following complete recovery from surgical procedure and completion of any adjuvant medical remedy which will have been given. A combination of epinephrine (adrenaline) (1:a hundred 000) is injected initially into the submucosal aircraft and higher up into the intersphincteric plane. It is essential to fully resect the mucosa, as incomplete resection will compromise the anastomosis. The distal part of the remaining sigmoid or descending colon is brought to the anus, on top of the interior sphincter the place an anastomosis might be performed. A tension-free anastomosis is essential and subsequently full mobilization of the splenic flexure is essential. In order to defend the anastomosis, a defunctioning ileostomy or colostomy is carried out. This could be reversed at a later stage following a water-soluble enema that reveals no anastomotic leak. The extent of inside sphincter excision has been proven to influence the postoperative resting tone. Several strategies may be employed to enhance the practical outcome by increasing the volume of the neorectal reservoir (such because the colonic J-pouch). Extralevator abdominoperineal excision of rectum Abdominoperineal excision of the rectum is performed for very low rectal cancers or locally superior main cancers that might be invading the ischiorectal fossa or posterior vaginal wall. Following completion of the stomach part, the surgeon will begin the perineal dissection. The dissection is progressed to the ischiorectal fossa on each side after which posteriorly in the course of the coccyx. Co-operation between the stomach and perineal surgeon is key at this point because the belly surgeon guides the perineal surgeon as to where the dissection must be performed.
Brahmi 60 caps discount visa
Fat medicine 852 brahmi 60 caps cheap online, ligaments and tendons medications requiring central line purchase brahmi 60 caps line, bones, and cartilage are all connective tissues or connective tissue buildings. There are three types- skeletal (attached to the skeleton), cardiac (forms the heart), and easy (in the partitions of hole organs). Nervous tissue consists of irritable cells referred to as neurons, which are extremely specialised to receive and transmit nerve impulses, and supporting cells referred to as neuroglia. Nervous tissue is located in nervous system structures-brain, spinal cord, and nerves. Osmotic strain, which reflects the solute focus of a solution, determines whether or not cells gain or lose water. In these options, cells swell and may rupture (lyse) as water rushes in by osmosis. Isotonic options, which have the identical soluteto-solvent ratio as cells, trigger no modifications in cell size or shape. Cell division has two phases, mitosis (nuclear division) and cytokinesis (division of the cytoplasm). Cytokinesis often begins during anaphase and progressively pinches the cytoplasm in half. Mitotic cell division provides an elevated variety of cells for progress and repair. Cell populations uncovered to friction (such as epithelium) exchange misplaced cells all through life. With some exceptions, muscle tissue becomes amitotic by the tip of puberty, and nervous tissue turns into amitotic shortly after start. The explanation for growing older is unknown, however chemical and bodily insults, as properly as genetic programming, have been proposed as potential causes. Hyperplasia (increase in size) of a tissue or organ may occur when tissue is strongly stimulated or irritated. Atrophy (decrease in size) of a tissue or organ happens when the organ is now not stimulated normally. Which of the next would you count on to discover in or on cells whose primary perform is absorption Which of the next are potential capabilities of the glycoproteins in the plasma membrane What kind of connective tissue acts as a sponge, absorbing fluid when edema occurs What sort of connective tissue prevents muscle tissue from pulling away from bones during contraction Although cells have variations that reflect their special capabilities within the physique, what practical skills do all cells exhibit What two structural characteristics of cell membranes decide whether substances can move by way of them passively What determines whether or not or not a substance could be actively transported via the membrane Explain the impact of the following solutions on dwelling cells: hypertonic, hypotonic, and isotonic. He is advised that he has a torn knee cartilage and to anticipate that recovery and restore will take a very lengthy time. One affected person has mind harm from a stroke, another had a coronary heart attack that severely broken his coronary heart muscle, and the third has a severely broken liver (a gland) from a crushing harm in a automotive accident. All three patients have stabilized and can survive, however just one will have full functional restoration by way of regeneration. Michael had a nervous behavior of chewing on the inner lining of his lip together with his front teeth. Think rigorously about the chemistry of the plasma membrane, and then answer this question: Why is minor injury to the membrane often not a problem List an important features of epithelial tissues, and give examples of each. Name a connective tissue with (1) a soft fluid matrix, and (2) a stony exhausting matrix. Two examples of chemotherapeutic drugs (used to deal with cancer) and their cellular actions are given below. As the outermost boundary of the body, the pores and skin protects towards accidents of many sorts. Skin and Body Membranes Body membranes cover surfaces, line body cavities, and kind protective (and usually lubricating) sheets round organs. They fall into two main teams: (1) epithelial membranes, which embody the cutaneous, mucous, and serous membranes; and (2) connective tissue membranes, represented by synovial membranes. Classification of Body Membranes 4-1 List the general functions of every membrane type-cutaneous, mucous, serous, and synovial- and provides its location in the physique. Its superficial epidermis consists of a keratinizing stratified squamous epithelium. Unlike other epithelial membranes, the cutaneous membrane is exposed to air and is a dry membrane. Mucous Membranes A mucous (myukus) membrane (mucosa) is composed of epithelium (the sort varies with the site) resting on a free connective tissue membrane called a lamina propria. Notice that the time period mucosa refers only to the placement of the epithelial membranes, not their mobile make-up, which varies. However, most mucosae contain either stratified squamous epithelium (as within the mouth and esophagus) or simple columnar epithelium (as in the remainder of the digestive tract). Serous Membranes A serous membrane (serosa) is composed of a layer of easy squamous epithelium resting on a skinny layer of areolar connective tissue. In contrast to mucous membranes, which line open body cavities, serous membranes line physique cavities which are closed to the outside (except for the dorsal physique cavity and joint cavities). The parietal (pah-rie-tal: parie = wall) layer strains a selected portion of the wall of the ventral physique cavity. It folds in on itself to kind the visceral (viser-al) layer, which covers the surface of the organs in that cavity. In the body, the serous layers are separated not by air however by a scanty amount of thin, clear fluid, called serous fluid, which is secreted by both membranes. The serous fluid permits the organs to slide simply throughout the cavity walls and each other without friction as they perform their routine features. This is extraordinarily essential when mobile organs such because the pumping heart and a churning stomach are concerned. The serosa lining the abdominal cavity and masking its organs is the peritoneum (per -to-neum). They additionally line small sacs of connective tissue referred to as bursae (berse) and the tubelike tendon sheaths. Chapter 4: Skin and Body Membranes 111 Cutaneous membrane (skin) Mucosa of nasal cavity Mucosa of mouth Esophagus lining Mucosa of lung bronchi (a) Cutaneous membrane (the skin) covers the body surface. Outer balloon wall (comparable to parietal serosa) Air (comparable to serous cavity) Inner balloon wall (comparable to visceral serosa) Parietal pleura Visceral pleura (d) A fist thrust into a flaccid balloon demonstrates the relationship between the parietal and visceral serous membrane layers.
Doorweed (Knotweed). Brahmi.
- Bronchitis; cough; lung diseases; skin diseases; decreasing sweating with tuberculosis; increasing urine; redness, swelling, and bleeding of the gums, mouth, and throat; and preventing or stopping bleeding.
- Are there safety concerns?
- What is Knotweed?
- How does Knotweed work?
- Dosing considerations for Knotweed.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96539
Proven 60 caps brahmi
The building blocks treatment tennis elbow brahmi 60 caps order fast delivery, or monomers medications similar to cymbalta brahmi 60 caps otc, of these fibers are made by the connective tissue cells and secreted into the ground substance in the extracellular area, where they be a part of together to kind the various fiber types. Because of its extracellular matrix, connective tissue is able to form a soft packing tissue around different organs, to bear weight, and to withstand stretching and different abuses, such as abrasion, that no different tissue could endure. At the other extreme, bone and cartilage have very few cells and enormous amounts of exhausting matrix, which makes them extraordinarily sturdy. Their main variations reflect particular cell varieties, fiber types, and the number of fibers within the matrix. From most inflexible to softest or most fluid, the main connective tissue lessons are bone, cartilage, dense connective tissue, unfastened connective tissue, and blood. Bone Bone, sometimes known as osseous (ose-us) tissue, consists of osteocytes (bone cells) sitting in cavities known as lacunae (lah-kune; "pits"). Because of its rocklike hardness, bone has an exceptional capacity to shield and help other body organs (for example, the skull protects the brain). It forms the supporting structures of the larynx, or voice field, attaches the ribs to the breastbone, and covers the ends of many (Text continues on web page 96. The matrix, which is produced by the connective tissue cells after which secreted to their exterior, has two main elements, a structureless ground substance and fibers. The ground substance of the matrix is composed largely of water plus some adhesion proteins and huge, charged polysaccharide molecules. The cell adhesion proteins serve as a glue that permits the connective tissue cells to attach themselves to the matrix fibers embedded within the ground substance. As these polysaccharides turn into more abundant, they trigger the matrix to vary from fluid to gel-like to agency in its consistency. Depending on the connective tissue sort, various sorts and amounts of fibers are deposited in the matrix and type part of it. These include collagen (white) fibers distinguished by their high tensile strength; elastic (yellow) fibers, which have the power to be stretched and then recoil; and Bone cells in lacunae Central canal Lacunae Lamella (a) Diagram: Bone Photomicrograph: Cross-sectional view of ground bone (165�). Chondrocyte (cartilage cell) Chondrocyte in lacuna Lacunae Matrix (b) Diagram: Hyaline cartilage Photomicrograph: Hyaline cartilage from the trachea (400�). Chondrocytes in lacunae Chondrocytes in lacunae Collagen fibers (c) Diagram: Fibrocartilage Photomicrograph: Fibrocartilage of an intervertebral disc (150�). Elastic fibers Collagen fibers Fibers of matrix Nuclei of fibroblasts Fibroblast nuclei (e) Diagram: Areolar Photomicrograph: Areolar connective tissue, a soft packaging tissue of the body (270�). Nuclei of fats cells Vacuole containing fats droplet Nuclei of fat cells Vacuole containing fat droplet (f) Diagram: Adipose Photomicrograph: Adipose tissue from the subcutaneous layer beneath the pores and skin (570�). The skeleton of a fetus is made largely of hyaline cartilage; however by the time the infant is born, most of that cartilage has been changed by bone. The exceptions embody the epiphyseal, or growth, plates in lengthy bones, which allow the bones to develop in length during youth. Although hyaline cartilage is probably the most plentiful kind of cartilage in the physique, there are others. Crowded between the collagen fibers are rows of fibroblasts (fiber-forming cells) that manufacture the constructing blocks of the fibers. Dense connective tissue forms robust, ropelike constructions such as tendons and ligaments. Tendons attach skeletal muscles to bones; ligaments connect bones to bones at joints. Chapter three: Cells and Tissues 97 Loose Connective Tissue Relatively talking, free connective tissues are softer and have more cells and fewer fibers than another connective tissue type except blood. It features as a universal packing tissue and connective tissue "glue" because it helps to hold the inner organs collectively and in their proper positions. A soft layer of areolar connective tissue referred to as the lamina propria (lahm-nah propre-ah) underlies all mucous i membranes. In reality, when considered through a microscope, a lot of the matrix appears to be empty area, which explains the name of this tissue kind (areola = small open space). Because of its free and fluid nature, areolar connective tissue provides a reservoir of water and salts for the encircling tissues, and basically all body cells obtain their vitamins from and release their wastes into this "tissue fluid. Many kinds of phagocytes wander by way of this tissue, scavenging for bacteria, useless cells, and different particles, which they destroy. Because the oilcontaining area appears empty and the thin rim of cytoplasm containing the bulging nucleus appears like a ring with a seal, fat cells are generally known as signet ring cells. Adipose tissue types the subcutaneous tissue beneath the skin, where it insulates the physique and protects it from bumps and extremes of both warmth and cold. Adipose tissue also protects some organs individually-the kidneys are surrounded by a capsule of fat, and adipose tissue cushions the eyeballs of their sockets. There are additionally fat "depots" in the physique, such as the hips and breasts, where fats is stored and out there for fuel if wanted. Reticular tissue is limited to sure sites: It forms the stroma (literally, "bed" or "mattress"), or internal framework of an organ. The stroma can help many free blood cells (largely lymphocytes) in lymphoid organs corresponding to lymph nodes, the spleen, and bone marrow. The "fibers" of blood are soluble protein molecules that turn out to be seen solely during blood clotting. Blood is the transport automobile for the cardiovascular system, carrying vitamins, wastes, respiratory gases, and lots of other substances throughout the physique. Skeletal Muscle Skeletal muscle tissue is packaged by connective tissue sheets into organs known as skeletal muscular tissues, that are connected to the skeleton. These muscle tissue, which can be managed voluntarily (or consciously), type the flesh of the physique, the socalled muscular system (see Chapter 6). When the skeletal muscles contract, they pull on bones Q: Cell division typically yields two daughter cells, each with one nucleus. Nuclei Part of muscle fiber (a) Diagram: Skeletal muscle Photomicrograph: Skeletal muscle (195�). Intercalated discs Nucleus (b) Diagram: Cardiac muscle Photomicrograph: Cardiac muscle (475�). Smooth muscle cell Nuclei (c) Diagram: Smooth muscle Photomicrograph: Sheet of clean muscle (285�). A: 98 Chapter 3: Cells and Tissues ninety nine Brain Spinal wire Nuclei of supporting cells 3 Nuclei of supporting cells Cell body of neuron Neuron processes Diagram: Nervous tissue spinal cord, and nerves. Neurons and supporting cells kind the brain, View histology slides >Study Area> or skin. The cells of skeletal muscle are lengthy, cylindrical, multinucleate, and they have obvious striations (stripes). Cardiac Muscle Cardiac muscle (covered in additional element in Chapter 11, is found solely in the coronary heart.
Discount brahmi 60 caps overnight delivery
The disease can also be commoner in sufferers with kind 1 diabetes mellitus (2�8%) treatment goals for depression buy 60 caps brahmi fast delivery, Down syndrome medicine 0031 quality 60 caps brahmi, sarcoidosis, infertility (both sexes), sufferers with IgA antibody deficiency and certain autoimmune issues (thyroid disease, rheumatoid arthritis, continual energetic hepatitis, Addison disease and Sj�rgen syndrome). Clinical features the disease may current at any time of life from the primary few months to old age. Babies and younger kids current after weaning (9 months to 3 years) with malabsorption and diarrhoea (frequent pale stools) but generally paradoxically with constipation, refusal to feed, weight loss/failure to thrive, vomiting, anorexia and irritability. Older youngsters and adults may current with anaemia (folate or iron deficiency), stomach discomfort, arthralgia, fatigue and malaise, diarrhoea, steatorrhoea and malabsorption. On examination, mouth ulcers and angular stomatitis are widespread and are associated with deficiencies of folate (85%), vitamin D (up to 30%), vitamin K (10%) and vitamin B12. Some adult coeliac disease patients current with infertility (both sexes) and females with repeated miscarriages. The classical manifestations of coeliac disease embrace malabsorption, continual diarrhoea, anaemia, rickets, failure to develop, stomach bloating, offensive cumbersome stools, dermatitis herpetiformis (blistering itchy rash on the again, elbow and scalp) and mouth ulcers. The overwhelming majority of patients who develop dermatitis herpetiformis may have coeliac illness. Other checks A small bowel follow-through shows an irregular look in 90% of patients although the appearances are non-specific. The normal fantastic feathery look of the mucosa is now not seen however is changed by a coarse mucosal sample with broad bars. As the disease turns into more severe the small bowel might appear as a featureless tube. Changes are mainly seen in the jejunum however distal spread is seen in more severe disease. The most important diagnostic take a look at is jejunal biopsy which may be achieved either at higher gastrointestinal endoscopy or utilizing a suction (Crosby) capsule. Other investigations which must be carried out embrace full blood depend and blood movie for Howell�Jolly bodies (splenic atrophy), liver operate checks and small bowel distinction research to exclude different causes of malabsorption/diarrhoea or lymphoma. The non-bowelrelated complications embody dermatitis herpetiformis and neurological dysfunction leading particularly to cerebellar ataxia often with a peripheral neuropathy. The major complications of coeliac illness associated to the intestinal disease are dietary deficiencies leading to iron-deficiency anaemia, polyvitamin deficiencies and osteoporosis with fractures (50%). The sufferers Vascular abnormalities of the gut 923 are also at an increased risk of mouth, throat, oesophageal and small bowel most cancers. Overall the incidence of malignancy in adult coeliac disease is in the area of 10%. Angiodysplasia might trigger gastrointestinal bleeding normally of the recurrent occult sort, however rarely the bleeding could also be overt and severe, inflicting life-threatening hypovolaemia. Treatment the only efficient treatment of coeliac illness is strict lifelong complete avoidance of gluten present in cereals such as wheat, rye and barley (many tolerate oats). The gluten-free food plan quickly induces scientific enchancment, which is mirrored by restoration of the villous structure of the mucosa. Although moderate quantities of oats are allowed, the British Society of Gastroenterology tips suggest oats be excluded a minimal of for the first yr whereas patients get accustomed to a gluten-free food regimen before oats are cautiously introduced. A gluten-free food plan must be life-long, as leisure of food regimen precipitates a relapse of signs and increases the incidence of problems. The diet should be supplemented by folic acid, iron, calcium and vitamin D as needed. Pathology and aetiology Gastrointestinal angiodysplasia is often found within the aged (60 years) with an estimated incidence of 0. The majority of angiodysplasias happen within the colorectal area, mainly in the best colon (70�80%), the most common web site being the caecum. However, lesions within the small bowel and gastroduodenal region may happen in their own right, or as synchronous lesions in affiliation with colonic angiodysplasias. Angiodysplasias are composed of ectatic, thin-walled vessels lined by endothelium alone or with small quantities of smooth muscle intimately associated with dilated, tortuous submucosal veins. Large lesions are associated with enlarged feeding arterioles and arteriovenous fistulas. The most favoured concept is intermittent, low-grade obstruction of submucosal veins at the stage of the muscularis propria. In time this venous obstruction results in dilatation and tortuosity of the associated submucosal venules and capillaries. This speculation is according to the excessive incidence of angiodysplasia in the best colon the place intraluminal and wall rigidity is highest. Another hypothesis postulates elevated expression of angiogenic factors because the cause. A attainable mechanism by which aortic stenosis could lead to the development of angiodysplasia is through the event of an acquired form of von Willebrand illness as a end result of mechanical disruption of von Willebrand multimers from the turbulent blood circulate passing via the narrowed aortic valve in affiliation with the thrombocytopenia which characterizes this illness. Angiodysplasia of the small gut presents with recurrent obscure bleeding in sufferers with unfavorable higher gastrointestinal endoscopy and colonoscopy (5%). Angiodysplasia of the stomach or duodenum is the least frequent and is liable for 5% of gastrointestinal bleeding episodes, which can be occult, presenting with irondeficiency anaemia, or overt, causing haematemesis. Vascular abnormalities of the intestine these constitute a heterogeneous group of situations which share a associated pathology consisting of abnormal lesions of the intestine alone or with related lesions in other organs together with the skin. In the overwhelming majority of cases, treatment is with endoscopic remedy, much less generally with interventional angiography. The lesions that are malformations quite than neoplasms embody angiodysplasia, phlebectasia, telangiectasia and haemangiomas. Angiodysplasia the phrases angiodysplasia, arteriovenous malformation, angioectasia, and vascular ectasia are sometimes used synonymously. The confusion is added to by the truth that whereas some authors use angioectasia as a generic time period, others reserve it for colonic lesions. Angiodysplasias are lesions which occupy the mucosa and submucosa of the gastrointestinal tract and encompass a cluster of arteriolar, venular and capillary vessels. Angiodysplasia can also be found incidentally during an endoscopy for unrelated reasons. In these patients angiodysplastic lesions are often a number of and will happen anywhere within the gut. The elevated danger of bleeding in uraemic sufferers is believed to be platelet dysfunction induced by the end-stage renal illness. The greater incidence of bleeding from angiodysplasia in sufferers with von Willebrand illness is said to the underlying coagulopathy. In sufferers with aortic stenosis the recurrent bleeding episodes are reduced markedly in those handled with aortic valve substitute. Initially all patients have higher gastrointestinal endoscopy and colonoscopy, with other endoscopy exams being performed if the trigger of the gastrointestinal bleeding stays obscure. Endoscopically, angiodysplasias have a attribute look of small (5�10 mm), flat, cherry purple lesions with a mesh of ectatic blood capillaries radiating from a central vessel. Opioid antagonist (naloxone) administration is reported to improve the detection rate of colonic angiodysplasias.
Generic brahmi 60 caps on line
A 4�6 week period of maturation of the T-tube tract is required earlier than the procedure can be carried out safely medications you can take when pregnant discount brahmi 60 caps line. Thereafter treatment 2 prostate cancer 60 caps brahmi effective, the T-tube tract is dilated to allow the introduction of the slender flexible choledochoscope. Endoscopic sphincterotomy with stone extraction is the simplest method of coping with the problem of retained stones and can be performed in sufferers with and with out T-tubes. Surgical management of missed stones is reserved for these patients in whom the above strategies have failed or problems have developed during or after attempted endoscopic or percutaneous stone extraction. The management of patients with recurrent ductal calculi is dependent upon their age and general condition. Endoscopic sphincterotomy and stone extraction is the first-line remedy and surgical procedure (open or laparoscopic) reserved if this strategy fails. During surgical procedure, the stones are removed atraumatically via biliary balloon catheters, stone-grasping forceps or Dormia baskets as described previously. A completion check by means of a choledochoscopic inspection or cholangiography abolishes or reduces the incidence of residual stones. In other situations, recurrent ductal calculi are often multiple and related to gross dilatation of the bile duct and in some cases obvious distal ductal stenosis. This may be main (papillary stenosis) or be secondary to trauma inflicted by metallic bougies introduced via the sphincter area at the time of exploration of the widespread bile duct. In patients with multiple ductal calculi, grossly dilated bile duct (>2 cm) or papillary stenosis, a drainage operation is indicated: choledochoduodenostomy or transduodenal sphincteroplasty. However, sphincteroplasty carries a big risk of pancreatitis and entails a sizeable duodenotomy. Recurrent ductal calculi Ductal calculi presenting 2 years or more after an operation are generally considered primary. This finding stresses the importance of avoiding non-absorbable material during operations on the biliary tract. The actual pathology remains unclear, nevertheless it seems doubtless that the clip is positioned too close to the common bile duct resulting in localized pressure necrosis. The internalized clip turns into covered with calcium bilirubinate to type a brown pigment stone. The sufferers who Intrahepatic calculi (hepatolithiasis) Intrahepatic stones (hepatolithiasis) are prevalent in Southeast Asia however uncommon in Western nations. The distal finish is closed with a working suture and the proximal end is anastomosed in an endto-side trend to the duodenum on the junction of the first with the second half. Intrahepatic stones are categorized as: intrahepatic stones, which �primary associated with intrahepaticform throughout the intrahepatic ducts and are duct strictures secondary, which type throughout the extrahepatic ducts however migrate �subsequently to the intrahepatic ducts. Glucuronolactone deficiency may thus result in increased deconjugation of bilirubin diglucuronide with formation of calcium bilirubinate stones. The situation is also called recurrent oriental cholangitis and has been just lately reviewed. Epidemiology Primary intrahepatic stones are prevalent in East Asian countries (Taiwan, China, Japan and Korea) and rare in Western countries, the Middle East and Africa. In Taiwan, major ductal calculi account for more than 50% of all circumstances of cholelithiasis and in Japan, 34%. Some have suggested that a low-protein food regimen decreases glucuronolactone in bile, which is an Bacterial an infection of the biliary tree and bile stasis appear to be the most important because the prevalence of micro organism within the bile of patients with hepatolithiasis exceeds 90%. All exhibit -glucuronidase enzyme exercise, which is believed to be liable for the hydrolysis of the soluble bilirubin glucuronide to the water-insoluble unconjugated bilirubin which then combines with ionized calcium and precipitates, forming calcium bilirubinate stones. Intrahepatic stones are often related to strictures and dilatations of the intrahepatic ducts. In Taiwan, which has a really high incidence of intrahepatic lithiasis, infestation with C. Likewise for disease located exclusively in the proper intrahepatic ducts, right anterior or posterior segmentectomy could also be essential. Right hepatic lobectomy is nonetheless inadvisable due to surgical risks especially as a end result of the percutaneous cholangioscopic strategy supplies a much safer and efficient treatment. In the past, an prolonged hepaticojejunostomy (Rouxen-Y) with a everlasting cutaneous access was used for the removal of stones from the best hepatic ductal system. However, this has been largely replaced by the percutaneous transhepatic remedy. When hepatolithiasis entails each intrahepatic ducts (more than 50% of patients), surgical treatment could also be used for left lateral hepatic segmentectomy or left hepatic lobectomy and prolonged hepaticojejunostomy (Roux-en-Y) with everlasting cutaneous entry. Some would nevertheless disagree with this and suggest percutaneous remedy for bilateral stones as the first possibility before recourse to surgical treatment. Percutaneous transhepatic approach the percutaneous transhepatic approach has a quantity of benefits. This remedy is relevant to sufferers with multiple bilateral intrahepatic stones. Strictures can be dilated by balloons or by bougienage and the passage of Yamakawa catheters via the tract. However, percutaneous transhepatic cholangioscopic stone removing requires an experienced interventional endoscopist, preferably working with an interventional radiologist. The longterm results of percutaneous transhepatic cholangioscopy are just like these of surgery. The most necessary elements affecting the recurrence are the presence of strictures and bile stasis. Clinical options Many patients with intrahepatic stones may remain asymptomatic for a few years and sometimes the situation is just discovered throughout routine investigation. Symptomatic sufferers can current with higher abdominal ache, occasional fever, rigors and, less regularly, jaundice. In addition, these patients have moderate elevations of serum transaminases and delicate to moderate iron-deficiency anaemia. Untreated sufferers with longstanding disease with recurrent assaults of bacterial cholangitis can develop biliary cirrhosis with coagulation defects, low serum albumin and the development of ascites. Ultrasound scanning is used for screening only as its diagnostic accuracy for documenting the complete extent of hepatolithiasis is limited. Cholangitis Acute bacterial cholangitis is a critical, life-threatening emergency caused by infection of an obstructed biliary tract. The systemic manifestations of the acute illness result from bacteraemia secondary to cholangiovenous reflux induced by the biliary hypertension (<20 cmH2O). The most typical obstructing agent is an occluding stone within the common bile duct, followed by bile duct strictures (including sclerosing cholangitis) and tumours of the bile ducts, pancreatic head and periampullary lesions. Less generally, cholangitis is secondary to bilioenteric anastomoses, spontaneous bilioenteric fistulas, cystic illness of the biliary tract and duodenal diverticula. The risk factors for cholangitis following this investigation are the presence of fever before the process and malignant biliary obstruction.
Brahmi 60 caps purchase
However treatment lower back pain buy brahmi 60 caps otc, lately this concept that there are numerous extra times (up to 10 times) neuroglia compared to symptoms glaucoma buy generic brahmi 60 caps neurons has been challenged and may even be roughly the same (Azevedo et al. It is, nonetheless, extraordinarily troublesome to put an actual quantity on this and solely an approximation has been attainable. Their main function is in offering nutrient support, upkeep of homeostasis and the production of the myelin sheath. They are found all through the mind and spinal wire, and can change their form, especially once they engulf particulate material. Macroglia are subdivided into seven differing kinds, again with every having a selected role. Oligodendrocytes these cells are responsible for the production of myelin sheaths (see next section). Schwann cells Like oligodendrocytes, Schwann cells are liable for the production of the myelin sheath (see next section), however within the peripheral nervous system. They even have an additional position in phagocytosis of any particles; subsequently assist to clean the surrounding surroundings. Satellite cells these cells encompass these neurons of the autonomic system and likewise the sensory system. They maintain a stable chemical balance of the encircling setting to the neurons. Radial glia Radial glial cells act as scaffolding onto which new neurons migrate to . Enteric glia these cells are discovered within the gastrointestinal tract and help digestion and maintenance of homeostasis. The basis of the embryological development is from the neural tube, or the precursor of the central nervous system. At the front, or upper end, of that tube like structure, there are three swellings. The human brain is broadly divided into these three major regions � the forebrain, midbrain and the hindbrain. In mammals, the primary part of this neural tube � the forebrain � turns into considerably larger, with the hindbrain remaining somewhat small compared. As beforehand mentioned, the opposite approach to classify the mind based on its parts is as follows. This is comprised of the smaller portion often identified as the diencephalon (thalamus and hypothalamus) and the bigger portion of the telencephalon (cerebral hemispheres). However, the time period cerebrum refers either to the whole brain, or just the forebrain and midbrain. The left and proper cerebral hemispheres are separated by the longitudinal fissure, the place the fold of dura passes down referred to as the falx cerebri. The two hemispheres are related on the decrease free fringe of the falx cerebri and this connecting bundle of fibers is termed the corpus callosum. Broadly talking, the hypothalamus may be subdivided into two major territories � lateral and medial. Each hemisphere has a frontal, temporal and occipital pole moving in an anterior to posterior path. These are positioned in the anterior, middle and posterior cranial fossae, respectively. The gray matter of the cerebral cortices is situated on its outer facet, and is thrown into folds referred to as gyri (singular, gyrus). On the lateral floor the frontal lobe and parietal lobe are separated from one another by the central sulcus (which is commonly not as obvious as its name may suggest). The pre-central gyrus is the primary motor cortex and plenty of descending motor fibers originate right here to descend via the inner capsule, the cerebral peduncles and the pyramids. It is to this region that common body sensation (such as touch, proprioception, etc. It is much less straightforward to see the division between the parietal and occipital lobes from the lateral surface. On the medial surface, the parieto-occipital sulcus is found, which serves to separate these two lobes. In addition, the calcarine sulcus, which lies within the heart of the first visual cortex, begins on the occipital pole, passing anterior to the corpus callosum, on the splenium. The cerebral cortex is split into frontal, temporal, parietal and occipital lobes. From this, the parietal lobe passes from the central sulcus to an arbitrary line between the parieto-occipital sulcus and to the preoccipital notch. The temporal lobes are situated anterior to this line, and inferior to the lateral sulcus. They end in the olfactory bulbs which are discovered on the inferior aspect of the frontal lobes. The second of the cranial nerves, the optic nerves, move through the optic canal of the skull and move medially to join the one of the reverse side to type the optic chiasma. As the fibers pass posterior, the fibers then separate to form the optic tracts which then pass posterior and across the cerebral peduncles. At this point, these nerves are carefully related to the Circle of Willis, which is mentioned in more element in Chapter 6 (Blood Supply of the Brain and Clinical Issues). The infundibular stem of the neurohypophysis, or posterior pituitary, emerges from the tuber cinereum in the interpeduncular fossa. Immediately lateral to the optic tracts, branches of both the anterior and center cerebral arteries enter here in the space generally recognized as the anterior perforated substance. These subcortical areas of gray matter in the forebrain include the caudate nucleus, putamen, and the globus pallidus, in addition to the subthalamic nucleus and the substantia nigra. Information from the cerebral cortex is fed to the caudate and putamen, and from there to the globus pallidus, before returning via the thalamus to motor areas of the cortex. The role of the basal ganglia in movement is simply poorly understood, however basal ganglia disorders usually have profound results on motion. Treatments embrace administering L-Dopa (the precursor of dopamine) or implanting dopaminergic neurons or stem cells. The caudate nucleus bulges into the lateral ventricle and is comprised of a head, body and a tail. The caudate nucleus is an arched structure and frequently can seem twice on sectioning the brain. The body of the caudate nucleus extends posterior and lateral to the place of the thalamus. The tail of the caudate nucleus curves in an inferior and anterior path into the temporal lobe ending in the amygdaloid physique. The lentiform nucleus is found lateral to the pinnacle of the caudate nucleus and thalamus. The lateral side of the lentiform nucleus is referred to because the putamen, and is closely associated to the claustrum and the insula. The two medial components of the lentiform nucleus are referred to as the globus pallidus.

Order 60 caps brahmi otc
Reddened i pores and skin may point out embarrassment (blushing) medications not to mix buy brahmi 60 caps with visa, fever treatment molluscum contagiosum discount 60 caps brahmi with amex, hypertension, irritation, or allergy. Under sure types of emotional stress (fear, anger, and others), some people turn out to be pale. Pale skin may also signify anemia, low blood pressure, or impaired blood circulate into the area. An irregular yellow skin tone normally signifies a liver dysfunction by which extra bile pigments are absorbed into the blood, circulated all through the body, and deposited in physique tissues. Sebaceous gland Sebaceous gland duct Dermal connective tissue Eccrine gland duct Hair in hair follicle Secretory cells (a) Photomicrograph of a sectioned sebaceous gland (100) (b) Photomicrograph of a sectioned eccrine gland (205) Homeostatic Imbalance 4. Acne is an energetic infection of the sebaceous glands accompanied by pimples on the skin. Seborrhea (sebo-reah; "fast-flowing sebum"), generally recognized as "cradle cap" in infants, is caused by overactivity of the sebaceous glands. It begins on the scalp as pink, raised lesions that progressively kind a yellow to brown crust that sloughs off oily scales. Careful washing to take away the extreme oil often helps cradle cap in a new child child. Chapter 4: Skin and Body Membranes 121 Sweat Glands Sweat glands, additionally called sudoriferous (sudo-rifer-us; sudor = sweat) glands, are broadly distributed within the skin. Sweat is acidic (pH from 4 to 6), a attribute that inhibits the growth of certain micro organism, that are always present on the skin floor. Notice, nonetheless, that the facial "pores" generally referred to once we talk about our complexion are the exterior outlets of hair follicles, not these sweat pores. They are equipped with nerve endings that cause them to secrete sweat when the exterior temperature or physique temperature is high. When sweat evaporates off the skin surface, it carries large quantities of physique heat with it. The heat-regulating capabilities of the physique are important-if internal temperature modifications quite lots of degrees from the normal 37�C (98. They are normally larger than eccrine glands, and their ducts empty into hair follicles. Their secretion incorporates fatty acids and proteins, as properly as all the substances present in eccrine secretion; consequently, it may have a milky or yellowish shade. The secretion is odorless, however when micro organism that reside on the skin use its proteins and fats as a supply of vitamins for his or her growth, it takes on a musky, disagreeable odor. Apocrine glands start to perform throughout puberty under the affect of androgens (male intercourse hormones). Although their secretion is produced virtually constantly, apocrine glands play a minimal position in thermoregulation. Consider, for example, the spiky hair fashion of punk rockers and the flowing locks of some high-fashion models. But, aside from serving a couple of minor protective functions-such as guarding the head in opposition to bumps, shielding the eyes (via eyelashes), and serving to to hold foreign particles out of the respiratory tract (via nostril hairs)-our body hair has lost much of its usefulness. A hair forms by division of the well-nourished stratum basale epithelial cells within the matrix (growth zone) of the hair bulb on the inferior end of the follicle. As the daughter cells are pushed farther away from the rising region, they turn out to be keratinized and die. Thus the bulk of the hair shaft, like the majority of the epidermis, is lifeless materials and virtually completely protein. Each hair is made up of a central core known as the medulla (me-dulah), consisting of large cells and air spaces, surrounded by a bulky cortex layer composed of several layers of flattened cells. The cortex is, in turn, enclosed by an outermost cuticle fashioned by a single layer of cells that overlap one another like shingles on a roof. The cuticle is essentially the most heavily keratinized area; it offers strength and helps maintain the inner hair layers tightly compacted. They are quick and stiff in the eyebrows, long and flexible on the head, and often nearly invisible nearly in all places else. When the hair shaft is oval, hair is smooth and silky and the Practice art labeling >Study Area>Chapter 4 particular person has wavy hair. Hormones account for the development of bushy regions-the scalp and, in the adult, the pubic and axillary areas. The inner epithelial root sheath is composed of epithelial tissue and types the hair. This dermal region supplies blood vessels to the epidermal portion and reinforces it. Its nipplelike hair papilla offers the blood supply to the matrix within the hair bulb (the deepest part of the follicle). Small bands of easy muscle cells-arrector pili (ah-rektor pili; "raiser of hair")-connect each side of the hair follicle to the dermal tissue. When these muscular tissues contract (as after we are cold or frightened), the hair is pulled upright, dimpling the pores and skin floor with "goose bumps. It is very dramatic in a scared cat, whose fur actually stands on end to make it look larger to scare off its enemy. Nails A nail is a scalelike modification of the dermis that corresponds to the hoof or claw of different animals. Each nail has a free edge, a body (visible connected portion), and a root (embedded in the skin). Its thickened proximal area, referred to as the nail matrix, is liable for nail growth. As the nail cells are produced by the matrix, they turn into closely keratinized and die. The exception to that is the area over the thickened nail matrix that seems as a white crescent and is recognized as the lunule (loonyul; lunul = crescent). As noted earlier, when the provision of oxygen within the blood is low, the nail beds take on a cyanotic (blue) solid. How do secretions of apocrine glands differ from those of the eccrine sweat glands When a manufacturing unit employee caught his finger in a machine, the complete nail, plus the nail matrix and bed, was torn off. Loss of homeostasis in body cells and organs reveals itself on the skin, typically in startling methods. Less frequent, but far more damaging to body well-being, are burns and pores and skin cancers. A burn is tissue injury and cell death caused by intense warmth, electricity, ultraviolet radiation (sunburn), or certain chemical substances (such as acids), which denature proteins and trigger cell demise within the affected areas. When the skin is burned and its cells are destroyed, two life-threatening problems outcome. First, the physique loses its treasured supply of fluids containing proteins and electrolytes as these seep from the burned surfaces.