
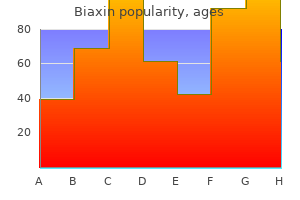
Biaxin dosages: 500 mg, 250 mg
Biaxin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills
Biaxin 250 mg without a prescription
Some genetic risk factors gastritis no symptoms biaxin 250 mg order mastercard, including issue V Leiden and the prothrombin G20210A mutation chronic gastritis sydney classification buy biaxin 250 mg overnight delivery, have been identified, but they account for much less than a minority of venous thromboembolic illness. A number of other risk components have been identified, together with immobilization during extended journey, obesity, smoking, surgical procedure, trauma, pregnancy, estrogen-containing contraceptives, postmenopausal hormone replacement, and inflammatory ailments. Chest ache, cough, or hemoptysis can indicate pulmonary infarction with pleural irritation. Low-grade fever, neck vein distention, and a loud P2 on cardiac examination can be seen. After initiating treatment with a parenteral agent, warfarin has historically been used for long-term oral anticoagulation. Warfarin can be initiated soon after a parenteral agent is given; however, no much less than 5 days are required for warfarin to achieve therapeutic anticoagulation. Novel oral anticoagulants, together with rivaroxaban, apixaban, and dabigatran, have the benefits of fastened dose regimens, fast onset of effective anticoagulation, no laboratory monitoring, and fewer drug and dietary interactions. However, the dabigatran antibody, idarucizumab, is a quickly acting antidote for dabigatran. Another method for pts at decrease danger of recurrence, particularly if there is an important cause to avoid long-term anticoagulation, is to contemplate low-dose aspirin after finishing the initial interval of normal anticoagulation. Inferior vena cava filters can be utilized if thrombosis recurs despite enough anticoagulation or if energetic bleeding precludes anticoagulation. Laboratory studies: Testing can suggest an underlying connective tissue disorders. Tissue and mobile examination: In order to present a specific diagnosis and assess disease exercise, lung biopsy is usually required. In addition, bronchoscopy can help by excluding continual infections or lymphangitic carcinomatosis. However, the extra in depth tissue samples provided by surgically obtained lung biopsies, sometimes obtained by video-assisted thoracic surgical procedure, are sometimes required to establish a specific diagnosis. Evidence for diffuse end-stage illness, similar to widespread honeycombing, or other main operative risks are relative contraindications to lung biopsy procedures. Supportive therapeutic measures embrace offering supplemental O2 for pts with vital hypoxemia (PaO2 <55 mmHg at rest and/or with exercise). Pulmonary manifestations might precede systemic manifestations of a connective tissue disorder. Lung involvement tends to be extremely immune to obtainable therapy, however cyclophosphamide and mycophenolate have modest advantages. Recurrent and migratory patchy consolidative and floor glass pulmonary opacities are frequent. It is seen virtually exclusively in cigarette people who smoke and improves with smoking cessation. Chest imaging regularly exhibits patchy bilateral ground glass opacities and dependent air-space consolidation. Granulomatous vasculitides embody inflammatory infiltrates of blood vessels with related granulomas. The two major classes of pleural effusions are transudates, that are caused by systemic influences on pleural fluid formation or resorption, and exudates, that are caused by local influences on pleural fluid formation and resorption. Common causes of transudative effusions are left ventricular heart failure, cirrhosis, and nephrotic syndrome. Common causes of exudative effusions are bacterial pneumonia, malignancy, viral infection, and pulmonary embolism. A more complete record of the etiologies of transudative and exudative pleural effusions is supplied in Table 137-1. Additional diagnostic procedures are indicated with exudative effusions to outline the cause of the native illness. Chylothorax Exudates fulfill at least one of many following three criteria: excessive pleural fluid/ serum protein ratio (>0. For exudative effusions, pleural fluid must also be examined for pH, glucose, white blood cell count with differential, microbiologic studies, and cytology. Primary spontaneous Ptx happens within the absence of underlying lung disease and sometimes results from apical pleural blebs. Simple aspiration may be enough treatment for an preliminary primary spontaneous Ptx, however recurrence typically requires thoracoscopic intervention. Secondary spontaneous Ptx happens within the setting of underlying lung illness, mostly continual obstructive pulmonary disease. Chest tube placement is often required for secondary spontaneous Ptx; thoracoscopy and/or pleurodesis (with pleural abrasion or a sclerosing agent) must also be considered. Traumatic Ptx, ensuing from either penetrating or nonpenetrating chest trauma, often requires chest tube placement. Iatrogenic Ptx can occur from transthoracic needle biopsy, thoracentesis, placement of a central venous catheter, or transbronchial biopsy. Treatment with supplemental O2 or aspiration is often enough for iatrogenic Ptx, however chest tube placement may be required. Positive pleural pressure in mechanical air flow can rapidly result in a tension Ptx with decreased cardiac output. Urgent treatment is required, either with a chest tube or, if not instantly out there, with a large-bore needle inserted into the pleural house through the second anterior intercostal space. Key illness processes in the mediastinum embrace mediastinitis and mediastinal lots. Pneumomediastinum is an additional mediastinal abnormality that may end result from alveolar rupture, esophageal perforation, or dissection of air from the neck or abdomen. Acute mediastinitis may result from esophageal perforation, following cardiac surgery with median sternotomy, or from infections in the neck, oral cavity, or face. Esophageal perforation can occur spontaneously or iatrogenically; surgical exploration of the mediastinum, restore of the esophageal perforation, and drainage of the pleural house and mediastinum are required. Mediastinitis after median sternotomy usually presents with wound drainage and is recognized by mediastinal needle aspiration. Chronic mediastinitis can range from granulomatous lymph node irritation to fibrosing mediastinitis. The most typical mass lesions within the anterior mediastinum are thymomas, lymphomas, teratomas, and thyroid lesions. Posterior mediastinal masses embrace neurogenic tumors, gastroenteric cysts, and esophageal diverticula. Biopsy procedures are typically required to diagnose mediastinal lots; needle biopsy procedures. Central hypoventilation syndrome is a rare dysfunction that includes a failure of the normal respiratory response to hypoxemia and/or hypercapnia. Parenchymal lung ailments, corresponding to continual obstructive pulmonary disease and interstitial lung disease, typically embrace dyspnea and cough. Sleep-disordered respiratory consists of daytime somnolence, snoring, and fragmented sleep.
Syndromes
- Protect the nails from exposure to detergents and chemicals by using protective rubber or plastic gloves, preferably with cotton liners.
- Alexander Graham Bell Association for the Deaf and Hard of Hearing - www.agbell.org
- Blindness
- Tenderness when the abdomen is pressed
- Name of the product (ingredients and strengths, if known)
- Cadmium
- Recurring infections
- Breathing difficulty
- Liver failure
250 mg biaxin with amex
Molecular aspects of the parotid gland gastritis diet coconut water purchase 250 mg biaxin mastercard, pancreas and liver are offered to emphasize the position of particular buildings and cell varieties in frequent medical and pathologic conditions gastritis symptoms in puppies purchase biaxin 250 mg with visa. An preliminary discussion concerning the basic features of a compound or branched gland is included in Chapter 2, Epithelial Glands Cell Biology. Partitions or septa extend from the capsule into the gland, creating lobes as giant divisions. Interlobar septa proceed to department as interlobular septa, subdividing lobes into a quantity of small lobules. The quantity of connective tissue decreases from the interlobar septa to the interlobular septa. Septa present applicable conduits for the main branches of a duct to extend from the inside of a gland to its exterior and for vessels and nerves to attain the interior of a gland. The fundamental histologic features of a salivary gland are the secretory items, the acini and the excretory ducts. An intercalated duct, lined by low squamousto-cuboidal epithelium, is the smallest duct connecting an acinus to a striated duct (see 17-2). A striated duct is lined by cuboidal-to-columnar epithelial cells with basal infoldings containing quite a few mitochondria. The intercalated and striated ducts are modestly developed within the sublingual gland. An interlobular duct is initially lined by cuboidal-to-columnar epithelium and becomes pseudostratified columnar. Several interlobular ducts converge to form a lobar duct current in interlobar septa. Lobar ducts are lined by stratified columnar epithelium, one of the few sites within the body with this kind of epithelium. Several lobar ducts, lined by stratified squamous epithelium, be a part of the main duct that drains the complete gland close to the opening into the oral cavity. The parotid, submandibular (or submaxillary) and sublingual glands are categorised as branched tubuloalveolar glands. Upon stimulation, the parasympathetic system induces the secretion of a water-rich saliva; the sympathetic system stimulates the discharge of a protein-rich saliva. The mucus and water in saliva lubricate the mucosa of the tongue, cheeks and lips throughout speech and wallowing, dissolve meals for the function of the taste buds and moisten meals for easy swallowing. The protecting perform of the saliva is dependent upon the antibacterial function of three constituents: 1. Amylase (ptyalin), which initiates the digestion of carbohydrates (starch) in the oral cavity. Parotid gland (17-4 and 17-5) Box 17-A Classification of exocrine glands � Depending on the structure of the excretory duct, glands may be divided into simple (unbranched duct) and branched or compound (branched duct). In holocrine glands (for example, the sebaceous glands of the skin), the entire cell is the secretory product. An apocrine gland (for instance, the mammary gland) releases its product along with a small amount of the apical cytoplasm of the secretory cell. It is a branched tubuloalveolar gland surrounded by a connective tissue capsule with septa, representing a component of the stroma, the supporting tissue of the gland. Septa additionally present support to blood vessels, lymphatics and nerves gaining entry to the acini, the primary parts of the parenchyma, the useful constituent of the gland. Acini are surrounded by reticular connective tissue, a wealthy capillary network, plasma cells and lymphocytes. The diameter of the intercalated duct is smaller than the acini, but the lumen of the duct is wider. Lobule Acinus Intercalated duct Striated duct Interlobular duct Lobar duct Main duct Myoepithelial cells Interlobular septum Interlobar septum Basement membrane Low cuboidal epithelium Cuboidal-to-columnar epithelium Pseudostratified columnar epithelium Columnar stratified epithelium Intercalated duct Striated duct Interlobular duct Lobar duct cells and, therefore, are classified as serous acini. Similar to all proteinproducing cells, a outstanding tough endoplasmic reticulum system occupies the cell basal region. The lumen of the acinus collects the secretory products, that are transported by lengthy intercalated ducts to the much less ample striated ducts (see 17-5). Submandibular (submaxillary) gland (see 17-4) ent in the secretory items, the serous cells are the predominant part. The intercalated ducts are shorter and the striated ducts are longer than these within the parotid gland. Sublingual gland (see 17-4) the submandibular gland is a branched tubuloalveolar gland surrounded by a connective tissue capsule. Septa derived from the capsule divide the parenchyma of the gland into lobes and lobules. However, connective tissue septa divide the glandular parenchyma into small lobes. The sublingual gland is a branched tubuloalveolar gland with both serous and mucous cells, though most of the secretory items include mucous cells. Plasma cells within the parotid gland secrete polymeric immunoglobulin A (pIgA), which binds to the secretory piece inserted within the plasma membrane of acinar, intercalated and striated epithelial cells. After transcytosis, pIgA is launched into the acinar lumen as proteolytic-resistant secretory IgA (SigA). The parotid gland consists solely of serous acini, whereas the submandibular and sublingual glands include both cell sorts. The serous cells are situated at the fundus of the acinus, forming a crescent-shaped structure (called the serous demilune) embracing the mucous cells located closer to the opening of the acinus into the intercalated duct. In blended acini, extensions of the acinar lumen project deeply between serous cells, forming intercellular secretory canaliculi for the transport of serous secretions. The outer floor of the acinus is surrounded by contractile myoepithelial cells in a basket-like trend. Several interlobular ducts drain into a wider lobar duct situated in the interlobar septum. Pancreatic acinus Centroacinar cell In the exocrine pancreas, only serous acini are current. A distinctive function of the pancreatic acinus is the presence of squamous-to-cuboidal epithelial centroacinar cells. The free apical domain of the serous acinar discharges zymogen granules between gaps of the centroacinar cell layer. Serous cells secrete a quantity of proteins, including proline-rich proteins (which are modified within the striated duct by the enzyme kallikrein), enzymes (amylases, peroxidases, lysozyme), lactoferrin, cystatins (cysteine-rich proteins) and histatins (histidine-rich proteins). Kallikrein, a serine protease secreted by epithelial cells of the striated duct, processes the proline-rich proteins and cystatins within the saliva. In addition, plasma cells secrete polymeric immunoglobulin A (pIgA), which reaches the lumen of the acinus and striated duct by transcytosis. The last saliva incorporates a posh of proteins with antimicrobial exercise and with digestive function (amylase). Bicarbonate, the primary buffering agent of the saliva, is produced in the striated duct. Plasma cell Proline-rich proteins Cystatins and histatins Plasma cell pIgA Sialic acid� and sulfate-rich mucins Enzymes amylase, lysozyme, peroxidase and lactoferrin Isotonic saliva Pellicle Kallikrein pIgA Bicarbonate Sympathetic nerve Parasympathetic nerve NaCl (active) transport) H2O (passive) transport) Capillary 1 Salivary gland acinus Hypotonic saliva NaCl (active transport) Mouth Intercalated duct 2 Striated duct In the mouth, proteins in the saliva form protecting films on the enamel called pellicles. The function of the pellicles is to present a barrier towards acids, retain moisture and regulate the adherence and activity of micro organism and yeast within the oral cavity.
Biaxin 250 mg buy discount
The dendrites are processes that arise as multiple tree-like branches of the soma gastritis acid diet effective 250 mg biaxin, forming a dendritic tree collectively chronic gastritis lasts purchase 500 mg biaxin otc. The entire surface of the dendritic branches is roofed by small protrusions called dendritic spines. Neurons have a single axon originating from the soma on the axon hillock and ending in a terminal arborization, the telodendron. The prosencephalon expands on both sides to form the telencephalon (cerebral hemispheres). By the sixth week, the diencephalon, the remaining part of the prosencephalon, gives rise to the optic outgrowth (retina and optic nerve of the eye). Midbrain Mesencephalon Rhombencephalon Pons Cerebellum Medulla oblongata the synaptic terminal or synaptic bouton. Note that although dendrites and axons branch extensively, axons branch at their distal end (the telodendron), whereas dendrites are a number of extensions of the soma or cell body. The surface membrane of the soma and the dendritic tree are specialised for the reception and integration of data, whereas the axon is specialised for the transmission of knowledge within the type of an action potential or a nerve impulse. Types of neurons (8-5) Prosencephalon 1 2 Eye 1 Fourth ventricle Spinal twine Telencephalon Cerebral Corpus cortex striatum 2 Diencephalon Thalamus Hypothalamus � the embryonic brainstem consists at this level of the following parts: (1) the prosencephalon, which supplies rise, as indicated above, to the telencephalon (developing the cerebral cortex and corpus striatum) and the diencephalon (developing the thalamus and hypothalamus); (2) the mesencephalon, which originates the midbrain; and (3) the rhombencephalon, which gives rise to the pons, cerebellum and medulla oblongata. The choroid plexus (formed by a double layer of pia mater called tela choroidea) hangs from the roof of the third ventricle. The ground of the third ventricle consists of the infundibulum, the tuber cinereum, the mammillary our bodies and the higher end of the midbrain. We come again to this portion of the third ventricle in Chapter 18, Neuroendocrine System, once we talk about the hypophysis. Cells migrate to the cortical plate of each hemisphere and form the cerebral cortex. The hippocampus, a cerebral cortex extension from the medial portion of the hemisphere link, advances into the temporal lobe, leaving behind the fornix, a trail of fibers. The concavity of the fornix embraces the choroid fissure (the insertion line of the choroid plexus extending into the lateral ventricle) and the tail of the caudate nucleus (whose head is attached to the thalamus). Consequently, the brainstem consists of three elements: midbrain, pons and medullas oblongata and fibers from the cerebral cortex lengthen on to the brainstem. Fibers extending from the thalamus to the cerebral cortex and fibers from the cortex extending into the brainstem, cut up the corpus striatum into the caudate nucleus and the lentiform nucleus. Multipolar neurons, which show many processes attached to a polygonal-shaped soma. Pyramidal cells of the cerebral cortex and Purkinje cells and neurons of the cerebellar cortex are two typical examples. Embryonically, pseudounipolar neurons derive from bipolar neuroblasts and the two neuronal processes fuse throughout later development (hence the prefix pseudo). Based on the length of the axon relative to the dendritic tree, multipolar neurons may be subclassified into: A. Golgi kind I neurons, when the axon extends beyond the boundaries of the dendritic tree. An space known as the neuropil could be discovered within a nucleus and between the neuronal cell bodies. The term neuropil designates an area with packed dendrites, axonal branches with ample synapses and glial cells. Clusters of neurons organized in a layer type a stratum, lamina or layer (cerebral cortex). When neurons form longitudinal teams, these teams are designated columns (see Box 8-E). Usually, skeletal (skull or vertebral column) defects happen along with malformations of the underlying brain and spinal cord. The latter results from an improper closure of the neural tube throughout neurulation. Congenital malformations associated with faulty neurulation are designated dysraphic (defective fusion) defects. Axons derived from a ganglion are organized as nerves, rami (singular ramus), or roots. Synaptic terminals and synapses (8-6 to 8-8) the synaptic terminal (see 8-6) is specialized for Box 8-D Neuronal migration � Neuronal migration from the intermediate zone to the cortical plate involves three highly regulated steps: (1) a progress cone extending away from the cell physique; (2) a leading neurite extending from the expansion cone and relocation of the centrosome into the neurite; and (3) assembly of microtubules extending from the centrosome toward the nucleus. The nucleus is surrounded by microtubules in a cage-like association and a traction pressure pulls the nucleus toward the centrosome (nucleokinesis). Cortical plate Leading neurite Growth cone Centrosome reposition the transmission of a chemical message in response to an motion potential. The synapse is the junction between the pre-synaptic terminal of an axon and a post-synaptic membrane receptor floor, usually a dendrite. Post-synaptic identifies the receiving aspect (usually dendritic or somatic, typically axonal). The pre-synaptic and post-synaptic membranes are separated by a space: the synaptic cleft. A dense materials coats the internal floor of those membranes: the pre-synaptic and post-synaptic densities. Pre-synaptic terminals contain a lot of membrane-bound synaptic vesicles with neurotransmitter contents (40 to one hundred nm in diameter) and mitochondria. They derive from the neuronal soma and are transported by molecular motor proteins along the axon by an axonal transport mechanism (see 8-7). Pre-synaptic terminals include mitochondria, parts of the sleek endoplasmic reticulum, microtubules and some neurofilaments. Synapses are categorised by their location on the post-synaptic neuron (see 8-8) as follows: 1. The function of the axonal cytoskeleton and motor proteins kinesin and cytoplasmic dynein was discussed in the Cytoskeleton section of Chapter 1, Epithelium Cell Biology. We review the bidirectional anterograde and retrograde transport of cargos along the axon: 1. Axon hillock Nucleolus Nucleus Nissl physique Astrocytes Oligodendrocyte Nissl physique (free ribosomes and tough endoplasmic reticulum) transport of neurotransmitters and mitochondria from the cell body toward the axon terminal and the plus end of microtubules. Cytoplasmic dynein mediates the retrograde axonal transport of development elements and recycling of axon terminal elements from the axon terminal to the cell physique towards the minus finish of microtubules (see Box 8-F). The dendritic floor of many neurons has dendritic spines that additional improve the synaptic floor space. Abundant neurotubules and neurofilaments and elements of the tough endoplasmic reticulum (Nissl bodies) could lengthen into the bottom of the dendrite. Axon hillock Myelin sheath Dendritic backbone Lysosome Soma or cell body Axon the axon arises from the perikaryon in an space devoid of Nissl substance, the axon hillock.
Biaxin 500 mg order visa
Long-term bisphosphonate therapy may be associated with atypical femur fractures; a tentative advice is to restrict therapy to 5 years chronic gastritis gerd 250 mg biaxin discount mastercard. Estrogen decreases the rate of bone reabsorption gastritis healing diet biaxin 500 mg with mastercard, but remedy should be fastidiously weighed within the context of elevated dangers of heart problems and breast most cancers. Teriparatide therapy should be adopted by antiresorptive agent therapy to forestall rapid loss of the newly formed bone. Osteomalacia is attributable to insufficient intake or malabsorption of vitamin D (chronic pancreatic insufficiency, gastrectomy, malabsorption) and issues of vitamin D metabolism (anticonvulsant remedy, continual renal failure, genetic disorders of vitamin D activation or action). Osteomalacia may also be attributable to long-standing hypophosphatemia, which can be because of renal phosphate losing. Proximal muscle weakness is a feature of vitamin D deficiency and should mimic main muscle issues. A lower in bone density is often related to loss of trabeculae and thinning of the cortices. With advancing osteomalacia, hypocalcemia could develop because of impaired calcium mobilization from undermineralized bone. Vitamin D deficiency ought to all the time be repleted at the side of calcium supplementation (1. Serum and urinary calcium measurements are efficacious for monitoring decision of vitamin D deficiency, with a objective of 24-h urinary calcium excretion of 100�250 mg/24 h. Hyperlipoproteinemia is characterized by hypercholesterolemia, isolated hypertriglyceridemia, or both. Diabetes mellitus, weight problems, ethanol consumption, oral contraceptives, glucocorticoids, renal disease, hepatic illness, and hypothyroidism can cause secondary hyperlipoproteinemias or worsen underlying hyperlipoproteinemic states. Cholesterol absorption inhibitors and bile acid sequestrants or nicotinic acid may be required (Table 181-2). When chylomicrons are current, a creamy layer floats to the top of plasma after refrigeration for a quantity of hours. Obesity, hyperglycemia, and hyperinsulinemia are attribute, and diabetes mellitus, ethanol consumption, oral contraceptives, and hypothyroidism might exacerbate the condition. Secondary forms of hypertriglyceridemia ought to be ruled out before making the prognosis of familial hypertriglyceridemia. The identification of different first-degree relatives with hypertriglyceridemia is helpful in making the prognosis. As a outcome, chylomicrons and triglycerides accumulate and trigger manifestations much like these in lipoprotein lipase deficiency. Pts with reasonable hypertriglyceridemia ought to prohibit fats, carbohydrate, and alcohol consumption. In these with familial hypertriglyceridemia, fibric acid derivatives, omega-3 fatty acids, or niacin can be administered if dietary measures are inadequate (Table 181-2). All pts should limit dietary ldl cholesterol and fat and avoid alcohol and oral contraceptives; pts with diabetes ought to be treated aggressively. Pts often current in maturity with xanthomas and untimely coronary and peripheral vascular illness. Cutaneous xanthomas are distinctive, within the type of palmar and tuberoeruptive xanthomas. Comorbidities, similar to diabetes mellitus, obesity, or hypothyroidism, must be optimally managed. Thus, is it crucial that pts with hypercholesterolemia be assessed for cardiovascular danger and for the need for intervention. Lifestyle the primary approach to a pt with hypercholesterolemia and high cardiovascular threat is to make any needed life-style adjustments. Dietary counseling to cut back the content material of saturated fats, trans fat, and ldl cholesterol in the food regimen. The basic medical constellation of hemochromatosis is a pt presenting with bronze pores and skin, liver disease, diabetes, arthropathy, cardiac conduction abnormalities, and hypogonadism. Alcoholic liver disease and continual extreme Fe ingestion can also be associated with a moderate improve in hepatic Fe and elevated body Fe shops. Clinical Features Early signs embrace weak point, lassitude, weight reduction, a bronze pigmentation or darkening of skin, belly ache, and lack of libido. If untreated, liver illness progresses to cirrhosis, and further to hepatocellular carcinoma in 30% of pts with cirrhosis. Diabetes mellitus is extra widespread in pts with a family historical past of diabetes, and hypogonadism could additionally be an isolated early manifestation. Typical signs of portal hypertension and decompensated hepatic cirrhosis may seem late in the scientific course. Diagnosis Serum Fe, % transferrin saturation, and serum ferritin ranges are increased. In an otherwise-healthy person, a fasting serum transferrin saturation >50% is irregular and suggests homozygosity for hemochromatosis. In most untreated pts with hemochromatosis, the serum ferritin level can also be significantly elevated. If either the % transferrin saturation or the serum ferritin degree is abnormal, genetic testing for hemochromatosis should be performed. Liver biopsy may be required in affected people to evaluate possible cirrhosis and to quantify tissue iron. Death in untreated pts results from cardiac failure (30%), cirrhosis (25%), and hepatocellular carcinoma (30%); the latter might develop despite adequate Fe removing. Since 1 unit of blood incorporates 250 mg Fe, and since up to 25 g of Fe should be removed, phlebotomy is carried out weekly for 1�2 years. Less frequent phlebotomy is then used to preserve serum Fe at 9�18 �mol/L (50�100 �g/dL). Chelating brokers corresponding to deferoxamine (infused subcutaneously utilizing a portable pump) remove 10�20 mg iron per day, a fraction of that mobilized by weekly phlebotomy. Chelation remedy is indicated, nonetheless, when phlebotomy is inappropriate, corresponding to with anemia or hypoproteinemia. Each of the 9 major varieties causes a singular pattern of overproduction, accumulation, and excretion of intermediates of heme synthesis. The main manifestations of the hepatic porphyrias are neurologic (neuropathic abdominal ache, neuropathy, and mental disturbances), whereas the erythropoietic porphyrias characteristically trigger cutaneous photosensitivity. Laboratory testing is required to confirm or exclude the varied kinds of porphyria. However, a definite diagnosis requires demonstration of the precise enzyme deficiency or gene defect. It has a prevalence of 1�3 in 100,000 however is much more widespread in certain components of the world (Northern Sweden, Great Britain).
500 mg biaxin buy with amex
A trial of radioiodine ought to be considered before subjecting pts gastritis urination biaxin 500 mg generic, a lot of whom are aged gastritis symptoms how long do they last discount 500 mg biaxin fast delivery, to surgery. Subtotal thyroidectomy provides definitive remedy of goiter and thyrotoxicosis. Pts must be rendered euthyroid with antithyroid drugs before surgical intervention. A thyroid scan offers a definitive diagnostic take a look at, demonstrating focal uptake within the hyperfunctioning nodule and diminished uptake within the the rest of the gland, as exercise of the conventional thyroid is suppressed. Carcinomas of the follicular epithelium include papillary, follicular, and anaplastic thyroid cancer. Medullary thyroid carcinoma arises from parafollicular (C) cells producing calcitonin and should happen sporadically or as a familial disorder, typically in association with multiple endocrine neoplasia type 2. Glandular enlargement might result in compression and displacement of the trachea or esophagus and obstructive signs. Age <20 or >45, male sex, and larger nodule measurement are associated with a worse prognosis. Near-total thyroidectomy is required for papillary and follicular carcinoma and should be performed by a surgeon who is very experienced in the procedure. If threat elements and pathologic features point out the need for radioiodine remedy, the pt should be treated for several weeks postoperatively with liothyronine (T3, 25 �g two to three times a day), adopted by withdrawal for an additional 2 weeks, in preparation for postsurgical radioablation of remnant tissue. This appears to be equally efficient as thyroid hormone withdrawal for radioablation remedy. Following surgical procedure, serum calcitonin provides a marker of residual or recurrent illness. The adrenal cortex produces three main classes of steroids: (1) glucocorticoids, (2) mineralocorticoids, and (3) adrenal androgens. The adrenal medulla produces catecholamines, with excess being caused by a pheochromocytoma (Chap. Clinical Features Some frequent manifestations (central obesity, hypertension, osteoporosis, psychological disturbances, pimples, hirsutism, amenorrhea, and diabetes mellitus) are comparatively nonspecific. More specific findings include easy bruising, purple striae, proximal myopathy, fat deposition within the face and nuchal areas (moon facies and buffalo hump), and barely androgenization. For initial screening, measurement of 24-h urinary free cortisol, the 1-mg in a single day dexamethasone take a look at (8:00 a. Therapy of adrenal adenoma or carcinoma requires surgical excision; stress doses of glucocorticoids have to be given pre- and postoperatively. Metastatic and unresectable adrenal carcinomas are handled with mitotane in doses gradually elevated to 6 g/d in three or 4 divided doses. In some cases, bilateral whole adrenalectomy is required to control hypercorticism. Primary hyperaldosteronism refers to an adrenal trigger and may be due to either an adrenal adenoma or bilateral adrenal hyperplasia. The time period secondary hyperaldosteronism is used when an extraadrenal stimulus for renin secretion is present, as in renal artery stenosis, decompensated liver cirrhosis, or diuretic remedy. Clinical Features Most pts with major hyperaldosteronism have difficult to management hypertension (especially diastolic) and hypokalemia. Edema is characteristically absent, unless congestive coronary heart failure or renal disease is present. Hypokalemia, brought on by urinary potassium loss, might trigger muscle weakness, fatigue, and polyuria, though potassium ranges may be regular in mild main hyperaldosteronism. In pts receiving potassium-wasting diuretics, the diuretic ought to be discontinued and potassium supplements should be administered for 1�2 weeks. If hypokalemia persists after supplementation, screening utilizing a serum aldosterone and plasma renin activity must be performed. Failure to suppress plasma aldosterone after saline or sodium loading confirms main hyperaldosteronism. Failure of aldosterone to suppress under 140 pmol/L (5 ng/dL) is indicative of autonomous mineralocorticoid extra. Alternative checks are the oral sodium loading test (300 mmol NaCl/d for 3 days) or the fludrocortisone suppression take a look at (0. Secondary hyperaldosteronism is treated with salt restriction and correction of the underlying cause. Clinical Features Manifestations embrace fatigue, weak point, anorexia, nausea and vomiting, weight reduction, stomach pain, cutaneous and mucosal pigmentation, salt craving, hypotension (especially orthostatic), and, often, hypoglycemia. Routine laboratory parameters may be regular, but sometimes serum Na is lowered and serum K increased. Serum Na tends to be low due to hemodilution stemming from excess vasopressin secreted in the setting of cortisol deficiency. If the response is irregular, then main and secondary deficiency could additionally be distinguished by measurement of aldosterone from the same blood samples. In secondary, but not main, adrenal insufficiency, the aldosterone increment from baseline might be normal (5 ng/dL). In these pts, alternative testing (metyrapone test or insulin tolerance testing) can be utilized for prognosis. Some pts benefit from doses administered three times day by day, and other glucocorticoids could also be given at equal doses. Mineralocorticoid supplementation is usually wanted for primary adrenal insufficiency, with administration of zero. Doses must be titrated to normalize Na and K levels and to keep normal blood pressure with out postural changes. All pts with adrenal insufficiency should be instructed in the parenteral self-administration of steroids and should be registered with a medical alert system. During durations of intercurrent sickness, the dose of hydrocortisone should be doubled. Thereafter, if the pt is improving and is afebrile, the dose may be tapered by 20�30% daily to ordinary alternative doses. In pts with hypertension, delicate renal insufficiency, or congestive coronary heart failure, an alternate method is to cut back salt intake and to administer furosemide. The first step in analysis is to determine the practical standing by measurement of plasma free metanephrines to screen for pheochromocytoma. Children and adolescents also have gotten extra overweight, indicating that the present developments will speed up over time. Obesity is related to an elevated danger of multiple health problems, together with hypertension, kind 2 diabetes, dyslipidemia, obstructive sleep apnea, nonalcoholic fatty liver disease, degenerative joint disease, and a few malignancies. Furthermore, regional fats distribution may influence the risks related to obesity. [newline]Central (primarily visceral) obesity (high ratio of the circumference of the waist to the circumference of the hips [waist-to-hip ratio], >0. Excess accumulation of physique fats is the consequence of environmental and genetic components; social elements and economic conditions also symbolize essential influences. The current enhance in obesity could be attributed to a mix of extra caloric consumption and decreasing physical activity.
Gur-Mar (Gymnema). Biaxin.
- What is Gymnema?
- Are there any interactions with medications?
- Are there safety concerns?
- Diabetes, metabolic syndrome, weight loss, stimulating digestion, malaria, cough, snake bites, softening the stool (laxative), and increasing urine excretion (diuretic).
- How does Gymnema work?
- Dosing considerations for Gymnema.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96816
Biaxin 500 mg discount with visa
The direct supply of blood to the adrenal medulla gastritis diet food recipes cheap 250 mg biaxin with amex, concerned in fast responses to stress viral gastritis symptoms biaxin 500 mg cheap line. The adrenal cortex and medulla are drained by the central vein, current in the adrenal medulla. The ventral pancreas varieties the head of the pancreas and associates with the widespread bile duct. Endocrine cells are first observed along the base of the differentiating exocrine acini by weeks 12 to sixteen. Islets of Langerhans (19-15 and 19-16) Dual blood provide: Acinar and insuloacinar vascular methods Each islet of Langerhans is provided by afferent arterioles, forming a network of capillaries lined by fenestrated endothelial cells. Venules leaving the islet supply blood to the pancreatic acini surrounding the islet. This vascular system enables a neighborhood action on the exocrine pancreas of hormones produced within the islet. An unbiased arterial system, the acinar vascular system, supplies the pancreatic acini. Insuloacinar portal system Arteriole Islet of Langerhans Venule Acinar vascular system Pancreatic acini the pancreas has two parts: 1. The exocrine pancreas, consisting of acini involved in the synthesis and secretion of several digestive enzymes transported by a duct system into the duodenum (see Chapter 17, Digestive Glands). The endocrine pancreas (2% of the pancreatic mass), formed by the islets of Langerhans scattered throughout the pancreas. A vascular part, the insuloacinar portal system (see 19-15), which consists of an afferent arteriole giving rise to a capillary network lined by fenestrated endothelial cells. Venules leaving the islets of Langerhans supply blood to adjacent pancreatic acini. Islets of Langerhans A cells secrete glucagon and are primarily situated at the periphery of the islet Exocrine pancreas Endocrine cells forming cords Vascular spaces (sinusoids) D cells produce gastrin and somatostatin (shown) F cells secrete pancreatic polypeptide B cells, the predominant cell kind, secrete insulin and are found within the core of the islet Immunohistochemistry panels from Mart�n-Lacave I, Garc�a-Caballero T: Atlas of Immunohistochemistry. Proinsulin consists of a connecting (C) peptide certain to A and B chains, held collectively by disulfide bonds. Within the secretory vesicle, the protease releases the C peptide from the disulfide-linked A and B chains. Ca2+ influx causes exocytosis of the secretory vesicle and the release of insulin into the bloodstream. An impartial vascular system, the acinar vascular system, provides blood directly to the exocrine pancreatic acini. Anastomosing cords of the endocrine cells A (cells), B (cells), D (cells) and F cells, every secreting a single hormone (see 19-16). A cells (cells) produce glucagon, B cells synthesize insulin, D cells secrete gastrin and somatostatin and F cells produce pancreatic polypeptide. Electron microscopy, to distinguish the size and structure of the secretory granules. B cells are centrally positioned (core distribution) and surrounded by the opposite cell varieties (mantle distribution). Peptides produced by cells of the islets of Langerhans (19-17) of gastrin from enteroendocrine cells, the secretion of pancreatic bicarbonate and enzymes and the contraction of the gallbladder. Pancreatic polypeptide is a 36-amino-acid peptide, which inhibits the secretion of somatostatin. Pancreatic polypeptide also inhibits the secretion of pancreatic enzymes and blocks the secretion of bile by inhibiting contraction of the gallbladder. Cell entry and fate of insulin (19-18) A cells (cells produce glucagon, a 29-amino-acid peptide (3. Glucagon derives from a big precursor, preproglucagon, encoded by a gene current on chromosome 2. About 30% to 40% of glucagon in blood is produced by the pancreas; the remainder comes from the gastrointestinal tract (enteroglucagon). Circulating glucagon, of pancreatic and gastrointestinal origin, is transported to the liver and about 80% is degraded earlier than reaching the systemic circulation. Insulin derives from a large singlechain precursor, preproinsulin, encoded by a gene located on the brief arm of chromosome 11. The large precursor offers rise to proinsulin, consisting of C peptide linking two chains, A and B chains. An improve in blood glucose stimulates the release of insulin and C peptide saved in secretory granules. Removal of C peptide by particular proteases ends in the separation of chains A and B. D (cells produce gastrin (see dialogue of enteroendocrine cells in Chapter 15, Upper Digestive Segment) and somatostatin. Somatostatin is a 14-amino-acid peptide equivalent to somatostatin produced in the hypothalamus. Hepatic insulin action, consisting of the suppression of gluconeogenesis and glycogenolysis. These actions be positive that part of dietary glucose is saved in hepatocytes and launched between meals or when metabolic calls for happen. About 50% of insulin arriving to the liver by the portal vein is degraded during the first clearance spherical. A second insulin clearance spherical takes place when insulin returns via the hepatic artery and reaches the hepatic sinusoids for degradation in hepatocytes. In addition to the primary and second clearance cross through the liver, circulating insulin is internalized and degraded in the convoluted tubules of the nephrons in the kidneys. Cell entry and fate of glucose (19-19) the principle motion of insulin on peripheral tissues is the regulation of glucose metabolism. The function is to store glucose and triglycerides to fulfill the energetic needs of a tissue, similar to muscle or adipose tissue. Insulin returns to the liver via the hepatic artery for a second clearance spherical. An excessive amount of glucose circulating in blood is seen when hepatocytes, skeletal muscle and adipocytes fail to take up glucose due to reducing mass or operate of insular B cells and/or elevated insulin resistance. The intracellular area of the subunit has tyrosine kinase activity, which autophosphorylates and triggers a selection of intracellular responses. Normally, thymocytes that acknowledge self-antigens are eradicated as they mature in the thymus. Increases in circulating glucose and lipid ranges can further affect insulin secretion and motion. The capability of adipose cells to retailer excess lipids is saturated in weight problems and in response to high-fat diets. Lipids are redistributed to skeletal muscle, coronary heart and liver, thus contributing to insulin resistance.
Purchase biaxin 250 mg without a prescription
The goal is to forestall the binding of pathogenic bacteria with out interfering with the endogenous bacterial flora by the use of antibiotics gastritis from not eating biaxin 250 mg best. Gastroenteroendocrine cells (15-18) Gastroenteroendocrine cells gastritis zucchini 500 mg biaxin cheap otc, together with the epithelial lining, the enteric nervous system and the immune system regulate the physiology of the gastrointestinal tract in well being and disease. Peptide hormones derive from gastroenteroendocrine cells and neuroendocrine mediators produced by neurons. Peptide hormones are synthesized by gastroenteroendocrine cells dispersed throughout the mucosa from the stomach by way of the colon. The inhabitants of gastroenteroendocrine cells is so giant that the gastrointestinal section is considered the largest endocrine organ in the physique. Gastrin-releasing peptide is launched by postsynaptic neurons activated by stimulation of the vagus nerve. Peptide hormones produced by gastrointestinal endocrine cells have the next basic features: 1. Secretin is released by cells within the duodenal glands of Lieberk�hn when the gastric contents enter the duodenum. Three types of gastrin have been described: little gastrin, or G17 (which incorporates 17 amino acids); big gastrin, or G34 (which accommodates 34 amino acids); and minigastrin, or G14 (which consists of 14 amino acids). Amines are a part of polypeptide hormones that can stimulate or inhibit target cell perform. Gastrinreleasing peptide three Postsynaptic neuron To goal cell Vagus nerve four Vagal stimulation of the pyloric antrum causes the release of gastrin-releasing peptide from postsynaptic neurons that stimulate directly the release of gastrin from G cells present in the antrum. Histamine potentiates the impact of acetylcholine and gastrin on the secretion of hydrochloric acid by parietal cells. Gastrin has a trophic effect on the mucosa of the small and enormous gut and the fundic area of the abdomen (see Box 15-E). Histamine H2 receptor�blocking medicine (such as cimetidine [Tagamet] and ranitidine [Zantac]) are effective inhibitors of acid secretion. The pits are deeper than in the cardiac glands and gastric glands of the fundus-body area. At the distal finish, the contents of the mucus-secreting cells displace and flatten the nuclei to the basal area of the cell. Abundant lymphocytes and plasma cells are seen within the lamina propria Mucosa Muscularis mucosae the continuity of the pyloric glands is difficult to visualize in histologic sections due to their tortuous path and highly branched nature. Note the basal position of the skinny nuclei and the light staining of the cytoplasm, reflecting the content of mucus. Muscularis mucosae Deep pit lined by mucus-secreting cells stimulates gastrointestinal motility. A neural control difficulties in early infancy, followed by obesity and mechanism regulates the release of motilin. Ghrelin binds to its receptor, present in growth hormone�secreting cells of the adenohypophysis, and Pyloric area of the stomach (15-19) stimulates the secretion of growth hormone. Pyloric glands differ from the cardiac and gastric Ghrelin plasma levels increase during fasting, trig- glands in the following layers: gering starvation by appearing on hypothalamic feeding 1. Pyloric glands have a larger lumen and are Prader-Willi syndrome (caused by abnormal gene extremely branched. Severe hypotonia and feeding loric gland is a mucus-secreting cell that resembles the mucous neck cells of the gastric glands. Most of the cell contains large and pale secretory Box 15-E Zollinger-Ellison syndrome mucus and secretory granules containing lysozyme, � Patients with gastrin-secreting tumors (gastrinomas, or Zollinger-Ellison syna bacterial lytic enzyme. Occasionally, parietal cells drome) display parietal cell hyperplasia, mucosal hypertrophy of the fundic area of may be discovered within the pyloric glands. Gastrinoma is extra frequent in males than in women In contrast to the cardiac opening of the stomand the age at onset is generally between forty and fifty five years of age. The sphincter separates the � the complications of gastrinomas are fulminant abdomen ulceration, diarrhea (caused acid-pepsin content material of the stomach from the alkaby an inhibitory impact of excessive gastrin on water and sodium reabsorption in the small line duodenal surroundings containing pancreatic intestine), steatorrhea (as the outcomes of pancreatic lipase inactivation in the duodenum secretions and bile. Its capabilities are ingestion, partial digestion and lubrication of the meals, or bolus. The mouth contains the lips, cheeks, enamel, gums (or gingivae), tongue, uvula and hard and soft palate. The oral cavity is lined by three types of mucosae with structural variations: (1) Lining mucosa (lips, cheeks, ventral floor of the tongue, soft palate, flooring of the mouth and alveolar mucosa). There are three transition sites of the oral mucosa: (i) the mucocutaneous junction (between the skin and the mucosa of the lips). Lips encompass three regions: (1) the cutaneous area (thin pores and skin; keratinized stratified squamous epithelium with hair follicles and sebaceous and sweat glands). The lamina propria binds to the periosteum of the alveolar processes of the maxilla and mandible. Collagenous fibers within the submucosa bind the mucosa to the periosteum of the onerous palate. The taste bud and uvula are lined by non-keratinizing stratified squamous epithelium extending into the oropharynx. The dorsal surface of the tongue is covered by non-keratinizing stratified squamous epithelium supported by a lamina propria associated with a skeletal muscle core. There are 4 forms of lingual papillae: (1) Filiform papillae, probably the most plentiful; the one sort of papilla without taste buds. Their ducts open into the crypts and furrows of the lingual tonsils and circumvallate papillae, respectively. Tastants (sweet, bitter, bitter, salty and umami) enter by way of the style pore and bind to style receptors (type 1 receptors, designated T1Rs) present in apical microvilli of taste receptor cells. An influx of Na+ inside taste cells causes depolarization of the style receptor cells. Cementum is associated with the periodontal ligament, firmly hooked up to the alveolar bone. A central chamber, the pulp, opens at the apical foramen, the site the place blood vessels, nerves and lymphatics enter and leave the pulp chamber. The ectoderm (ameloblasts), cranial neural crest (odontoblasts) and mesenchyme (cementocytes) contribute to tooth development. The levels of tooth improvement are: (1) Bud stage: Ectodermic epithelial cells to proliferate and type the epithelial tooth bud. The bud of the everlasting tooth develops from the dental lamina and stays dormant. Odontoblasts produce predentin (non-mineralized material surrounding the apical processes of the odontoblast) and dentin (consisting of 20% natural material, primarily kind I collagen; 70% inorganic materials; and 10% water). Mineralized dentin (crystals of hydroxyapatite and fluoroapatite) types the dentinal tubes containing the odontoblast apical processes. Ameloblasts, current within the growing tooth solely, face the dentin materials and secrete enamel. The extracellular matrix of the developing enamel (amelogenesis) accommodates two lessons of proteins: amelogenin (90%) and non-amelogenins (10%), together with enamelin and ameloblastin.
250 mg biaxin discount overnight delivery
Minor neuroimaging criteria Obstructive hydrocephalus or abnormal enhancement of basal leptomeninges three gastritis zucchini 250 mg biaxin generic free shipping. Major clinical/exposure standards Detection of specific anticysticercal antibodies gastritis diet oatmeal cookies buy 250 mg biaxin mastercard. Minor clinical/exposure criteria Clinical manifestations suggestive of neurocysticercosis Individuals coming from or living in an space the place cysticercosis is endemic Diagnosis is confirmed by one absolute criterion, by two major criteria or one major and one confirmatory neuroimaging standards plus any clinical/exposure criterion, or by one major neuroimaging criterion plus two clinical/exposure criteria (including at least one major clinical/exposure criterion), along with the exclusion of other pathologies producing related neuroimaging findings. A possible analysis is supported by one major neuroimaging criterion plus any two clinical/exposure standards or by one minor neuroimaging criterion plus at least one main clinical/exposure criterion. Larvae become fluid-filled unilocular hydatid cysts inside which daughter cysts develop, as do germinating cystic constructions (brood capsules). Expanding cysts exert the results of space-occupying lesions, inflicting symptoms in the affected organ (usually liver and lung); the liver is concerned in two-thirds of E. Compression of a bile duct could mimic biliary illness, and rupture or leakage from a hydatid cyst could trigger fever, pruritus, urticaria, eosinophilia, or anaphylaxis. Symptoms are rare and normally gentle, but infection, significantly in Scandinavia, may cause vitamin B12 deficiency because the tapeworm absorbs large quantities of vitamin B12 and interferes with ileal B12 absorption. Up to 2% of contaminated pts, particularly the elderly, have megaloblastic anemia resembling pernicious anemia and might suffer neurologic sequelae as a outcome of B12 deficiency. These organisms can inflict direct injury, elicit hypersensitivity, or inoculate toxins or pathogens. Burrows appear as darkish wavy lines (3�15 mm in length), with most lesions positioned along the digital internet spaces or on the volar wrists, elbows, scrotum, and penis. Bedding and clothing must be washed in scorching water and dried in a heated dryer, and shut contacts (regardless of symptoms) must be treated to prevent reinfestations. Eggs are cemented firmly to hair or clothing, and empty eggs (nits) stay affixed for months or years after hatching. Head lice are transmitted amongst schoolchildren and body lice amongst catastrophe victims and indigent people; pubic lice are normally transmitted sexually. The body louse is a vector for the transmission of diseases such as louse-borne typhus, relapsing fever, and trench fever. In this infestation, maggots invade dwelling or necrotic tissue or body cavities and produce scientific syndromes that vary with the species of fly. Certain flies are attracted to blood and pus, and newly hatched larvae enter wounds or diseased pores and skin. Pts sometimes develop sepsis from Aeromonas hydrophila, which colonizes the gullets of commercially available leeches. Examine stomach for evidence of hepatomegaly, ascites, or stomach aortic aneurysm. S1, first heart sound; S2, second coronary heart sound; A2, aortic element of the second heart sound; P2, pulmonic component of the second heart sound. Midsystolic Clicks At lower left sternal border and apex, often followed by late systolic murmur in mitral valve prolapse. Diastolic Murmurs � Early diastolic murmurs: Begin immediately after S2, are high-pitched, and are usually caused by aortic or pulmonary regurgitation. Graphic representation of the systolic pressure gradient (green shaded area) between left ventricle and aorta in pt with aortic stenosis. Left-sided murmurs and sounds usually are louder during expiration, as is the pulmonic ejection sound. Following launch of the Valsalva maneuver, right-sided murmurs are most likely to return to control intensity earlier than left-sided murmurs. Left-sided S4 and S3 are often accentuated by exercise, significantly when due to ischemic coronary heart disease. Chronic processes: cardiomyopathy, amyloid, sarcoid, scleroderma, myocardial tumor Ventricular hypertrophy/enlargement 1. Wolff-Parkinson-White patterns Small or absent R waves in the right to midprecordial leads. Imaging could also be compromised in pts with persistent obstructive lung illness, thick chest wall, or slender intercostal spaces. Upper: Parasternal long axis view during systole and diastole (left) and systole (right). Lower: Parasternal quick axis view throughout diastole (left) and systole (right) demonstrating a lower in the left ventricular cavity dimension throughout systole in addition to an increase in wall thickness. Severity of valvular stenosis is measured by Doppler (peak stress gradient = 4 � [peak velocity]2); valve areas are calculated using further Doppler techniques. Yield of figuring out cardiac source of embolism is low in the absence of cardiac history or physical findings. Nuclear imaging is extra sensitive, however less particular, than stress echocardiography for detection of ischemia. It is most helpful in analysis of suspected coronary anatomic anomalies and to exclude high-grade coronary stenoses in pts with chest pain and intermediate pretest chance of coronary artery disease. Table 114-2 summarizes key diagnostic features of the noninvasive imaging modalities. Physical Examination Wide, fastened splitting of S2, systolic murmur from move throughout pulmonic valve, attainable diastolic circulate rumble across tricuspid valve, prominent jugular venous v wave. Echo distinction (agitated saline injection into peripheral systemic vein) might visualize transatrial shunt. Physical Examination Holosystolic murmur at decrease left sternal border, which may be accompanied by a palpable thrill, loud P2; diastolic flow murmur throughout mitral valve. Therapeutic choices are restricted and embody pulmonary artery vasodilators (see Chap. May go undetected in youth or suspected by the presence of a systolic ejection click; usually identified throughout echocardiography that was obtained for one more purpose. Usually asymptomatic, however could cause headache, fatigue, or claudication of decrease extremities. Physical Examination Hypertension in higher extremities; delayed femoral pulses with decreased strain in decrease extremities. Systolic murmur is best heard over the higher again on the left interscapular area. Continuous murmur over the scapula can also be current as a outcome of collateral blood move. Echocardiography Can delineate site and size of coarctation, and Doppler determines the strain gradient across it. Recurrent coarctation after surgical restore may be amenable to percutaneous balloon dilatation. Repaired congenital coronary heart illness with residual defects adjacent to web site of a prosthetic patch or transcatheter device 3.
Cheap biaxin 250 mg without prescription
The dense line terminates when the membrane surfaces separate to enclose the cytoplasm on the surface of the sheath (the tongue) and the intraperiod line terminates because the tongue turns away from the sheath gastritis emedicine biaxin 250 mg overnight delivery. They correspond to areas of residual cytoplasm gastritis pain remedy buy 250 mg biaxin with amex, preserving the viability of myelin. As the myelin sheath approaches the node of Ranvier region, an extra ring of cytoplasm separates the cytoplasmic surfaces of the cell membrane. These tongues make contact with the axolemma, or floor membrane of the axon, within the paranodal region. The apposed interdigitating processes of myelinating Schwann cells and the incisures of SchmidtLanterman are linked by tight junctions. They are known as autotypic tight junctions as a end result of they link plasma membranes of the same cell. Tight junctions include a number of proteins, together with claudin-1, claudin-2 and claudin-5 and zonula occludens-1 and zona occludens-2. Cx32 is concentrated in the paranodal area and the incisures of Schmidt-Lanterman. Mutations within the Cx32 gene determine the demyelinating X-linked Charcot-Marie-Tooth disease. Internal mesaxon 3 the spiral is extra extensive and the plasma membranes of the Schwann cell are intently packed. Two apposed parts of the Schwann cell membrane form the interior and exterior mesaxon. Central nervous system Inner leaflets Cytoplasm Major dense line (close apposition of the two inner leaflets) the most important dense line denotes the close apposition of the inner leaflets of the plasma membrane of an oligodendrocyte or Schwann cell. The intraperiod line represents the closely apposed (but not fused) outer leaflets of the spirally wrapped plasma membrane of an oligodendrocyte or Schwann cell. Axolemma Axon Outer leaflets Extracellular area Inner leaflets Cytoplasm Intraperiod line (close apposition of the two outer leaflets) Electron micrographs courtesy of Ilya I. Heterotypic tight junctions are seen between the axolemma (surrounding the axon) and the Schwann cell paranodal cytoplasmic loops adjacent to the node of Ranvier. Instead, Cx32 predominates within the paranodal membranes and incisures of SchmidtLanterman and varieties intercellular channels linking parts of the identical cell. Cytoplasm (major dense line) Two extracellular loops Four transmembrane domains N-terminal and C-terminal intracellular tails Three proteins are significantly relevant: 1. The illness is most often an autosomal-dominant syndrome but is genetically heterogeneous. Charcot-Marie-Tooth disease sort 2 is an axonal polyneuropathy (with normal nerve conduction velocity) determined by defects in axonal transport (mutation of a kinesin), membrane trafficking and protein synthesis. The commonest characteristics of PelizaeusMerzbacher disease are flickering eyes and physical and psychological developmental disabilities. The homotetrameric structure offers intermembrane adhesion important for the compaction of myelin. Unmyelinated nerve fibers (8-13) Unmyelinated axons predominate within the gray matter. Each Schwann cell is prepared to house a variety of axons occupying individual invaginations of its cytoplasm. The complete axolemma of such axons is freely uncovered to the interstitial tissue, and axons are partially protected by a basal lamina surrounding the supportive Schwann cell. Nerve impulses alongside these axons travel repeatedly and, subsequently, much less quickly than saltatory conduction. A Schwann cell can accommodate a number of axons in individual cytoplasmic invaginations or pockets and no myelin is produced. In myelinated nerves, impulse conduction is confined to the nodes of Ranvier, leaping (saltatory) from node to node at a maximum velocity of a hundred and twenty m/s. The impulse conduction in unmyelinated nerves is steady, with a lowered maximum velocity of 15 m/s). Demyelinating diseases can be immune-mediated, inherited, metabolic and virus-induced. Immune-mediated demyelinating ailments embody a quantity of sclerosis and monophasic demyelinating illnesses (for instance, optic neuritis). Two attribute pathologic findings are the a number of sclerosis plaque, a demyelination lesion of the white matter, and Creutzfeldt cells, reactive astrocytes with several nuclear fragments. Adrenoleukodystrophy is an inherited X-linked demyelination dysfunction characterised by progressive demyelination related to dysfunction of the adrenal cortex. Progressive weaknes and stiffness within the legs (paraparesis), appear in early adulthood and center age. Metabolic demyelination issues embody central pontine myelinolysis, a syndrome during which neurologic dysfunction is observed following fast correction of hyponatremia in people with alcohol abuse or malnutrition. A typical pathologic discovering could be symmetrical demyelinated lesions in the central pons, a very vulnerable space of the brain stem. Degenerative processes of particular teams of neurons of the brain cause motion problems, dementia syndromes and autonomic perturbations. It is characterized by progressive degeneration of motor neurons, beginning with moderate weak point in one limb and progressing to severe paralysis (swallowing and respiratory disorders), resulting in demise in about 3 years. Lateral sclerosis refers to the hardness to palpation of the lateral columns of the spinal wire. The accumulation of plaques within the extracellular house consisting of amyloid (Greek amylon, starch; eidos, resemblance) fibrils containing -amyloid (A) peptide. Amyloid fibrils have a predominant -sheet construction forming unfolded or partially unfolded conformations of proteins and peptides. Historically, amyloidosis was observed within the mid19th century as iodide or Congo red�stained deposits in organs of sufferers who died from this situation. Amyloid fibrils symbolize the loss of function of normally soluble, functional peptide and proteins in addition to the self-assembly of poisonous intermediates. Keep in thoughts that the protecting mechanisms in opposition to amyloid formation include the housekeeping ubiquitin�proteasome and autophagy techniques, which forestall the formation and accumulation of misfolded and aggregated polypeptide chains. Two reactive astrocytes (Creutzfeldt cells) with a quantity of nuclear fragments are seen (hematoxylin�eosin, H&E). In addition, vascular damage (ischemia) and parenchymal irritation (activated microglia and reactive astrocytes) improve the results of A peptide�containing plaques in the brain. Alterations within the stabilizing perform of tau, a microtubule-associated protein, result in the accumulation of twisted pairs of tau in neurons. In regular neurons, soluble tau promotes the meeting and stability of microtubules and axonal vesicle transport. Hyperphosphorylated tau is insoluble, lacks affinity for microtubules and self-associates into paired helical filaments. Demyelinization Spinal nerve White matter Clustered Ventral horn with motor neurons pseudounipolar neurons Symmetrical lack of myelinated fibers in a piece of spinal twine (crossed cerebrospinal tracts) from a patient with amyotrophic lateral sclerosis.
Buy cheap biaxin 250 mg online
In this preparation stained with orcein gastritis diet natural remedies generic 500 mg biaxin, dark blue�stained elastic fibers are seen alongside the wall of the terminal bronchiole and the respiratory bronchiole as nicely as in the wall of a department of the pulmonary artery (tunica interna and adventitia) diet for chronic gastritis patients biaxin 250 mg buy cheap on line. The lining epithelium of the terminal bronchiole incorporates membership cells (Clara cells) tough to resolve at low magnification. The intrapulmonary segmentation ends in the organization of a pulmonary lobule and a pulmonary acinus. Pulmonary lobule and pulmonary acinus (13-9 and 13-10) A terminal bronchiole and the associated region of pulmonary tissues that it supplies constitute a pulmonary lobule (see 13-9). A pulmonary lobule includes the respiratory bronchioles, alveolar ducts, alveolar sacs and alveoli. The pulmonary acinus, the unit of fuel exchange of the lung, is provided by a respiratory bronchiole. Emphysema is permanent enlargement of the air spaces distal to the terminal bronchioles, related to the destruction of their walls. The respiratory bronchiole and the preliminary portion of the alveolar duct show an interrupted wall with typical clean muscle knobs and scattered elastic fibers bulging into the lumen (see 13-9 and 13-10). At the distal finish of the alveolar duct, the sleek muscle knobs disappear and the lining epithelium is primarily sort I alveolar epithelial cells. At the alveolar duct, muscle knobs are lined by alveolar capillaries, which, in turn, are lined initially by sort I alveolar cells. Following airway injury, club cells proliferate and migrate to replenish alveolar epithelial cells. In addition, proliferative club cells can produce ciliated cells and additional membership cells. Respiratory portion of the lung (13-12) Terminal bronchioles give rise to three generations of respiratory bronchioles (0. Respiratory bronchioles are the transition from the conducting to the respiratory portion of the lung. The alveolus (13-13 to 13-15; see 13-10 and 13-12) About 300 million air sacs, or alveoli, in every lung provide a complete surface area of 75 m2 for oxygen and carbon dioxide exchange. The alveolar epithelium is composed of two distinct cell types (see 13-12 and 13-13): 1. They derive from bone-marrow monocytes and are regularly seen in the alveolar lumen and interstitium. Alveolar dendritic cells (see 13-15), actively monitor the alveolar air area for antigens and take them up for presentation to T cells. After airway harm, club cells can proliferate to regenerate the bronchiolar epithelium and even migrate to replenish alveolar epithelial cells. At the electron microscope degree, the apical dome-shaped area of club cells incorporates cytoplasmic dense secretory granules, mitochondria and numerous vesicles. Alveolus Alveolus uct ar d eol Alv Ciliated cell Alveolus Obliterative bronchiolitis or constrictive bronchiolitis Peribronchiolar inflammatory cell infiltrate the histologic sample of obliterative bronchiolitis of a terminal bronchiole is compatible with irregular tissue repair and irritation in response to tissue harm, including deficient epithelial regeneration, peribronchiolar fibroproliferation and continual Reduction of the inflammatory cell infiltrate. Obliterative bronchiolitis is a frequent complication Peribronchiolar fibrosis of hematopoietic stem-cell transplantation or lung transplantation. Remnants of the muscle knobs lined by a low cuboidal-to-squamous easy epithelium may be seen at the alveolar openings. Air flow three Saccular outpocketings 2 Muscle knob: Smooth muscle cell bundles (muscle knobs), innervated by parasympathetic nerve fibers, contract to constrict the lumen of the bronchiole. In bronchial asthma, muscle contraction, triggered by histamine launch from mast cells, is persistent. In addition to capillaries, the interstitium contains elastic and collagen fibers produced by interstitial fibroblasts. Alveolar cells are separated from capillary endothelial cells by the associated basal laminae produced by them. Multiple small perivascular lymphatics are responsible for maintaining fluid balance in the alveolar interstitium. The cytoplasm shows dense membrane-bound lamellar bodies, representing secretory granules containing pulmonary surfactant. Surfactant is released by exocytosis and spreads over a thin layer of fluid that usually coats 464 the alveolar surface (see 13-16). By this mechanism, the pulmonary surfactant lowers the surface pressure on the air-fluid interface and thus reduces the tendency of the alveolus to collapse on the end of expiration. As previously indicated, club cells, positioned in terminal bronchioles, also secrete pulmonary surfactant. Alveolar macrophages are important for catabolizing the surfactant that lines the surface of the alveoli. There are two completely different sources of alveolar macrophages: (1) Self-renewal macrophages derived from a fetal yolk sac progenitor. Alveolar capillaries type an interconnected community round alveoli and are lined by steady endothelial cells, associated with one another by occluding junctions. The endothelial basal lamina fuses with the basal lamina of the alveolar epithelium, where the alveolar capillary is intently related to the alveolar wall (the favorable website for gasoline exchange). At this web site, fluids can move from capillaries to the interstitium, to drain eventually into para-alveolar lymphatics adjoining to an arteriolar wall similar to branches of the pulmonary or bronchial arteries. In patients with heart illness, alveolar macrophages include many vacuoles crammed with hemosiderin, resulting from phagocytosis of pink blood cells and degradation of their hemoglobin. Alveolar macrophages are sentinel cells migrating over the luminal surface of the alveolus. These cells monitor any inhaled dust or micro organism that will have escaped entrapment by the mucous lining within the airway. When stimulated by metabolic merchandise of bacteria, macrophages launch chemotactic components that induce transendothelial migration of leukocytes, which join macrophages to neutralize invading microorganisms. An excess of asbestos (composed of silica, iron, sodium, magnesium and other metals) causes macrophages to launch chemical agents, producing alveolitis and eventual fibrosis of Alveolar the lung. Surfactant turnover is facilitated by the phagocytic operate of alveolar macrophages. Macrophages can take up inhaled asbestos and trigger asbestosis (interstitial pulmonary fibrosis; see 13-17), the deposition of collagen and asbestos our bodies. The subsequent step is to explore how normal construction and function of the airways are disrupted throughout illness. Asthma, to emphasize how mucus hypersecretion and bronchoconstriction interface with the immune system. Chronic bronchitis and emphysema, to strengthen the idea of pulmonary lobule and pulmonary acinus by exploring two examples of persistent obstructive pulmonary illness. Acute respiratory distress syndrome, to stress how a broken alveolar air-blood barrier leads to severe medical situations. Asthma can be triggered by repeated antigen publicity (allergic asthma) or by an abnormal autonomic neural regulation of airway perform (non-allergic asthma). The basic symptoms of bronchial asthma are wheezing, cough and dyspnea (shortness of breath). The luminal obstruction of airways by mucus, caused by hypersecretion of bronchial mucous glands and goblet cells, together with bronchiolar constriction. Vasodilation of the bronchiolar microvasculature with increased vascular permeability and edema.