
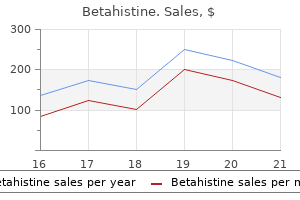
Betahistine dosages: 16 mg
Betahistine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

Betahistine 16mg online
It is crucial that sufferers identified by the screening program receive a rapid symptoms low blood sugar 16 mg betahistine cheap overnight delivery, accurate treatment ibs 16 mg betahistine purchase free shipping, and definitive prognosis because the medical implications and therapies for the assorted forms of hyperphenylalaninemia are totally different. All genetic types of hyperphenylalaninemia are attributable to defects that immediately or indirectly affect the activity of the enzyme phenylalanine hydroxylase. Treatment ought to start inside the first month of life to keep away from irreversible neurologic harm. When began early, remedy is mostly efficient in stopping the long-term neurologic sequelae of this disease. However, commonplace remedy appears unable to stop extra subtle mental and behavioral disabilities. They seem to tolerate a higher dietary protein consumption while sustaining acceptable serum phenylalanine concentrations. Many new child infants now go home from the hospital before 24 hours of age, thereby creating issues for screening packages. Screening before 24 hours will increase the chance of a false-negative end result, whereas delaying screening until after discharge will increase the danger of poor compliance. If the plasma phenylalanine concentration and the plasma phenylalanineto-tyrosine ratio are increased, the patient should be positioned on a low-phenylalanine diet. The most common medical presentations are listed in Table 99-3, together with a differential diagnosis of the classes of metabolic disorders that may be related to every presentation. She also has an elevated danger of getting a child with main start anomalies, together with intrauterine growth restriction, microcephaly, psychological retardation, and a congenital coronary heart defect, as properly as a broad vary of minor anomalies. It usually produces a extreme coagulopathy, hypoglycemia, and fulminant hepatic failure. Women with either of these problems improve remarkably after supply, suggesting that the fetus is causing a toxic effect on the mother that resembles that seen in patients with inborn errors of fatty acid oxidation. Long-chain 3-hydroxyacylCoA dehydrogenase deficiency may be seen as an isolated deficiency or as part of trifunctional protein deficiency that affects all three enzyme actions. The fetus, in flip, is at risk for vital postnatal issues related to its enzyme deficiency. There are, nevertheless, a number of groups of issues that include significant exceptions: congenital disorders of glycosylation, fatty acid -oxidation issues, respiratory chain issues, neurotransmitter problems, and peroxisomal issues (see Dysmorphic Syndromes). Although most of the medical disorders that affect the growing fetus are mentioned later, the disorders that may result in congenital ascites or hydrops fetalis are discussed here. The neurologic difficulties, such as altered consciousness (encephalopathy), altered tone, or seizures, are mentioned elsewhere on this e-book (see Chapters 59 and 62). As noted in these chapters, these neurologic difficulties are most commonly brought on by an infection, mind malformations, or hypoxemicischemic encephalopathy, and less generally by inborn errors of metabolism. The distinction between these two teams is somewhat arbitrary because patients with a disorder that produces metabolic encephalopathy typically have seizures, and conversely, patients with a dysfunction that produces metabolic seizures typically have encephalopathy. Nevertheless, the excellence is helpful because sufferers usually fall extra easily into one group than the other. A number of specific metabolites are overproduced because of a selected enzyme deficiency. In extra, these metabolites serve as endogenous toxins that impair other metabolic or physiologic processes. Disruption of these processes leads, in turn, to production of additional metabolites, which further impair cellular processes. Early interruption of the cascade via such relatively easy measures as fluid and caloric support may abort episodes of metabolic decompensation. Physicians who care for kids who present with a metabolic dysfunction in late infancy, childhood, or even adulthood typically receive a retrospective historical past of "sepsis" in the neonatal interval that was never confirmed by tradition and that resolved spontaneously; these episodes may need represented an interrupted metabolic intoxication syndrome. Early nonspecific supportive remedy can abort the pathologic cascade or delay the onset of a extra fulminant course until a provisional metabolic prognosis and specific treatment turn into obtainable. The initial signs are often poor feeding associated with a poor suck and irritability. Muscle tone is decreased, generally marked by a fluctuating pattern of decreased and increased tone. In the case of urea cycle defects, hyperammonemia will increase the respiratory drive, resulting in hyperpnea. These symptoms typically progress rapidly, sometimes within a matter of hours, however more often during the course of a few days. It is essential to suspect a metabolic disorder as early as potential in its course to interrupt the progression of signs as a end result of many of these problems are life threatening. The diagnostic evaluation of a new child suspected of having a metabolic encephalopathy should include testing for disorders of amino acid metabolism, natural acid metabolism, the mitochondrial respiratory chain, and the urea cycle (see Table 99-3). The differential analysis for these sufferers can usually be narrowed by the presence of other clinical or routine laboratory findings, corresponding to acidosis, hyperammonemia, hypoglycemia, ketosis, or lactic acidemia. The prognosis will be narrowed additional by performing extra specialised laboratory testing, including plasma amino acid evaluation, urine organic analysis, plasma carnitine evaluation with acylcarnitine profile, and urine carnitine analysis with acylcarnitine profile. Effort must be made to perform a prompt and vigorous laboratory analysis of the affected person suspected of getting a metabolic encephalopathy as a outcome of many of them are potentially treatable. The issues that produce metabolic encephalopathy are mentioned later on this chapter. Metabolic Seizures There are an ever-growing number of inborn errors of metabolism which have been acknowledged as a cause of seizures in the neonatal period or early infancy. As within the case of patients who present with a metabolic encephalopathy, many of the issues that produce neonatal seizures are doubtlessly treatable. The strategy to laboratory testing of these patients ought to embody the same laboratory testing famous in the preceding for the evaluation of sufferers with suspected metabolic encephalopathy. In addition, the affected person with a suspected metabolic seizure disorder should bear additional, specialized testing for both probably treatable and untreatable issues, with emphasis directed towards identification of doubtless treatable disorders. The medical options, biochemical basis, diagnostic testing, remedy, and prognosis for a quantity of of the problems that produce metabolic seizures are offered within the following. The disorders are introduced in three groups: treatable disorders, potentially treatable issues, and untreatable disorders, to allow the attending doctor to prioritize his or her diagnostic evaluation. Treatable Disorders the treatable problems embody folinic acid-responsive seizures, glucose transporter kind I deficiency, pyridoxinedependent epilepsy, and pyridoxal 5-phosphatedependent epilepsy. More particularly, sufferers with both issues share the identical biochemical abnormalities. The biochemical hallmark of those seizure issues is cerebral folate deficiency. Neither dysfunction has been reported to produce seizures in the course of the neonatal interval. Glucose transporter sort 1 deficiency is (in virtually all cases) an autosomal dominant dysfunction that reduces glucose transport by roughly 50%, leading to impaired power production by the mind and a range of neurologic abnormalities. They can have a selection of seizure sorts, including partial, generalized, or myoclonic seizures. Many affected infants also develop episodic eye actions, ataxia, oculomotor apraxia, developmental delay, microcephaly, and "stroke like occasions with reversible hemiplegia" as they become old. Glucose transporter type 1 deficiency can be handled successfully with a low-carbohydrate, high-fat diet (ketogenic diet), which provides ketones as an alternative gas source for the brain.
Betahistine 16mg cheap without prescription
Causes include familial treatment with cold medical term safe betahistine 16mg, syndromic symptoms low potassium betahistine 16mg discount without prescription, and chromosomal abnormalities and environmental influences throughout gestation. It may be associated with different ocular features of significance: a high diploma of hypermetropia, retinal folds, a tendency for choroidal effusions, and the late occurrence of glaucoma. Typically this type is associated with other ocular anomalies such as colobomas of the iris, ciliary physique, fundus, or optic nerve, or colobomatous orbital cysts. It is usually accompanied by different congenital anomalies, similar to central nervous system defects and psychological retardation, and has been observed in isolation, in genetic defects. Treatment involves reconstruction of the orbit to enhance the looks of the face. Because of the heterogenicity of related findings, infants with microphthalmia must be evaluated by both an ophthalmologist and a geneticist. An apparently enlarged eye could additionally be attributable to colobomatous microphthalmia with an related massive cyst, congenital megalocornea, or congenital glaucoma (see p. Colobomatous microphthalmia outcomes when the embryonic optic vesicle fails to shut. Tissue that originally ought to have turn out to be intraocular is encased in a cystic construction exterior the attention within the orbit. If the cyst becomes sufficiently large that proptosis happens, the microphthalmic eye simulates an enlarged eye. The overlying conjunctiva and the conjunctival vessels superimpose a filmy, vascular sample. A generalized bluish discoloration of the underdeveloped sclera is regular in premature infants. Rarely, a congenital weakness in a small space of the sclera produces a bluish bulge called a staphyloma. The lightblue colour is attributable to thinness of the sclera that transmits the darker colour of the underlying uveal tissue. Osteogenesis imperfecta could additionally be related to an identical bluish discoloration of the sclera in the term neonate due to inadequately developed scleral collagen. Blue sclera may be seen in other systemic illnesses such as Marfan syndrome, EhlersDanlos syndrome, and Crouzon syndrome. Intrascleral nerve loops appear as darkly pigmented dots about 3 to 4 mm from the limbus. Congenital ocular melanosis and oculodermal melanosis (nevus of Ota) occur as a unilateral slateblue pigmentation in infancy. Megalocornea as an isolated finding is normally inherited in an autosomal dominant method. Megalophthalmia, which is often inherited as an X-linked recessive trait, is characterised by deep anterior chambers, subluxation of the lens, hypoplastic iris, and cataract formation in early adult life. A corneal diameter of lower than 10 mm could additionally be an isolated finding or may be related to different ocular anomalies. Cases of autosomal dominant and recessive inheritance of microcornea have been described. In the traditional term toddler, a similar appearance may be seen for the first 48 hours after delivery. A persistently hazy or cloudy cornea suggests congenital glaucoma or start damage. This condition is characterized by bilateral cloudy corneas, regular corneal diameter, and regular intraocular pressure. If this measurement exceeds 12 mm, congenital glaucoma have to be thought of, particularly if corneal haze, tearing, and photophobia are present. Associated ocular findings embrace glaucoma, corneal pannus, cataract, irregular optic discs, and foveal hypoplasia. Because the fovea subserves our best imaginative and prescient, its maldevelopment causes the nystagmus and poor visible acuity. The classic signs of congenital glaucoma include tearing, light sensitivity, and blepharospasm. Congenital glaucoma can occur as a major illness or secondary to numerous other ocular circumstances or systemic syndromes. In addition to visual impairment from glaucomatous injury, amblyopia from visual deprivation or anisometropia can stop a profitable visible outcome. The prognosis is decided by the age of onset, time to analysis, and associated ocular and systemic conditions. Unlike glaucoma in adults, the therapy is surgical in the overwhelming majority of cases, and medical management is used just for temporizing the situation or better visualization for varied surgical procedures. It can happen as a single ocular finding, have a Mendelian mode of inheritance, be associated with a chromosomal abnormality, or be associated with other malformation syndromes (Box 103-4). Aganglionic megacolon (Hirschsprung disease) may additionally be associated with iris heterochromia. Abnormal Red Reflex this is probably considered one of the most necessary abnormalities that requires instant evaluation. The term leukocoria is used to describe a white pupil seen by the naked eye or through the pink reflex test. False-positive red reflex check outcomes are generally brought on by small pupils, shifting gaze, limited patient cooperation, poor illumination from the ophthalmoscope, and examiner inexperience. Regardless, these patients ought to be over-referred to the ophthalmologist to verify the true-positive outcomes. Abnormal purple reflexes also can result from misaligned eye or excessive or uneven refractive errors. Because typical iris colobomas result from an irregular closure of the embryonic fissure, in addition they could also be related to a coloboma of the ciliary body, fundus, or optic nerve. When the optic nerve or macula is involved in the coloboma, visual issue occurs. It is always sensible to evaluate the fundus for a pathologic condition when an iris coloboma is detected. The lens grows constantly during life, laying down new lens fibers on its external surface a lot as an onion does. The lens is preserved in capsules (anterior and posterior), and has a nuclear core and surrounding cortical portion. Childhood cataracts could be categorised as congenital, childish, or juvenile, depending on the age of onset. Congenital and infantile cataracts are answerable for about 10% of all blindness worldwide. The etiology of pediatric cataracts could be broadly categorized and summarized as hereditary, metabolic. Furthermore, cataracts may be categorized according to their morphology as diffuse/total, anterior polar, lamellar, nuclear, posterior polar, posterior lentiglobus, posterior (and anterior) subcapsular, persistent hyperplastic major vitreous, and traumatic. Damage that happens within the early embryonic period produces opacifications in the middle of the lens.
16 mg betahistine cheap amex
Postoperative decrease esophageal dilation in children following the performance of Nissen fundoplication treatment x time interaction cheap betahistine 16 mg without prescription. This chapter focuses on the strategy to infants with protracted diarrhea and is a review of current literature on childish diarrheal illnesses medications 25 mg 50 mg betahistine 16mg buy visa. Intractable diarrhea is a term coined many years ago by Avery to describe chronic, unexplained diarrhea in young kids. Protracted diarrhea has been used more just lately to describe infants with unfastened and frequent stools of sufficient severity to require nutritional assist within the form of parenteral alimentation. This emphasis on enough support of whole caloric intake and dietary rehabilitation has dramatically improved the survival of affected infants. Diarrhea is assessed as either secretory or osmotic; however, in a quantity of circumstances both mechanisms could additionally be involved. Secretory diarrhea is the outcome of both impaired absorption of NaCl from villous enterocytes or elevated chloride secretion from crypt cells, secondary to exogenous toxins from micro organism or viruses or endogenous substances (hormones, neurotransmitters, or cytokines), or from inherent defects in the sodium or chloride channels. Osmotic diarrhea outcomes from nonabsorbable substances within the intestinal lumen, which increases the osmolality of the luminal contents. This leads to either retention of fluid or secretion of fluid into the intestinal lumen, therefore leading to diarrhea. In contrast to secretory diarrhea, usually osmotic diarrhea improves with fasting. Osmotic diarrhea may be distinguished from secretory diarrhea by measuring the electrolyte concentration in the stool and the osmotic hole. Some diarrheal issues could have a secretory and osmotic component, as is sometimes seen in celiac disease. Although diarrhea alone could also be liable for an increase in fat excretion of as much as 11 g per day (normally, <7 g fat/day is excreted by individuals consuming 100 g fat/day), when bigger quantities of fats are found in the stool the affected person ought to be evaluated for a disorder of fats absorption. Based on the outline of diarrhea as osmotic or secretory or combined osmotic and secretory parts, childish diarrheal etiologies can be distinguished, as proven in Box 92-1. Disorders of Carbohydrate Absorption the enterocytes in the small gut have at their apical floor brush border various enzymes liable for the digestion of carbohydrates. Patients with carbohydrate malabsorption disorders, regardless of the trigger, current with extreme watery diarrhea, which ends from osmotic action exerted by the malabsorbed oligosaccharide4 (lactose, sucrose, or glucose) within the intestinal lumen. The malabsorbed sugars are then fermented by colonic bacteria, producing a combination of gases. Congenital sucrase-isomaltase deficiency is caused by lowered exercise of the brush border enzyme sucrase-isomaltase. Patients present with diarrhea, usually seen around the age of 3 to 6 months when the infant is weaned from breast milk to child meals that comprise sucrose. Affected infants present with severe, chronic or intermittent watery diarrhea, belly distention, cramping, metabolic acidosis, and failure to thrive. A detailed historical past will present the correlation of the onset of diarrhea and the dietary modifications. Stool osmolality reveals an elevated osmolar gap (>50 mOsm), indicating the presence of malabsorbed sugars. Congenital lactase deficiency can be diagnosed by obtaining an excellent dietary history and can be demonstrated by a scarcity of enhance in blood sugar after a load of lactose. When handled appropriately the sufferers have good catch-up development with normal psychomotor growth. Maltase-glucoamylase is very related to sucrase-isomaltase (59% homology), and has two catalytic sites that are equivalent to these of sucraseisomaltase. The medical symptoms are very similar to different disaccharidase deficiencies with diarrhea, abdominal distention, and bloating. Endoscopy with biopsies will present decreased ranges of the enzyme when symptomatic therapy requires starch elimination from the food regimen. The babies often present very quickly after birth with watery diarrhea, vomiting, poor weight acquire, lactosuria, aminoaciduria, and adjustments within the nervous system. Congenital lactase deficiency is brought on by the deficiency of lactase, within the small intestine and has been linked to chromosome 2q21. Usually, congenital lactase deficiency is an isolated deficiency, however Nichols and associates have reported it in association with different disaccharidase deficiencies corresponding to maltase-glucoamylase. Breast milk and different industrial formulation have lactose; therefore, the onset is usually within the first 10 days of life. The diarrhea resolves after switching to a lactose-free formulation,9 which confirms the diagnosis. Apart from diarrhea, these babies are vigorous and have a good urge for food; they exhibit poor weight achieve but no vomiting. Infants current in the neonatal interval with severe watery diarrhea, which can lead to rapid dehydration and dying. These infants current initially of breastfeeding or ingestion of glucose-containing formulation with severe watery diarrhea that usually can be confused with urine. The predominant sugar of breast milk is lactose, which is hydrolyzed to glucose and galactose earlier than being absorbed. As with congenital lactase deficiency, hypercalcemia resolves after initiation of a glucose-free diet and management of diarrhea. The analysis is made by the onset of diarrhea after the introduction of glucose, the presence of glucose in stools, hypoglycemia, hypernatremic dehydration, and regular intestinal morphology. The diarrhea improves on elimination of glucose, galactose, and lactose from the diet. In the terminal ileum the bile salts are sure with ileal bile acid binding protein. Stool fecal elastase is a superb marker extremely sensitive and particular for pancreatic insufficiency. This dysfunction can present very early in life with meconium ileus, which is an obstruction of the ileum on account of thick meconium plugs. Infants produce restricted quantities of pancreatic lipase and only attain adult ranges by 2 years of age;29 subsequently, infants rely on gastric lipase for fat digestion. Bile salt stabilization of fatty acids and monoglycerides to kind micelles, which in flip stabilize cholesterols, diglycerides, and fat-soluble vitamins. Patients current with failure to thrive in infancy secondary to exocrine pancreatic insufficiency and variable levels of bone marrow failure. The first criterion is demonstration of a hematologic cytopenia, which includes any of the three cell strains. Affected infants have characteristic phenotypic options, together with aplastic alae nasi (which offers the appearance of a beaklike nostril with massive nostrils),60 extension of the hairline to the brow with upswept frontal hair,61 low-set ears, massive anterior fontanelle, micrognathia, thin lips, microcephaly,sixty two aplasia cutis (patchy distribution of hair with areas of alopecia), dental anomalies, poor development, pancreatic exocrine aplasia, and anorectal anomalies (mainly imperforate anus). It was described by many teams, together with Nezelof and Watchi (1961),forty eight Bodian and colleagues in the United Kingdom (1964),forty nine Burke and colleagues in Australia (1967),50 and Shwachman in the United States (1964). Patients present with exocrine pancreatic insufficiency with poor weight achieve, failure to thrive, hypoalbuminemia, edema, and anemia.
Buy discount betahistine 16mg online
Leveling right here refers to the intraoperative willpower of where on the bowel the ganglion cells make an appearance symptoms kidney failure dogs proven 16 mg betahistine. This is finished by taking seromuscular biopsies and having the pathologist evaluate the frozen sections medicine 3605 v order betahistine 16 mg amex. Primary pull-through procedures are being carried out with much higher frequency and would now be thought-about the standard of care. Here, as a substitute of the normal three stages (ostomy, definitive restore, ostomy takedown), the operation is finished in one stage, and with no protective stoma. Occasionally, a main repair with a protective ostomy is performed-a twostage operation, in that ostomy takedown remains to be required. The three traditional open abdominal surgical strategies used to treat Hirschsprung illness are (1) Swenson, (2) Soave, and (3) Duhamel. Over the last decade, experience with laparoscopic/transanal approaches has increased. Systematic evaluations present that more youngsters achieved continence with the laparoscopic/ transanal strategy. Regardless of the process performed, these patients should be followed for years postoperatively. Postoperative care and long-term points are similar to these for patients with anorectal malformations. Because there seems to be no detriment to dilations, some surgeons start a dilator program in all patients, including residence dilation by the mother and father. Also, unique to patients with Hirschsprung illness is the potential of a retained aganglionic phase contributing to ongoing, postoperative constipation. This happens when poorly vascularized, poorly ganglionated, or frankly aganglionic bowel is brought down in the pullthrough. Anal sphincter achalasia can also occur, and injection with botulinum toxin might help make this analysis. All the potential issues, nonetheless, must be balanced by the long-term results, which indicate that approximately 90% of these patients finally obtain normal or nearnormal bowel operate. Anorectal Anomalies Anorectal malformations, or imperforate anus, are a class of congenital malformations that covers a wide spectrum of defects. Overall, most sufferers do reasonably well, with greater than 75% attaining a good diploma of bowel management when they have adequate remedy. The estimated risk for a couple having a second baby with an anorectal malformation is approximately 1%. Traditionally, the terms excessive, intermediate, and low had been used to describe numerous degrees of imperforate anus. However, terminology should relate to the location of the rectal fistula for both prognostic and therapeutic implications. More than 80% of male sufferers with imperforate anus have a fistulous connection between the rectum and the urinary tract. This can go from the rectum to the bladder (rectovesical), to the prostatic urethra (rectoprostatic), and to the bulbar urethra (rectobulbar). An unusual type of imperforate anus happens when the rectum ends blindly within the pelvis. More than 50% of those sufferers have Down syndrome and nearly all patients with Down syndrome and imperforate anus have this variant. In the perineal fistula, the rectum opens on the perineal pores and skin anterior to the anal dimple. A vestibular fistula opens within the posterior side of the introitus but exterior the hymen. A cloaca is a malformation during which the rectum, vagina, and urethra all open into a typical channel of variable size, which then opens onto the perineum. A rectovaginal fistula is extremely unusual; these are often rectovestibular fistulas. Anorectal malformations could additionally be related to malformations of the sacrum and backbone. Hemivertebrae in the thoracic and lumbar spine are additionally related to imperforate anus. Tethered twine is a defect regularly related to imperforate anus, seen in up to 25% of circumstances. It normally coincides with very excessive anal defects, a really irregular sacrum, or spina bifida. Cause and effect is unclear, as is the benefit of surgical remedy of the tethered twine, however the current standard of care is to search for tethered wire in all sufferers with imperforate anus and surgically treat if found. The width of the range is most likely related to how diligently the defects are sought. The larger the malformation, the extra frequent are the associated urologic abnormalities. Patients with a persistent cloaca or rectovesical fistula have a 90% chance of an related genitourinary abnormality. Conversely, youngsters with perineal fistulas have less than a 10% likelihood of an related urologic defect. Hydronephrosis, urosepsis, and metabolic acidosis from poor renal operate are the main sources of mortality and morbidity in newborns with anorectal malformation. In reality, an intensive urologic analysis should take priority over the colostomy itself in sufferers with high lesions. In patients with lower lesions corresponding to perineal fistulas, the urologic analysis can be performed on an elective foundation. This analysis should embody an ultrasonographic research of the kidneys and the whole stomach to rule out the presence of hydronephrosis or any other obstructive process. Approximately 5% of sufferers with imperforate anus have associated esophageal atresia, and up to 10% have important cardiac malformations such as tetralogy of Fallot, ventricular septal defect, or patent ductus arteriosus. The preliminary analysis of imperforate anus is nearly always made during the first new child bodily examination. The first is whether a colostomy shall be wanted, deferring definitive repair until later in life, or whether or not to proceed with definitive repair. The second is to decide whether or not related defects, such as urologic abnormalities, require extra pressing therapy. This time must be used to complete the work-up and focus on choices with the household. On the opposite hand, some associated abnormalities can carry morbidity and mortality dangers in the first 24 hours, and these must be addressed. Intravenous fluids, antibiotic protection, an belly ultrasound, a radiograph of the backbone, anteroposterior and lateral radiographs of the sacrum, a cardiac evaluation, and a nasogastric tube are indicated. In the male, the presence of a well-developed midline groove between the buttocks, a distinguished anal dimple, and meconium exiting via a small orifice positioned anterior to the sphincter within the midline of the perineum are evidence of a perineal fistula. These malformations can be repaired through a perineal strategy in the course of the new child period without a colostomy.
Generic betahistine 16mg fast delivery
Hypoglycemia is present in at least half the cases treatment vitamin d deficiency safe betahistine 16mg,76 and could additionally be manifested soon after birth medicine vs dentistry buy cheap betahistine 16mg line. Plasma progress hormone levels have been reported to be normal, and somatomedin levels had been reported to be increased in a single infant. These infants could require glucose infusion at excessive charges in the instant neonatal period. Patients with Beckwith-Wiedemann syndrome are also predisposed to certain malignancies (adrenal carcinoma, nephroblastoma) and seem to have an elevated threat for malignancies associated with hemihypertrophy. Chromosomal studies have been reported in several sufferers with Beckwith-Wiedemann syndrome. At postmortem examination, the pituitary gland may be hypoplastic or aplastic, the thyroid and adrenal glands small, and the mobile structure of the adrenals disorganized, with atrophy or absence of the fetal cortex. Radiographic research have demonstrated the absence of the septum pellucidum and massa intermedia. Hypoplasia or aplasia of the adenohypophysis with out cerebral or facial anomalies may occur. The underlying pathogenic mechanisms remain unclear, although aplasia of the anterior pituitary was found in siblings of three patients and in two patients with familial histories of consanguinity. Whether the dysfunction is brought on by failure of the pituitary to kind or by degeneration of the pituitary is unknown. It can also be attainable that abnormalities of the hypothalamus with a deficiency in hypophysiotropic releasing hormones are liable for the a quantity of endocrinopathies observed in these infants. Cortisol is changed cautiously, with maintenance doses of hydrocortisone for proven hypoadrenalism. Familial isolated glucocorticoid deficiency has been described in a household of 5 siblings; in two of the infants, glucocorticoid production was regular initially and poor at a later age. This discovering means that in some families there may be a degenerative process in the adrenal gland. Maternal steroid therapy resulting in neonatal subclinical adrenal insufficiency was reported in an infant with cushingoid facies, transient hypoglycemia, and a poor response to intravenous corticotropin at 20 hours. However, maternal steroid therapy, similar to that for continual asthma, solely rarely has been related to neonatal adrenal insufficiency and hypoglycemia. There are feeding problems, a failure to thrive, and regurgitation within the neonatal interval; hypoglycemia, convulsions, and shock or even death may happen in infancy or early childhood. The syndrome is characterised by hyperpigmentation, normal serum electrolyte concentrations, and an unusually extreme, untoward response to sickness or stress. There is commonly a history of affected siblings, and an autosomal recessive mode of inheritance has been instructed. Congenital adrenal hyperplasia (see Chapter 98) may be diagnosed in the neonatal period due to the presence of hypoglycemia. Two male infants have been reported with glucagon deficiency; the disorder became evident on the second to third day of postnatal life, with repeated convulsive movements, hypotonia, weak crying, and poor sucking. In both infants, the prognosis was based mostly on a low basal glucagon focus and a robust hyperglycemic response to glucagon. In one of the infants, the response to glucagon was lacking, and in the other, there was a lack of response to hypoglycemia and alanine infusion. The mother and father of this second toddler were closely related and had partly deficient glucagon secretion; two siblings of this toddler died before 5 months of age with probable hypoglycemia. Some of these infants may develop adrenal calcification, which may be identified on follow-up. Fructose is the primary sweetening agent in nature, occurring largely in fruits, vegetables, and honey, and is commonly added as a sweetener to foods and beverages within the type of disaccharide sucrose. In people, the liver is the main site of fructose metabolism, with considerably less essential sites being the kidney, gut, and different tissues. Fructose is metabolized by specific enzymes that convert it into intermediates of the glycolytic-gluconeogenic pathway. The strategic enzymes associated with disorders of fructose metabolism have been recognized. Fructose-1phosphate is break up into dihydroxyacetone phosphate and glyceraldehyde by the action of aldolase. Glyceraldehyde is converted to glyceraldehyde-3-phosphate by the motion of triokinase. Dihydroxyacetone phosphate and glyceraldehyde-3-phosphate are the intermediates in the glycolytic-gluconeogenic pathway. Additionally, fructose1,6-bisphosphatase is a key gluconeogenic enzyme that catalyzes the conversion of fructose-1,6-biphosphate into fructose-6-phosphate. It has been suggested that intravenous fructose be used for the therapy of hypoglycemia in both adults and new child infants because of the dearth of hyperglycemia associated with its administration and, subsequently, the lack of reactive hypoglycemia. However, warning ought to be exercised as a result of the metabolism of fructose in the liver causes increased lactate formation, high-energy phosphate depletion, elevated uric acid formation, and inhibition of protein synthesis. Essential fructosemia is a rare and innocent disorder characterised by the appearance of fructose within the urine. This dysfunction is the consequence of a deficiency of fructokinase, which leads to an incapability to metabolize fructose. Hereditary fructose intolerance, or aldolase-B deficiency, leads to an inability to break up fructose-1-phosphate into triose phosphates. The enzymatic activity contributing to the formation of fructose-1,6-biphosphate from triose phosphates can be lowered. Clinical manifestations embody hypoglycemia after the ingestion of meals containing fructose, lethargy, nausea, vomiting, pallor, sweating, and proof of liver dysfunction corresponding to jaundice, hepatomegaly, a bleeding tendency, and proximal renal tubular dysfunction. Treatment consists of the whole elimination of all sources of fructose from the food plan, including meals and drugs. Fructose-1,6-bisphosphatase deficiency ought to really be known as a defect in gluconeogenesis quite than a disorder of fructose metabolism as a end result of these infants can tolerate fructose of their diets. Fructose-1,6-bisphosphatase is the key regulatory enzyme in the gluconeogenic pathway concerned in the formation of fructose-6-phosphate, the immediate precursor of glucose-6-phosphate, and at last glucose. A deficiency of this enzyme ends in an lack of ability to make glucose from all gluconeogenic precursors. These infants can present in the neonatal interval with hypoglycemia and extreme metabolic acidosis. The medical manifestations are related to hypoglycemia and acidosis and embrace lethargy, tachycardia, apnea, hypotonia, and tachypnea. The defect is inherited as an autosomal recessive disorder and is seen extra typically in ladies than boys. Treatment is aimed on the maintenance of plasma glucose by way of frequent feedings and avoidance of extended periods of fasting. A therapeutic routine consisting of the continuous nighttime administration of glucose by the nasogastric route, as in glycogen storage disease, ought to be successful. Hereditary fructose intolerance may manifest within the neonatal interval if the susceptible toddler is fed a sucrosecontaining formulation or given desk sugar, fruits, or fruit juices. Symptoms include vomiting, failure to thrive, excessive sweating, and unconsciousness or convulsions. Hypoglycemia is frequently seen, as are fructosemia and fructosuria, after the ingestion of fructose.
Buy cheap betahistine 16 mg on-line
This group supplies Omegaven at 1 g/kg per day for neonates with a conjugated bilirubin of greater than 2 symptoms kidney infection buy 16mg betahistine. These studies indicate persistence and symptoms when quitting smoking betahistine 16mg generic line, at instances, progression of fibrosis despite normalization of bilirubin. Some facilities are arguing for lipid minimization as the preliminary therapy for parenteral nutritionssociated cholestasis. Quantitative neonatal glucose-6-phosphate dehydrogenase screening: distribution, reference values, and classification by phenotype. Clinical practice guideline: administration of hyperbilirubinemia within the newborn toddler 35 weeks or more of gestation. Provisional Committee for Quality Improvement and Subcommittee on Hyperbilirubinemia. In: American Academy of Pediatrics, American College of Obstetricians and Gynecologists, eds. Phototherapy to prevent severe neonatal hyperbilirubinemia within the newborn infant 35 or more weeks of gestation. End-tidal carbon monoxide hour-specific nomogram: For early and pre-discharge identification of babies with increased bilirubin manufacturing. Neonatal hyperbilirubinemia within the low-intermediate-risk category on the bilirubin nomogram. Trends in hospitalizations for neonatal jaundice and kernicterus in the United States, 19882005. Evaluation of opposed occasions as a result of change transfusions in time period and near-term newborns. Management of hyperbilirubinemia in newborns: measuring performance through the use of a benchmarking model. Pyruvate kinase deficiency as a cause of extreme hyperbilirubinemia in neonates from a polygamist community. Bilirubin photoisomerization in premature neonates under low- and high-dose phototherapy. Current Italian practices regarding the management of hyperbilirubinaemia in preterm infants. The effectiveness of oral tin mesoporphyrin prophylaxis in decreasing bilirubin manufacturing after an oral heme load in a transgenic mouse mannequin. Erythroblastosis fetalis and its affiliation with common edema of the fetus, icterus gravis neonatorum, and anemia of the newborn. A new transcutaneous bilirubinometer, BiliCheck, used in the neonatal intensive care unit and the maternity ward. Relation between serum bilirubin ranges 450 ol/L and bilirubin encephalopathy; a Danish population-based research. Rehospitalisation after delivery hospitalisation: patterns among infants of all gestations. Total serum bilirubin exceeding change transfusion thresholds within the setting of common screening. Suppression of bilirubin manufacturing within the Crigler-Najjar type I syndrome: studies with the heme oxygenase inhibitor tin-mesoporphyrin. Genome-wide affiliation examine identifies a susceptibility locus for biliary atresia on 10q24. A controlled, randomized, double-blind trial of prophylaxis in opposition to jaundice amongst breastfed newborns. Alpha-1 antitrypsin deficiency: a conformational disease related to lung and liver manifestations. Orlistat treatment of unconjugated hyperbilirubinemia in Crigler-Najjar illness: a randomized controlled trial. Severe neonatal hyperbilirubinemia and adverse short-term penalties in Baghdad, Iraq. Intravenous immune globulin in neonatal immune hemolytic disease: does it cut back hemolysis Effects of sulfisoxazole, hypercarbia, and hyperosmolality on entry of bilirubin and albumin into brain areas in young rats. Developmental follow-up of breastfed term and near-term infants with marked hyperbilirubinemia. Hemolysis and hyperbilirubinemia in an African American neonate heterozygous for glucose-6-phosphate dehydrogenase deficiency. Relationship of benzyl alcohol to kernicterus, intraventricular hemorrhage, and mortality in preterm infants. Glucose-6-phosphate dehydrogenase deficiency and extreme neonatal hyperbilirubinemia: a complexity of interactions between genes and environment. Bilirubin genetics for the nongeneticist: hereditary defects of neonatal bilirubin conjugation. Predischarge bilirubin screening in glucose-6-phosphate dehydrogenase-deficient neonates. Acute hemolysis and severe neonatal hyperbilirubinemia in glucose-6-phosphate dehydrogenase-deficient heterozygotes. Hyperbilirubinemia among African American, glucose-6-phosphate dehydrogenasedeficient neonates. Gilbert syndrome and glucose-6-phosphate dehydrogenase deficiency: a dose-dependent genetic interaction essential to neonatal hyperbilirubinemia. Post-phototherapy neonatal bilirubin rebound: a possible cause of significant hyperbilirubinaemia. A single dose of Snmesoporphyrin prevents development of severe hyperbilirubinemia in glucose-6-phosphate dehydrogenase-deficient newborns. Direct comparison of Sn-mesoporphyrin, an inhibitor of bilirubin production, and phototherapy in controlling hyperbilirubinemia in time period and nearterm newborns. A comparison of other risk-assessment methods for predicting vital neonatal hyperbilirubinemia in time period and near-term infants. Selectivity of imidazoledioxolane compounds for in vitro inhibition of microsomal haem oxygenase isoforms. Interaction of hemolysis and hyperbilirubinemia on neurodevelopmental outcomes within the collaborative perinatal project. Impact of common bilirubin screening on extreme hyperbilirubinemia and phototherapy use. Genomic alterations in biliary atresia counsel area of potential illness susceptibility in 2q37. Coexpression of gene polymorphisms involved in bilirubin manufacturing and metabolism. Hidden dangers: early discharge and bilirubin toxicity because of glucose 6-phosphate dehydrogenase deficiency. Zincrotoporphyrin is a selective inhibitor of heme oxygenase activity within the neonatal rat. An approach to the management of hyperbilirubinemia in the preterm infant less than 35 weeks of gestation.
Diseases
- Cushing syndrome, familial
- PANDAS
- Bickel Fanconi glycogenosis
- M?ller Barth Menger syndrome
- Lymphoma, gastric non Hodgkins type
- Skin peeling syndrome
Betahistine 16 mg buy generic on-line
Additionally symptoms to pregnancy betahistine 16 mg buy fast delivery, calcitonin increases calcium and phosphorus excretion medicine cabinets with mirrors betahistine 16mg order without a prescription, so the overall impact of calcitonin is to decrease serum calcium and phosphorus concentrations. With regard to magnesium, calcitonin might lower both its release from bone and renal tubular reabsorption. It is during these intervals of calcium stress that a tonic antiresorptive hormone will greatest exert its results to limit skeletal loss and promote mineral accretion. Fetal Calcitonin Function Calcitonin is expressed by human thyroidal C cells early in gestation, and it circulates in fetal blood at levels which might be higher than those in the mom. Normative data for preterm and newborn full-term infants are extraordinarily limited and the results regularly troublesome to examine because of the completely different tools and software used. Nitrogen, vitality, minerals, and nutritional vitamins enable a excessive velocity of body size progress, representing about 1. The fetus maintains its hypercalcemic state in a excessive calcitonin and estrogen surroundings, selling the modeling-to-remodeling ratio in favor of modeling and thus growing endocortical bone. In addition, in accordance with the mechanostat theory of bone growth, fetal bone can be pushed by the mechanical drive utilized to the fetal skeleton during the intrauterine resistance coaching supplied by common fetal kicks towards the uterine wall. Various components influence the processes of development, mineralization, and bone structure. This results in a large discount in calcium availability for bone mineralization compared with the prenatal state of affairs. The hormonal environment changes postnatally as a result of the placental supply of estrogen and heaps of different hormones has been cut off. The physical density of lengthy bones such as the femoral diaphysis decreases by about 30% during the first 6 months of life. This change is generally the outcome of an increase in marrow cavity measurement, which is quicker than the increase within the crosssectional area of the bone cortex. In term infants, these postnatal modifications have been classically referred to as physiologic osteoporosis of infancy, however they seem to happen without a rise in bone fragility. However, in multivariate evaluation, physique weight was the major and in addition the only vital predictor of these parameters. Postnatal diversifications of the skeletal system to extrauterine circumstances additionally occur in premature infants, with the distinction being that they happen earlier than they do in time period infants. These postnatal changes have been classically called osteopenia of prematurity, and these changes could be accompanied by an increase in bone fragility and the danger for fracture. Radiologically, nonetheless, figuring out "osteopenia" is troublesome and its scientific interpretation is unsure. Thus an emphasis on clearly defining infants as having rickets may be extra clinically related. This variance in definition is at least partially due to the dearth of scientific signs in lots of neonates, even at a very low serum complete calcium concentration. A better definition of neonatal hypocalcemia can be based mostly on the metabolically energetic element of calcium, ionized calcium, because adjustments in ionized calcium concentration usually have a tendency to have physiologic significance. Under circumstances of regular acid-base status and normal albumin ranges, the serum whole calcium stage and Ca2+ are linearly correlated, so total serum calcium measurements stay useful as a screening test. Neonates on the biggest risk for symptomatic or asymptomatic neonatal hypocalcemia, such as the infants of diabetic mothers or preterm or asphyxiated neonates, are frequently sick for a mess of reasons, and the contribution of neonatal hypocalcemia to signs related to their primary illness can be simply obscured. From a medical viewpoint, as a result of Ca2+ concentrations are maintained within narrow ranges underneath regular circumstances, the potential threat for disturbances of physiologic perform will increase because the Ca2+ focus decreases. The early and late forms of hypocalcemia have different causes and occur in different medical settings. Early neonatal hypocalcemia happens during the first four days of life and represents an exaggeration of the conventional fall in serum calcium focus that occurs during the first 24 to 48 hours of life. Trabecular bone, which is richly vascularized, represents the main supply of probably quickly mobilized calcium. Because intestinal calcium absorption is correlated with intake, and dietary calcium is normally low on the primary day of life, the serum calcium focus decreases on the first day of life. In full-term infants, hypocalcemia is normally defined as an ionized calcium concentration of less than 1. An exaggerated rise in calcitonin secretion in untimely infants may play a contributory position. Hypocalcemia is temporary, and usually the serum calcium focus progressively reverts to regular after 1 to three days. Factors contributing to serum calcium normalization embrace elevated calcium intake with feedings, elevated renal phosphorus excretion, and improved parathyroid perform. Prematurity and birth asphyxia are regularly associated issues that independently improve the danger for hypocalcemia. The pure historical past is often much like that of early neonatal hypocalcemia in preterm infants, however hypocalcemia generally persists for several additional days. The incidence of hypocalcemia can also be increased within the infants of gestational diabetic mothers, and the position of hypomagnesemia has been demonstrated. In these infants, the following factors might contribute to early hypocalcemia: a decreased calcium intake owing to delayed feedings, an increased endogenous phosphorus load ensuing from the discount of the glomerular filtration price, and an elevated serum calcitonin focus. Theoretically, the correction of acidosis with alkali could further irritate hypocalcemia by inducing decreased calcium flux from bone to the extracellular fluid and by reducing the ionized calcium concentration. This definition is a statistical one and relies on assumptions of regular distributions of physiologic variables. Further investigation must outline physiologically necessary limits for time period and preterm neonates. Characteristically, early neonatal hypocalcemia occurs most incessantly in preterm infants, infants with proof of respiratory melancholy at birth, infants of diabetic mothers, infants with significant growth restriction, and infants of moms treated with anticonvulsants during being pregnant. In preterm infants, the reference values for ionized calcium are available just for reasonably untimely infants who show values similar to those for fullterm infants. The frequency of hypocalcemia varies inversely with delivery weight and gestational age. In preterm infants, the postnatal lower within the serum calcium level usually happens extra quickly than it does in term infants, the magnitude of the melancholy being inversely proportional to gestation. The cause for the maintenance of Ca2+ is unsure but might be associated to low serum protein focus and pH associated with prematurity. The sparing impact of Ca2+ Late Hypocalcemia Hypocalcemia is conventionally outlined as late when it occurs after the first four days of life. Late neonatal hypocalcemia usually develops at about four to 7 days of age (see Box 96-1) and extra regularly in term than preterm infants. Late hypocalcemia was frequently observed in infants fed cow milk or evaporated milk because of their excessive phosphorus content material. With the introduction of adapted infant formulas, late hypocalcemia, although not abolished, has turn out to be uncommon, though it appears to happen extra incessantly in the Southwestern a half of the United States. It may also be more widespread amongst Hispanic and male infants, however additional information is required concerning these possibilities. These variations correlate with absolutely the phosphorus amount, however not with the different calcium-to-phosphorus ratios in formulation. The pathogenesis of this transient hypoparathyroidism in late neonatal hypocalcemia is poorly understood. Serum calcium levels incessantly enhance when these infants are given human milk, lower-phosphate formulation, and calcium supplements.
Buy generic betahistine 16 mg online
Injuries of the brachial plexus have long been acknowledged as a consequence of inauspicious labor and delivery symptoms 0f parkinson disease 16 mg betahistine with amex. An avulsion of the nerve root treatment mastitis best 16mg betahistine, or preganglionic lesion, is mostly associated with the presence of Horner syndrome (sympathetic chain), elevated hemidiaphragm (phrenic nerve), or winged scapula (long thoracic nerve). Surgical repair of nerve root avulsion has been recommended by some investigators, including Solonen and co-workers,23 who reported good leads to three infants with full avulsion of the cervical nerve roots who underwent surgical procedure throughout the first 3 months of life. Abduction splinting of the limb in the first few months of life is pointless and may additional complicate decrease plexus injury. Gentle range-of-motion exercises could also be used to forestall adduction and internal rotation contracture. Infants with incomplete recovery might require later reconstructive surgery to reduce deformity and useful disability. In young children without mounted contractures and secondary bony deformities, tendon transfers could also be used to stability asymmetric forces. Shortening of the sternocleidomastoid muscle leads to tilting of the pinnacle toward the affected muscle and rotation of the chin towards the opposite facet. Birth trauma, intrauterine malposition, muscle fibrosis, and venous abnormality inside the muscle have all been implicated, but no single cause has been identified. Davids and associates demonstrated that the sternocleidomastoid muscle is contained inside a separate fascial compartment. A palpable mass is typically present throughout the affected muscle through the first few weeks of life. Flattening of the head and slight facial asymmetry or plagiocephaly are usually current. Cervical hemivertebrae are sometimes much less deforming than unsegmented, unilateral cervical bars. As in all instances of congenital spinal curvature, a careful seek for other systemic anomalies, similar to these involving the cardiac and genitourinary methods, have to be made. Anteroposterior and lateral views of the neck should be obtained initially; computed tomography could also be necessary in some cases. Particular attention should be given to the higher cervical backbone, especially the occipitoatlantal (occiput-C1) and the atlantoaxial (C1-C2) areas. If no underlying skeletal abnormalities are recognized, a program of stretching workout routines is indicated to lengthen the contracted sternocleidomastoid muscle. The head is first tilted towards the other shoulder, and the chin is then rotated toward the affected facet. Exercises should be carried out gently, and the corrected position ought to be maintained for 5 to 10 seconds on each repetition. A program of 10 to 15 repetitions carried out 4 occasions daily is sufficient generally. This procedure seldom fails if begun in the course of the first 3 months of life, however seldom succeeds if begun after 18 months of age. It may be impossible to reverse the facial asymmetry that has developed due to head tilting. There were no clavicular fractures in these patients, although different authors have reported clavicular fractures after cesarean delivery. Complete fractures usually have a tendency to be accompanied by traditional signs and indicators. Discoloration, tenderness, and crepitation at the fracture site are common physical findings. Brachial plexus palsy, neonatal sepsis, traumatic separation of the proximal humeral epiphysis, humeral shaft fracture, and shoulder dislocation must be considered in the differential prognosis. The remedy of clavicular fracture is easy; asymptomatic sufferers with incomplete fractures need no immobilization. The remedy can embody applying a figure-eight harness of gauze and tape or securing the affected arm to the chest with a bandage for 7 to 10 days. An elastic bandage loosely applied around the chest and concerned extremity after a cotton pad has been placed within the axilla may be thought-about for bigger infants. Isolated right-sided involvement is commonest, with bilateral involvement much less frequent and isolated left-sided involvement typically seen solely in the context of dextrocardia. It is postulated that compression from the subclavian artery may explain the predilection for right-sided illness, and cervical ribs might account for bilateral illness. Congenital pseudarthrosis of the clavicle is usually asymptomatic in infants, with operative repair delayed till early childhood. Long-Bone Fractures Fractures of different lengthy bones are often seen after a difficult supply. Fractures or separations of the proximal humeral epiphysis may occur with the same drive that produces clavicular fracture and brachial plexus injury. Symptoms and indicators may be comparable; pseudoparalysis, swelling, pain on passive movement, and crepitation with shoulder joint movement are normally present. Arthrography and magnetic resonance imaging can also be used to establish the analysis. When the prognosis is confirmed soon after harm, the affected limb ought to be immobilized in a Velpeau bandage. Treatment is pointless if the prognosis is delayed until callus formation has occurred. Scaglietti identified that late contractures of the shoulder in sufferers with fractures or separations resulting from a severely displaced proximal humerus may be difficult to distinguish from contractures attributable to brachial plexus damage. Neonatal fractures normally contain the higher extremity, significantly the shoulder area, and are the end result of a troublesome supply. Fractures of the decrease extremity are much less widespread and may be indicative of an underlying neuromuscular dysfunction, particularly those that restrict joint mobility, such as arthrogryposis multiplex congenita. Clavicle Fractures of the clavicle are the most typical kind of fracture in neonates. The incidence of clavicular fractures ranges from 2 to 7 circumstances per 1000 live births. McBride and colleagues reported 9106 newborns prospectively screened for clavicular fracture. Clinical determinants of the finish result of guide stretching within the therapy of congenital muscular torticollis in infants: a prospective examine of eight hundred and twenty-one instances. Congenital muscular torticollis: sequela of intrauterine or perinatal compartment syndrome. Congenital muscular torticollis and sternomastoid tumor: result of nonoperative therapy. The timed look of some congenital malformations in orthopaedic abnormalities.
Betahistine 16 mg discount free shipping
Glucose imbalances treatment ingrown toenail 16mg betahistine discount overnight delivery, hyperkalemia symptoms 5-6 weeks pregnant 16 mg betahistine with amex, and hypocalcemia are the commonest metabolic derangements associated to transfusion, owing to the shortcoming of the toddler to effectively metabolize and/or excrete many compounds within the blood elements similar to anticoagulants, preservatives, and other solutes. Hypoglycemia Hypoglycemia (see Chapter 95) may end up from the combination of decreased glucose infusion rates throughout transfusion and impaired glycogenolysis and gluconeogenesis within the liver of the preterm neonate. Continuous glucose infusion rates of larger than 3 to 4 mg/kg per minute are often required in preterm infants; if maintenance fluids are suspended during transfusion, glucose infusion charges can lower to roughly 0. Furthermore, reported incidences of hypoglycemia in neonates either during or after trade transfusions range from 1. Hypoglycemia occurring after exchange transfusion is believed to be attributable to intraprocedural hyperglycemia, which causes rebound hypoglycemia from insulin secretion. Current transfusion considerations and tips focus on lowering each transfusion number and donor exposures. Nevertheless, hematologic, immunologic, infectious, cardiovascular, and metabolic problems can happen. Many of these risks exist for transfusion recipients of any age, whereas others pose a higher risk to the neonatal recipient. Parents have to be suggested of the dangers, advantages, and alternate options to transfusion, and informed consent should be documented within the medical record along with the indications for, and outcomes of, the prescribed transfusion. Previously irradiated and stored (24 hours) units may have plasma K+ unsafe for large-volume transfusion to neonates, particularly if administered rapidly. Therefore, they want to be issued immediately post-irradiation, or washed or volume-reduced to take away extracellular K+ that accumulates after processing. These embody hemolysis from shear and/or warmth stress imposed on erythrocytes by extracorporeal circuits, infusion devices, filters, blood warmers, or phototherapy light exposure. When a hemolytic transfusion reaction is suspected, the transfusion ought to be instantly stopped, blood cultures (from patient and blood component(s)) must be obtained, and the transfusion service ought to be notified. Mannitol could additionally be administered to drive diuresis, but osmotic diuresis in neonates is controversial due to concerns about alterations in cerebral microcirculation and threat of intraventricular hemorrhage. These reactions are believed to result from the release of pyrogenic cytokines by leukocytes throughout the plasma throughout storage. Because of the immaturity in neonatal liver and kidney perform, and the low quantity of skeletal muscle mass, transfusion of citrate-enriched blood can outcome in hypocalcemia from citrate toxicity. The amount of citrate infused into a neonate throughout a small-volume transfusion (10-15 mL/ kg) could be very unlikely to cause hypocalcemia; nevertheless, the citrate load during an change transfusion can reach very excessive ranges and result in symptomatic hypocalcemia. In a retrospective evaluation of 106 infants undergoing one hundred forty change transfusions, symptomatic hypocalcemia was one of the most widespread severe unwanted effects. Eighty-one infants have been classified as "wholesome" if indication for trade was solely asymptomatic hyperbilirubinemia; 25 infants had been categorised as "unwell" if co-morbid circumstances existed. Notifying the transfusion service for additional laboratory analysis of the response is important to correctly classify the reaction so that the patient can be managed appropriately. For delicate or localized cases, transfusion may be continued as quickly as signs have subsided; nonetheless, extreme allergic reactions (anaphylactoid or anaphylactic reactions) might require therapy with corticosteroids and/or epinephrine. The identical blood unit should never be restarted in extreme instances, even after symptoms have abated. In these instances, IgA-deficientlasma merchandise could also be obtained, however require using uncommon donor registries. Prolonged latency of clinical manifestations and dying is believed to result from thymic and/or extrathymic semi-tolerance for allogeneic cytotoxic T lymphocytes. Fortunately, this complication can be prevented by pretransfusion gamma irradiation of cellular blood components at a dose of two. Many transfusion providers irradiate all cellular blood products given to preterm infants born weighing 1. The recognized and presumed indications for irradiation of blood elements for neonates are listed in Box 89-1. Treatment is especially supportive, including fluid and/or vasopressor assist in the face of hypotension. These antibodies activate and sequester recipient neutrophils throughout the endothelium of the lungs, finally leading to the manufacturing of vasoactive mediators and capillary leak. Transfusion of adult blood merchandise containing plasma with naturally occurring anti-T antibodies into neonates with T-activation can present with intravascular hemolysis following transfusion, or unexplained failure to obtain the anticipated post-transfusion hemoglobin increment. Alternatively, T-activation could also be detected within the laboratory without any evidence of clinical hemolysis, making broad-based screening impractical. T-activation has been reported primarily in neonates with necrotizing enterocolitis, particularly in these with severe illness requiring surgical intervention but in addition in septic infants with other surgical issues. Those infants with T-activation had Clostridia cultured from blood, peritoneal fluid, or stool in 14 of 16 (88%) of cases and have been extra more likely to have intestinal perforation at laparoscopy. Infants with discrepancies in ahead and reverse blood typing and evidence of hemolysis on smear should be suspected of T-activation. The prognosis is confirmed by particular agglutination tests using peanut lectin Arachis hypogea and Glycine soja. Severity and remedy can vary from full recovery with conservative medical administration to intestinal perforation and bowel necrosis requiring surgical intervention. Some hypothesize that even subtle reductions in blood flow and subsequent reperfusion occurring in response to hypoxia might contribute to bowel harm. Infection leads to neuroinvasive illness (meningo-encephalitis, spastic paralysis) in roughly 20% of people, with extra extreme sequelae in the aged and immunocompromised. Despite intensive donor screening and laboratory testing, infections can still be transmitted through blood merchandise. Pathogen inactivation provides the benefit of eliminating the chance of infection with any nucleic acidcontaining agent, which includes viruses, micro organism, protozoa, and fungi (prions excluded). However, present pathogen-inactivation techniques using nucleic acidinactivating brokers are still under investigation as a outcome of no single technique has proved to be efficient for all blood parts. Approximately one third of these with untreated chronic hepatitis will develop hepatic fibrosis and cirrhosis inside 2 a long time; those with cirrhosis have a 1% to 5% risk of hepatocellular carcinoma 20 years after cirrhosis is diagnosed. This is due to shorter window periods from time of acute an infection to laboratory markers of infection (16-32 days) within the donor population. This is finished by holding the placental end of the umbilical wire, and gently moving blood inside the umbilical vessels toward the neonate. This "stripping" is carried out one to 4 times prior to clamping and cutting the wire. In these circumstances transfused paternal cells categorical the antigens to which the mom has been sensitized, and are passively transferred through the placenta to the neonate. Antileukocyte and antiplatelet antibodies have been present in 16% and 12% of mothers, respectively. Additionally, it was found that the height bilirubin concentration was greater for infants who had obtained delayed twine clamping in comparison with infants with immediate clamping.
Purchase 16mg betahistine mastercard
More acidic pediatric amino acid options improve calcium and phosphorus solubility medications in pregnancy buy betahistine 16 mg on-line. This quantity of calcium provided by the parenteral route is about 60% to 80% of that deposited by the fetus during the last trimester of gestation symptoms 7dpiui betahistine 16 mg on-line. Their use has dramatically decreased the incidence of fractures and radiographically recognized osteopenia. A related reduction has also been noticed in preterm infants fed preterm formulas. In contrast, phosphorus is usually nicely absorbed, however phosphorus retention is related to calcium and protein accretion. Absorption of calcium is at present greatest evaluated using stable isotope methods, bearing in mind the endogenous intestinal calcium secretion (Table 96-5). Routine evaluation of bone mineral status using biochemical testing is indicated for infants with birth weight less than 1500 g however not those with delivery weight larger than 1500 g. Routine administration of preterm infants, especially these with delivery weight less than 1800 to 2000 g, should include human milk fortified with minerals or formulation designed for preterm infants. If solely breastfed, a follow-up serum alkaline phosphatase at 2 to 4 weeks after discharge from the hospital could also be thought of. At 6 months of corrected age, backbone and total bone mineral density, corrected for anthropometric values, is in the vary of normal term newborn infants. Although the long-term penalties are unclear, the advantages of prevention and therapy embody avoidance of fractures and presumably improved linear development and peak bone mass. Severe rickets can also limit pulmonary standing, as a outcome of historically it was thought that rickets was, partially, a pulmonary illness attributable to poor lung expansion within the absence of a standard rib cage. De Curtis to the previous editions of this chapter, portions of which remain unchanged. Feeding untimely new child infants palmitic acid in quantities and stereoisomeric position similar to that of human milk: results on fat and mineral stability. Malignant infantile osteopetrosis initially presenting with neonatal hypocalcemia: case report. Feto-maternal vitamin D status and toddler whole-body bone mineral content material within the first weeks of life. Subcutaneous fat necrosis of the newborn: hypercalcemia with hepatic and atrial myocardial calcification. Short and long-term end result of sufferers with pseudo-vitamin D deficiency rickets treated with calcitriol. Neonatal factors predicting childhood peak in preterm infants: proof for a persisting impact of early metabolic bone illness Effect of different dosages of oral vitamin D supplementation on vitamin D status in wholesome breastfed infants: a randomized trial. Canadian Paediatric Society: Vitamin D supplementation: recommendations for Canadian moms and infants. Calcium absorption in very low start weight infants with and with out bronchopulmonary dysplasia. Dietary reference intakes for calcium, phosphorus, magnesium, vitamin D, and fluoride. Maternal vitamin D standing throughout pregnancy and childhood bone mass at age 9 years: a longitudinal examine. Long-term follow-up of extraordinarily low delivery weight infants with neonatal renal failure. Effects of ethnicity and vitamin D supplementation on vitamin D status and changes in bone mineral content material in infants. Targeting dietary vitamin D intakes and serum 25hydroxyvitamin D in healthy infants. Physical exercise combined with therapeutic massage improves bone mineralization in premature infants: a randomized trial. Effects of 1,25dihydroxycholecalciferol on restoration and resolution of late transient neonatal hypocalcemia. Calcium-regulating hormones and parathyroid hormone-related peptide in regular human being pregnant and postpartum: a longitudinal examine. Bone isoenzyme of serum alkaline phosphatase and serum inorganic phosphate in metabolic bone disease of prematurity. Lower whole blood ionized magnesium concentrations in hypocalcemic infants of gestational diabetic mothers. Net calcium absorption in untimely infants: results of 103 metabolic balance research. Lethal skeletal dysplasia from focused disruption of the parathyroid hormone-related peptide gene. Dual-energy X-ray absorptiometry research of bone mineral status in new child infants. Phosphorus consumption in preterm babies and variation of tubular reabsorption for phosphate per liter glomerular filtrate. Urinary phosphate/creatinine, calcium/creatinine, and magnesium/creatinine ratios in a wholesome pediatric inhabitants. Ablation of calcitonin/ calcitonin gene-related peptide-alpha impairs fetal magnesium but not calcium homeostasis. High frequencies of elevated alkaline phosphatase exercise and rickets exist in extraordinarily low birth weight infants despite present dietary help. Factors affecting new child bone mineral content material: in utero results on newborn bone mineralization. Circulating ranges of soluble alphaKlotho are markedly elevated in human umbilical cord blood. Clinical problems of extracellular calcium sensing and the molecular biology of the calcium-sensing receptor. Mutations within the human Ca(2+)-sensing receptor gene cause familial hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism. Executive abstract for the report: assessment of nutrient necessities for toddler formulation. Reference values of physique composition obtained by twin power X-ray absorptiometry in preterm and time period neonates. Parathyroid hormone and parathyroid hormone-related peptide in venous umbilical twine blood of healthy neonates. Physical exercise programs for selling bone mineralization and progress in preterm infants. Calcium absorption, kinetics, bone density, and bone structure in sufferers with hereditary vitamin D-resistant rickets. Neonatal severe hyperparathyroidism: genotype/phenotype correlation and the usage of pamidronate as rescue remedy. Maternal, fetal and neonatal vitamin D and calcium metabolism throughout being pregnant and lactation.