
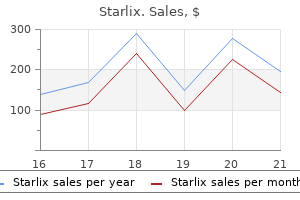
Starlix dosages: 120 mg
Starlix packs: 30 pills, 60 pills, 90 pills

Generic starlix 120 mg on line
Accelerating axonal progress promotes motor recovery after peripheral nerve injury in mice antiviral brandon cronenberg starlix 120mg generic amex. A rat model research of atrophy of denervated musculature of the hand being quicker than that of denervated muscular tissues of the arm anti viral buy starlix 120mg fast delivery. Differentiation of activated satellite tv for pc cells in denervated muscle following single fusions in situ and in cell tradition. Effects of short- and long-term Schwann cell denervation on peripheral nerve regeneration, myelination, and measurement. Mechanisms of illness: what factors restrict the success of peripheral nerve regeneration in humans Does use of a myoelectric prosthesis forestall cortical reorganization and phantom limb pain Postoperatively, the higher limb is splinted with shoulder adduction and elbow flexion for 6 weeks, after which rehabilitation train is begun. The shoulder is kidnapped progressively, with full range of passive abduction potential three months after operation. In a meta-analysis of nerve reconstruction for elbow flexion in adults with brachial plexopathy, intercostal to musculocutaneous switch without interpositional nerve grafts resulted in British Medical Research Council grade M3 strength or greater in 72% of sufferers, whereas solely 47% of sufferers who underwent nerve grafting achieved grade M3 strength. The rationale is to use the less important donor nerve to regain function of the more valued recipient nerve. Theoretically, one given receptor can only be reinnervated by one type of donor nerve. For instance, in axilla-level ulnar nerve damage with an intact median nerve, the department of the anterior interosseous nerve to the pronator quadratus could be transferred to the deep motor branch of the ulnar nerve to revive operate of intrinsic musculature of the hand,5 whereas transection of the ulnar nerve at axilla level, even reconstructed instantly, will always result in irreversible atrophy of intrinsic musculature of the hand. The third indication for nerve transfer, which is extra controversial, is a nerve damage mixed with significant vascular and bony injuries. Application of nerve switch in that scenario might keep away from troublesome dissection by way of the scarred space and unnecessary injury to necessary structures. An instance is transfer of the nerve to the triceps for reconstruction of the axillary nerve6 for sufferers with axillary nerve damage in the infraclavicular area, where the axillary artery has just been repaired with vein grafting weeks or months before. This operation is principally indicated for complete brachial plexus root avulsion, whereby very limited extraplexal donor nerves on the ipsilateral facet are available. The second-stage operation is performed 6 to 9 months later when regenerating axons have reached the axilla of the injured aspect. This aware effort restricts the spontaneous performance of the reconstructed nerve. Our expertise in children has indicated that the extent of co-contraction is affected by the modality of switch. Nearly impartial motor recovery was gained only in patients with restore of nerves innervating the upper trunk or both the biceps and median nerves, though co-contraction was noteworthy if the C7 was transferred to the median or the radial nerve alone. Recently, some authors have reported contralateral C7 transfer via a prespinal and retropharyngeal tunnel to the ipsilateral higher or the lower trunk by standard nerve grafts with a length of as a lot as 7 cm and even by a direct coaptation. This method is indicated particularly in young youngsters in whom the size of grafting can be up to 10 cm. Intraoperatively, the biceps department is dissected intraneurally and transected as proximally as potential, and at a degree where the biceps department enters into the biceps, one fascicle of the ulnar nerve is divided and sutured directly to the biceps branch. Reported operative outcomes were usually satisfying: recovery of elbow flexion (M3) was obtained in 100 percent of the circumstances with avulsion of C5-C640,forty one and in 70% with avulsion of C5-C6-C7. A precondition of efficiency of this switch is sweet strength of the triceps, which is a minimal of M4. The anterior branch of the axillary nerve is dissected proximally into the quadrilateral area and cut. The nerve to the lengthy head of the triceps is divided at its entrance into the muscle and transferred to the divided anterior branch of the axillary nerve. Postoperatively, the power of C7 musculature could be weaker by M1 grade than that earlier than surgery, however it recovers significantly over a period of 6 months. This is as a result of musculature generally classed as C7 can really be innervated significantly by the lower trunk. In a collection of 40 patients who had received direct coaptation of the phrenic nerve to the anterior division of the higher trunk for restoration of elbow flexion, 82. In the previous, the hypoglossal nerve has been used for nerve transfer reconstruction of brachial plexus palsy. In a report of 14 patients who had undergone this switch, by a nerve graft with mean length of 15 cm in adults and 7. This risk arises because the supinator is supplied by C5 and C6 fibers operating within the deep department of the radial nerve, in distinction to the C7-dominated bulk of radial nerve components. In a report of obturator nerve switch to the femoral nerve, a affected person with femoral nerve palsy, which was brought on by removal of a tumor involving the lumbar plexus, obtained M4 strength of the quadriceps and could stroll practically normally. It can additionally be utilized for lengthy nerve defects when regenerating axons after nerve grafting have to progress over an extended distance to reach the goal. Contralateral C7 switch for treatment of brachial plexus root avulsions in children: a report of 12 instances. Clinical use of supinator motor branch transfer to the posterior interosseous nerve in C7�T1 brachial plexus palsies. Intratemporal facial nerve switch with direct coaptation to the hypoglossal nerve. Clinical software of ipsilateral C7 nerve root switch for therapy of C5 and C6 avulsion of brachial plexus. Anatomic research of the intercostal nerve transfer to the suprascapular nerve and a case report. Evaluation of intercostal to musculocutaneous nerve transfer in reconstructive brachial plexus surgery. Suprascapular nerve reconstruction in 118 cases of grownup posttraumatic brachial plexus. Different practical reorganization of motor cortex after switch of the contralateral C7 to totally different recipient nerves in younger rats with complete brachial plexus root avulsion. Nerve transfer surgical procedure for adult brachial plexus harm: A 10-year experience at Louisiana State University. Nerve switch to deltoid muscle using the nerve to the long head of the triceps, half 1: an anatomic feasibility study. Long thoracic nerve neurotization for restoration of shoulder operate in C5-7 brachial plexus preganglionic accidents: case report. Sensory restoration of the hand with intercostal nerve transfer following complete avulsion of the brachial plexus. Results of nerve switch methods for restoration of shoulder and elbow operate in the context of a Meta-analysis of the English literature. Results of intercostal nerve switch to the musculocutaneous nerve in brachial plexus delivery palsy. Intercostal nerve transfer of the musculocutaneous nerve in avulsed brachial plexus injuries: analysis of sixty six sufferers. Spinal accent neurotization for restoration of elbow flexion in avulsion accidents of the brachial plexus.
Syndromes
- Weight loss
- Ultrasound of the abdomen or kidneys
- Apple juice
- Arthritis
- Oxygen, if needed
- Contact dermatitis (may be caused by poison ivy)
- Pregnancy ultrasound
- Portal vein obstruction (liver)
Buy 120mg starlix fast delivery
Simple decompression versus anterior submuscular transposition of the ulnar nerve in extreme cubital tunnel syndrome: a potential randomized research hiv infection symptoms in tamil starlix 120mg purchase online. Simple decompression or subcutaneous anterior transposition of the ulnar nerve for cubital tunnel syndrome highest hiv infection rates world purchase 120 mg starlix with mastercard. Simple decompression or anterior subcutaneous transposition for ulnar neuropathy on the elbow: a cost-minimization analysis-Part 2. Submuscular transposition of the ulnar nerve: evaluate of security, efficacy and correlation with neurophysiological consequence. Analysis of higher and decrease extremity peripheral nerve injuries in a population of patients with multiple injuries. Relationship of the frequent peroneal nerve and its branches to the pinnacle and neck of the fibula. Bilateral widespread peroneal nerve palsy secondary to extended squatting in natural childbirth. Role of magnetic resonance imaging in entrapment and compressive neuropathy-what, the place, and the method to see the peripheral nerves on the musculoskeletal magnetic one hundred thirty. High-resolution sonography of the widespread peroneal nerve: detection of intraneural ganglia. Imaging of foot and ankle nerve entrapment syndromes: from well-demonstrated to unfamiliar websites. Results of decompression of 4 medial ankle tunnels within the treatment of tarsal tunnels syndrome. Usefulness of electrodiagnostic methods within the evaluation of suspected tarsal tunnel syndrome: an evidence-based evaluate. Ultrasound of nerve entrapments in osteofibrous tunnels of the upper and decrease limbs. High-resolution sonography of lower extremity peripheral nerves: anatomic correlation and spectrum of disease. A optimistic Tinel signal as predictor of pain relief or sensory restoration after decompression of chronic tibial nerve compression in patients with diabetic neuropathy. The optimistic effect of neurolysis on diabetic patients with compressed nerves of the decrease extremities: a scientific evaluate and meta-analysis. Prevention of ulceration, amputation, and discount of hospitalization: outcomes of a 249 2031. The relationship of the double crush to carpal tunnel syndrome (an evaluation of 1,000 cases of carpal tunnel syndrome). In its most general sense the time period covers any nerve on this physique region, whereas in its most specific sense, it refers only to these nonspinal anatomic elements rising from the chest throughout the circle of the first rib. Brachial plexus entrapments in a given subcategory are usually topic to definite goal analysis and proof by standardized diagnostic examinations. The subdiagnoses include fibrous bands proximal to the scalene muscles, anterior scalene muscle syndromes involving spasm or hypertrophy of the anterior scalene muscle, anomalous cervical rib syndromes, proximal fibrous band entrapments, middle scalene muscle syndromes, entrapment of the midplexus at the degree of the clavicle and first rib, distal plexus entrapments ensuing from adhesions, and axillary nerve syndromes. This includes the accent nerve to the extent that it affects the sternocleidomastoid and trapezius muscular tissues, the lengthy thoracic nerve as it affects the serratus anterior muscle,12 the dorsal scapular nerve as it affects the levator scapulae and rhomboid muscles and the cervical plexus. The term moreover refers to various vascular entrapments affecting the subclavian, brachial, and axillary arteries and veins but also together with the jugular vein in these contexts in which venous outflow is obstructed. Common themes amongst these numerous component subdiagnoses, aside from their shared space of location within the physique, is that their origin is in degenerative or congenital issues, although the effects of moderately extreme trauma, such as whiplash injury, are included as nicely. From a nerve diagnosis viewpoint, only tumors or important intrinsic nerve accidents and discontinuities of the brachial plexus are actually excluded. Vascular impingement on the thoracic outlet Brachial plexus entrapment by proximal fibrous band Interscalene brachial plexus entrapment Middle scalene syndrome First rib neurologic impingement syndrome Cervical rib syndromes Post�clavicle fracture syndromes Gilliatt-Sumner hand Distal plexus/axillary nerve entrapment Diffuse brachial plexus neuritis/neuropathy/fibrosis Each of these classes has its own distinct presentation, physical examination findings, check results, therapy strategy, and outcomes, though some overlap may exist. A variety of specialists on this area have proven that, specialized neuroimaging of the brachial plexus. Additionally, to an even higher diploma than in spinal analysis, image-guided injections function critically important trendy confirmatory tests and establish causality. This is an issue with terminology and never a discovering that each one elements of the brachial plexus are resistant to entrapment. However, the median nerve, with widespread entrapment at the carpal tunnel, conducts C6 sensory fibers to the first and second digits and C7 sensory fibers to the third digit along with T1 motor innervation to the thenar eminence. Therefore a patient with motor abnormalities affecting both thenar and hypothenar eminences however with sensory abnormality and pain into solely the fourth and fifth digits is more likely to be suffering from entrapment of the lower trunk of the brachial plexus on the scalene triangle, which affects C8 and T1 only. Physical Examination Findings Diagnosis of a brachial plexus entrapment requires each a "neurologic examination" and a "peripheral nerve examination. The examiner assesses the lumbricals (the examiner hyperextends the metacarpal-phalangeal joint and asks the patient to prolong the proximal and distal interphalangeal joints towards resistance), the digital interosseous abductors and adductors (the patient spreads the fingers aside and draws them together against resistance), opposition of the primary and fifth digits, and the primary to second fingertip pincer grip, as well as examining for any atrophy of the thenar or hypothenar eminence. Strength of hand pronation and supination and wrist extension, flexion, and radial and ulnar deviation are all assessed, in addition to gross grip power and finger extension. Separately, arm abduction should be examined distinctly as to the first 30 degrees, driven by the supraspinatus, in addition to for 30 to ninety levels, that are progressively driven by the deltoid. With the arm held at ninety degrees and the forearm prolonged, the examiner assesses energy for additional abduction, adduction, protraction, and retraction. Next the examiner assesses for biceps, triceps, and brachioradialis reflexes, with quick comparability to patellar and Achilles tendon reflexes. Next, percussion is addressed to the course of the radial, posterior interosseous, median, and ulnar nerves simply distal to the elbow, on the elbow, and progressively proximally for the radial, median, and ulnar nerves within the upper arm approaching the axilla. Within the axilla, the quadrangular space ought to be palpated for any axillary nerve entrapment as properly as assessing the deep surface of the pectoralis muscle tissue from within the axilla after which again assessing the distal plexus by percussing it through the pectoralis muscular tissues from an anterior contact level on the chest under the clavicle. Then the supraclavicular area must be methodically assessed by distinct percussion of the anterior scalene, center scalene, and levator scapulae muscle tissue. The posterior shoulder must be assessed as to supraspinatus and trapezius muscular tissues, the mesial scapular border, and the rhomboid muscular tissues for sensitivity from muscle spasm. The sternocleidomastoid muscle must be palpated in sufferers with related ear ache, as a result of this muscle might apply painful traction to the mastoid area, or trapezius ache, because of the incidence of accessory nerve entrapments on the deep floor of the sternocleidomastoid muscle. Another widespread presentation includes pain alongside the mesial scapular border in a patient with no cervical backbone pathology that would be in maintaining with such an isolated focus of neurologic pain. This serratus anterior muscle pain can also be perceived alongside the lateral body wall. Scapular winging is usually detectable by having the patient face a wall and place his or her palms on the wall, push back towards the examiner, after which shrug the shoulders upward. An axillary nerve syndrome can come up where the axillary nerve separates from the radial nerve on the terminus of the posterior cord. The axillary nerve turns sharply in a posterior path, passing through the quadrangular area within the posterior wall of the axilla, the place palpation ought to identify a painful nerve element. Causes of scalene muscle tears include whiplash damage in rear-end motorized vehicle accidents, some highintensity sport actions, and extra pressure when the shoulders are taped or pulled for radiographs during cervical backbone surgery. B, Nerve-perpendicular views (correlated spatially with the coronal view using radiology software program corresponding to eFilm) can be utilized to sequentially follow nerve caliber and picture intensity, while identifying particular components. In A, the white arrow points to an orange cross that the software program has placed on the C6 spinal nerve when the corresponding nerve cross part has been chosen at the pink arrow in B. Cross-sectional views of the C5, C7, C8, and T1 parts are identified with small green arrows in B.
Starlix 120mg purchase visa
With this in hand hiv infection when undetectable 120 mg starlix effective, one can determine whether or not to proceed with resection and restore hiv infection treatment guidelines starlix 120 mg cheap fast delivery, or neuroplasty and removal of scar tissue. When a lesion is clearly nonfunctional and resection and restore are required, neurophysiology may be helpful to decide the region to be resected. On the distal facet, a similar state of affairs is restricted by the degeneration that begins days after harm. At least 3000 nerve fibers a minimal of 5 microns in diameter are required to see a recordable potential. In common, this many fibers in a recovering nerve predicts spontaneous practical recovery. With an interelectrode distance lower than 2 cm, the electrical current spreads too significantly from the stimulating to the recording electrodes. Sometimes a stimulating or recording electrode is placed outdoors the surgical field with a subdermal needle or surface electrodes. Some effort has been given to measure specifically the axons of greatest interest, the motor axons. During hip replacement revisions, the sciatic nerve has been monitored with alternate strategies. These points serve equally properly throughout all areas of intraoperative neurophysiologic monitoring. Among the various strategies used for intraoperative neurophysiologic monitoring,31-33 just a few have been the subject of highquality formal outcome research. The most dependable of the research that have been done underlie the apply suggestions to use monitoring as an choice to alert the surgeon to incipient problems in time to intervene and improve outcomes. Among an important of those reasons is the truth that the intraoperative uses of these two methods range significantly. Wellcontrolled research for each sort of software would take numerous topics keen to be unmonitored and an institutional review board keen to allow randomly unmonitored patients. Preoperative and intraoperative electrophysiologic evaluation of brachial plexus injuries. Value of nerve action potentials in the surgical administration of traumatic nerve lesions. Electrophysiologically guided untethering of secondary tethered spinal cord syndrome. Intraoperative monitoring of lower cranial nerves in skull base surgery: technical report and evaluate of 123 monitored circumstances. Nerve transection without neurotonic discharges throughout intraoperative electromyographic monitoring. Intraoperative monitoring of segmental spinal nerve root function with free-run and electrically-triggered electromyography and spinal wire operate with reflexes and F-responses. Preoperative and intraoperative electro-physiologic evaluation of brachial plexus injuries. Intra-operative electrophysiological analysis of spinal root avulsion during surgical restore of brachial plexus stretch injuries. Intraoperative nerve motion potential recordings: technical issues, problems, and pitfalls. Electromyography, nerve action potential, and compound motor motion potentials in obstetric brachial plexus lesions: validation within the absence of a "gold normal. Intraoperative spinal monitoring with somatosensory and transcranial electrical motor evoked potentials. Filler the development of most subspecialties in neurosurgery has been intently associated with developments in imaging: x-ray studies, pneumoencephalography, and angiography, all of which have played a large position in guiding backbone and mind surgical planning for many many years. Nonetheless, peripheral nerve surgical procedure is one subspecialty by which scientific physical examination and exploratory surgical procedure to outline the pathologic process have continued to play a dominant role. The resulting neurograms then served as a model for discovering further nondiffusion tractographic methods for peripheral nerves. However, nerve ultrasonography is capable of confirming adjustments in nerve caliber in settings of disease32 and for guidance of some procedures. The two major forms of neurographic techniques which were described are diffusion neurography and T2-based neurography. T2-based neurography, nonetheless, could be reliably utilized with many current top-quality scientific scanners, with minor modifications. Once the technical limitations are resolved, nonetheless, T2-based neurography has the benefit of improvement in quality of detail because the severity of the nerve abnormality increases-the opposite of diffusion neurography. Diffusion-Based Tractographic Techniques Neural tissue is amongst a quantity of tissues within the body that show the property of linearly correlated water diffusion. Instead of diffusing freely in any path (isotropic diffusion), the water molecules in neural tissue are inclined to move linearly alongside the main longitudinal axis of the neural tissue (anisotropic diffusion). The detailed biophysical foundation of this restricted diffusion is still not fully understood as a result of water molecules should move freely via cell membranes. Tissue distinction arises on T1- and T2-weighted pictures as a outcome of the spinning protons in water molecules interact with surrounding tissues and with one another, and these interactions trigger small changes within the spin price in order that the spins desynchronize. In diffusion-based imaging, tissue distinction additionally arises as a result of the relative diploma of diffusional isotropy and anisotropy in a given tissue can have an result on the speed of sign decay in that tissue. When diffusion carries a proton to a new position in the gradient, its native magnetic field power adjustments slightly, and thus its spin rate adjustments, which outcomes in desynchronization of the spins. When the gradient is parallel, the nerve protons transfer rapidly to new positions in the gradient, and their sign decays extra rapidly than in an isotropic tissue. When the course of the gradient is strictly perpendicular, the protons stay in the identical subject energy area of the gradient as they diffuse alongside the longitudinal axis of the nerve, and so they show little or no signal decay in relation to surrounding isotropic tissues. In a peripheral nerve, anisotropic water makes up only a small fraction of the whole water in the nerve, and therefore the impact becomes apparent solely when both fats and isotropic water alerts are suppressed; this was one of many discoveries made by Howe and colleagues in 1992. For each peripheral and central nervous system tissue, Filler and colleagues4,9 also identified that it was possible to consider each voxel (three-dimensional pixel) in an image volume through the use of multiple gradient directions to determine both the magnitude and the path in three-dimensional space of the anisotropy after which utilizing this information to depict precise curving neural tracts, rather than simply displaying two-dimensional variations in distinction in cross sections. Until then, the relative amount of anisotropic diffusion had been used to assign contrast to a given picture pixel in a cross section or to assign colors to areas of neural tissue that respond to a given gradient course. In tractography, however, each voxel is represented by an arrow that could be a vector in three-dimensional area, which represents a tensor. Multiple vectors-revealing crossing and splitting fibers-are calculated in spherical vector ("mannequin free") strategies. A number of three-dimensional computer graphic methods are now used to assemble tractographic pictures from these linear anisotropy traces: that is the basis of tractographic diffusion tensor and vector imaging. Of most importance was that demonstrating the presence of fascicles became the premise of dependable identification of nerve, in distinction from other tissues which could be comparable in measurement and form in cross sectional photographs. Endoneurial fluid is a low-protein liquid that lies inside the privileged house of the endoneurium, confined by the perineurial blood-nerve barrier, and bathes the axons. A related impact could be produced with inversion recovery�type sequences that obtain fats suppression. Then, by number of an acceptable echo time (90 msec), a T2 weighting may be achieved that ends in suppression of muscle sign, thereby leaving many of the sign from endoneurial fluid intact. Any considered one of several methods can be used to suppress brilliant fluid signals from flowing blood.
Starlix 120mg buy discount on line
The effect of botulinum toxin sort A treatment of the lower extremity on the level of useful abilities in kids with cerebral palsy: evaluation with aim attainment scaling hiv infection from dried blood starlix 120mg cheap with visa. Analgesic effects of botulinum toxin A: a randomized antiviral over the counter medicine starlix 120 mg discount free shipping, placebo-controlled medical trial. Medium-term response characterisation and risk issue evaluation of botulinum toxin sort A within the management of spasticity in youngsters with cerebral palsy. The use of botulinum toxin sort A in youngsters with cerebral palsy: a retrospective study. Efficacy of botulinum toxin A, serial casting, and combined remedy for spastic equinus: a retrospective evaluation. A pilot research of delayed versus immediate serial casting after botulinum toxin injection for partially reducible spastic equinus. Changes in ankle spasticity and strength following selective dorsal rhizotomy and bodily therapy for spastic cerebral palsy. Changes in hip spasticity and energy following selective dorsal rhizotomy and bodily remedy for spastic cerebral palsy. Long-term end result after selective dorsal rhizotomy in kids with spastic cerebral palsy. Pilot research on trihexyphenidyl in the remedy of dystonia in youngsters with cerebral palsy. Levetiracetam therapy for remedy of choreoathetosis in dyskinetic cerebral palsy. Selective dorsal rhizotomy versus orthopedic surgical procedure: a multidimensional evaluation of end result efficacy. Partington the intrathecal delivery of baclofen, by way of an implanted pump, has been an evolving therapy for more than 30 years. As a results of this need, the overwhelming majority of medical expertise and revealed literature involves using the programmable SynchroMed infusion pump (Medtronic, Inc. In this setting, spasticity is outlined as a velocity-dependent enhance in resistance to passive movement. The Ashworth Scale, with some minor variations, is in widest use for measuring spasticity (Table 242-1). Regardless of the choice of scale, crucial facet of a grading system is to develop inner consistency, significantly in multidisciplinary clinics. The screening test sometimes concerned intrathecal injection of baclofen, both as a bolus dose administered by way of lumbar puncture or with a lumbar drain catheter attached to an exterior drug pump. Presumably, as the bolus effect wears off, the patient transiently experiences a stage of tone management that may be acceptable in a long-term, steady-state scenario. In my program, unpublished information noted that in 100 consecutive patients present process check doses, 98 had a positive response and went on to undergo implantation. As a consequence of this finding, screening exams are actually hardly ever utilized in my program. Although the typical screening take a look at is carried out in order to affirm a response to the drug, one other type of the take a look at to consider is using a catheter-based trial to examine the connection between the anatomic catheter place and the result. Clinical evaluation of tone is made and recorded once a gentle state is achieved (which could be hours or days later), and then the catheter is pulled down a quantity of segments to the next stage of curiosity. The remark is repeated at the new level, and the entire course of is then continued till the catheter is low enough that it may be eliminated. For example, a baby could also be started on oral baclofen however can shortly attain a dose restrict at which the unwanted effects outweigh the specified effect on tone. Focal injection therapies (usually with both botulinum toxin or phenol) have wonderful results however are of restricted use when the child has widespread hypertonicity. This last group of sufferers is most frequently only ambulating in remedy or household settings. For patients with a prior posterior spinal fusion with instrumentation, pump placement is identical as described, however catheter placement needs modification. If the fusion is completed at a time when the lengthy run pump surgery is anticipated, one choice is to coordinate with the spine surgeon to leave a segment instrumented however without bone graft, so that a puncture through a small incision can nonetheless be done (assuming that the extent can be identified). A catheter can be positioned after which tucked into a subcutaneous pocket in the paraspinal area at the time of fusion. A catheter may be placed above an current fusion, for instance, via a small upper thoracic or cervical laminotomy, after which tunneled down into the thoracic backbone. I favor this method, because it minimizes the length of subcutaneous tubing and since coming into through the fusion mass exposes the tubing to nearly no stresses from spinal movement. Both of these elements are believed to contribute to reducing the danger of catheter fracture. When drilling down to the dura, the surgeon must take care to enable for the regularly present rotational deformities. In the most difficult instances, I favor to place the catheter with the patient in the prone position (to allow for greatest surgical management, use of fluoroscopy, etc. For children with hydrocephalus and shunts, the basic surgical approach remains the identical, but profitable catheter placement could also be tougher to affirm. On event, it has been necessary to make a small laminotomy to visualize the dura instantly and confirm puncture. Postoperatively, an elastic stomach binder is positioned to improve healing of the pocket. In my program the kid can additionally be saved at flat bed rest for 72 hours postoperatively, though my colleagues and I are presently conducting a prospective trial to set up whether or not a shorter period has related, or improved, morbidity. The laterality of the stomach pocket is a matter of surgeon and affected person selection, but most often the best facet is used. At my institution, antibiotic choice is a perform of which pathogens have been encountered in scientific follow in addition to of an understanding of carrier states within the affected person population. A small incision is planned over a decrease lumbar interspace, although care is taken to carry out the lumbar puncture slightly off-midline in order to keep away from having the catheter traverse the interspinous ligament. Currently, the one catheter out there with the SynchroMed pump system is the Ascenda catheter (Medtronic). Care must be taken as a end result of this catheter is troublesome to visualize radiographically once the guidewire is removed. Subfascial location is often used in smaller sufferers and in sufferers with a history of an infection, but some sufferers with subfascial pockets have complained of increased ache with refills as they age. Rarely, a child is instantly too loose and/or sedated postoperatively, and the dose is decreased. The final optimum dose is very empiric and can probably not be established for 6 to 12 months after pump placement. Higher doses may be needed in children with spastic dystonia, however doses larger than 1500 �g/day are extremely uncommon.
120 mg starlix purchase with amex
Five of the seven patients exhibited long-term benefit after 7 years of follow-up hiv infection personal stories discount 120 mg starlix mastercard. They really helpful the use of only 4-mm isocenters antiviral cold sore cream 120mg starlix order otc,6 the results of which appeared to be as efficacious as those noticed after radiofrequency lesioning. In different research, Mindus and colleagues54 reported that the lowest efficient target dose was a hundred and sixty Gy. They used Gamma Knife radiosurgery to create a conformal volume of radiation for the amygdala and hippocampus. The goal volume was about 7 cm3 and included the pinnacle and body of the hippocampus, the anterior portion of the parahippocampal gyrus, and the basolateral region of the amygdaloid complicated. In 2004, R�gis and associates63 reported a potential multicenter examine of 20 patients treated with Gamma Knife radiosurgery for mesial temporal lobe epilepsy. Analysis of seizure control after a 2-year follow-up showed that the median variety of seizures per month dropped from 6. The solely everlasting neurological deficits have been 9 visual area deficits, though five sufferers had transient unwanted effects similar to melancholy, headache, nausea, vomiting, and imbalance. In another multicenter trial of 2009, Barbaro and coworkers64 randomized 30 sufferers with mesial temporal lobe epilepsy to obtain both a excessive (24 Gy, n = 13) or low (20 Gy, n = 17) dose delivered to the target. Ten patients in each group have been seizure free at 36 months of follow-up, giving remission charges of 77% within the high-dose group and 59% in the lowdose group. In phrases of neurocognitive and psychological outcomes as properly as seizure management results, a quantity of studies demonstrated the security and efficacy of radiosurgery for mesial temporal lobe epilepsy. R�gis and associates63 famous no vital cognitive deficits at 24 months postoperatively in the multicenter research. A longterm follow-up research after radiosurgery reported by Bartolomei and coworkers65 showed that the neuropsychological outcomes have been steady. A prospective research by Quigg and colleagues66 demonstrated that neuropsychological parameters such as language, verbal reminiscence, cognitive efficiency/mental flexibility, and temper had been comparable earlier than and after radiosurgery. These research showed the safety and efficacy of radiosurgery for mesial temporal lobe epilepsy. In 2000, R�gis and associates67 used Gamma Knife radiosurgery to treat 10 sufferers with medically refractory epilepsy associated with hypothalamic hamartoma. Another report of 30 patients by R�gis and associates68 demonstrated the protection and efficacy of radiosurgery for hypothalamic hamartoma. These research confirmed a close relationship between seizure consequence and the marginal dose. Marginal doses of 17 Gy or higher appear to be required in Gamma Knife radiosurgery. A multicenter, potential pilot study of Gamma Knife radiosurgery for mesial temporal lobe epilepsy: seizure response, opposed occasions, and verbal memory. Prospective managed trial of Gamma Knife surgery for important trigeminal neuralgia. Gamma Knife radiosurgery for trigeminal neuralgia: analysis of a multi institutional study. Gamma Knife radiosurgery for thalamotomy in parkinsonian tremor: a five-year expertise. Gamma Knife radiosurgery for remedy of trigeminal neuralgia: idiopathic and tumor related. Histological effects of trigeminal nerve radiosurgery in a primate mannequin: implications for trigeminal neuralgia radiosurgery. Gamma Knife surgery for trigeminal neuralgia: end result, imaging, and brainstem correlates. Gamma Knife radiosurgery for trigeminal neuralgia: the Washington University preliminary experience. Glycerol rhizotomy versus Gamma Knife radiosurgery for the remedy of trigeminal neuralgia: an analysis of patients treated at one establishment. Stereotactic radiosurgery for primary trigeminal neuralgia: state of the proof and recommendations for future reviews. Gamma Knife surgery for idiopathic trigeminal neuralgia carried out utilizing a far-anterior cisternal target and a high dose of radiation. Radiosurgical treatment of trigeminal neuralgia: evaluating high quality of life and therapy outcomes. Stereotactic radiosurgery for major trigeminal neuralgia using the Leksell Gamma unit. Gamma Knife remedy of trigeminal neuralgia: scientific and electrophysiological examine. Cyberknife concentrating on the pterygopalatine ganglion for the remedy of continual cluster headaches. Long-term end result of Gamma Knife radiosurgery for remedy of typical trigeminal neuralgia. Stereotactic gammathalamotomy with a computerized brain atlas: technical case report. Gamma Knife thalamotomy for movement issues: analysis of the thalamic lesion and medical outcomes. Gamma Knife thalamotomy and pallidotomy in patients with motion disorders: preliminary outcomes. Gamma Knife surgical procedure for cancer pain-pituitary gland-stalk ablation: a multicenter potential protocol since 2002. Role of pituitary radiosurgery for the administration of intractable ache and potential future functions. Magnetic resonance photographs related to clinical end result after psychosurgical intervention in extreme anxiousness disorder. Radiosurgical lesions in the normal human mind 17 years after Gamma Knife capsulotomy. Treatment of resistant obsessive-compulsive disorder with ventral capsular/ventral striatal gamma capsulotomy: a pilot prospective examine. Subnecrotic stereotactic radiosurgery controlling epilepsy produced by kainic acid injection in rats. First selective amygdalohippocampal radiosurgery for mesial temporal lobe epilepsy. Gerszten and Kristina Gerszten Malignancy involving the spine is an important scientific drawback in oncology, together with both primary and secondary malignant spine tumors. In a examine of 2000 sufferers with bony metastases, almost 70% were found to have vertebral body metastases. The precept methods used to treat malignant spine tumors are radiation therapy and surgical procedure. Chemotherapy, radionuclide therapy, hormonal therapy, and immunotherapy therapies also play a big position in chosen tumors. Surgery is normally reserved for spinal instability or subluxation, persistent neurological deficits regardless of different forms of remedy, and intractable pain attributable to an isolated lesion. Standard surgical interventions right now embody percutaneous cement augmentation, posterolateral decompression, and anterior and posterior segmental fixation. However, open surgical procedures for malignant spine tumors are related to vital morbidity and a excessive complication price on this already debilitated patient population.
Wu Long (Oolong Tea). Starlix.
- What is Oolong Tea?
- What other names is Oolong Tea known by?
- Are there any interactions with medications?
- Reducing the risk of ovarian cancer.
- Skin allergies, diabetes, high blood pressure, preventing tooth decay, reducing the risk of cancer, osteoporosis, promoting weight loss, and other conditions.
- Are there safety concerns?
- How does Oolong Tea work?
- Dosing considerations for Oolong Tea.
- Mental alertness.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97045
Starlix 120mg discount
A multicenter potential research of this method in diabetic sufferers reported a discount in the prevalence of foot ulceration in 665 patients with out earlier ulceration from 15% to 0 hiv infection early signs and symptoms generic 120 mg starlix. The authors declare that this triple nerve decompression technique also improves sensation and reduces foot pain in diabetic sufferers with sensory neuropathy antiviral for cold buy cheap starlix 120mg line. Simple decompression or anterior subcutaneous transposition for ulnar neuropathy on the elbow: a cost-minimization analysis-part 2. Prospective randomized controlled examine evaluating easy decompression versus anterior subcutaneous transposition for idiopathic neuropathy of the ulnar nerve at the elbow: part 1. Neurosurgical prevention of ulceration and amputation by decompression of lower extremity peripheral nerves in diabetic neuropathy: replace 2006. Role of magnetic resonance imaging in entrapment and compressive neuropathy-what, where, and tips on how to see the peripheral nerves on the musculoskeletal magnetic resonance picture: part 1. A novel endoscopic technique in treating single nerve entrapment syndromes with special consideration to ulnar nerve transposition and tarsal tunnel release: clinical software. Estimating the prevalence of delayed median nerve conduction in the general inhabitants. A sequence of cases of parasthesias, primarily of the hand, or periodic recurrence, and presumably of vasomotor origin. The precept of decompression in the therapy of certain diseases of the peripheral nerves. Median nerve compression within the carpal tunnel-functional response to experimentally induced managed stress. Role of magnetic resonance imaging in entrapment and compressive neuropathy-what, where, and how to see the peripheral nerves on the musculoskeletal magnetic resonance image: half 2. Carpal tunnel syndrome and the Riche-Cannieu anastomosis: electrophysiologic findings. Increase of vibration threshold throughout wrist flexion in patients with carpal tunnel syndrome. Correlation of clinical indicators with nerve conduction checks within the diagnosis of carpal tunnel syndrome. The sensitivity and specificity of checks for carpal tunnel syndrome range with the comparison topics. The position of ultrasonographic measurements of the median nerve in the analysis of carpal tunnel syndrome. The value of ultrasonographic measurement in carpal tunnel syndrome in patients with adverse electrodiagnostic tests. Correlating ultrasound findings of carpal tunnel syndrome with nerve conduction studies. The position of ultrasound within the prognosis and management of carpal tunnel syndrome: a new paradigm. Carpal tunnel syndrome: correlation of magnetic resonance imaging, medical, electrodiagnostic, and intraoperative findings. The utility of magnetic resonance imaging in evaluating peripheral nerve disorders. Median nerve compression may be detected by magnetic resonance imaging of the carpal tunnel. Efficacy of a fabricated personalized splint and tendon and nerve gliding exercises for the remedy of carpal tunnel syndrome: a randomized controlled trial. Stress carpal tunnel pressures in patients with carpal tunnel syndrome and normal patients. Neutral wrist splinting in carpal tunnel syndrome: a comparison of night-only versus full-time put on directions. Position of the wrist related to the bottom carpal-tunnel strain: implications for splint design. An revolutionary hand brace for carpal tunnel syndrome: a randomized controlled trial. Splinting vs surgical procedure within the treatment of carpal tunnel syndrome: a randomized managed trial. A randomized managed trial of surgical procedure vs steroid injection for carpal tunnel syndrome. Long time period follow-up of carpal tunnel syndrome during being pregnant: a cohort study and review of the literature. Prospective research of constructive factors for improvement of carpal tunnel syndrome in pregnant girls. Distal nerve blocks on the wrist for outpatient carpal tunnel surgery offer intraoperative cardiovascular stability and cut back discharge time. Endoscopic release of the carpal tunnel: a randomized potential multicenter study. Measurement of strain within the carpal canal earlier than and after endoscopic administration of carpal tunnel syndrome. Endoscopic launch of the carpal ligament: a model new approach for carpal tunnel syndrome. A 12-year experience using the Brown two-portal endoscopic process of transverse carpal ligament release in 14,722 sufferers: defining a new paradigm in the therapy of carpal tunnel syndrome. Intra-individual comparability between open and 2-portal endoscopic launch in clinically matched bilateral carpal syndrome. Deformity of the small finger caused by avulsion of the insertion of the third volar interosseous muscle. Dissociated small hand muscle atrophy in amyotrophic lateral sclerosis: frequency, extent, and specificity. Medial brachial and antebrachial cutaneous nerve injuries: impact on end result in revision cubital tunnel surgical procedure. Late outcomes of eradicating the medial humeral epicondyle for traumatic ulnar neuritis. Anterior transposition compared with simple decompression for treatment of cubital tunnel syndrome. Prospective randomized controlled study comparing simple decompression versus anterior subcutaneous transposition for idiopathic neuropathy of the ulnar nerve at the elbow: Part 1. Randomized, potential research evaluating ulnar neurolysis in situ with submuscular transposition. A, In the conventional plexus, the cervical spinal nerves and trunks of the brachial plexus comply with a straight trajectory with even spacing. B, Scalene syndrome is demonstrated by a gentle deformation of the course of the nerve components and lack of space between them (arrows). C2, A extra anterior image aircraft in the same patient exhibiting both a pointy kink (K) in the center of the decrease trunk related to a fibrous band and nerve hyperintensity (H) in keeping with decrease trunk motor symptoms. This kind of pathology is extra prone to respond to supraclavicular neuroplasty than to first rib resection. A, Hyperintense axillary nerve (ax) in a performer who developed severe axillary and deltoid pain associated with choreographic work. Adhesion of the distal plexus could result in axillary nerve irritation because of differential motion on the quadrangular area through which it passes after a short distance of travel. Patients often current with failed "rotator cuff" surgical procedure undertaken for shoulder ache that has been misdiagnosed.
Purchase starlix 120 mg without prescription
Comparison of postoperative radiotherapy and chemotherapy in the multidisciplinary management of malignant gliomas hiv infection rate per exposure purchase starlix 120 mg without a prescription. A joint Radiation Therapy Oncology Group and Eastern Cooperative Oncology Group Study antiviral blu ray starlix 120mg purchase visa. Equivalence of radiation schedules for the palliative remedy of brain metastases in sufferers with favorable prognosis. Treatment of spina epidural metastases: randomized prospective comparability of laminectomy and radiotherapy. Fractionated external beam radiation therapy for meningiomas of the cavernous sinus. Stereotactic radiosurgery plus complete mind radiotherapy versus complete mind radiotherapy alone for patients with a quantity of brain metastases. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for remedy of brain metastases. Neurocognition in patients with mind metastases handled with radiosurgery or radiosurgery plus whole-brain irradiation: a randomized managed trial. Long-term follow-up of acoustic schwannoma radiosurgery with marginal tumor doses of 12 to 13 Gy. Relative roles of microsurgery and stereotactic radiosurgery for the treatment of sufferers with cranial meningiomas: a single surgeon 4-year integrated expertise using both modalities. Stereotactic radiosurgery for pituitary adenomas: an intermediate evaluation of its security, efficacy, and position in the neurosurgical treatment armamentarium. Long-term results of Gamma Knife surgery for the remedy of craniopharyngioma in 98 consecutive cases. Gamma knife radiosurgery for glomus jugulare tumors: volumetric evaluation in 17 sufferers. An evaluation of the dose-response for arteriovenous malformation radiosurgery and other elements affecting obliteration. Recommendations for the administration of intracranial arteriovenous malformations: a press release for healthcare professionals from a particular writing group of the Stroke Council, American Stroke Association. A prospective cohort study of microvascular decompression and gamma knife stereotactic radiosurgery for sufferers with trigeminal neuralgia. Long-term outcomes and late problems after intracavitary yttrium-90 colloid irradiation of 261 2143. Intracavitary brachytherapy utilizing stereotactically utilized phosphorous-32 colloid for treatment of cystic craniopharyngiomas in 53 patients. GliaSite brachytherapy for remedy of recurrent malignant gliomas: a retrospective multiinstitutional evaluation. GliaSite brachytherapy boost as part of preliminary treatment of glioblastoma multiforme: a retrospective multi-institutional pilot study. Roentgentherapy of epitheliomas of the tonsillar region, hypopharynx and larynx from 1920 to 1926. Development and aftercare of medical guidelines: the balance between rigor and pragmatism. Durability of Class I American College of Cardiology/American Heart Association clinical follow guidelines suggestions. Level of scientific evidence underlying recommendations arising from the Comprehensive Cancer Network Clinical Practice Guidelines. Attitudes towards and use of cancer management pointers in a nationwide sample of medical oncologists and surgeons. The focus of oxygen dissolved in tissues on the time of irradiation as a think about radiotherapy. Temperature dependence of the restore of X-ray damage in surviving cells (aerobic and hypoxic). The impact of a number of small doses of x rays on pores and skin reactions in the mouse and a fundamental interpretation. Dose fractionation, dose fee and isoeffect relationships for regular tissue responses. The utility of the linear-quadratic dose-effect equation to fractionated and protracted radiotherapy. The integrated logistic formula and prediction of issues from radiosurgery. A easy technique for outlining goal volumes on orthogonal simulation movies utilizing magnetic resonance pictures. The NeuroStation: a extremely accurate, minimally invasive resolution to frameless stereotactic neurosurgery. Clinical implementation of a Monte Carlo treatment planning system for radiotherapy. Phase I trial of gross whole resection, everlasting iodine-125 brachytherapy, and hyperfractionated radiotherapy for newly diagnosed glioblastoma multiforme. Interstitial irradiation of brain tumors, using a miniature radiosurgery device: preliminary expertise. Phase I research of intraoperative radiotherapy with Photon Radiosurgery System in kids with recurrent mind tumors: preliminary report of first dose degree (10 Gy). Stereotactic radiosurgery of the mind using the primary United States 201, cobalt-60 supply gamma knife. Use of hybrid pictures in planning Perfexion Gamma Knife therapies for lesions close to important structures. Heavy charged-particle Bragg peak radiosurgery for intracranial vascular issues. Stereotactic radiosurgery with the Cobalt-60 gamma unit in the surgical management of intracranial tumors and arteriovenous malformations. Radiosurgery as a part of the preliminary management of patients with malignant gliomas. Stereotactic percutaneous single dose irradiation of brain metastases with a linear accelerator. Radiosurgery for solitary mind metastases utilizing the cobalt-60 gamma unit: methods 261 2143. A multiinstitutional expertise with stereotactic radiosurgery for solitary brain metastasis. A Non-invasive, relocatable stereotactic body for fractionated radiotherapy and a quantity of imaging. Adaptation and verification of the relocatable Gill-Thomas-Cosman body in stereotactic radiotherapy. Initial clinical experience with frameless stereotactic radiosurgery: analysis of accuracy and feasibility. Frame-less mask-less bite-block-less stereotactic radiosurgery remedy with real-time surface imaging: a phantom and volunteer research. Volumetric modulated arc therapy: a review of present literature and clinical use in practice.
Cheap 120mg starlix with mastercard
A combination of views stages of hiv infection medscape 120 mg starlix overnight delivery, in our opinion anti viral bronchitis starlix 120mg cheap online, presents one of the best approach to the complex issues of sufferers with brachial plexus injuries. Some patients could benefit from medicines and time, in addition to neural interventions carried out at major procedures. Tendon switch choices about the shoulder in patients with brachial plexus injury. Muscle transpositions within the shoulder and upper arm for sequelae of brachial plexus palsy. Pulley for strengthening a muscle replacement operation throughout two joints in brachial plexus lesion: description of the surgical approach. Surgical reconstruction of the paralytic shoulder by multiple muscle transplantations. Stability of reconstructed paralyzed shoulders utilizing a mirrored long head biceps method. Modified latissimus dorsi and teres main switch for exterior rotation deficit of the shoulder. Functional reconstruction of the irreparable higher trunk defect of the brachial plexus-a case report. Trapezius switch to restore exterior rotation in a affected person with a brachial plexus damage. Upper and decrease trapezius muscle switch to restore shoulder abduction and exterior rotation in longstanding upper sort palsies of the brachial plexus in adults. Lower trapezius transfer for shoulder exterior rotation in patients with paralytic shoulder. Contralateral decrease trapezius switch for restoration of shoulder exterior rotation in traumatic brachial plexus palsy: a preliminary report and literature evaluation. Results of the latissimus dorsi and teres main tendon transfer on to the rotator cuff for brachial plexus palsy at delivery. Closed discount and tendon switch for therapy of dislocation of the glenohumeral joint secondary to brachial plexus delivery palsy. Palliative treatment of a collection of 103 instances of paralysis from elongation of the brachial plexus. Surgical method and anatomic examine of latissimus dorsi and teres main transfers. Triceps to biceps switch to restore elbow flexion in three sufferers with brachial plexus palsy. Reconstruction of elbow flexion by transposition of pedicled lengthy head of triceps brachii muscle. Pectoral transplantation for paralysis of the flexors of the elbow; a new approach. Surgical technique of pedicled bipolar pectoralis major transfer for reconstruction of elbow flexion in brachial plexus palsy. Latissimus dorsi transplantation for loss of flexion or extension on the elbow; a preliminary report on technic. Lower trapezius muscle switch for reconstruction of elbow extension in brachial plexus injuries. Brachialis muscle transfer to reconstruct finger flexion or wrist extension in brachial plexus palsy. Tendon transfers for remedy of the paralyzed hand following brachial plexus damage. Report of 14 transfers for radial nerve palsies and ten transfers for brachial plexus lesions. Reconstruction of elbow flexion, wrist and finger extension by transposition of pedicled latissimus dorsi muscle and flexor carpi ulnaris muscle. Surgical remedy of brachial plexus posterior twine lesion: a mix of nerve and tendon transfers, about 9 sufferers. Transfer of the supinator muscle to the extensor pollicis brevis for thumb extension reconstruction in C7-T1 brachial plexus palsy. Restoration of prehension with the double free muscle method following full avulsion of the brachial plexus. Reconstruction of finger and elbow operate after complete avulsion of the brachial plexus. Free muscle transplantation mixed with intercostal nerve crossing for reconstruction of elbow flexion and wrist extension in brachial plexus accidents. Transfer of one fascicle of ulnar nerve to functioning free gracilis muscle transplantation for elbow flexion. Ultrasonographic analysis of functioning free muscle switch: comparison between spinal accessory and intercostal nerve reinnervation. Double muscle transfer for higher extremity reconstruction following full avulsion of the brachial plexus. Double free-muscle switch to restore prehension following complete brachial plexus avulsion. Significance of elbow extension in reconstruction of prehension with reinnervated free-muscle switch following complete brachial plexus avulsion. Significance of shoulder function in the reconstruction of prehension with double free-muscle switch after complete paralysis of the brachial plexus. A one-stage shoulder arthrodesis and Brooks Seddon pectoralis major to biceps tendon transfer for upper brachial plexus accidents. Combined glenohumeral arthrodesis and above-elbow amputation for the flail limb following a complete posttraumatic brachial plexus damage. Wrist arthrodesis after double free-muscle switch in traumatic total brachial plexus palsy. Tenodesis of extensor digitorum in treatment of brachial plexus accidents involving C5, 6, 7 and eight nerve roots. Osteotomy of the humerus to improve external rotation in nine patients with brachial plexus palsy. Muscle preservation using an implantable electrical system after nerve harm and restore. Pain relief from preganglionic injury to the brachial plexus by late intercostal nerve switch. Long term follow-up outcomes of dorsal root entry zone lesions for intractable ache after brachial plexus avulsion accidents. Percutaneous T2 and T3 radiofrequency sympathectomy for complicated regional ache syndrome secondary to brachial plexus harm: a case collection. High cervical spinal wire stimulation after failed dorsal root entry zone surgery for brachial plexus avulsion pain. Cervical spinal twine stimulation for the administration of ache from brachial plexus avulsion. In a evaluation of lower extremity nerve injuries in Wroclaw, Poland,1 the incidence of accidents to nerves of the decrease extremity was 20% that of such injuries in the higher extremity. Irrespective of collection, the peroneal nerve was the decrease extremity nerve most commonly injured. The mechanisms of nerve harm, stretch, contusion, laceration, and compression could additionally be in play within the lower extremity, collectively or in isolation.

Generic starlix 120mg with mastercard
An evaluation of the intra-osseous arterial anastomoses in the human vertebral body at completely different ages hiv infection swollen lymph nodes buy starlix 120mg low price. Anatomic basis for the pathogenesis and radiologic options of vertebral osteomyelitis and its differentiation from childhood discitis hiv virus infection process video starlix 120 mg cheap on-line. The vascular anatomy of the spine and its relationship to pyogenic vertebral osteomyelitis. Spontaneous pyogenic vertebral osteomyelitis and endocarditis: incidence, danger elements, and outcome. The scientific presentation and influence of diagnostic delays on emergency department sufferers with spinal epidural abscess. Tuberculous spondylitis and pyogenic spondylitis: comparative magnetic resonance imaging options. Pyogenic, tuberculous, and brucellar vertebral osteomyelitis: a descriptive and comparative research of 219 instances. Spinal epidural abscess: expertise with forty six sufferers and evaluation of prognostic factors. Vertebral osteomyelitis in Goteborg, Sweden: a retrospective examine of patients during 199095. Surgical website infection in spinal surgical procedure: detection and management based on serial C-reactive protein measurements. The medical use of erythrocyte sedimentation price in pyogenic vertebral osteomyelitis. Spinal epidural abscess efficiently treated with percutaneous, computed tomography-guided, needle aspiration and parenteral antibiotic remedy: case report and evaluate of the literature. Septic hematogenous lumbar spondylodiscitis in aged patients with multiple threat components: efficacy of posterior stabilization and interbody fusion with iliac crest bone graft. Pyogenic spondylitis within the elderly: a report from Japan with probably the most aging society. Outcome of medical treatment of bacterial abscesses without therapeutic drainage: evaluation of instances reported in the literature. Surgical treatment of pyogenic vertebral osteomyelitis with spinal instrumentation. Spinal epidural abscesses: conservative remedy for selected subgroups of patients. Decreased morbidity from acute bacterial spinal epidural abscesses using computed tomography and nonsurgical remedy in chosen patients. Anterior radical debridement and anterior instrumentation in tuberculosis spondylitis. One-stage anterior interbody autografting and instrumentation in primary surgical management of thoracolumbar spinal tuberculosis. The use of allograft or autograft and expandable titanium cages for the treatment of vertebral osteomyelitis. Evaluation of the danger of instrumentation as a overseas physique in spinal tuberculosis. Anterior debridement and fusion followed by posterior pedicle screw fixation in pyogenic spondylodiscitis: autologous iliac bone strut versus cage. Treatment of pyogenic vertebral osteomyelitis with anterior debridement and fusion adopted by delayed posterior spinal fusion. Surgical remedy of vertebral osteomyelitis with recombinant human bone morphogenetic protein-2. The position of thoracoscopic spinal surgery in the management of pyogenic vertebral osteomyelitis. Long-term outcomes of ventro-dorsal versus ventral instrumentation fusion within the treatment of spondylitis. Percutaneous transpedicular automated nucleotomy for debridement of infected discs. Percutaneous drainage and steady irrigation in patients with severe pyogenic spondylitis, abscess formation, and marked bone destruction. Extended cervicolumbar spinal epidural abscess related to paraparesis successfully decompressed using a minimally invasive method. Anterior surgery with insertion of titanium mesh cage and posterior instrumented fusion carried out sequentially on the identical day under one anesthesia for septic spondylitis of thoracolumbar spine: is the use of titanium mesh cages secure The medical traits, therapeutic consequence, and prognostic elements of non-tuberculous bacterial spinal epidural abscess in adults: a hospital-based research. Spontaneous epidural abscess: analysis of 15 cases with emphasis on diagnostic and prognostic components. Treatment methods and end result in sufferers with non-tuberculous spinal epidural abscess: a evaluation of 46 circumstances. Axial pain localized to the positioning of the infection will finally turn into severe and may be related to paraspinous muscular spasm and tenderness to palpation of the affected vertebral segments. Fever, a key signal in combination with severe again ache, is reported in lower than 50%, and neurological impairment is much less widespread, with reviews going from 28% to 35%. Blood cultures, in the setting of fever and sepsis, may be useful in diagnosing the causative organism. Unfortunately, with out baseline radiographs the modifications can simply be interpreted as representing nonspecific degenerative changes. Standing long-cassette photographs can be utilized to monitor deformity development and are helpful in surgical planning. Computed tomography is in the end more sensitive than plain radiography with regard to bony modifications and extraspinal collections, but it provides restricted detail of the pathologic process throughout the spinal canal. Radionuclide studies are extra delicate than radiographs in figuring out areas of inflammation but present little anatomic detail, in addition to demonstrating a low positive predictive worth in circumstances of malignancy or degenerative changes. In some cases, nonetheless, because of the indolent nature of some pathogens, cultures could yield negative findings, even within the setting of overt illness on imaging and clinical evaluation. In some situations, therapy could be initiated without biopsy, notably within the setting of sepsis. Failure to respond to treatment, however, ought to prompt the clinician to contemplate biopsy to guide additional therapy. Despite this, tubercular osteomyelitis and other nonpyogenic infections of the backbone remain a related drawback in sure regions of the world and are discussed intimately in Chapter 291. Patients with compromised immune techniques are incessantly subjected to invasive procedures that lead to bacteremia and subsequent infection of the backbone. Each spinal segmental artery offers vascularization for all of the tissues that represent that vertebral segment. The disk is located on the heart of the spinal segment, which is why an infection often involves the intervertebral disk and the adjacent finish plates. Once bacteria seed the subchondral bone adjoining to the vertebral finish plate, the micro organism can directly invade the disk, inflicting what normally is the primary seen radiologic sign of infection: discitis. Untreated discitis, can evolve to spondylodiscitis, affecting the adjacent vertebral our bodies with related bony destruction, abscess formation, or each.
120 mg starlix cheap visa
These patients extra generally have multiple fusiform neurofibromas rather than plexiform neurofibromas hiv infection quiz trusted 120 mg starlix. Prior biopsy or attempted elimination is associated with the next incidence of serious ache or neurological deficit antiviral kleenex starlix 120 mg buy on line. There is an admixture of cells and peripheral nerve parts, together with fibroblasts, Schwann cells, perineural cells, mast cells, endothelial cells, and heaps of axons, compared with a schwannoma. Nerve fibers, highlighted by immunohistochemical staining for neurofilaments, arborize all through the tumor mass, helping differentiate a neurofibroma from a schwannoma. The needed steps in the removal of a fusiform solitary neurofibroma are much like those for a schwannoma. The capsule is left intact, with dissection on the floor gently separating off the stretched fascicles. A large neurofibroma can generally, on dissection, reveal itself to be a number of smaller neurofibromas adherent to one another. Dissection separates out the varied tumors and entering and exiting fascicles that need to be sacrificed. Surgical choice making could require one to consider leaving some tumor behind somewhat than sacrificing perform. As with the large schwannoma, an alternative method is to first open and evacuate the tumor contents and then dissect away the fascicles. Plexiform tumors may be particularly tough to take away with out inflicting a major deficit. Consideration could be being given to early resection of plexiform tumors while still small, thus avoiding the danger for malignant development and minimizing the danger of surgery. Indications for surgical procedure embrace want for tissue diagnosis, severe ache, progressive neurological deficit, and compromise of surrounding constructions. SurgicalApproach the sequence of surgical steps used to take away a neurofibroma is similar to that of a schwannoma. Microsurgical approach is used to isolate the proximal and distal poles of the tumor. Unlike a schwannoma, there can be more than one getting into and exiting fascicle that wants to be sacrificed with the tumor. This will necessarily increase the chance for neurological deficit with tumor elimination. The slide displays a myxomatous matrix with collagen fibrils and distinguished mucopolysaccharide staining. Desmoid Tumors these tumors are benign however are inclined to invade soft tissue, making their surgical resection problematic. The commonest location is the dorsum of the hand due to synovial fluid escaping from the wrist joint. In this location, the suprascapular nerve is usually compromised by the presence of the cyst. Intraoperative photograph exhibiting the publicity of a desmoid tumor (arrow) of the right anterior cervical area. An intraneural cyst can happen when fluid from the joint tracks alongside an articular nerve department. The fluid then expands both the articular department and the extra proximal mother or father nerve. Simply draining the fluid from the father or mother nerve will result in a excessive recurrence price. Also, well-documented instances have been revealed showing involvement of the median, sciatic, and recurrent laryngeal nerves. Treatment entails a wide surgical publicity to decide normal anatomy distal and proximal to the lesion earlier than skeletonizing the involved nerve and transferring it away from the lesion. Surgical excision may be challenging as a outcome of the tumors are sometimes not encapsulated and have a tendency to insinuate by way of tissue planes. These tumors can happen in the supraclavicular area and compromise the brachial plexus. On histologic sections, tumor cells are large and polyhedral with plentiful cytoplasm containing eosinophilic granules consultant of lysosomes. Other places that may produce neural compromise embody naturally occurring tunnels via which nerves journey. These embrace the carpal tunnel, cubital tunnel, tarsal tunnel, and fibular head area. Another common area for lipoma development is the radial tunnel, leading to a radial nerve or posterior interosseous nerve syndrome. Lower Extremity Nerve Location Femoral Obturator Sciatic Peroneal Posterior tibial Sciatic complex Sciatic No. A collection of 146 peripheral non-neural sheath tumors: 30-year experience at Louisiana State University Health Sciences Center. Often, an area decompression such as a carpal tunnel release is enough to relieve the neural signs without an attempt at removing the tumor and resulting neurological deficit. Spinal meningiomas with concurrent extradural localization and en plaque progress are exceptional, with lower than 10 circumstances in the literature. Involvement of the lower cervical roots with extension into the brachial plexus has been reported. Complete surgical excision is usually unrealistic resulting in a high recurrence price. Macrodystrophia (overgrowth of the hand and fingers) can occur secondary to a lipoma. The extra widespread kind, known as perineurioma, consists of intraneural tumor formed from perineurial cells with onion bulb formation. In our personal follow, if the lesion is clearly very focal and really distal in a motor nerve, one can think about resection and grafting. The latter presentation could be problematic for a good end result from resection and nerve grafting. Radiation-Induced Brachial Plexus Lesions (Actinic Plexitis) Radiation causes direct cellular damage, microvascular ischemic harm, and extrinsic constriction of nerve bundles by surrounding fibrotic tissues. The median interval earlier than onset is 1 to four years, but a latent interval of up to 30 years has been reported. The therapy targets of radiation-induced plexopathy include management of pain and restoration in motor perform. Neuropathic ache may reply to medical therapy, whereas transcutaneous electrical nerve stimulation and dorsal root entry zone lesions could be considered for intractable instances of persistent pain. Success charges differ in the literature, and although some have noted improvement in motor function and ache, others have reported deterioration because of such surgery. Axial magnetic resonance image showing a well-demarcated, enhancing meningioma in the proper brachial plexus. Intraoperative photograph displaying fusiform swelling of the nerve representing localized hypertrophic neuropathy. Similar look of fusiform swelling or onion whorl may also be seen in Charcot-Marie-Tooth disease and in Dejerine-Sottas disease.