
Quibron-t dosages: 400 mg
Quibron-t packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Order 400 mg quibron-t with mastercard
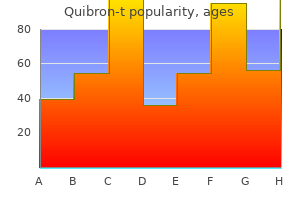
Changes in skin bacteriome and mycobiome correlated with illness in psoriasis patients: A pilot research allergy medicine used in meth cheap quibron-t 400 mg with visa. Yeast metabolic merchandise allergy symptoms sneezing runny nose quibron-t 400 mg purchase overnight delivery, yeast antigens and yeasts as attainable triggers for irritable bowel syndrome. Standaert-Vitse A, Sendid B, Joossens M, Francois N, Vandewalle-El Khoury P, Branche J et al. Jawhara S, Thuru X, Standaert-Vitse A, Jouault T, Mordon S, Sendid B, Desreumaux P, Poulain D. Colonization of mice by Candida albicans is promoted by chemically induced colitis and augments inflammatory responses by way of galectin-3. Interactions between commensal fungi and the C-Type lectin receptor dectin-1 affect colitis. Joossens M, Huys G, Cnockaert M, De Preter V, Verbeke K, Rutgeerts P, Vandamme P, Vermeire S. Correlation between gastrointestinal fungi and ranging degrees of chronic hepatitis B virus infection. Mutation of gene of mannose-binding protein related to continual hepatitis B viral infection. Mid-esophageal ulceration and candidiasis-associated distal esophagitis as two distinct scientific patterns of tetracycline or doxycycline-induced esophageal injury. Antimicrobial agent, tetracycline, enhanced higher alimentary tract Candida albicans an infection and its associated mucosal proliferation in alloxan-induced diabetic rats. Gastrointestinal colonization by Candida albicans mutant strains in antibiotic-treated mice. Sustained gastrointestinal colonization and systemic dissemination by Candida albicans, Candida tropicalis and Candida parapsilosis in grownup mice. Gastrointestinal candidiasis in rats handled with antibiotics, cortisone, and azathioprine. Influence of antibiotics or sure intestinal micro organism on orally administered Candida albicans in germ-free and traditional mice. The relation between oral Candida load and bacterial microbiome profiles in Dutch older adults. Navazesh M, Mulligan R, Pogoda J, Greenspan D, Alves M, Phelan J, Greenspan J, Slots J. Enterococcus faecalis inhibits hyphal morphogenesis and virulence of Candida albicans. Using high throughput sequencing to explore the biodiversity in oral bacterial communities. Oral candidiasis: Pathogenesis, scientific presentation, diagnosis and remedy strategies. Detection of enormous numbers of pneumococcal virulence genes in streptococci of the mitis group. Yokoyama T, Sasaki J, Matsumoto K, Koga C, Ito Y, Kaku Y, Tajiri M, Natori H, Hirokawa M. A necrotic lung ball caused by co-infection with Candida and Streptococcus pneumoniae. Biosynthesis of teichoic acids in Streptococcus pneumoniae and closely associated species. Fungi of the murine intestine: Episodic variation and proliferation during antibiotic therapy. Jawhara S, Habib K, Maggiotto F, Pignede G, Vandekerckove P, Maes E, Dubuquoy L, Fontaine T, Guerardel Y, Poulain D. Modulation of intestinal inflammation by yeasts and cell wall extracts: Strain dependence and unexpected antiinflammatory position of glucan fractions. Saccharomyces boulardii decreases inflammation and intestinal colonization by Candida albicans in a mouse model of chemically-induced colitis. Saccharomyces boulardii and Candida albicans experimental colonization of the murine gut. Prophylactic Saccharomyces boulardii versus nystatin for the prevention of fungal colonization and invasive fungal infection in untimely infants. Index Note: Page numbers in italic and daring discuss with figures and tables respectively. Beck and colleagues embody behavioural components of their treatment however mainly emphasize the cognitive aspects of depression, in two key respects. Firstly, cognition is given a causal standing by conferring a vulnerability to depression in some individuals. This cognitive vulnerability, or susceptibility, is purported to have its roots in early childhood experiences and their impression on the unique cognitive organization and beliefs a person develops. A assortment of beliefs, assumptions, attitudes or guidelines around a particular theme is recognized as a schema (Beck, 2011; James, Reichelt, Freeston & Barton, 2007). Schemata represent the particular means a person constructs and views themselves, different folks and the world. People with opposed early experiences can develop unhelpful core beliefs that form into maladaptive schema. Case Illustration Angela: cognitive vulnerability Like all case illustrations on this e-book, Angela is an actual consumer who has consented for details of her remedy to be included. She was referred for remedy with a 4-year history of melancholy and extreme fear following relationship issues together with her husband. Assessment revealed a key part of her early experience was being part of a large household, often feeling missed and neglected by her dad and mom. Angela compensated her schema by being submissive and acquiescent in key relationships. Once an individual is in a depressed state their propensity for negative thinking continues and adverse ideas turn into more plausible (Barber & DeRubeis, 1989). This was deeply upsetting for Angela and provoked thoughts and images of herself as ugly and unattractive. Sometime later she found her husband had been having affairs and this activated her core perception of being worthless. She felt too weak to challenge him and as a substitute hid what he had accomplished and tried to regain his approval. Thoughts that she was ugly and nugatory triggered emotions of disgrace, harm and anxiety and these maintained her submissive behaviours. The datapoints symbolize scores on the Beck Depression Inventory (Beck, Steer & Garbin, 1988) completed by Angela at each remedy session. These show a gradual decrease from reasonable melancholy to remission, achieved throughout 4 months of acute section treatment. In the principle body of treatment, the primary batch of periods usually have a strong behavioural emphasis, then the major target shifts towards unfavorable automated thinking, then onto underlying beliefs, assumptions and guidelines for dwelling. The acute phase classes are adopted by continuation booster classes to shield the client from relapse and, ideally, a follow-up session around a 12 months after the end of treatment.
Order quibron-t 400 mg fast delivery
This kind of angina happens at rest allergy symptoms ear ache quibron-t 400 mg buy, rather than on exertion allergy shots build up phase quibron-t 400 mg online buy cheap, without any initiating factors. Vasospastic angina is a wide range of angina pectoris (chest pain) occurring at relaxation, rather than on exertion. In this angina type, myocardial ischemia is as a result of of transient vasospasm with or with none underlying pathology. Epidemiology of Vasospastic Angina Vasospastic angina is an uncommon cause of myocardial ischemia, liable for roughly 5 % of angina instances. Patients are generally younger than those with steady or unstable angina secondary to coronary artery atherosclerosis. It is believed that this decline is as a outcome of of increased use of calcium antagonists to deal with hypertension. Etiology of Vasospastic Angina Causes of vasospastic angina Coronary artery spasm can happen on account of various danger elements corresponding to stress, smoking, cocaine use, insulin resistance, and drugs which have the impact of constricting blood vessels, corresponding to triptans. Rarely, coronary artery vasospasm may be triggered after coronary artery bypass surgery or near a drug-eluting stent. Pathophysiology of Vasospastic Angina the underlying mechanism inflicting vasospasm in vasospastic angina is debatable, and lots of theories have been put forward lately. Vasospasm occurs in response to local vasoconstrictor stimuli in the coronary phase. Impaired regulation of myofibril contraction in easy muscle cells of coronary vessels causes smooth muscle hyperactivity, resulting in vasospasm. Other abnormalities of the endothelium similar to defect within the enzyme endothelial nitric oxide synthase can lead to decreased ranges of nitric oxide. Nitric oxide is a pure vasodilator, and its decreased synthesis can lead to vasoconstriction. Sudden vasoconstriction ensuing from any of the aforementioned phenomena results in decreased coronary blood flow which causes myocardial hypoxia which triggers angina. In vasospastic angina, focal coronary artery spasm occurs and considerably reduces the diameter of the coronary artery lumen, causing short-term occlusion and leading to myocardial ischemia. This vasospasm can happen in normal-appearing arteries in addition to arteries affected by atherosclerosis. The commonest artery affected is the best coronary artery; the second mostly affected is the left anterior descending artery. Some proposed theories relate to endothelial dysfunction and elevated contractility of vascular clean muscle. Another principle is that repeated episodes of coronary vasospasm might cause neointimal hyperplasia, contributing to stenosis in the artery. Rho-kinase is also believed to play a role within the pathogenesis of this situation, involved in regulating vascular easy muscle contractility. Other elements which have been suggested as contributory to the pathogenesis of coronary artery spasm embrace autonomic nervous system dysfunction, magnesium deficiency, chronic low-grade inflammation, and elevated oxidative stress (with smoking). Some patients may expertise these assaults during or after exercise, including those who have co-existing fastened coronary artery stenosis. Patients usually experience assaults of angina in clusters, from midnight to early morning (midnight � eight:00 am). Patients with variant coronary syndrome may also expertise asymptomatic ischemic episodes. If coronary artery spasm causes a protracted disturbance in coronary blood circulate, it could trigger a myocardial infarction Syncope may also happen if there are disturbances to the center rhythm similar to asystole, atrioventricular block, or ventricular tachyarrhythmias. In addition, arrhythmias could additionally be detectable during an episode of variant angina, corresponding to ventricular tachycardia, atrioventricular block, and bradyarrhythmia. Coronary angiography Coronary angiography is considered the gold standard in the analysis of variant angina. There is usually an absence of organically stenosed arteries detected on an angiography; however, there are some sufferers who do have coronary artery stenosis co-existing with coronary artery spasm. Provocation testing can be used for the definitive analysis of coronary variant syndrome. Coronary vasospasm can be provoked throughout angiography by injecting acetylcholine and ergonovine into the coronary arteries. Sudden cardiac arrest, with or with out syncope, can occur because of ischemia-induced ventricular fibrillation. Atherosclerosis can even happen afterward at the website of vasospasm, resulting in local coronary thrombosis. Medical remedy � � A nitrate can be administered to relieve an attack of angina in an acute setting. The major drug used to treat variant coronary syndrome is a calcium channel blocker, corresponding to diltiazem. They could additionally be given alone or along with isosorbide mononitrate, a long-acting nitrate. Note: Beta-blockers are contraindicated as they reduce the dilatation of the graceful musculature by way of blocking the beta-2 receptors and increase the tone of the coronary vessels. New medication � � Nicorandil is a K+-channel agonist that can be added in recurrent cases. Fasudil is a novel drug which inhibits rho-kinase, stopping acetylcholineinduced vasospasm. Surgery � Complete cardiac denervation with plexectomy, with or without coronary artery bypass surgery, is an choice for resistant cases; nonetheless, procedural risks are excessive and results have been inconsistent. Prognosis of Vasospastic Angina If the situation is controlled from an early stage, the prognosis could be favorable. Complications, similar to acute myocardial infarction, coronary artery bypass grafting, and cardiac demise usually occur early on after the onset of angina. His chest ache happens after climbing greater than 2 flight of stairs or walking for greater than 10 minutes and resolves with rest. He is obese, has a history of type 2 diabetes and has smoked 15 to 20 cigarettes a day for the previous 25 years. Which of the following greatest represent the more than likely etiology of this affected person situation Sudden disruption of an atheromatous plaque, with a resulting occlusive thrombus D. His chest pain happens after climbing more than 2 flights of stairs or walking for more than 10 minutes and resolves with relaxation. Arthritides, endocarditis, the consumption of cocaine, emboli caused by heart valve prostheses, or other paradoxical embolisms are of less significance for etiology. In perfusion of less than 25 % of the traditional move, the tissue is irreversibly broken. After 6�12 hours, this damage could be seen by light microscope in the form of yellowish spots. After a number of days, granulation tissue forms, containing a hemorrhagic edge and many marginal leukocytes. Tme 0�24 hours Occluded artery Infarct Gross Light microscope Early coagulative necrosis, launch of necrotic cell contents in blood; edema, hemorrhage, wavy fibers.
Quibron-t 400 mg discount fast delivery
Despite these advantages allergy medicine doesn't work quibron-t 400 mg discount online, AmBd might proceed to play a job in select makes use of and patient populations allergy forecast hutto tx quibron-t 400 mg quality, similar to neonates and kids, intrathecal use in patients References a hundred sixty five 13. Amphotericin B formulations exert additive antifungal activity in combination with pulmonary alveolar macrophages and polymorphonuclear leukocytes against Aspergillus fumigatus. In vitro pharmacodynamics of rapid versus continuous infusion of amphotericin B deoxycholate against Candida species in the presence of human serum albumin. Pharmacodynamic activity of amphotericin B deoxycholate is related to peak plasma concentrations in a neutropenic murine mannequin of invasive pulmonary aspergillosis. Activities of antifungal brokers against yeasts and filamentous fungi: Assessment according to the methodology of the European Committee on Antimicrobial Susceptibility Testing. Infusion-related toxicity of three completely different amphotericin B formulations and its relation to cytokine plasma levels. Liposomal amphotericin B and amphotericin B-deoxycholate present totally different immunoregulatory effects on human peripheral blood mononuclear cells. Induction of prostaglandin synthesis because the mechanism responsible for the chills and fever produced by infusing amphotericin B. Pharmacodynamics of amphotericin B in a neutropenic-mouse disseminated-candidiasis mannequin. Postantifungal effects of echinocandin, azole, and polyene antifungal agents in opposition to Candida albicans and Cryptococcus neoformans. Absence of amphotericin B-Tolerant persister cells in biofilms of some Candida species. Antifungal susceptibility of Candida biofilms: Unique efficacy of amphotericin B lipid formulations and echinocandins. Comparison of the antifungal activity of micafungin and amphotericin B towards Candida tropicalis biofilms. Clinical follow: Combination antifungal therapy for mold infections: Much ado about nothing Combination antifungal remedy for the treatment of invasive yeast and mildew infections. Activity of mixed antifungal agents against multidrug-resistant 166 Polyenes for prevention and therapy of invasive fungal infections 38. The combination of amphotericin B and azithromycin as a potential new therapeutic approach to fusariosis. Potentiation of antifungal exercise of amphotericin B by azithromycin against Aspergillus species. Antifungal activities of tacrolimus in combination with antifungal agents towards fluconazole-susceptible and fluconazole-resistant Trichosporon asahii isolates. Rifampin enhances the activity of amphotericin B in opposition to Fusarium solani species advanced and Aspergillus flavus species complex isolates from Keratitis sufferers. Role of cell protection in opposition to oxidative damage within the resistance of Candida albicans to the killing effect of amphotericin-B. Pharmacodynamics of fluconazole, itraconazole, and amphotericin B towards Candida albicans. Liposomal amphotericin B (AmBisome()): A evaluate of the pharmacokinetics, pharmacodynamics, medical expertise and future directions. Comparative evaluation of amphotericin B lipid complicated and liposomal amphotericin B kinetics of lung accumulation and fungal clearance in a murine model of acute invasive pulmonary aspergillosis. Pharmacokinetics, excretion, and mass steadiness of 14C after administration of 14C-cholesterol-labeled AmBisome to healthy volunteers. Plasma protein binding of amphotericin B and pharmacokinetics of sure versus unbound amphotericin B after administration of intravenous liposomal amphotericin B (AmBisome) and amphotericin B deoxycholate. Pharmacokinetics, excretion, and mass balance of liposomal amphotericin B (AmBisome) and amphotericin B deoxycholate in humans. Evaluation of amphotericin B interpretive breakpoints for Candida bloodstream isolates by correlation with therapeutic consequence. Population pharmacokinetics of liposomal amphotericin B in pediatric sufferers with malignant ailments. Increased antifungal drug resistance in clinical isolates of Cryptococcus neoformans in Uganda. Interactions between triazoles and amphotericin B against Cryptococcus neoformans. Large-scale evaluation of in vitro amphotericin B, triazole, and echinocandin activity in opposition to Coccidioides species from U. Sporothrix schenckii sensitivity to voriconazole, itraconazole and amphotericin B. Activities of caspofungin, itraconazole, posaconazole, ravuconazole, voriconazole, and amphotericin B in opposition to 448 latest medical isolates of filamentous fungi. In vitro amphotericin B resistance in medical isolates of Aspergillus terreus, with a head-to-head comparison to voriconazole. Concentrations of amphotericin B in faeces and blood of wholesome volunteers after the oral administration of various doses. Effects of decontamination of the digestive tract and oropharynx in intensive care unit patients on 1-year survival. Randomized scientific trial of perioperative selective decontamination of the digestive tract versus placebo in elective gastrointestinal surgery. Comparison of amphotericinB and N-D-ornithyl amphotericin B methyl ester in experimental cryptococcal meningitis and Candida albicans endocarditis with pyelonephritis. Comparative efficacy and distribution of lipid formulations of amphotericin B in experimental Candida albicans an infection of the central nervous system. Compartmentalized intrapulmonary pharmacokinetics of amphotericin B and its lipid formulations. Pharmacokinetics of amphotericin B lipid complex in critically unwell sufferers on steady veno-venous haemofiltration. Population pharmacokinetics of liposomal amphotericin B and caspofungin in allogeneic hematopoietic stem cell recipients. Population pharmacokinetics of amphotericin B in youngsters with malignant ailments. Amphotericin B in kids with malignant disease: A comparability of the toxicities and pharmacokinetics of amphotericin B administered in dextrose versus lipid emulsion. Safety, tolerability and pharmacokinetics of liposomal amphotericin B in immunocompromised pediatric patients (abstract). Caspofungin versus liposomal amphotericin B for empirical antifungal remedy in sufferers with persistent fever and neutropenia. Hyperkalemia associated with speedy infusion of typical and lipid complex formulations of amphotericin B. A randomized, double-blind comparative trial evaluating the security of liposomal amphotericin B versus amphotericin B lipid advanced in the empirical remedy of febrile neutropenia. Severe hypertension related to using amphotericin B: An appraisal on the reported cases.
Generic quibron-t 400 mg free shipping
Candida lusitaniae: In vitro susceptibility and in vivo correlation in experimental murine candidiasis fifty three allergy treatment philippines order 400 mg quibron-t mastercard. Programs and Abstracts of the Conference on candida and Candidiasis: Biology allergy shots 3 year old 400 mg quibron-t order free shipping, Pathogenesis and Management (Baltimore). In vitro exercise of amphotericin B, flucytosine and fluconazole against yeasts inflicting bloodstream infections. Antifungal susceptibility testing of yeasts - evaluation of technical variables for check automation. In vitro susceptibilities of medical and environmental isolates of Cryptococcus neoformans to five antifungal medicine. Saccharomyces cevevisiae infections and antifungal susceptibility research by colorimetric and broth macrodilution methods. In vitro susceptibility of scientific isolates of Zygomycota to amphotericin B, flucytosine, itraconazole and voriconazole. In vitro susceptibilities of 217 scientific isolates of zygomycetes to standard and new antifungal brokers. In vitro determination of optimal antifungal combinations towards Cryptococcus neoformans and Candida albicans. In vitro interplay of flucytosine combined with amphotericin B or fluconazole against thirty-five yeast isolates decided by each the fractional inhibitory concentration index and the response surface method. Rates and extents of antifungal actions of amphotericin B, flucytosine, fluconazole, and voriconazole in opposition to Candida lusitaniae decided by microdilution, Etest, and time-kill methods. Combined exercise of amphotericin B and 5-fluorocytosine against Cryptococcus neoformans in vitro and in vivo in mice. Combination of amphotericin B with flucytosine is lively in vitro in opposition to flucytosine-resistant isolates of Cryptococcus neoformans. Efficacy of amphotericin B together with flucytosine in opposition to flucytosine-susceptible or flucytosine-resistant isolates of Cryptococcus neoformans throughout disseminated murine cryptococcosis. Combination remedy with fluconazole and flucytosine within the murine mannequin of cryptococcal meningitis. Effect of fluconazole on fungicidal activity of flucytosine in murine cryptococcal meningitis. Interactions among amphotericin B, 5-fluorocytosine, ketoconazole, and miconazole in opposition to pathogenic fungi in vitro. Susceptibility of Aspergillus to 5-fluorocytosine and amphotericin B alone and together. Oral versus intravenous flucytosine in patients with human immunodeficiency virus-associated cryptococcal meningitis. Intraperitoneal flucytosine within the management of fungal peritonitis in sufferers on continuous ambulatory peritoneal dialysis. Management of Candida peritonitis by extended peritoneal lavage containing 5-fluorocytosine. Serum and intraperitoneal levels of amphotericin B and flucytosine throughout intravenous treatment of critically sick sufferers with Candida peritonitis. Review of the literature apropos of a case with examine of bone penetration of 5-fluorocytosine. Septic arthritis because of nonencapsulated Cryptococcus neoformans with coexisting sarcoidosis. Diffusion of 5-fluorocytosine in bronchial secretions in patients with respiratory insufficiency. Study of serial bronchoalveolar lavage in sufferers with aspergilloma: Cell response on the affected websites and penetration of miconazole and flucytosine into the lesion. Direct detection of recent flucytosine metabolites in human biofluids by 19F nuclear magnetic resonance. Flucytosine conversion to fluorouracil in humans: Does a correlation with gut flora standing exist An in vitro research on the energetic conversion of flucytosine to fluorouracil by microorganisms in the human intestinal microflora. Identification of minor metabolites of 5-fluorocytosine in man by chemical ionization gasoline chromatography mass spectrometry. Pharmacokinetic research on the oral antimycotic agent 5-fluorocytosine in individuals with normal and impaired kidney operate. Flucytosine pharmacokinetics in a critically unwell affected person receiving continuous renal alternative therapy. Evidence of excessive concentrations of 5-flucytosine in kids aged under 12 years: A 12-year review 188 Flucytosine 122. Pharmacokinetics and pharmacodynamics of antifungals in youngsters and their scientific implications. Flucytosine dosing in an overweight affected person with extrameningeal cryptococcal an infection. Evolving position of flucytosine in immunocompromised sufferers: New insights into security, pharmacokinetics, and antifungal therapy. Toxicity of amphotericin B plus flucytosine in 194 sufferers with cryptococcal meningitis. Infections with Cryptococcus neoformans within the acquired immunodeficiency syndrome. Effect of 5-fluorocytosine and 5-fluorouracil on human and rat hepatic cytochrome P 450. Evaluation of hepatotoxicity with remedy doses of flucytosine and amphotericin B for invasive fungal infections. Disseminate sporotrichosis of pores and skin and bone cured with 5-fluorocytosine: Photosensitivity as a complication. Acute and persistent results of flucytosine on amphotericin B nephrotoxicity in rats. Falsely elevated serum creatinine levels secondary to the presence of 5-fluorocytosine. The evolution of pulmonary cryptococcosis: Clinical implications from a study of forty one sufferers with and with out compromising host factors. Flucytosine: Experience in sufferers with pulmonary and other types of cryptococcosis. Treatment of cryptococcal meningitis with combination itraconazole and flucytosine. Combination flucytosine and high-dose fluconazole in contrast with fluconazole monotherapy for the therapy of cryptococcal meningitis: A randomized trial in Malawi. Short-term topical remedy of vulvovaginal candidiasis with the mixture of 5-fluorocytosine and candicidin.
Quibron-t 400 mg cheap on line
In symptomatic sufferers allergy shots help asthma buy discount quibron-t 400 mg on-line, candiduria represents true an infection; due to this fact allergy shots exhaustion order quibron-t 400 mg line, therapy is recommended. Despite these uncertainties, patients with signs and signs of cystitis and with solely fungus present in tradition should be thought of as candidates for treatment [5]. Several antifungal brokers have been used for the remedy of Candida cystitis primarily fluconazole, amphotericin B bladder irrigation and flucytosine [50,51]. Fluconazole is a water-soluble triazole that has an oral bioavailability of greater than 90% and is excreted unchanged in the urine to a large diploma (80%), with urinary focus reaching 10 instances that of blood [52]. Published expertise with different azoles, similar to itraconazole and voriconazole, are restricted since these agents undergo a high degree of hepatic metabolism and achieve restricted concentrations in the urinary tract [52]. Lower doses and shorter courses are discouraged, as Candida cystitis ought to be treated as an advanced urinary tract infection requiring higher dose and longer duration therapy [54]. Continuous bladder irrigation with amphotericin B through an indwelling urinary catheter is an old modality of therapy of Candida cystitis first described in 1960 [55]. The eradication price of candiduria using this therapeutic method varied from 43% to one hundred pc relying on the study [56,57]. Two randomized trials have compared completely different concentrations of amphotericin B in bladder irrigation used for the therapy of funguria [48,58�60]. The first one in contrast concentrations of 5, a hundred, and 200 mg/L, every administered three times daily for 3 days [48]. Although, on day 1, the efficacy rates for elimination of funguria (80%�85% for all treatment groups) were considerably better for amphotericin B bladder irrigations than for placebo, by day 10, clearance rates for the three concentrations fell to forty two. Another randomized study evaluating concentrations of 10 mg/L and 50 mg/L administered by steady irrigation for 72 hours to 26 sufferers reported efficacy rates of 67% and 100%, respectively [58]. Descriptions of drug administration vary from intermittent instillation (up to 3 times daily with medicine dwell occasions of 2�3 hours) to continuous irrigation (usually via a 3-way Foley catheter) [57]. In spite of all these research, the optimal method of supply for amphotericin B bladder irrigation has not been established. A randomized, prospective study compared the efficacy on day 1 of therapy delivered as steady irrigation of 50 mg/L for forty eight hours with that of intermittent instillation of 10 mg/100 mL 3 times daily [59]. Eight out of ten sufferers within the continuous infusion group had clearance of fungus from the urine at seventy two hours, in contrast with three of the ten patients in the intermittent treatment group. Moreover, the optimal period of therapy of amphotericin B bladder irrigation is unknown. A single dose has shown restricted success for patients with out apparent upper tract illness [60] and will not be significantly completely different from drug supply for 7 days [47]. A 2-day routine has also been evaluated with efficacy rates of 75% reported in one research [61]. Despite the dearth of solid evidence for the use of amphotericin B bladder irrigation for the remedy of Candida cystitis, such treatment strategy remains to be beneficial by some authorities in clinical practice [62]. Finally, flucytosine has been successfully used in the remedy of urinary candidiasis with response rates of over 90% [64]. Its limitation contains bone marrow, hepatic and gastrointestinal toxicity, de novo resistance (25%) observed in C. Its use ought to only be restricted to circumstances of azole-resistant strains at a dose of 25 mg/kg four occasions every day given orally for 7�14 days [5]. Fungal bezoar formation is essentially the most critical complication of Candida pyelonephritis. Renal colic might occur with the passage of fungal stones, which are parts of fungus bezoars. Excretory urography or retrograde pyelography reveals a filling defect in the collecting system. Other problems of Candida pyelonephritis include papillary necrosis and native suppurative illnesses resulting in pyonephrosis and perinephric or intrarenal abscess formation. Upper urinary tract infections often require systemic antifungal remedy, in addition to immediate investigation and imaging of the urinary system to exclude obstruction, papillary necrosis, and fungus-ball formation. Amphotericin B bladder irrigation has no function within the remedy of patients with pyelonephritis. Systemic antifungal remedy with both parenteral amphotericin B deoxycholate at >0. Flucytosine is occasionally mixed with amphotericin B to cowl for resistant Candida spp. Adequate drainage of the urinary tract system by placement of a stent or nephrostomy tube, in addition to surgical removal of fungus balls is always important. Irrigation of nephrostomy tube with either amphotericin B or fluconazole is advisable in some cases to achieve excessive concentrations 494 Fungal infections of the genitourinary tract of the antifungal agent at the web site of an infection. One of the most important pharmacokinetic disadvantages of echinocandins is the poor glomerular filtration or tubular secretion leading to subtherapeutic antifungal focus within the urine. However, the echinocandins achieve a excessive tissue focus independent of glomerular filtration making them an acceptable alternative for the therapy of renal candidiasis caused by resistant non-albicans pressure in the absence of urinary tract obstruction [67,68]. Oral fluconazole is the preferred routine; however, in case of fluconazole-resistant Candida spp. It occurs often secondary to systemic infections in immunosuppressed sufferers and is difficult by prostatic abscess formation. Patients present with irritative voiding symptoms, perineal pain, fever, and acute urinary retention. Surgical drainage in case of abscess formation along with systemic antifungal therapy is recommended. It has been mainly reported in patients with malignancies, diabetes, intravenous drug use, continual alcoholism and in renal transplant recipients [82�86]. Three illness patterns of genitourinary aspergillosis have been described in the literature. The first and commonest sample outcomes from hematogenous spread of disseminated Aspergillus infection and is associated with multiorgan involvement together with kidney and prostate. The second pattern is the outcomes of a panurothelial ascending infection, involving the urethra, bladder, ureters, prostate, and kidneys and is secondary to iatrogenic bladder instrumentation [87,88]. The third sample consists of a localized parenchymal necrosis with an obstructing fungal bezoar formation that can be seen in any part of the urinary tract. Patients with genitourinary tract aspergillosis normally present with fever and microscopic hematuria. Urine culture is invariably negative making the diagnosis of urinary tract aspergillosis difficult in the absence of clinical suspicion. Repeated massive volume urine culture on Sabouraud dextrose medium or brain�heart enriched infusion broth has been advised. However, the yield is poor as a outcome of Aspergillus organisms have a tendency for tissue attachment and invasion. Tissue culture or pathological examination showing the fungal hyphae in renal tissue remains the standard diagnostic modality [89,90]. Management of urinary tract aspergillosis requires the mixture of medical and surgical interventions [91�96].
Quibron-t 400 mg buy cheap on line
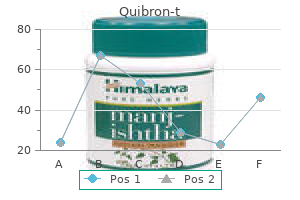
The purpose is to indirectly change the content material of pondering by influencing: (a) how ideas are processed within the mind allergy shots benadryl quibron-t 400 mg purchase with visa, similar to rumination and suppression; (b) larger consciousness of the consequences of these processes allergy medicine starts with c quibron-t 400 mg buy generic line. Restoring normal reflective, attentional and reminiscence processes is the best way of facilitating cognitive change. The key antecedents of motion are motivational states, somewhat than environmental triggers. The similar self-regulation mannequin is used with every of those varieties but treatment parameters and dynamic focus are considerably different. The purpose of this part is to orient therapists towards the primary clinical and contextual points that have a bearing on these sub-types, so that treatment could be adjusted accordingly. There are two causes for prioritizing early-onset despair, as explored in Chapter 7. Firstly, people who go on to develop extremely recurrent despair are prone to have their first-onset prior to the age of eighteen. Highly recurrent melancholy, by which we imply three or more major episodes, can be difficult to deal with. The purpose is, as talked about in Chapter 4, that maintenance processes turn into more autonomous when depression turns into highly recurrent. Depressed moods can be activated by relatively mild stress, and this brings particular difficulties for each consumer and therapist. These shoppers are also at excessive risk of relapse, so their priority status is evident. This is a single diagnostic class with a diverse range of medical presentations. We contemplate the varied therapeutic implications and remedy changes in Chapter 9. They must be excessive priority purchasers, due to the misery they expertise throughout such a formative interval of life, and likewise because untreated adolescent depression can contribute to recurrent difficulties later. At any point in time, between 4% and 5% of adolescents aged 13�18 years are affected by main melancholy, and younger ladies usually have a tendency to be affected than younger males (Thapar et al. Early-onset depression is related to by no means marrying, much less adaptive social and occupational functioning, poorer quality of life, higher medical and psychiatric comorbidity, a more negative view of self and life, more lifetime depressive episodes, extra suicide makes an attempt, and greater depression severity inside recurrent episodes (Jonsson et al. However, these are associations, not inevitabilities: if adolescent despair goes untreated the above sequelae are extra doubtless; whether it is efficiently handled and vulnerabilities are addressed, a extra adaptive developmental path can be forged. Hence the urgent must intervene as successfully and as early as attainable in the lifespan (Curry & Wells, 2005). Not surprisingly, due to this fact, adults with extremely recurrent melancholy are prone to have experienced their first-onset in adolescence (Lewinsohn, Rohde, Seeley, Klein & Gotlib, 2000). We have chosen to consider the remedy of challenging circumstances, to discover the aetiology and upkeep of early-onset depression, and ways of supporting the developmental tasks of adolescence. He was attending college intermittently, having angry outbursts, but not self-harming or abusing alcohol or drugs. He is a good instance of the challenges working with adolescent despair: a teenager in a downward spiral of psychological health, reluctant to receive assist, in a household whose conflicts are contributing to the maintenance of his difficulties. The largest trial included in this meta-analysis was the Treatment for Adolescents with Depression Study (March et al. There have been two additional trials of notice since the 2007 meta-analysis (Klein et al. All three remedies achieved approximately 50% discount in despair symptoms, one year after remedy, and there have been no variations between remedies. The health-economic argument for prioritizing adolescent melancholy, and treating it more effectively, is clear-cut: the long-term savings on all metrics are huge if young individuals are in a place to find a healthier path, not to point out the higher high quality of life for those people. First-Onsets throughout the Lifespan How, then, can we method adolescent depression with recent eyes The knowledge represented in this graph come from a large-scale research of depressed adults who have been interviewed to discover out once they first experienced a major episode (Zisook et al. Approximately 70% of first-onsets were precipitated by, or related to, major life stress. This decreased to approximately 40% in second episodes and roughly 30% in third episodes. Treatment of early-onset melancholy has to handle the influence of actual opposed occasions similar to trauma, abuse, neglect, tutorial stress, bullying, interpersonal conflict and ostracization: these are the widespread precipitants of adolescent melancholy. Depressed adolescents are prone to have suffered, or be suffering, the consequences of these types of experiences (Harkness, Bruce & Lumley, 2006; Lewinsohn, Allen, Seeley & Gotlib, 1999; Williamson, Birmaher, Frank, Anderson, Matty & Kupfer, 1998). Remember: from a self-regulation perspective, depressed moods are a traditional consequence of those experiences. Diathesis�Stress Interactions Pre-existing susceptibilities (diatheses) interact with stressors (adverse experiences) and their interplay triggers the onset of a depressive disorder (Lewinsohn, Joiner & Rohde, 2001). The relative contribution of stress, life occasions and adverse experiences is bigger in first-onsets, and these need to be a higher part of the formulation and treatment focus. The nature of the life stress and adversity the younger individual has skilled: is it minor or major, a single occasion or recurring, previous or present The quality and amount of household and social support: what has been provided and what has been received Case Illustration Daniel: diathesis�stress interactions within the precipitation of early-onset depression a. Life stress and adversity Daniel was the youthful of two brothers, whose dad and mom separated when he was very young. He was an emotionally delicate boy whose mother was over-protective of him, particularly in relation to his older brother, who might be verbally aggressive and at instances vindictive. Daniel and his mother tried to shield each other from the aggressive Early-Onset Depression 139 older brother and, at instances, Daniel would go into the road of fire to shield his mother. However, his mom also had an explosive mood and was controlling and important of Daniel, a few of the time. Daniel was clever and inventive, preferring music and film to extra typical academic topics. Resilience and susceptibility factors It was a confusing family situation for Daniel, to have a mother who was alternately protective, controlling and hostile. It created an ambivalent mother�son relationship and an unstable, unpredictable and uncertain house life. The household conflicts produced an setting that led to each anxious avoidance and submissiveness in Daniel, with proneness to embarrassment, disgrace and humiliation. Over the previous 5 years he had turn out to be extra self-conscious in social conditions: his social nervousness has turn out to be increasingly problematic, leading to intermittent avoidance. In the earlier 2 years, he had been bothered by obsessive thoughts, significantly that he would possibly harm others by saying or doing the incorrect thing. Daniel was confused: he generally felt protected by his mother and liable for her wellbeing. He additionally felt disregarded, controlled and criticized, and in these mental states his self-esteem and self-efficacy markedly lowered.
Discount quibron-t 400 mg with mastercard
Infusionrelated reactions (such as ache at the injection web site allergy medicine for dogs 400 mg quibron-t buy fast delivery, chills allergy medicine 94% 400 mg quibron-t buy with visa, rigors, fever, phlebitis, headache, bronchospasm, hypotension, nausea, and vomiting) happen in 70%�90% of sufferers and may diminish despite continued therapy [9,20,30,31]. Azotemia, hypokalemia, hypomagnesemia, hyperchloremia, renal tubular acidosis, or nephrocalcinosis have all been reported as manifestations of such toxicity [9]. Depending on the manifestation, affected person risk components and formulation of amphotericin B, such reactions occur in 24%�80% of sufferers [30,32]. While amphotericin B continues to be considered an possibility for the prophylaxis of choose patient populations at increased risk of mold infections, such use of amphotericin B has largely been replaced by the extended-spectrum triazoles. More lately, such comparisons have concerned the use of a lipid-based formulation. Caspofungin was higher tolerated than amphotericin B, with a decreased incidence of nephrotoxicity (2. Alternatively, amphotericin B could also be used first-line for empirical or preemptive therapy in choose high-risk Antifungals for prevention and therapy of invasive fungal infections 405 sufferers. Controlled medical trials for the remedy of invasive candidal infections [42�44], along with a more recent meta-analysis [45], have observed the shortage of great differences in mortality rates between AmBd and the comparative agent. In distinction, each echinocandins and fluconazole reveal significant reductions in general adverse results, particularly nephrotoxicity [45]. Although not included within the meta-analysis, voriconazole was subsequently found to be non-inferior to amphotericin B for remedy of candidemia [46]. For remedy of invasive aspergillosis, amphotericin B is currently really helpful as an various to voriconazole remedy [38]. This suggestion is based largely on a randomized study, which compared voriconazole and amphotericin B deoxycholate (1�1. In contrast to its function as alternate therapy in most patients with candidiasis and aspergillosis, amphotericin B (in combination with flucytosine) is still recommended as a "first-line" agent for induction treatment of severe cryptococcal disease, notably meningitis, severe pulmonary infections, and cryptococcemia [39]. Amphotericin B also continues to play a job in the treatment of extreme, invasive histoplasmosis and blastomycosis [40,48�50]. For reasonable to severe cases of blastomycosis, amphotericin B can be thought of first-line therapy based mostly on clinical treatment charges starting from 70% to 91% [40,49]. While flucytosine monotherapy is fungistatic towards most isolates, mixtures with amphotericin B ends in fungicidal activity against most species [54]. Combinations with other brokers cut back the speed of resistance growth in opposition to flucytosine [58�62]. Bioavailability is high (78%�89%), and maximum serum concentrations occur approximately 2 hours after an oral dose [68,69]. Gastrointestinal unwanted side effects (nausea, vomiting, diarrhea, and belly discomfort) occurred in approximately 6% of sufferers receiving flucytosine remedy [69,71]. Hepatotoxicity related to flucytosine use (reported with a variety of 0%�41%) most commonly manifests as reversible elevations in transaminases and/or alkaline phosphatase [69,71�73]. Reversible myelosupression (in as much as 27% of patients) mostly manifests after 2�4 weeks of remedy as either leukopenia or thrombocytopenia [71,73,74]. More commonly, flucytosine is utilized in mixture with other antifungals (notably amphotericin B) to deal with 406 Antifungal use in transplant recipients: Selection, administration, and monitoring cryptococcal infections [39,62], choose infections attributable to Candida spp. For the initial remedy of invasive cryptococcal infections, flucytosine is used in combination with amphotericin B due to poor clinical response charges with either fluconazole or amphotericin B monotherapy [58,72,76�78]. Furthermore, scientific rates have been shown to improve with mixture therapy [39,58]. Amphotericin B in combination with flucytosine improves survival compared to amphotericin B monotherapy or together with fluconazole. Current Infectious Diseases Society of America remedy guidelines suggest amphotericin B plus flucytosine as first-line remedy for the preliminary management of invasive cryptococcal infections [39]. Less frequently, flucytosine together with amphotericin B has been used for select candidal infections (such as endocarditis, meningitis, and endophthalmitis) [3]. Finally, though flucytosine has additionally been used within the therapy of chromoblastomycosis, efficacy information is proscribed to case reviews [75]. Triazoles the triazole class of antifungals consists of fluconazole, itraconazole, voriconazole, posaconazole and most just lately, isavuconazole. These agents share many characteristics; nonetheless, they range greatly with reference to pharmacokinetics, clinical use, and toxicity [80�83]. Triazoles work within the fungal cell membrane and stop the conversion of lanosterol to ergosterol by inhibiting the cytochrome P450 dependent 14-demethylase. While information are restricted with isavuconazole, cross resistance between different triazoles is expected to affect isavuconazole as well. The medical outcome is yet to be characterized; consequently, patients failing prior triazole therapy could require another antifungal class [80,82,83]. In vitro and in vivo knowledge have demonstrated that triazoles have a concentration-independent fungistatic exercise in opposition to Candida spp. As a class, the triazoles reveal favorable exercise in vitro in opposition to most Candida spp. Voriconazole, posaconazole, and isavuconazole demonstrate elevated exercise in vitro (relative to fluconazole) in opposition to each C. Triazoles also show activity in vitro against most endemic mycoses, such as Coccidioides spp. Furthermore, triazoles show activity in vitro in opposition to Cryptococcus neoformans [9,20,ninety six,ninety seven,99]. In contrast to the other triazoles, fluconazole lacks exercise in opposition to Aspergillus spp. Additionally, itraconazole, voriconazole, posaconazole, and isavuconazole exhibit activity in opposition to Fusarium spp. Finally, posaconazole and isavuconazole show exercise in vitro against Mucorales [96,99]. Historically, among the triazoles, fluconazole reveals the most favorable pharmacokinetic profile; nonetheless, lately this is being challenged with the addition of isavuconazole and new dosage formulations of posaconazole. Available in each intravenous and oral (tablets and suspension) dosage formulations, fluconazole reveals linear pharmacokinetics [9,20,96]. Bioavailability following oral administration is excessive (>90%) and independent of gastric pH or the presence of meals for absorption [20,ninety six,one hundred,101]. In contrast, the oral bioavailability of itraconazole is highly variable and pH dependent based on the formulation utilized [20,96]. Overall, the capsule formulation Antifungals for prevention and therapy of invasive fungal infections 407 has a decrease in bioavailability compared to the answer [96]. The oral capsule formulation has optimal absorption when given with food or in the presence of low gastric pH [102]. Voriconazole is on the market as both intravenous and oral (tablets and suspension) formulations [103]. Oral bioavailability is roughly 96%, however could additionally be decreased by about 20% and delayed by an hour when administered with meals [20,103�105]. Therefore, oral voriconazole is recommended to be administered both 1 hour before or 1 hour after meals [103,104].