
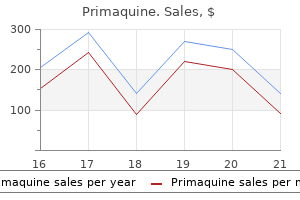
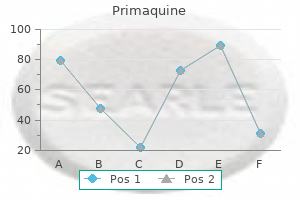
Primaquine dosages: 15 mg
Primaquine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 240 pills, 300 pills

Discount 7.5mg primaquine amex
There are fewer than thirty cases of leiomyoma reported within the English literature medications like lyrica primaquine 7.5mg buy generic on line, with the biggest sequence containing 4 instances medications used to treat depression buy primaquine 7.5mg on line. Generally, sufferers have excellent retention of visible operate and ocular motility as a result of the encapsulated nature of the lesion. If the lesion is located next to the optic nerve, it could produce a compressive optic neuropathy. There are uncommon circumstances of intracranial extension101b,101c and extension into paranasal sinuses101d have been reported. Some vascular-derived lesions might exhibit high-velocity circulate on Doppler ultrasonography. At the time of surgery, the lesions could also be adherent to the surrounding orbital tissues due to their long-standing duration. Careful dissection to find the appropriate cleavage aircraft of the capsule is required, however the lesion is much less readily delivered than are other encapsulated orbital tumors. The nuclei of the tumor cells have ovoid, rounded poles (cigar-shaped) with small nucleoli; mitotic exercise is absent. The cytoplasm is fibrillar and infrequently intensely eosinophilic; with the Masson trichrome stain, nonstriated longitudinal filaments are extra easily demonstrated; when seen in cross-section, many cells have perinuclear halos because of retraction of conglutinated filaments. A variably distinguished and typically strikingly ectatic vascular pattern can be demonstrated throughout the tumor. Intense interstitial collagenization may be seen in older lesions, and even foci of bone formation can be encountered. On immunohistochemical analysis, tumor cells sometimes present optimistic immunoreactivity with vimentin, easy muscle actin, and desmin. Electron microscopy demonstrates the presence of cytoplasmic skinny actin filaments with fusiform densities, pinocytotic plasmalemmal vesicles, plasmalemmal hemidemisomes, and basement membrane formation. Probably the most important histopathologic differential diagnosis is a schwannoma, which additionally shows nuclear palisading and might have a fibrillary background character. Schwannomas are protein S100-positive, present less intense cytoplasmic eosinophilia, and should manifest myxoid foci (Antoni B pattern), features which are virtually always absent in strong leiomyomas. By electron microscopy, a schwannoma contains cells with interweaving processes which may be electron-lucent and devoid of clean muscle filaments, though vimentin filaments and neurotubules may be current in the cytoplasm. Because the delivery of those tumors may be difficult owing to the intense adherence of their capsules to surrounding orbital tissue planes and buildings, great care ought to be exercised and blunt dissection ought to be used as opposed to sharp dissection. There is one case report within the literature of a noncircumscribed orbital leiomyoma which was not ammenable to surgical remedy that has been treated efficiently using the gonadotropinreleasing hormone analogue goserelin. The latter tumor seems as a small, blue-red nodule within the dermis, and is recognized most often between 20 and 40 years of age. Around the orbit, the glomus tumor occurs most frequently in the eyelid skin102, but has been seen in found in the conjunctiva in affiliation with rectus muscles102a as properly. The purpose for this is that tumor appears to take origin from specialized mural smooth muscle cells that are associated with an arteriolar�venular anastomosis that is a thermal regulatory unit and is referred to as the Sucquet�Hoyer canal. Ultrastructural studies show cytoplasmic features consistent with clean muscle differentiation. There are additionally case stories of leiomyosarcoma arising in the paranasal sinuses 105a,105b and secondarily invading the orbit. The nuclear:cytoplasmic ratio is larger than that in benign leiomyomas; nuclear hyperchromatism and pleomorphism are notable, as are mitotic figures. It is an anomaly that rare intraocular tumors may also demonstrate striated muscle differentiation; in some species. The fetal rhabdomyoma happens within the head and neck region of boys from the perinatal period to age 3 years; it has a particular predilection for the retroauricular area. In some instances, these hamartomatous lesions can be seen in the nevoid basal cell carcinoma syndrome and could be associated with malformations of the anterior chamber angle. Most extracardiac rhabdomyomas happen within the head and neck (oral cavity and retroauricular area). There are at least four cases of rhabdomyoma of the orbit117a,117b,117c that have been reported (age vary 16 months to 31 years). On acquiring deeper sections, nonetheless, the connection of the tumor with the medial rectus contained a focus of mitotically energetic spindle cells. These radiological findings are helpful in differentiating the mass from rhabdomyosarcoma. Macroscopically, rhabdomyoma are circumscribed however unencapsulated lots, ranging in color from grey to redbrown. On histopathology the basic tumor shows bland primitive spindled cells associated with fetal myotubules in a myxoid stroma. The intermediate kind present larger differentiation, with interlacing massive strap-like striated cells and rhabdomyoblasts simulating clean muscle. Skeletal muscle differentiation is easily demonstrated in all instances with immunohistochemical staining for myoglobin, desmin, and muscle-specific actin. A postradiation leiomyosarcoma with hanging nuclear pleomorphism and tumor large cells. The tumor cells have a glassy eosinophilic cytoplasm brought on by the presence of filaments. The tumors may be richly vascular; occasionally a prominent lamination of tumor cells around capillaries and venules (perithelial pattern) may be conspicuous, probably signifying that the tumor cells originated from vascular mural easy muscle. Primary orbital leiomyosarcoma is capable of distant metastasis, in addition to of spread into surrounding compartments. It is therefore most likely wisest to proceed with an orbital exenteration based on everlasting microscopic diagnosis. The efficacy of radiotherapy and chemotherapy is unclear, however their use in these lesions has been reported. Note that the orbital connective tissues and easy muscle cells are of neural crest origin (mesectoderm), so not often a neurogenic appearance might be supplied by an orbital connective tissue neoplasm. Benign mesectodermal leiomyomas have been described within the ciliary body of the eye. Rhabdomyosarcoma, in fact, has been reported to come up in the eyelids110 as well as within the conjunctiva. Sometimes this Z-band materials can turn into excessive and seem at the mild microscopic degree as crystalloids. There is a bimodal age distribution of orbital rhabdomyosarcoma, with ~75% occurring throughout the first decade of life. The common age is 7 years old, though the tumor has been found congenitally,126 and even late in life. In some cases, the growth could additionally be so speedy that the proptosis turns into massively exacerbated over a weekend. Rhabdomyosarcoma may also come up from compartments surrounding the orbit and secondarily lengthen into it. Proptosis and paraxial globe displacement are the commonest findings on scientific examination. Blepharoptosis and strabismus could additionally be current, and a mass could additionally be palpable within the orbit.
Diseases
- Hip dysplasia (human)
- Hepatitis E
- Maternal hyperphenylalaninemia
- Dissociative amnesia
- Myalgic encephalomyelitis
- Polycystic kidney disease
Purchase primaquine 15 mg online
In impact medications education plans discount 7.5 mg primaquine visa, the most lateral levator is superior anteriorly and stuck to the anterior superolateral orbital rim medicine engineering primaquine 7.5 mg low price, which immediately counteracts the tendency to retraction. It is essential that the strip be developed far sufficient posteriorly that the fixation not tether the lid superiorly throughout closure. Elner and colleagues reported82 their optimistic expertise with a way using a graded, full-thickness blepharotomy approach originally described and introduced by Leo Koornneef. Both authors currently favor this environment friendly method for the correction of moderate-to-severe eyelid retraction. Scleral spacer grafts interposed between the superior borders of the tarsal plates and the inferior fringe of the recessed levator aponeurosis. The appearance of the levator muscle immediately after levator lengthening by two enjoyable myotomy incisions. Topical brokers embrace phentolamine,83 thymoxamine hydrochloride,eighty four guanethidine sulfate,eighty five,86 propranolol,eighty five and bethanidine. Botulinum toxin kind A interferes with acetylcholine launch from the motor nerve terminal,92 effectively creating a flaccid paralysis that lasts a number of weeks. Complete ptosis of the higher eyelid may be induced by injecting botulinum toxin sort A, 1. The constant abrasion of the cilia against the cornea dangers keratitis or ulceration. Even if the cilia are destroyed, keratinized eyelid pores and skin may still irritate the cornea. An extensive discussion of all the reported causes of higher eyelid entropion is beyond the scope of this chapter. Nonetheless, a thorough history, medical examination, and if needed, conjunctival biopsy, ought to set up the trigger generally. The proper upper eyelid margin is totally inverted owing to tarsal kink syndrome. In anticipation of future ptosis restore, a posterior strategy was used so as to depart the levator undisturbed. Moderate entropion contains the additional findings of lash-to-globe contact in the main place, thickening of the tarsal plate, and lid retraction. In extreme entropion, one finds gross distortion of the eyelid margin, metaplastic lashes. In order to avoid damage to the lash follicles, the surgical aircraft is terminated earlier than approaching within 2 mm of the lid margin. Everting sutures extending into the upper aspect of the tarsal plate are placed, and excess skin is excised before wound closure. When additional eyelid margin rotation is important, the eyelid margin may be cut up at the gray line to a depth of 2 mm. Herpes zoster ophthalmicus is usually evident because of the everyday prodrome, unilateral dermatome sample of vesicular eruption, seasonal incidence, and occasional attribute keratitis and uveitis. Chronic blepharoconjunctivitis often has typical slit-lamp findings, such as lid margin telangiectasia, scurf, collarettes, sebum, meibomian foam, punctate keratitis, papillary conjunctivitis, and marginal corneal infiltrates. Erythema multiforme major (Stevens�Johnson syndrome), usually triggered by a bacterium, virus, or antibiotic, is characterised as cutaneous and mucosal bullous lesions that may heal with vital scarring, dry eye, and symblepharon. Ocular cicatricial pemphigoid, characterized by bilateral progressive subepithelial conjunctival scarring, is finest diagnosed by contemporary conjunctival biopsy findings of linear deposition of antibasement membrane antibodies. Conjunctival Leukoplakia and Marginal Epidermidalization Scarring and metaplasia of the eyelid margin can produce a roughened floor that abrades the cornea and produces an uncomfortable punctate keratopathy in the absence of trichiasis or distichiasis. Keratinization could additionally be treated by excision and overgrafting,104 curettage and cryotherapy,one hundred and one,103,105 and topical retinoic acid. Mere epilation, which has undoubtedly been practiced since time immemorial, could present a quantity of weeks of reduction before the indomitable lash reemerges to joust with the cornea. This observation has resulted in quite a few treatments directed toward the perfect of selective destruction of the lash follicle. The hardy lash follicle is troublesome to eradicate with out inducing harm to adjacent regular eyelid buildings. The inadequacy of current therapies is finest illustrated by noting how the champions of each particular follicle-destructive therapy enthusiastically catalog, within the opening paragraphs of their reviews, the shortcomings of all other therapies. Cryosurgery must be utilized to the concerned lashes twice as a rapid freeze monitored by a thermocouple to �20�C to �25�C followed by a slow thaw to room temperature (Table 258. Blinding acceleration of pemphigoid symblepharon and painful reactivation of trigeminal herpes zoster105 owing to cryotherapy could happen. Frank keratinization of the tarsal conjunctiva by moist white keratin plaques known as leukoplakia. Laser thermal ablation,113 popularized by Ewan,112 is probably the most selective methodology of lash follicle destruction. Recurrence rates of as a lot as 50% have been reported with current methods,a hundred and fifteen and ideal treatment settings have but to be decided. Nonetheless, laser ablation is ideally fitted to sufferers in whom only a few lashes must be treated and in whom retreatment is possible. Apparently, fewer unwanted effects have resulted utilizing contemporary fractionated doses with whole therapies of 2800 to 3200 cGy. Techniques of surgical publicity of lash follicles followed by microscopically controlled lash follicle ablation are beginning to gain favor as surgeons gravitate toward selective follicle destruction for distichiasis. The everted upper eyelid may distract the upper punctum from the tear movie, promote conjunctival epithelialization or exuberant granulation-like lots, and fail to protect the cornea from exposure. The return of the eyelid to a normal place resulted in full cessation of the neuralgia. During this ready interval, one could consider therapeutic massage of tissues and steroid injection in order to improve remodeling of scar tissues. The ready interval ends as quickly as the hypertrophic scars pale, soften, and begin diminishing in dimension. Dissection within this relatively cold aircraft facilitates controlled excision of scar and reconstructive skin grafting. In the case of eyelid burns, it may be very important grade the depth of burn as a result of this guides subsequent administration. Collier J: Nuclear ophthalmoplegia with especial reference to retraction of the lids and ptosis and to lesions of the posterior commissure. Salvi M, Scalise D, Stolarski C: Upper eyelid retraction within the absence of different evidence for progressive ophthalmopathy is related to eye muscle autoantibodies. Goldberg R, Seiff S, McFarland J, et al: Floppy eyelid syndrome and blepharochalasis. Schlotzer-Schrehardt U, Stojkovic M, Hofmann-Rummelt C, et al: the Pathogenesis of floppy eyelid syndrome: involvement of matrix metalloproteinases in elastic fiber degradation.
Primaquine 7.5mg purchase amex
Even full contraction of the frontalis muscle will solely minimally elevate the upper eyelid margin medicine xifaxan 15mg primaquine discount with mastercard. This is clear in patients with unilateral blepharoptosis the place the ipsilateral brow is commonly more elevated and deeper forehead furrows exist within the forehead above medicine 751 m primaquine 7.5 mg with mastercard. This finding represents a unconscious response over time by the frontalis to try to help the ptotic eyelid to elevate. The eyebrow represents a transition from the thicker pores and skin of the brow to the thin skin of the eyelid. The forehead is a part of the higher third of the face as defined by a line drawn through the pupils. When evaluating the forehead, it should be thought of in continuity with the relaxation of the face. The muscular layer is composed of 4 muscle tissue, one elevator and three depressors. Inferiorly it inserts into the supraorbital dermis and interdigitates with the corrugator and procerus muscle. The frontalis muscle spreads laterally across the forehead to the world just above the tail of the forehead. Lack of the elevator muscle lateral to this will intensify the temporal forehead ptosis, or hooding, associated with involutional modifications. Brow melancholy is a perform of three muscular tissues, the orbicularis oculi, the procerus, and the corrugator supercilii. As the muscle circles across the eye the superior fibers be part of the inferior fibers in what is identified as the lateral raphe. The superior arc of this muscle remains superficial to the corrugator, and when contracting pulls the brow inferiorly and closes the eyelid. The procerus muscle originates from attachments to the fascia overlying the nasal bone at the root of the nose. The procerus muscle fibers ascend to interdigitate with the inferior fibers of the central frontalis muscle. Some of those fibers continue through the frontalis to insert within the supraorbital dermis as well. Contraction of this muscle creates horizontal pores and skin folds over the root of the nose and depresses the head or medial side of each brows. The corrugator supercilii can additionally be a strong depressor of the central brow, originating from the glabellar ridges and superomedial orbital rim. Commercially obtainable preparations of injectable botulinum toxin have turn into more and more more well-liked for his or her paralytic impact on each the corrugator supercilii and procerus with subsequent reduction in glabellar rhytids. Pharmacologically weakening these largely vestigial muscular tissues has the esthetic benefit of a extra relaxed and fewer offended facial expression. The frontal department of the facial nerve supplies unique innervation to the frontalis muscle, in addition to to the superior fibers of the orbicularis oculi. Various procedures have been defined to restore the conventional structure of the forehead and brow. Many of our sufferers need to stall or reverse the inevitable modifications related to growing older and regain a younger appearance. Others are just excited about a functional resolution to restore or improve their peripheral visual fields. A thorough evaluation is crucial to separate these useful and esthetic considerations. In patients with vital dermatochalasia, elevating the forehead reduces the feeling of fullness within the higher lid. Patients note marked improvement within the forehead fatigue following brow elevation. It is extremely essential for the affected person to understand the relationship between eyebrow position and dermatochalasia. Branches of the facial nerve providing innervation to the forehead and forehead muscle tissue. The patient subconsciously compensates for this by maintaining frontalis contraction and forehead elevation. Older sufferers will often describe an inability to hold their eyes open within the night because the exhausted frontalis muscle yields to gravity. Over time this chronic frontalis contraction will lead to a rise in the depth and variety of brow furrows. Most usually, patients arrive for consultation with preconceived notions about the power of blepharoplasty alone. While a conservative blepharoplasty might meet the visible concerns of this patient, great care must be taken to guarantee they understand the potential for increased brow ptosis postoperatively. Blepharoplasty will reduce the sense of heaviness on the higher eyelid and globe, decreasing the subconscious drive to elevate the brow. Relaxation of the frontalis contraction will lead to lower forehead place in addition to introducing more pores and skin into the eyelid. Laterally, the galea aponeurotica is steady with the temporoparietal fascia, also called the superficial temporal fascia. The galea aponeurotica splits to cover the anterior and posterior floor of the frontalis muscle. More inferiorly, alongside the posterior floor of the frontalis muscle, the galea splits as quickly as once more to incase the forehead fat pad. The galeal layer posterior to the fats pad has agency adhesions to the supraorbital rim. The portion of the fats pad lateral to this lacks these attachments and is subject to greater gravitational descent. Time spent preoperatively explaining these interrelationships will improve patient acceptance of their surgical outcomes. By explaining to patients that their involutional modifications are a mixture of both forehead ptosis and dermatochalasia they will be more accepting of the suitable surgical solutions and postoperative results. In assessing forehead position and potential surgical procedures, the surgeon should pay consideration to gender differences. Patients are sometimes motivated to surgical solutions when they discover that their brow place and upper lid pores and skin is starting to evolve much as their mother and father did. A history of sun publicity with associated actinic injury as well as tobacco use can even accelerate the involutional modifications of the brow and forehead. Precise observations and measurements must be made through the preoperative assessment. A recording is made of the relative position of the brow to the superior orbital rim.
Effective 7.5mg primaquine
Thus medicine ball slams generic primaquine 15 mg on line, whether or not an eyelid tumor has extended into the orbit may be troublesome to verify medications made easy generic 15mg primaquine overnight delivery. Computed tomography shows an infiltrative or circumscribed mass that enhances with contrast material. In a collection of head and neck angiosarcomas from the Mayo clinic, the 2- and 5-year survival rates were 53% and 41%, respectively. Involvement of the posterior orbit is associated with a bleak prognosis, with most reported patients finally buying recurrent or metastatic tumor. Angiosarcoma accounts for less than 1% of soppy tissue sarcomas and has a predilection for the pores and skin and superficial gentle tissues. It must be remembered that angiosarcoma might attain the orbit by extension from adjacent structures such because the maxillary sinus193 or by metastasis from another main site. These lumina often comprise erythrocytes and may be lined with anaplastic endothelial cells. Because these tumor cells type aggregates, they might type intraluminal buds or papillary projections. The tumor cells could show a spread of differentiation; the differentiated tumors exhibit proliferating endothelial cells outlined with reticulin fibers. Undifferentiated areas are composed of pleomorphic polygonal cells, which resemble epithelial or melanocytic cells. Ultrastructural features differ depending on the diploma of differentiation of the endothelial tumor cells. They might show luminal pinocytotic vesicles, polarized basal lamina, intercellular tight junctions, and intercellular canaliculi. Immunohistochemical stains for endothelial cell markers may confirm the analysis of angiosarcoma. Lectins are animal or plant proteins that show specific binding to sure glycoproteins. Ulex europaeus agglutinin I lectin is a helpful marker for endothelial cells186 and has shown positive staining of angiosarcoma cells. Similarly, if the diagnosis of angiosarcoma was unsure, labeling of contemporary tissue with fluorescent acetylated low-density lipoprotein could present evidence for an endothelial-cell origin of the tumor. The tumor is present in adults and is characterised by an epithelioid or histiocytoid endothelial cell part. Hemangiopericytoma, which is derived from pericytes that surround blood vessels, has a predilection for the orbit. In the orbit, the tumor usually develops throughout the lumens of thrombosed orbital varices and should rarely come up within arteries. Orbital intravascular papillary endothelial hyperplasia usually causes progressive proptosis and has a well-circumscribed look on computed tomography. Surgical excision is normally healing, though native recurrence could develop at a later time. Microscopically, there could additionally be remnants of the preexistent vein or artery on the periphery of the tumor. The fronds of endothelial cells often type a single layer however could kind a quantity of concentric layers around the cores of fibrin or collagen. Electron microscopy demonstrates spindle-shaped cells with features of endothelial cells forming a polarized basement membrane and containing quite a few micropinocytotic vesicles on the plasmalemma. A 55-year-old man acquired proptosis, conjunctival an infection and chemosis, restricted motility, and ache in the best eye. The lumen is occluded by organizing the thrombus with areas of papillary hyperplasia. Patients with malignant nerve sheath tumor have a high mortality rate as a end result of both intracranial extension and distant metastasis. The major therapy of those tumors is complete excision, usually exenteration for orbital tumors. Because of the proclivity for extension alongside nerves, examination of margins with frozen sections might point out the need for craniotomy. Although the tumor may be immune to adjuvant therapy, chemotherapy or radiotherapy is commonly combined with surgical excision of the tumor. Late recurrences, nonetheless, can happen, as evidenced by one affected person who developed recurrence 18 years after preliminary surgical resection of the tumor. Patients with neurofibromatosis reportedly have a 3�13% likelihood of acquiring a malignant nerve sheath tumor; nevertheless, these figures may be exaggerated. These tumors sometimes come up in the main nerve trunks, such because the sciatic nerve, the brachial plexus, and the sacral plexus. Thus, the tumors characteristically develop within the proximal portions of the upper and lower extremities and the trunk. Isolated case stories have appeared describing orbital tumors in patients with and with out neurofibromatosis. Clinically, the looks of a mass beneath the uneroded skin of the supranasal quadrant suggests the potential for a malignant nerve sheath tumor. There could also be ache, hypesthesia, or anesthesia within the distribution of the involved nerve. In the collection of orbital malignant nerve sheath tumors reported by Jakobiec and colleagues,215 the sufferers ranged in age from 19 to 75 years, with half the patients youthful than 50 years. There was no strong sex predilection, with 5 men and three ladies in the series. Patients with malignant nerve sheath tumor had a poor prognosis, with an especially speedy and unfavorable clinical course after incomplete excision. The tumor exhibited regionally aggressive behavior and a strong neurotropism frequently extending alongside the trigeminal nerve toward the middle cranial fossa, with involvement of the pons demonstrated at post-mortem in two cases. These cells also exhibit a high mitotic rate and nuclear pleomorphism, suggesting the malignant habits of the tumor. Heterotopic components may be present, including bone, cartilage, muscle, and glandular tissue. She subsequently underwent orbital exenteration with resection of the frontal bone however acquired intracranial invasion of the tumor and died ~1 yr later. Radiologic adjustments of the orbit and skull reflect the lytic, mixed, or sclerotic phases of the illness. The prognosis is made by the attribute radiographic findings, and an elevated serum alkaline phosphatase level could also be found. Ophthalmic mani- festations can include angioid streaks, choroidal sclerosis, and extraocular muscle palsies. One attention-grabbing affected person offered with a 5-year historical past of progressive proptosis and limitation of ocular motility. Also, improvement of proptosis may sign sarcomatous transformation of the skull involving the orbit. This thickening develops in affected infants after which subsides over a quantity of months without inflicting everlasting ocular injury. The brown tumor is a focal lesion of bone associated with hyperparathyroidism, which may develop in the orbit.
Bonplandia trifoliata (Angostura). Primaquine.
- How does Angostura work?
- Fever, diarrhea, spasms, induce vomiting, preventing return of malaria, and purging the bowels.
- Are there safety concerns?
- Dosing considerations for Angostura.
- What is Angostura?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96712
Order 7.5mg primaquine fast delivery
Usually medicine 4 the people primaquine 7.5 mg fast delivery, the iris is inflamed 5 medications primaquine 15mg buy otc, and the uveal tract is concerned with a continual nongranulomatous inflammation. Other related disorders are: phacogenic uveitis, a poorly defined entity which additionally happens after lens protein publicity and is characterized by nongranulomatous inflammation; phacolytic glaucoma, which happens in the context of a hypermature cataract with presence in the anterior chamber of macrophages laden with denatured lens materials that block the anterior chamber drainage system. Molecular mimicry, a course of by which an immune response directed in opposition to a foreign protein cross-reacts with a standard host protein, might play a role in autoimmunity. Inflammatory cells then invade and release more cytokine proteins that regulate the event and triggering of lymphocytes. Tissue Reactions to Artificial Intraocular Lens Implants In eyes with intraocular lens implants, an inflammatory reaction of the iris and ciliary body can occur. Granulomatous response to the implanted lens is much less widespread and is most often seen when the haptics (positioning loops of artificial lens) are in contact with the iris and the ciliary body. Chronic inflammation of the ciliary physique was observed in 18�33% of eyes on histopathologic examination however was famous clinically in solely 0. Granulomatous irritation could be seen at the erosion website brought on by the haptics. Transient and chronic inflammatory reaction could also be associated to the intraocular lens and surface contaminants; multinucleated big cells are probably a reaction to a overseas physique (an intraocular lens). It contains isolated ocular involvement or association of ocular inflammation and systemic illness. The latter comprises ankylosing spondylitis, reactive arthritis (including Reiter syndrome), psoriatic arthropathy, inflammatory bowel disease with arthritis and undifferentiated spondylarthropathy. Various environmental factors have been instructed, primarily infectious agents corresponding to Chlamydia trachomatis and the gram-negative enterobacteria Klebsiella, Salmonella, Yersinia, Shigella and Campylobacter jejuni64 Different theories have been proposed together with the Anterior Autoimmune Uveitis the prevalence of acute anterior ocular irritation or uveitis is 0. It is the most common form of uveitis accounting for 50�92% of all uveitis circumstances generally occurring between age 20 and age 50. The basis of autoimmune uveitis lies in the complex interplay of regulatory controls that function antimicrobial and antineoplastic defenses but assault ocular cells. In every instance, specific bacterial pathogens could infect a distant website, resulting in a sterile inflammation within the eye and different organs. In 80% of sufferers, the condition is bilateral, and if initially unilateral, it eventually affects the contralateral eye in 30%. The entrance of the attention stays relatively unaffected, with irritation starting at concerning the peripheral pars plana. Other issues embrace cataract, angle-closure glaucoma from peripheral anterior synechiae, retinal and choroidal neovascularization, and vitreous hemorrhage. Few macrophages, B cells, or pure killer lymphocytes are present within the inflammatory infiltrate. However, B lymphocytes predominate inside the aqueous humor and on the iris-ciliary body junction. It is often a persistent bilateral nongranulomatous anterior uveitis of variable severity, small keratic precipitates, anterior synechiae and anterior vitreous cells. The iris may present infiltration by plasma cells, occasionally containing Russell our bodies. Immunoglobulins M and G are current in the anterior chamber aqueous between acute attacks, suggesting that the primary insult ends in a leaky blood�ocular barrier. This facilitates sequestering of circulating antigenantibody complexes and results in recurrence and chronic inflammation. Cystoid macular edema is commonly found, and to a lesser extent, retinal vasculitis and subretinal neovascularization occur. The physiopathology of Birdshot chorioretinopathy implies an autoimmune course of affecting the choroid and the retina. This would again counsel a genetic susceptibility associated with environmental elements. Heterochromia is secondary to stromal iris atrophy that can have a patchy distribution. The involved eye can truly be darker if the stromal atrophy unmasks the pigmented epithelium. Lymphocytes (a combination of interleukin-2 receptor-negative helper and suppressor T-cells and B lymphocytes) and plasma cells infiltrate the iris and the ciliary body. Hyalinization of iris arterioles contributes to their fragility and vascular occlusion. Based on these findings, a vascular trigger to this dysfunction has been instructed but no evidence for energetic vascular inflammation has been discovered. Findings of abnormal melanin production together with membranous degeneration of nerve fibers lead some authors to recommend abnormal adrenergic innervation, both primary or secondary to the inflammation. Fluorescein angiography shows early hypofluorescence of the patches, adopted by hyperfluorescence within the late venous phase. The course of normally begins within the peripapillary region and extends by recurrences in an irregular style to the midperiphery. Retinal vasculitis, papillitis, hyalitis, and neovascularization have occasionally been observed. Defects in Bruchs membrane may happen, allowing subretinal neovascularization and fibrosis to extend into the choroid. The reason that septic emboli happen more incessantly in the retina than within the choroid is unknown. Diffuse irritation shows quite a few micro organism and inflammatory cells with necrosis and hemorrhage of the involved tissues. During the course of bacteremia, any causative bacteria can lodge in eye and produce endophthalmitis. Certain organisms clearly have a tendency to invade the eye from the blood stream. In massive tuberculomas, caseation necrosis is present with zonal granulation surrounding the coagulative necrosis. Miliary choroidal tuberculosis causes a multifocal, discrete, sarcoid-like irritation, but with caseating necrosis affecting the centers of the epithelioid granulomas. Leprosy (Mycobacterium leprae) this disease affects 10 million folks living between the tropics of Cancer and Capricorn. In lepromatous leprosy, ocular involvement includes the cornea, sclera, and iris; iridocyclitis can be either insidious or acute and exudative. The iris often develops striking white globular our bodies enmeshed in the stroma (leprotic pearls). In lepromatous leprosy, histopathologic examination reveals granulomatous irritation occurring with characteristic formation of lepromas. In tuberculoid leprosy, lesions are akin to noncaseat- Metastatic Bacterial Endophthalmitis Several distinct scientific types of metastatic bacterial endophthalmitis can be empirically designated as focal (anterior or posterior), diffuse (anterior or posterior), and panophthalmitis.
15 mg primaquine order free shipping
Moderate defects (40�50%) of the upper and decrease lid should be transformed in a pentagonal lid defect by freshening the margins and then closed with cantholysis and often a semicircular flap as described by Tenzel symptoms jaw pain and headache buy primaquine 7.5 mg with amex. In the lower lid medicine 877 primaquine 15mg with visa, they tend to happen on the junction of the middle and lateral third of the lid and are sometimes associated with systemic anomalies, most notably the autosomal dominant situation mandibulofacial dysostosis (Treacher Collins syndrome). Defects in the upper lid are inclined to be full thickness, with the adjoining lid margin normal. In the lower lid, partial-thickness defects with adjoining margin abnormalities are more common. Morphologically, these defects vary from small divots in the lid margin to large triangular or quadrilateral defects involving the complete lid margin. A variety of theories have been postulated concerning the pathogenesis of those defects. It is usually inherited in an autosomal dominant trend with incomplete penetrance; however, sporadic circumstances are well recognized. It is believed that this situation is said to a main growth arrest of the canthal space on the time of growth of the lid fold. The resultant fusion of the lid at the lateral or medial canthus can provide rise to pseudoexotropia or pseudoesotropia, respectively. In exterior ankyloblepharon, a lateral canthoplasty could be performed when the patient is 3�4 years old, with care taken to go away an overlying edge of conjunctiva to avoid keratinization of the lid margin and secondary corneal irritation. Burns and Cahill have emphasised that in inner ankyloblepharon, the medial canaliculus and punctum could additionally be concerned, and any restore on this area should contain cautious identification of these buildings. The situation often presents as an isolated medical finding; nevertheless, different associated ocular anomalies embrace ptosis; a double row of meibomian glands; lateral displacement of the inferior punctum; strabismus; and telecanthus. The exact explanation for congenital euryblepharon is unknown, but proposed mechanisms embody abnormal separation of the lid fissure, irregular displacement of the lateral canthus, abnormal pull of the platysma muscle, and hypoplasia of the orbicularis muscle or the tarsal plate. This abnormality has been reported in isolation, with other abnormalities, and in affiliation with other syndromes. Type 3 is related to ectodermal syndromes such as the popliteal pterygium syndrome, which is characterized by cleft lip or palate, popliteal pterygia, and genitourinary abnormalities, whereas type 4 is associated with cleft lip or palate alone. The occurrence of various systemic abnormalities with this situation underscores the importance of a pediatric assessment and genetic counseling for these patients. Pathologically, these bands have been proven to be composed of an outer layer of epithelial tissue overlaying a fibrovascular core. It has been proposed that a relative arrest of epithelial growth permits a more fast proliferation of mesodermal tissue to bridge the longer term lid fissure. The subsequent separation of the lid fold stretches these bands and contributes to their sometimes-elongated appearance. It is important to accurately determine the underlying defect in these patients, as a end result of this to a degree dictates the surgical method used in the repair. If downward displacement of the lateral canthus is critical, a lateral canthoplasty is indicated, with reattachment of the lower limb of the lateral canthal tendon to a more superior and posterior position on the orbital rim. This procedure may be mixed with shortening of the lower lid if a redundancy of the lower lid is noted at the time of repair. Epicanthus palpebralis, the most common sort of epicanthal fold, is characterized by a fold of skin that begins medially and is symmetrically distributed between the upper and the decrease lid. Epicanthus tarsalis is most incessantly encountered in Asians and consists of a skin fold originating from the lateral side of the upper lid and extending to the medial canthal area earlier than dissipating. Epicanthus inversus (see part on Blepharophimosis Syndrome) is usually associated with other lid anomalies and consists of a fold of skin originating in the lower lid and extending upward to the medial canthal area. Proposed mechanisms embrace arrested fetal development, hypoplasia of the nasal bones, and an extra or deficiency of pores and skin within the medial canthal space relative to bone development. In some cases, a hereditary component is apparent, and that is especially true of the dominantly inherited blepharophimosis syndrome. What is widespread to all these strategies is the rotation of skin from areas of relative extra to areas of relative deficiency. Despite the variety of procedures advocated to restore this deformity, sure widespread surgical ideas apply to all strategies of repair. It is necessary to fastidiously dissect the orbicularis from the transposition flap to have the ability to flatten the medial canthal space. Carefully sutured apposition of the skin edges is required to cut back postoperative scarring. Four forms of epicanthus are actually recognized, depending on the position of the pores and skin fold: epicanthus palpebralis, epicanthus tarsalis, epicanthus supraciliary, and epicanthus inversus. It can involve either the higher or the decrease eyelid, though involvement of the decrease eyelid is far more frequent. Epiblepharon often resolves spontaneously within the first few years of life, with growth of the nasal bridge. Important within the preliminary assessment of those patients is distinguishing this condition from congenital entropion, marked by an precise turning inward of the eyelid margin and lashes. Initial remedy is conservative, with the use of topical lubricants and attention to the ocular surface. If irritation of the ocular floor necessitates surgical correction, simple excision of the excess skin and orbicularis with main closure of the wound has proved to be efficient. Congenital entropion tends to worsen with time, whereas epiblepharon usually spontaneously improves. In circumstances by which the corneal epithelium is in good condition, surgery is elective. The really helpful therapy is to take away a horizontal strip of pores and skin and orbicularis beneath the eyelid margin and reattach the lower lid retractors to the tarsal plate to trigger eversion of the decrease lid. In this condition, a vertical kink develops in the tarsal plate of the higher lid in utero, resulting in direct apposition of the lid margin to the globe. This situation requires instant consideration, as a outcome of corneal scarring and an infection are early complications. If extra horizontal lid laxity is discovered, then a horizontal lid-shortening procedure could be corrective. The lower lid ectropion related to blepharophimosis is due to inadequate vertical lid pores and skin and could be corrected with a tarsal strip procedure. A variant of congenital ectropion is total bilateral eversion of the higher lids in newborns, initially described by Adams in 1896. This can generally be achieved conservatively by use of lubrication and a moisture chamber. Chlamydial infection can also trigger this and applicable smears and cultures should be done. Females with type 2 could additionally be infertile owing to hypogonadism and specific hormonal deficiencies.
Primaquine 15mg overnight delivery
The major drawback is in distinguishing between neoplastic and inflammatory proliferations aquapel glass treatment purchase primaquine 15 mg. In addition to relying on applicable morphology treatment tinnitus cheap primaquine 15 mg without a prescription, the prognosis of a neoplastic proliferation might relaxation on the demonstration of monoclonality. Because most orbital lymphoid proliferations are of B-cell lineage, this dedication is often not required. These antibodies can also be used to determine the forms of lymphocytes current in an inflammatory course of. Staining for expression of the Bcl-2 protein has turn out to be useful in the differentiation of follicle center-cell lymphomas from reactive follicular hyperplasia. These are digested in a buffer with proteinase K to destroy cell cytoplasm and enzymes. The combination is then extracted with phenol and chloroform to take away protein and cellular debris. The other bands are germline bands from nonlymphoid cells present within the specimen. The tissue is placed into a guanidinium isothiocyanate buffer and homogenized in this to disrupt cytoplasm and destroy nucleases. If a lymphoma is current, the cells are all derived from one precursor cell, and all have the same gene rearrangement. If more than 1% of the cells current have the identical rearrangement, a band might be produced on a Southern blot and a monoclonal population shall be identified. From Blanco R: the polymerase chain response and its future functions in the clinical laboratory. The primers hybridize in such a fashion that extension from every 3-hydroxyl finish is directed towards the other. If the newly synthesized strand extends to or beyond the region complementary to the opposite primer, it acts as a template for new primer extension response. After ~30 cycles, the primers and deoxyribonucleoside triphosphates are progressively exhausted, the Taq polymerase is saturated with product, and the response reaches a plateau. The primers are designed to flank only a rearranged immunoglobulin H gene so that no bands are produced from nonlymphoid cells. If a monoclonal population is present, a robust band within a sure measurement range is produced. Because of this, the most meticulous laboratory method is required, as is the inclusion of established constructive and adverse control samples. All of those and different molecular strategies are also used as analysis tools in ophthalmology. In recent years, the genetic mutations in lots of hereditary ailments with ocular involvement have been identified and some of these genetic checks have turn into available for scientific testing of sufferers to screen for illness (Table 269. It is essential to recognize that genetic testing depends on patient selection. Patients with convincing phenotypic proof of illness or a member of the family with a recognized mutation are the most effective candidates for genetic testing. Yin X-M, Dong Z: Essentials of apoptosis: a guide for basic and medical research. Symonds H, Krall L, Remington L, et al: p53-dependent apoptosis suppresses tumor development and development in vivo. Henderson S, Rowe M, Gregory C, et al: Induction of bcl-2 expression by EpsteinBarr virus latent membrane protein 1 protects contaminated B cells from programmed cell dying. Pelletier M, Rossignol J, Oliver L, et al: Soluble factors from neuronal cultures induce a particular proliferation and resistance to apoptosis of cognate mouse skeletal muscle precursor cells. Iwaki T, Iwaki A, Tateishi J, et al: Alpha B-crystallin and 27-kd heat shock protein are regulated by stress situations within the central nervous system and accumulate in Rosenthal fibers. Pezzella F, Gatter K: What is the value of bcl-2 protein detection for histopathologists Narayanan S: Concepts, ideas, and purposes of selected molecular biology strategies in scientific biochemistry. New York: Oxford University Press in cooperation with the American Academy of Ophthalmology; 2006. The plica is a semilunar fold of loose conjunctiva near the internal canthus, wealthy in goblet cells. Cryptophthalmos in a young boy from Guatemala, with eyelid colobomatous defects, and lid fusion to the globe. Cryptophthalmos is related to multiple main malformations in over half the circumstances, called Fraser syndrome (syndactyly, malformed ears, craniofacial anomalies, irregular genitalia, etc). Some authors have postulated that colobomas and cryptophthalmos might indeed symbolize a spectrum of the identical deformity, grading from the least severe isolated eyelid coloboma, to the most severe coloboma with superior cryptophthalmos (associated with deformities of the nostril and higher lip too). In the conjunctiva, they embrace vascular or lymphatic abnormalities (capillary hemangiomas or lymphangiomas). They are highly vascular, unencapsulated tumors that are troublesome to handle, because of their intermingling with normal adnexal/orbital constructions. Note additionally the pine needle-shaped ldl cholesterol clefts, indicating distant hemorrhage within the mass. Histopathology exhibits edematous conjunctiva, and papillary projections with a single central blood vessel in each one. In the conjunctiva, hamartomatous lesions include dermoids, lipodermoids, episcleral osseous choristomas, complex choristomas, and ectopic lacrimal gland. The most common location of the stable conjunctival dermoid is the inferotemporal limbus. A lipodermoid (or dermolipoma) is a variant of the strong conjunctival dermoid, and is usually located in the lateral canthus. It incorporates outstanding adipose tissue, and could additionally be invested within the lateral rectus muscle tendon insertion (making surgical excision extra difficult). Conjunctival inflammations are frequent disorders, as a result of the conjunctiva is prone to assault by a selection of exogenous agents (bacteria, particles, poisonous agents, eye drops). Conjunctival inflammation may be divided into two broad scientific patterns; acute and continual. The kinds of inflammatory Summary Table of Conjunctival Inflammations and Infections A Working Classification 1. Systemic or dermatologic disease-related (see box Conjunctival Manifestations of Systemic Diseases and Dermatologic Diseases) cellular infiltrates differ in several problems; neutrophils are conspicuous in acute bacterial infections, eosinophils and basophils in acute allergic responses. Mononuclear cells are present in lower-grade viral infections, and multinucleated large cells can happen in herpetic or overseas physique reactions. The giant papillae are often polygonal and flat-topped and include multiple blood vessel, because of chronic coalescence of a quantity of papillary fronds. Histopathology reveals mounds of amorphous eosinophilic materials, which consists of exudates of immunoglobulin protein and fibrin. Acute papillary conjunctivitis is characterised by vascular dilatation (hyperemia) and edema (chemosis). The velvet look is due to dilated capillaries which might be viewed on-end, inside their small papillary projections. Acute papillary conjunctivitis is nonspecific, and has a number of causes (including infectious, allergic, toxic).
Purchase 15mg primaquine otc
Scarring may develop if this extraordinarily thin pores and skin is treated like thicker facial skin symptoms flu 7.5 mg primaquine purchase fast delivery. The medial third of the pretarsal and preseptal eyelid skin is vulnerable to medications ok for dogs primaquine 7.5 mg order visa scarring and should be treated cautiously. The pretarsal skin ought to be left untreated in patients with important lid laxity and threat of ectropion. The higher eyelid is treated just like the decrease eyelid with one move or at most two low-density passes, placed superior to the higher eyelid crease. A specialised laser eyelid clamp bar (Khan-Baker Laser Eyelid Clamp, Storz Instrument Co. The lateral chin and cheek skin overlying the mandible is vulnerable to scarring, heals slowly, and incessantly provokes pruritus postoperatively. The nasolabial folds and marionette strains respond incompletely to even heavy laser resurfacing. Some upper lip rhytids are fairly deep and inconceivable to take away completely with out creating scarring. Treatment should extend barely across the vermilion border to keep away from a demarcation line. With experience, extra passes could additionally be delivered to specific lip rhytids in patients at low danger for scarring. A good good factor about resurfacing of the upper lip and chin area is a slight lip eversion and increased vermilion present. Concerns have been revealed relating to the tremendous propensity of the skinny neck pores and skin to scar. If active zits is present, resurfacing must be delayed to avoid additional scarring as a outcome of reactivation of zits in the course of the therapeutic part. Elevated scars must be shaved until flush with the encircling tissues, after which the scar and surrounding tissues are resurfaced so as to mix together after reepithelialization. Thin flat scars could also be handled with a easy resurfacing so as to blend with surrounding areas. Widened scars might reply to laser excision adopted by reapproximation of the wound edge. Trap-door deformities or tissue elevations typically seen adjacent to scar edges could additionally be flattened by resurfacing and shrinking the elevated areas. Some areas distended by persistent edema, together with malar luggage will respond properly as a result of the laser reverses the continual collagen laxity. Depressed scars may be debulked using pinpoint pulsed laser vaporization techniques. In: Proceedings of the twenty seventh Annual Symposium of the American Society of Ophthalmic and Plastic Reconstructive Surgery, Chicago. Such lesions are normally vaporized using a 3-mm-diameter single-spot pulsed laser approach. A colour change from yellow-white to reddish brown indicates that the lesion has been completely vaporized, normally to the extent of the orbicularis muscle. For unknown causes (possibly associated to the laxity of adjacent skin and intensely skinny dermis) these deep laser wounds typically heal nicely without scarring. Titanium laser eye defend with unique antirotational posts and eyelash traction bar. Retreatments are usually lighter than the unique treatment as a outcome of part of the dermis has already been ablated. Although occlusive dressings are believed to accelerate wound healing and cut back instant postoperative discomfort, the creator advises against postoperative dressings due to the chance of an infection and toxic shock. Patients are instructed to not choose at crusts because they might incite bleeding or scarring. Gauze sponges soaked in white vinegar and ice water, blended as 1 tablespoon of white vinegar to 1 pint of chilled distilled water, are utilized thrice day by day for a soothing antipruritic effect and for antibacterial exercise. Reepithelialization is often accomplished by days 7�14 depending on the age of the patient � though rarely therapeutic could also be delayed a yr or longer. Topical antibiotics or other sensitizing topical brokers ought to be averted because 65% of sufferers develop contact dermatitis. Pretreatment oral antibiotics should present sufficient gram-positive coverage and stop frank erysipelas or cellulitis. Alternatively, Erythromycin 250�500 mg orally four times per day or Dicloxacillin 250 mg orally 4 times per day may be prescribed. Cellulitis after resurfacing often seems within 2�10 days of surgical procedure and may be characterised by redness, discomfort, exudate, and often an accompanying foul odor (Tina Alster, private communication, 1996). Acne or milia may present across the time of epithelialization or thereafter and are associated with topical white petrolatum application. Milia regularly follow laser resurfacing and appear clinically as a painless crop of small, white, dome-shaped elevations. Herpetic infections must be handled by increasing the Acyclovir, Valacyclovir, or Famciclovir dose to the levels used to treat herpes zoster, possibly including intravenous therapy. The lesions related to laser resurfacing might seem atypical as a crop of small, uncooked, pink lesions (more raw-looking than the surrounding resurfaced skin) clustered as a small grouping. There is most likely not a characteristic vesicular stage if the dermis has not but regenerated. These erosion-like lesions might progress to typical discrete white punctate lesions, and more lesions could appear if the outbreak is left unchecked. Candida could superficially colonize the moist pores and skin floor, usually before reepithelialization. Some surgeons in humid locales routinely treat all patients prophylactically with a single oral dose of Fluconazole (Diflucan) 200 mg orally before resurfacing. However, the author has not found this needed and avoids routine prophylaxis because of the numerous drug interactions associated with Fluconazole, a fungal cytochrome P-450 inhibitor. Hyperpigmentation normally results from elevated epidermal melanin in addition to the buildup of melanin in subepidermal macrophages. Itching is normally most intense along the mandibular border or pretrichial brow. Patients could evidence telltale petechiae or excoriations and be unaware that they scratch and abrade this space while asleep. Treatment includes delicate antiinflammatory steroids, ice packs or cool soaks, and an oral antihistamine similar to oral Diphenhydramine (Benadryl) 50 mg taken earlier than going to sleep. For the anxious or apprehensive patient in whom pruritus interferes with sleep, Doxepin hydrochloride (Sinequan capsules) 25 mg taken orally at bedtime ought to induce drowsiness, reduce anxiety, and diminish itching. Once reepithelialization is complete, the intense erythema may be disguised with a concealer consisting of a dense yellow or green base coated by a flesh tone. Concealer could also be bought from division retailer beauty counters or prepared for the affected person during session with a makeup artist, expert beautician, cosmetic marketing consultant, or aesthetician. Although extended erythema beyond 3 months is sometimes famous in extraordinarily fair individuals with clear skin, it will definitely resolves in most cases. There are anecdotal reports of using the pulsed dye laser with a 1-mm spot measurement to treat persistent erythema.
Primaquine 7.5mg purchase line
Given its parasympathetic innervation treatment meaning 15mg primaquine generic with visa, the main lacrimal gland was thought to take part in reflex lacrimation symptoms celiac disease 15mg primaquine cheap overnight delivery. However, research have revealed that after elimination of the principle lacrimal gland, keratitis sicca develops in the involved eye regardless of normal-functioning accent lacrimal glands. The lacrimal artery provides the gland before continuing anteriorly to provide blood to the temporal upper and decrease eyelids. The ectoderm embeds itself into the surrounding mesenchyme and forms an epithelial wire. The wire extends cephalad and caudad to attain the ocular and nasal ends of the pathway. The opening or entrance into this tear drainage system is via the superior and inferior puncta. The lacrimal papilla separates the ciliated eyelid margin, lateral to the punctum, from the nonciliated lid margin medially. The inferior punctum is located barely extra laterally (1�2 mm) than the superior punctum. As the face develops, the maxilla grows extra rapidly than the frontal bone, stretching the inferior canaliculus additional laterally. The ampulla is the beginning of the stratified squamous epithelium-lined drainage system. The canaliculus is 1�2 mm in diameter and is roofed by fibrous connective tissue which begins at the lacrimal papilla, and extends to surround the lacrimal sac because the lacrimal fascia. Closer to the lid (distally), the canaliculi are enveloped by the muscle of Riolan. These pretarsal fibers gradually wrap round to the posterior surface of the canaliculi, the place they be part of with fibers from the muscle of Riolan at the place of the common canaliculus. In the remaining 90%, the upper and decrease canaliculi join to form a standard canaliculus earlier than entering the lacrimal sac. The lacrimal sac lies throughout the lacrimal sac fossa, a bony depression on the inferomedial orbital rim. The superomedial orbital bony rim descends to terminate as the posterior lacrimal crest. Anatomy of the Eyelids, Eyebrow, Midface, and Lacrimal Drainage System onto the posterior lacrimal crest adjacent to the lacrimal sac and are thought to play a role within the lacrimal pump mechanism. The intricacy of the medial canthal muscular and fascial network to the lacrimal excretory system allows the environment friendly draining of tears from the conjunctival lake. Several theories concerning lacrimal pump mechanics, driven by orbicularis contraction, have been outlined. Jones48 postulated that during an lively blink, contraction of the orbicularis oculi would compress the ampulla and canaliculi, propelling the tears towards the lacrimal sac. He additionally advised that the simultaneous contraction of the pretarsal and preseptal orbicularis would increase the lacrimal sac creating adverse pressure inside, thereby drawing the tears from the canaliculi into the sac. A negative-pressure section was recorded only on the end of each blink, drawing the tears from the tear lake into the canalicular system instantly after lid opening. The incomplete circle of the orbital rim (demonstrated in red), the lacrimal fossa between the anterior lacrimal crest (A) and the posterior lacrimal crest (P), and the sutura notha (arrow). Oriented vertically through the middle of the lacrimal fossa runs the lacrimomaxillary suture, the union of these two bones. Ethmoidal sinus air cells pneumatize the lacrimal bone and extend anteriorly into the region of the lacrimal sac fossa in ~93% of orbits. If observed on dissection, the sutura notha can alert the surgeon to the proximity of the anterior facet of the lacrimal sac. The descending process of the lacrimal bone joins the ascending extension of the inferior turbinate bone to type the medial wall of the canal. This relational anatomy explains the infrequent but serious complication of cerebrospinal fluid leakage after exterior dacryocystorhinostomy. The total length of the lacrimal sac is 10�15 mm on common with a width of 3�5 mm. Once the lids are separated such that the puncta are open, the negative pressure inside the system attracts tears from the tear lake into the ampullae and canaliculi. A membranous or mucosal phase of the nasolacrimal duct extends for a further 3�5 mm beneath the inferior turbinate before opening into the nasal cavity at the ostium lacrimalis. The ostium is located ~30�35 mm inward from the external nares in adults and ~20 mm in infants. The toddler nasolacrimal duct, in contrast with that of an adult, displays less lateral angulation and a more medially angled path alongside its bony course, owing to the immature facial and nasal bony anatomy. The valve of Rosenm�ller, positioned between the canaliculi and the lacrimal sac, helps to forestall the retrograde flow of tears back towards the eye. The valve of Hasner, located on the entrance of the nasolacrimal duct into the inferior meatus, is a fold of the nasal mucosa and epithelium. Sensory innervation from the lacrimal drainage system is distributed through each ophthalmic (V1) and maxillary (V2) divisions of the trigeminal nerve (V). The infratrochlear department of the nasociliary nerve (branch of V1) receives input from the medial lid and canthal area. Vascularity of Lacrimal Drainage Region the vascular supply to the area of the nasolacrimal fossa is primarily from the exterior carotid artery. The exterior maxillary artery branches from the carotid underneath the mandible and continues throughout the face within the nasolabial fold as the facial artery. The continuation of this vessel superiorly along the levator ala nasi muscle is termed the angular artery. The venous branches (facial and angular vein) follow a course similar to that of their arterial counterparts. Ettl A, Priglinger S, Kramer J, et al: Functional anatomy of the levator palpebrae superioris muscle and its connective tissue system. Katowitz Congenital anomalies of the eyelid are a various group of issues with a wide spectrum of clinical shows. An understanding of the surgical anatomy, pure history, and administration options is fundamental to the profitable remedy of those often-difficult instances. The function of this chapter is (1) to evaluate the pertinent historical, medical, and present therapeutic options out there and (2) to help to facilitate essentially the most accurate prognosis and appropriate administration of these anomalies. The surgical procedures are outlined in precept, and readers are referred to the appropriate references for extra detailed accounts. Congenital ptosis deserves extra complete consideration and is discussed in detail elsewhere on this quantity (see Chapter 256). For ophthalmologists coping with congenital eyelid anomalies, it is very important recognize that many of these abnormalities are related to systemic issues. Assessment of these sufferers ought to minimally include a radical bodily examination by each an ophthalmologist and pediatrician. Further subspecialty evaluations and particularly genetic counseling ought to be made out there to the mother and father to enable them to make knowledgeable choices in regards to the risk to potential future offspring. An understanding of the pure historical past of these anomalies is essential because some could resolve spontaneously.