
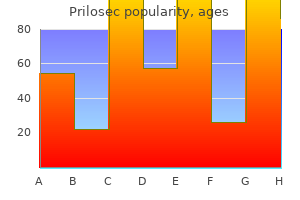
Prilosec dosages: 40 mg, 20 mg, 10 mg
Prilosec packs: 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps
Buy 40 mg prilosec overnight delivery
Multiple spinal intramedullary cavernomas with vascular pores and skin nevus or "Cobb syndrome": a case report chronic gastritis liver disease prilosec 20 mg effective. Three-dimensional angioarchitecture of spinal dural arteriovenous fistulas gastritis diet 7 hari 20 mg prilosec purchase overnight delivery, with special reference to the intradural retrograde venous drainage system. Myelopathy as a end result of intracranial dural arteriovenous fistulas draining intrathecally into spinal medullary veins. Intracranial subarachnoid hemorrhage resulting from cervical spine dural arteriovenous fistulas: literature review and case presentation. Spinal dural arteriovenous fistulas supplied by branches of the internal iliac arteries. Arteriovenous malformation of the cauda equina with arterial provide from branches of the internal iliac arteries. Successful administration of spinal dural arteriovenous fistulas undetected by arteriography. Outcome after the treatment of spinal dural arteriovenous fistulae: a contemporary single-institution sequence and meta-analysis. Surgical remedy of spinal dural arteriovenous fistulae: a consecutive collection of 154 patients. Microsurgical management of glomus spinal arteriovenous malformations: pial resection technique: medical article. Spinal glomus-type arteriovenous malformations: microsurgical remedy in 20 instances. Long-term natural history of incidentally discovered cavernous malformations in a single-center cohort. The pure historical past of conservatively managed symptomatic intramedullary spinal cord cavernomas. Use of microscopeintegrated near-infrared indocyanine green videoangiography in the surgical therapy of intramedullary cavernous malformations: report of eight circumstances. Symptomatic spinal cavernous malformations: indication for microsurgical treatment and outcome. Prognostic elements for the outcome of surgical and conservative remedy of symptomatic spinal twine cavernous malformations: a evaluate of a series of 20 patients. Intramedullary cavernous malformations: medical features and surgical technique via hemilaminectomy. Clinical presentation and surgical management of intramedullary spinal wire cavernous malformations. Preoperative coil marking to facilitate intraoperative localization of spinal dural arteriovenous fistulas. Application of indocyanine green videoangiography in surgical procedure for spinal vascular malformations. Intraoperative indocyanine green video-angiography as an help to the microsurgical remedy of spinal vascular malformations. Effectiveness of intraoperative near-infrared indocyanine green videoangiography in a case with recurrent spinal perimedullary arteriovenous fistula. The validity of intraoperative angiography for the remedy of spinal arteriovenous fistula. Comparative effectiveness analyses of intraoperative neurophysiological monitoring in spinal surgery. Editorial: Intraoperative neurophysiological monitoring and spinal deformity surgical procedure. Intraoperative neurophysiologic monitoring and neurologic outcomes in patients with epidural spine tumors. Surgery for intramedullary spinal cord tumors: the function of intraoperative (neurophysiological) monitoring. Postoperative paraplegia with preserved intraoperative somatosensory evoked potentials. Postoperative neurological deficits could occur despite unchanged intraoperative somatosensory evoked potentials. Discrepancy between provocative check and medical results following endovascular obliteration 414 3606. A cerebrovascular lesion in the setting of pregnancy presents a singular neurosurgical challenge during which the health of two patients-mother and child-is at stake. Cerebrovascular problems during being pregnant and the puerperium are rare however may be devastating to the mother and fetus. The exact incidence of cerebrovascular illness during pregnancy is unsure; estimates vary from zero. Physiologic modifications throughout being pregnant, maternal and fetal needs, and disorders distinctive to pregnancy all current particular problems to neurosurgeons managing pregnant sufferers with a cerebrovascular disorder. The diagnosis and management of cerebrovascular illness throughout pregnancy have modified dramatically for the rationale that 1990s, especially with the rising availability of endovascular techniques to deal with different lesions. New imaging technologies, higher understanding of the physiologic characteristics of being pregnant, and advances in cerebrovascular surgery have enabled neurosurgeons to better meet the wants of pregnant patients. Magnetic resonance imaging has larger sensitivity and resolution than does computed tomography. Angiography could be useful, particularly when intra-arterial thrombolytic treatment is anticipated. Helpful initial laboratory investigations embrace a whole blood cell rely, measurement of electrolytes and erythrocyte sedimentation price, coagulation studies, and urinalysis. When a cardiac source is suspected, a chest radiograph, electrocardiogram, and echocardiogram should be obtained. Transesophageal echocardiography is superior to transthoracic echocardiography and is secure for pregnant patients. Appropriate medical care, together with intravenous hydration, antibiotic therapy, and treatment of seizure issues, is important when indicated. Arterial Occlusion Arterial embolism or thrombosis accounts for 60% to 80% of circumstances of ischemic stroke throughout being pregnant. Potential interventions for arterial occlusion in pregnant women include antiplatelet agents and anticoagulation. Antiplatelet agents corresponding to aspirin have the potential to cross the placental barrier. Two main issues with endovascular remedy of stroke are problematic in regard to the pregnant patient: iodinated distinction materials and radiation exposure. When carried out by an skilled technician, the anticipated dose to the fetus may be properly under established threat thresholds throughout endovascular thrombectomy. No teratogenic effects have been reported; however, the American College of Radiology recommends that this be utilized in pregnancy only if completely needed. The most typical causes of stroke in being pregnant are arterial occlusion, venous thrombosis, and preeclampsia/ eclampsia. Venous sinus thrombosis is believed to come up as a outcome of the hypercoagulable state of pregnancy, along with alterations in cerebral vessel walls. Imaging modalities similar to computed tomography, magnetic resonance imaging, and angiography are useful. Investigation of potential predisposing factors with tests such as coagulation research is necessary.
Diseases
- Mondini dysplasia
- Temporomandibular joint dysfunction (TMJ)
- Lehman syndrome
- Ectrodactyly cardiopathy dysmorphism
- Tricho-hepato-enteric syndrome
- Cataract congenital autosomal dominant
- Tracheobronchomalacia
- Oculopharyngeal muscular dystrophy
- Tolosa Hunt syndrome
- Neurofibrillary tangles
10 mg prilosec buy with amex
Intraventricular tissue plasminogen activator for the prevention of vasospasm and hydrocephalus after aneurysmal subarachnoid hemorrhage gastritis vinegar prilosec 10 mg buy generic. Risk elements for hydrocephalus requiring external ventricular drainage in patients with intraventricular hemorrhage chronic gastritis raw vegetables prilosec 20 mg purchase mastercard. The impression of microsurgical fenestration of the lamina terminalis on shunt-dependent hydrocephalus and vasospasm after aneurysmal subarachnoid hemorrhage. Choice for the removing of bloody cerebrospinal fluid in postcoiling aneurysmal subarachnoid hemorrhage: external ventricular drainage or lumbar drainage Marked discount of cerebral vasospasm with lumbar drainage of cerebrospinal fluid after subarachnoid hemorrhage. Hydrocephalus and vasospasm after subarachnoid hemorrhage from ruptured intracranial aneurysms. Prediction of ventriculoperitoneal shunt placement based mostly on kind of failure during external ventricular drain wean. Comparison of incidence and threat components for shunt-dependent hydrocephalus in aneurysmal subarachnoid hemorrhage patients. Predictors for delayed ventriculoperitoneal shunt placement after external ventricular drain elimination in patients with subarachnoid hemorrhage. A retrospective analysis of cerebrospinal fluid drainage quantity in subarachnoid hemorrhage and the necessity for early or late ventriculoperitoneal shunt placement. Incidence, timing, and predictors of delayed shunting for hydrocephalus after aneurysmal subarachnoid hemorrhage. Does lamina terminalis fenestration cut back the incidence of persistent hydrocephalus after subarachnoid hemorrhage Independent predictors of shunt-dependent regular stress hydrocephalus after aneurysmal subarachnoid hemorrhage. Predictors of shunt dependency after aneurysmal subarachnoid hemorrhage: results of a single-center scientific trial. Incidence of ventricular shunt placement for hydrocephalus with clipping versus coiling for ruptured and unruptured cerebral aneurysms within the Nationwide Inpatient Sample database: 2002 to 2007. Chronic shunt dependent hydrocephalus after early surgery and early endovascular treatment of ruptured intracranial aneurysms. Prognostic value and determinants of ultra-early angiographic vasospasm after aneurysmal subarachnoid hemorrhage. Sustained elevated cerebral blood circulate with prophylactic hypertensive hypervolemic hemodilution (triple-H therapy) after subarachnoid hemorrhage. Relationship between the timing of aneurysm surgery and the development of delayed cerebral ischemia. Combined endovascular therapy for both intracranial aneurysm and symptomatic vasospasm. Balloon angioplasty for the remedy of vasospasm: results of the primary 50 cases. Bedside detection of brain ischemia using intracerebral microdialysis: subarachnoid 379 3256. Cognition following subarachnoid hemorrhage from anterior speaking artery aneurysm: relation to timing of surgical procedure. Education of referring doctors about sudden onset headache in subarachnoid hemorrhage. Regionalization of remedy for subarachnoid hemorrhage: a cost-utility evaluation. Relationship between the volume of craniotomies for cerebral aneurysm carried out at New York state hospitals and in-hospital mortality. Mortality charges, hospital length of stay, and the price of treating subarachnoid hemorrhage in older patients: institutional and geographical difference. In-hospital mortality and morbidity after surgical therapy of unruptured intracranial aneurysms within the United States, 1996-2000: the impact of hospital and surgeon volume. Increasing therapy of ruptured cerebral aneurysms at high-volume centers within the United States. Hospital quantity and 1-year mortality after therapy of intracranial aneurysms: a research based mostly on patient registries in Scandinavia. Impact of a devoted neurocritical care group in treating patients with aneurysmal subarachnoid hemorrhage. Participants in the International MultiDisciplinary Consensus Conference on the Critical Care Management of Subarachnoid Hemorrhage. Impact of pattern of admission on outcomes after aneurysmal subarachnoid hemorrhage. Increased fee of complications on a neurological surgical procedure service after implementation of the Accreditation Council for Graduate Medical Education workhour restriction. Three-dimensional hollow intracranial aneurysm fashions and their potential position for teaching, simulation, and coaching. Surgical approaches to complex vascular lesions: the use of digital actuality and stereoscopic evaluation as a device for resident and pupil education. Impact of age on 30-day postoperative end result of surgery for ruptured and unruptured intracranial aneurysms. Age-related trends within the remedy and outcomes of ruptured cerebral aneurysms: a study of the nationwide inpatient pattern 2001-2009. Effect of age on outcomes of treatment of unruptured cerebral aneurysms: a examine of the National Inpatient Sample 2001-2008. Comparison of longterm outcomes associated with endovascular remedy versus surgical remedy amongst Medicare beneficiaries with unruptured intracranial aneurysms. Age-related complications following endovascular remedy of unruptured intracranial aneurysms. Endovascular therapy for ruptured cerebral aneurysms in the aged: poor accessibility of the guiding catheter and use of local anesthesia as the predictors of procedure-related rupture. Elderly patients with intracranial aneurysms have larger high quality of life after coil embolization: a decision evaluation. Elective surgery for asymptomatic, unruptured, intracranial aneurysms: a cost-effctiveness evaluation. Age limit for surgical treatment of poor-grade patients with subarachnoid hemorrhage: a project of the Chugoku-Shikoku division of the Japan Neurosurgical Society. Critical age affecting 1-year practical end result in elderly patients aged 70 years with aneurysmal subarachnoid hemorrhage. Intracranial arterial aneurysms: consideration on the higher age limit for surgical remedy. Management and long-term end result following subarchnoid haemorrhage and intracranial aneurysm surgical procedure in elderly patients: an audit of 199 consecutive cases. A simple scoring system for correct prediction of end result inside four days of a subarachnoid hemorrhage.
Prilosec 10 mg buy free shipping
The bone flap ought to be centered roughly 6 to 7 cm above the external auditory meatus gastritis burning stomach prilosec 20 mg generic without prescription. An different mathematical method to the perfect location of a recipient vessel could permit for a more localized craniotomy gastritis diet for toddlers generic prilosec 40 mg online. At this level, the dura is opened in a cruciate method, and care is taken not to disturb or injure the naturally developed transdural collateral vessels. Furthermore, within the event that the middle meningeal artery is providing significant dural collateral vessels to the mind, the incision is modified in order to protect the center meningeal artery. Under the working microscope and utilizing microsurgical approach, the surgeon inspects the brain surface for a suitable recipient M4 branch. The recipient vessel is then isolated, and any small cortical branches are coagulated and divided. Background material is then placed behind this vessel, and a small malleable microsuction gadget is placed beneath the background materials, thus offering steady suction and a dry operative subject. This will guarantee the power to maneuver the vessel backwards and forwards through the anastomosis and facilitate the suturing. The reduce finish is then trimmed of any remaining adventitial tissue and "fishmouthed" to a measurement 2. Alternatively, a small portion of vessel wall can be reduce away with microscissors, though this will likely end in a narrower anastomosis. We favor the former technique and then expand the opening through the use of microscissors. The corners are anchored, after which interrupted sutures are positioned evenly spaced apart, or the again wall is run from one corner suture to the other. Again, the area should be rigorously inspected to ensure appropriate placement of the sutures. After the suturing however earlier than the final suture is accomplished, the vessels are flushed with heparinized saline. Once the anastomosis is accomplished, the realm is carefully inspected; the surgeon ensures move by using either a Doppler probe or a flow probe. Alternatively, carefully milking the realm between two forceps and alternating release of one forceps and then the other will point out adequacy of the anastomosis. The cut circulate is measured after the vessel has been reduce, which thereby removes the downstream resistance. If the recipient vascular mattress is hemodynamically compromised, resistance ought to be low, and, ideally, the cut flow and bypass flow shall be related. AminHanjani and colleagues47 defined this phenomenon by the "cut move index": the ratio of the cut flow to the bypass flow. Some authors have also described intracranial endarterectomies to treat significant stenosis. A, the anchoring sutures being positioned at the corners of the arteriotomy and donor vessel. A layer of Gelfoam is positioned over the dura, and the bone flap is replaced with miniplates and screws. One hundred eighteen sufferers have been excluded from the examine because the referring physicians believed that the sufferers would benefit extra greatly from surgical intervention. Of the remaining 1377 patients, 714 had been randomly assigned to undergo medical therapy, and 663 to bear surgical revascularization; the mean follow-up interval was 55. The reported rates of stroke had been 18% among sufferers receiving medical management and 20% among the surgically handled patients. Nonfatal and deadly stroke occurred each more frequently and earlier in the sufferers operated on. Secondary survival analyses evaluating the two teams for main strokes and all deaths, for all strokes and all deaths, and for ipsilateral ischemic strokes demonstrated a similar lack of benefit from surgery. Many sufferers in the research had very minor symptoms, and no evaluation of hemodynamic function was obtainable. Selection biases clearly affected affected person choice, inasmuch as 118 patients were excluded from the examine, and neither radiographic nor medical perfusion was assessed. Postoperative complications- including an infection, scalp necrosis, hemorrhages, cerebrospinal fluid leak, seizures, and ischemic events-were reported in 11% to 26% of cases. Patency of bypass vessels has been reported as high as 90% to 91%, though several ischemic occasions had been nonetheless noticed in sufferers with patent vessels. Ninety-eight sufferers had been included in every category and had had an ischemic occasion inside three months of enrollment. At 2 years of follow-up, the outcomes with regard to each finish factors of death and recurrent ischemic events have been extra favorable with surgical therapy (P =. Conversely, the 30-day risk of stroke was greater within the patients who underwent surgery (14. In order to additional enhance recruitment, the initially stringent standards concerning surgeon experience had been loosened. Despite the clearly planned inclusion standards, the hemodynamic testing results have been what ultimately decided eligibility. These critiques have prompted further examine to identify sufferers who will best profit from microsurgical revascularization. Surgeons have obtained some data of the natural historical past of the disease, and even with current medical therapies, the danger of severe stenosis and hemodynamic compromise is significant. Determining the optimum combos of medical therapies must be additional evaluated, but adjuvant options for patients at larger threat are additionally a necessity. As medical, endovascular, and surgical methods all continue to enhance, rigorous examine must be ongoing. The Greater Cincinnati/Northern Kentucky Stroke Study: preliminary first-ever and complete incidence charges of stroke amongst blacks. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. Chinese-white differences within the distribution of occlusive cerebrovascular illness. Race-ethnicity and determinants of intracranial atherosclerotic cerebral infarction. Importance of intracranial atherosclerotic disease in patients with symptomatic stenosis of the inner carotid artery. Natural history of stenosis from intracranial atherosclerosis by serial angiography. Gender variations in outcomes among patients with symptomatic intracranial arterial stenosis. Effect of continual middle cerebral artery stenosis on the local cerebral hemodynamics.
Order 40 mg prilosec amex
If a surgical strategy is decided to be optimum for the affected person gastritis diet juice buy prilosec 20 mg cheap, monumental concentration should be targeted on every detail of the operation gastritis gas discount prilosec 40 mg online, as a result of the margin for error is nonexistent. The surgeon must be experienced, relaxed, and psychologically prepared for surprising problems of anatomy or intraoperative rupture. During times of temporary arterial occlusion, the surgeon should transfer quickly and thoughtfully to decrease the ischemic threat. In the current period, surgical teams must be in a position to slip in and out of these slim confines, leaving only a clip or two as proof that the areas have been violated. Causes of morbidity and mortality from surgery of aneurysms of the distal basilar artery. Bleeding aneurysms of the basilar artery: direct surgical administration in four cases. Surgical clipping of advanced basilar apex aneurysms: a strategy for successful end result utilizing the pretemporal transzygomatic transcavernous method. Basilar apex aneurysms: surgical outcomes and perspectives from an preliminary expertise. Ligation of the vertebral (unilateral or bilateral) or basilar artery in the remedy of large intracranial aneurysms. Advances within the neurosurgical remedy of aneurysms, arteriovenous malformations, and hematomas of the vertebral circulation. The use of extracorporeal circulation and profound hypothermia in the remedy of ruptured intracranial aneurysm. Giant fusiform intracranial aneurysms: evaluation of a hundred and twenty sufferers handled surgically from 1965 to 1992. A Comprehensive Reference Guide to the Diagnosis and Management of Neurosurgical Problems. Microsurgical treatment of basilar apex aneurysms: perioperative and long-term clinical consequence. Partial anterior petrosectomies for higher basilar artery trunk aneurysms: a cadaveric and clinical study. A mixed trans-sylvian and subtemporal strategy for basilar bifurcation aneurysms. Combined transsylviansubtemporal publicity of cerebral aneurysms involving the basilar apex. The carotid-oculomotor window in exposure of higher basilar artery aneurysms: a cadaveric morphometric examine. Anatomical research of the orbitozygomatic transsellar-transcavernous-transclinoidal approach to the basilar artery bifurcation. Mobilization of the transcavernous oculomotornerve throughout basilar aneurysm surgical procedure: biomechanical bases for better end result. Role of uncal resection in optimizing transsylvian access to the basilar apex: cadaveric investigation and preliminary clinical expertise in eight sufferers. Early treatment of ruptured aneurysms with Guglielmi removable coils: effect on subsequent bleeding. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and scientific consequence in 403 patients. Endovascular treatment of acutely ruptured and unruptured aneurysms of the basilar bifurcation. Intracranial aneurysms treated with the Guglielmi removable coil: midterm medical ends in a consecutive collection of one hundred patients. Albuquerque As with most kinds of technology-heavy fields, the specialty of endovascular neurosurgery has seen an amazing quantity of progress and refinement with the inexorable march of progress. The earlier introduction of balloon- and stent-assisted coiling and the current availability of flow-diverting stents have helped usher on this new period of growth. Furthermore, the natural historical past and threat of rupture must be weighed in opposition to the safety of the proposed remedy in addition to the medical condition and life expectancy of the affected person. In basic, incidental cerebral aneurysms are treated extra aggressively in youthful than in older patients. Likewise, larger aneurysms and aneurysms positioned in the posterior circulation are most likely to be handled more usually than smaller, anterior circulation lesions. An exhaustive discussion of this complicated decision-making process is past the scope of this chapter. Aneurysms located on or around the circle of Willis were the first lesions treated successfully with endovascular techniques. Detachable balloons were previously flow-directed down the vessels until the goal lesion was reached. Guglielmi and associates7,8 initially described a small neck diameter as a potential think about determining completeness of aneurysm occlusion utilizing the Guglielmi removable coil. They described their sequence of 43 posterior circulation aneurysms in forty two patients treated with their removable coil. Of these forty two aneurysms, sixteen had neck diameters lower than 4 mm, and 26 had neck diameters of 4 mm or extra. The investigators achieved complete occlusions in 13 of the 16 narrow-necked aneurysms but in only four of the 26 wide-necked aneurysms. They hypothesized that a the smaller neck diameter allowed for a extra dense packing of coils and better transforming of the neck of the aneurysm. The identical group followed up this initial multicenter retrospective evaluate with a retrospective single-center examine specifically addressing neck diameter as a determinant of aneurysm occlusion. Using published measurements of the diameters of the reference vessels, the investigators were able to correct for image magnification to calculate the "actual" neck diameters of the aneurysms of their sequence. Complete aneurysm occlusion was noted in 17 of 20 (85%) narrow-necked aneurysms, in contrast with solely eight of 51 (15. A three-dimensional rotational angiogram demonstrates a neck diameter less than 4 mm (short arrow), a dome diameter larger than 8 mm (long arrow), and a dome-to-neck ratio higher than 2: 1. Overall medical and radiographic outcomes were better in the second cohort (Group 2), during which aneurysms had been chosen for coiling on the basis of their dome-to-neck ratio and neck diameter, than within the initial 25 patients (Group 1). Two sufferers (8%) in Group 1 experienced permanent neurological complications instantly related to aneurysm coiling. In Group 2, there were no deaths and only 1 case (1%) of a everlasting neurological deficit associated to aneurysm coiling. Aneurysm occlusion rates had been reportedly 72% with ruptured and 80% with unruptured aneurysms that have been chosen on the premise of favorable angiomorphologic traits but only 53% for aneurysms with dome-to-neck ratios lower than 2: 1. Since the study, these findings have served as a foundation for the selection of cerebral aneurysms for main coil embolization. Generally, most interventional procedures can be performed with patients underneath aware sedation or general anesthesia according to the preferences of the endovascular neurosurgeon. With use of acutely aware sedation, real-time neurological assessments may be made, as essential, to ensure the security of the patient during the procedure. Performing interventions on this manner requires the patient to remain nonetheless and cooperative all through the process, which may be tough in certain situations.
HP 200 (Cowhage). Prilosec.
- Are there safety concerns?
- Are there any interactions with medications?
- How does Cowhage work?
- Dosing considerations for Cowhage.
- What is Cowhage?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96981
20 mg prilosec discount visa
Safety and efficacy of intraoperative angiography in craniotomies for cerebral aneurysms and arteriovenous malformations: a evaluation of 1093 consecutive cases gastritis lasting weeks generic prilosec 20 mg fast delivery. Is routine intraoperative angiography in the surgical treatment of cerebral aneurysms justified Intraoperative computed tomography angiography with computed tomography perfusion imaging in vascular neurosurgery: feasibility of a new idea symptoms of gastritis and duodenitis safe 20 mg prilosec. Intraoperative computed tomography with built-in navigation system in a multidisciplinary working suite. Intraoperative magnetic resonance imaging findings during deep brain stimulation surgical procedure. The new technology polestar n20 for typical neurosurgical operating rooms: a preliminary report. Loftus Ischemic stroke remains a leading reason for demise and disability within the developed world. This chapter focuses on the pure historical past and optimum medical management of carotid occlusive illness. The manifestations of an infarction on this vast arterial territory are additionally extremely variable, however most frequently embrace contralateral weakness and hemisensory loss. Whereas varied iterations of aphasia are associated with lesions of the dominant hemisphere, hemineglect and apraxic syndromes are related to ischemia of the nondominant middle cerebral artery. The anterior choroidal artery supplies the posterior limb of the internal capsule, the posterolateral thalamus, and the lateral geniculate body, infarctions of which current clinically as the triad of contralateral hemiparesis, hemisensory loss, and hemianopsia. The traditional deficit in posterior cerebral artery infarctions is a contralateral visual field reduce, but the presentation of posterior cerebral artery territory infarcts is, once more, extremely variable. Miller Fisher described the connection between carotid occlusive disease and stroke. Atherosclerosis is a disease of the arterial intima that causes progressive narrowing of the vessel lumen. Lipids are deposited or taken up by monocytes or macrophages, most notably by lowdensity lipoproteins. Lipid-laden macrophages, or foam cells, continue to accumulate, as do numerous connective tissue elements and clean muscle cells. Inflammatory cells additionally play a job in the development of atherosclerotic plaque as oxidative stress and free radical production additional injury the endothelium. Two further studies evaluated the correlation between cerebral angiographic findings and carotid bruits, reported that the predictive value of carotid bruit for ipsilateral extracranial carotid atherosclerosis was approximately 75%, and quoted the false-positive price to be 10%. Asymptomatic patients with carotid artery stenosis of lower than 75% are counseled that their annual stroke threat is approximately 1%. In a potential study of 339 sufferers utilizing serial Doppler examinations with a median follow-up of 29 months, 2% of patients with 50% to 80% carotid stenosis, 8. Furthermore, neither of those research managed for the use of platelet antiaggregants, and each excluded patients who underwent carotid artery surgery. Both research also reported on symptomatic patients with contralateral asymptomatic carotid stenosis. Although it has been tough to show conclusively that tight control of serum glucose levels reduces the danger of stroke, it undoubtedly reduces the incidence of different microvascular complications of diabetes, and consensus among authorities is that serum glucose ranges lower than 126 mg/dL are optimal. Aspirin works by irreversibly inhibiting platelet cyclooxygenase, which prevents the formation of thromboxane A2, each a potent vasoconstrictor and an inducer of platelet aggregation. In healthy people, a single aspirin ends in a 98% inhibition of thromboxane A2 manufacturing inside 1 hour of ingestion. Several massive, randomized controlled medical trials have found aspirin to be useful within the secondary prevention of cardiovascular occasions and dying. Studies exhibiting its effectiveness within the secondary prevention of stroke have used doses ranging from 30 to 1500 mg/day. Some authors have advocated higher doses of aspirin, on condition that these doses can have useful results unrelated to cyclooxygenase inhibition. The primary finish factors in the Aspirin in Carotid Endarterectomy trial were stroke, myocardial infarction, and death. Three months after surgery, the danger of stroke, myocardial infarction, or death was 6. Although it has not been studied specifically in patients with carotid atherosclerosis, it has been proven to reduce the danger of stroke, myocardial infarction, and vascular demise in sufferers with current non-cardioembolic stroke, and it has been demonstrated to reduce the relative threat of demise or nonfatal stroke by 12% compared with aspirin. Despite its proven advantages in decreasing the incidence of stroke, its aspect effect profile, significantly its significant hematologic unwanted aspect effects that embrace reversible neutropenia and thrombotic thrombocytopenic purpura, limits its widespread implementation. In a study enrolling more than 19,000 patients with atherosclerotic vascular disease manifesting as an ischemic stroke, a latest myocardial infarction, or symptomatic peripheral arterial disease, clopidogrel (75 mg/day) was discovered to be more practical than 325 mg of aspirin in decreasing the danger of ischemic stroke, myocardial infarction, and vascular death. In the group of more than 6400 sufferers who entered the research having skilled a stroke, there was a relative threat reduction of seven. In distinction to ticlopidine, the aspect effect profile of clopidogrel is comparatively benign. Dipyridamole is a phosphodiesterase inhibitor that increases the levels of intracellular cyclic adenosine monophosphate. The stroke price decreased in the combined treatment arm in contrast with both agent alone. Both low-dose aspirin and high-dose dipyridamole in a modified launch kind alone were associated with better outcomes than the placebo was. Combinations of platelet antiaggregant remedy (aspirin plus ticlopidine or aspirin plus clopidogrel) are additionally utilized by clinicians, however no evidence-based data have demonstrated their profit over single agents alone in preventing ischemic stroke generally or in carotid occlusive disease particularly. Warfarin has also been used in the main and secondary prevention of stroke in patients with nonvalvular atrial fibrillation. Trials comparing warfarin to aspirin within the secondary prevention of non-cardioembolic stroke are ongoing. When out there, these information may help to define the usefulness of warfarin in treating carotid occlusive disease. The procedure has been validated by multicenter, randomized, potential scientific trials across at least two generations of carotid surgeons as superior to medical management alone for symptomatic sufferers with higher than 50% carotid stenosis and for asymptomatic patients with larger than 60% carotid stenosis. Risk elements related to cerebrovascular recurrence in symptomatic carotid illness: a comparative study of carotid plaque morphology, microemboli assessment and the European carotid surgical procedure trial threat mannequin. Prevalence of asymptomatic carotid illness: outcomes of duplex scanning in 348 unselected volunteers. Risk of stroke in asymptomatic persons with cervical arterial bruits: a inhabitants study in Evans County, Georgia. Correlation of bruits over the carotid artery with angiographically demonstrated lesions. The threat of stroke within the territory of an asymptomatic stenosed extracranial internal carotid artery: degree of stenosis, intermittent claudication and silent cerebral infarction as predictors of stroke. Prevention of a primary stroke: a evaluate of tips and a multidisciplinary consensus assertion from the National Stroke Association. Short-term reductions in blood strain: overview of randomised drug trials of their epidemiological context. Prevention of stroke by antihypertensive drug remedy in older individuals with isolated systolic hypertension. Predictors of carotid stenosis in older adults with and with out isolated systolic hypertension.
Cheap prilosec 20 mg otc
They are fragile and can rupture during microsurgery gastritis diet plan foods buy prilosec 40 mg online, causing postoperative rebleeding more incessantly than do saccular aneurysms gastritis not eating 10 mg prilosec for sale. The prognosis of those uncommon aneurysms is essential earlier than surgery because the technique for clipping or other therapy is completely different than that for saccular aneurysms. New endovascular options such as circulate diverters have has proven reasonable ends in few patients, however their efficacy has not been validated in bigger sequence. Testing the competency of collateral move must be a part of the preoperative planning and determination making. Application of an encircling clip is another methodology that has limits due to the chance that the perforating vessel could need to be sacrificed. Up to 28% of patients require a second therapeutic intervention to safe the aneurysm. Wrapping the aneurysm is another alternative; nonetheless, due to the fragility and likelihood of further aneurysm progress, the success rate after wrapping alone is low. The most necessary level in the administration of those aneurysms is thorough preoperative analysis and planning for each possible scenario in order to avoid hemorrhagic and ischemic complications. Axel Perneczky advocated the keyhole strategy within the 1980s, the goal being to make the minimal craniotomy wanted to access deep-seated lesions. The supraorbital/keyhole craniotomy has been broadly studied in cadaveric collection and case series reports have proven its advantages and disadvantages, particularly as compared with open procedures. This technique permits for a wider operative subject at depth at the price of a smaller working angle; that is key for affected person choice for this operation. With less dissection of the temporalis muscle, a smaller opening within the bone, and minimal brain manipulation, it makes for a sooner, much less painful recovery. This technique can be useful for treating a extensive range of tumors within the anterior skull base; the optic, suprasellar, and parasellar areas; and the temporal and frontal lobes. In addition, in this period of endovascular treatment of nearly all of aneurysms, those encountered by the neurosurgeon are of the complex varieties: multilobulated aneurysm, giant aneurysm, fusiform aneurysm with poor dome-to-neck ratio, or aneurysm in arterial branches originating from the neck or physique. The selection of craniotomy ought to be primarily based on the expertise of the surgical group and the familiarity with a given approach. With good patient selection, the rates of morbidity and mortality of this method are roughly the same as these for more open techniques. The mixed price of morbidity and mortality associated with intraoperative rupture is as high as 30% to 35%. The kind of reaction to the intraoperative rupture is set by when it happens. Proximal management is crucial, and the surgeon should have the flexibility to apply a temporary clip on the mother or father vessel earlier than coping with the aneurysm. If the rupture occurs earlier than exposure of the aneurysm, two large-bore suctions ought to be within the wound instantly: one on the outlet of the aneurysm (with the help of cotton patties if the surgeon prefers) to assist visualize the proximal vessel, which is then short-term clipped, and another short-term clip may be applied to the distal vessel. The dissection is then accomplished with the affected person in a situation of high blood pressure to cut back the ischemic insult. If the rupture occurs after the dissection of the neck of the aneurysm is accomplished, then with correct suctioning, the clip may be applied directly throughout the neck of the aneurysm. Radiologic and post-mortem series counsel that the incidence of infundibulum is 6% to 16% and increases with age. Special Consideration: Minimally Invasive Surgery Advances in open surgery have been primarily in the improvement of minimally invasive craniotomies, which can be utilized to deal with all kinds of aneurysms. They embody the mini� pterional craniotomy, the lateral supraorbital craniotomy, and the orbital pterional craniotomy. These exposures have the benefit of smaller and more cosmetic incisions, smaller craniotomies, and minimal mind exposure. They also decrease problems related to temporal muscle dissection and removing of the zygomatic arch. Therefore, one of the best strategy is probably to return to use of temporary clips and reassess the standard of clipping. Preoperative planning for managing an intraoperative rupture is the one approach to ensure a stepwise method to this complication. Again, use of Doppler imaging or intraoperative angiography can verify the patency of the mother or father vessel if deemed needed. Underestimation of angiographic options of related conditions such as extreme atherosclerosis might end in difficulties with short-term clipping. Vigilant perioperative and postoperative care of these critically unwell patients is obligatory to ensure good outcomes. Paralleling the developments in endovascular remedy options is the advance in surgical methods, including minimally invasive approaches, better know-how, and better equipment. Although most aneurysms are nonetheless handled handled in an endovascular method, an elevated armamentarium is available to the surgeon for the treatment of huge and sophisticated aneurysms. Does therapy modality of intracranial ruptured aneurysms affect the incidence of cerebral vasospasm and medical end result Shunt-dependent hydrocephalus after rupture of intracranial aneurysms: a prospective research of the affect of treatment modality. Orbital pain and unruptured carotid�posterior communicating artery aneurysms: the function of sensory fibers of the third cranial nerve. Symptomatic vasospasm and outcomes following aneurysmal subarachnoid hemorrhage: a comparison between surgical repair and endovascular coil occlusion. A universal subarachnoid hemorrhage scale: report of a committee of the World Federation of Neurosurgical Societies. Surgery: Specific Sites and Results of Series in Aneurysms Affecting the Nervous System. Multislice computerized tomography angiography within the analysis of intracranial aneurysms: a comparability with intraarterial digital subtraction angiography. Therapeutic determination and administration of aneurysmal subarachnoid haemorrhage based on computed tomographic angiography. Experience and end result with postmortem cerebral angiography performed as routine procedure of the post-mortem. Unruptured intracranial aneurysms: pure history, scientific outcome, and risks of surgical and endovascular therapy. Morphological and clinical danger factors for posterior communicating artery aneurysm rupture. Recovery of third nerve palsy after endovascular remedy of posterior communicating artery aneurysms. Intraoperative angiography in cerebral aneurysm surgery: A potential study of a hundred craniotomies. Preoperative predictive value of the necessity for anterior clinoidectomy in posterior communicating artery aneurysm clipping. Microsurgical anatomy of the cisternal anterior choroidal artery with special emphasis on the preoptic and postoptic subdivisions. Surgical treatment of 127 anterior choroidal artery aneurysms: a cohort study of resultant ischemic issues. The keyhole idea in aneurysm surgery-a comparative examine: keyhole versus normal craniotomy. The A4 and A5 segments run over the physique of the corpus callosum, with the transition between the 2 segments delineated arbitrarily at the level of the coronal suture.

Prilosec 20 mg buy fast delivery
Additionally gastritis diet or exercise prilosec 10 mg discount otc, their use has compared very favorably to stent-assisted coil embolization of cerebral aneurysms in some stories gastritis diet ����� purchase 20 mg prilosec. Given these outcomes, these investigators judged that the indications for use of flow-diverting stents could probably be expanded to embody a wider vary of cerebral aneurysms. These types of stories will invariably affect how flowdiverting stents are used sooner or later. If long-term studies bear out the benefits in efficacy, safety, or costs with flow-diverting expertise, the indications for its use will proceed to broaden to a bigger subset of cerebral aneurysms. Fortunately, the rate of hemorrhage after initial coil embolization of aneurysms is reportedly fairly low, at 0. This situation forces predominant reliance on data obtained from the remedy of a more heterogenous and sure more complicated group of aneurysms as a baseline. When confronted with an aneurysm recurrence, the surgeon should initially resolve whether or not the aneurysm is giant enough to be a candidate for re-treatment. Then he or she must weigh the attendant risks of re-treatment in opposition to the perceived threat of aneurysm rupture. Given related rates of major aneurysm recurrences, North American centers had a better price of re-treatment (21% in ruptured aneurysms, 10. Angiographic outcomes are the subject of much scrutiny because of the belief that complete occlusion of an aneurysm mitigates the chance of hemorrhage. Unfortunately, recurrences and/or rehemorrhages can happen in aneurysms that have been originally thought to be utterly occluded. Primary coil embolization stays the preferred technique of endovascular treatment of these aneurysms and is the muse on which extra difficult therapies are primarily based. Selection of cerebral aneurysms for remedy utilizing Guglielmi removable coils: the preliminary University of Illinois at Chicago experience. Endovascular treatment of posterior circulation aneurysms by electrothrombosis using electrically detachable coils. Intravascular stent and endovascular coil placement for a ruptured fusiform aneurysm of the basilar artery. Natural history of unruptured intracranial aneurysms: Probability of and danger factors for aneurysm rupture. Endovascular occlusion of intracranial aneurysms with Guglielmi removable coils: Correlation between coil packing density and coil compaction. Lifelong rupture threat of intracranial aneurysms depends on risk factors: A potential finnish cohort study. Cerecyte coil trial: Angiographic outcomes of a prospective randomized trial evaluating endovascular coiling of cerebral aneurysms with either Cerecyte or bare platinum coils. Balloon-assisted coil embolization of intracranial aneurysms: incidence, issues, and angiography outcomes. Unruptured intracranial aneurysms: threat of rupture and dangers of surgical intervention. Endovascular treatment of fusiform aneurysms with stents and coils: technical feasibility in a swine model. Curative cerebrovascular reconstruction with the Pipeline Embolization Device: the emergence of definitive endovascular therapy for intracranial aneurysms. International subarachnoid aneurysm trial 2009: endovascular coiling of ruptured intracranial aneurysms has no important advantage over neurosurgical clipping. Length of keep and total hospital expenses of clipping versus coiling for ruptured and unruptured adult cerebral aneurysms within the Nationwide Inpatient Sample database 2002 to 2006. Impact of International Subarachnoid Aneurysm Trial outcomes on therapy of ruptured intracranial aneurysms in the United States. Geographic variation and regional developments in adoption of endovascular strategies for cerebral aneurysms. Lifelong rupture threat of intracranial aneurysms is dependent upon threat components: a potential Finnish cohort study. Risk of rupture of small anterior communicating artery aneurysms is similar to posterior circulation aneurysms. Aneurysm geometry: an important criterion in choosing sufferers for Guglielmi removable coiling. Safety and efficacy of balloon remodeling approach during endovascular treatment of intracranial 391 3371. Use of the Outreach distal entry catheter as an intracranial platform facilitates coil embolization of select intracranial aneurysms: technical notice. Balloon assistance as a routine adjunct to the endovascular therapy of cerebral aneurysms. Use of the Ascent balloon for a 2-in-1 reworking technique: feasibility and preliminary expertise: case report. HyperForm remodelingballoon for endovascular treatment of wide-neck intracranial aneurysms. Balloon remodeling of complicated anterior communicating artery aneurysms: technical issues and complications. Angles between A1 and A2 segments of the anterior cerebral artery visualized by threedimensional computed tomographic angiography and affiliation of anterior communicating artery aneurysms. Impact of anatomical variations of the circle of Willis on the incidence of aneurysms and their recurrence rate following endovascular therapy. Endovascular treatment of difficult ruptured anterior speaking artery aneurysms based on the anatomical options of the anterior speaking artery advanced. Feasibility and limitations of endovascular coil embolization of anterior communicating artery aneurysms: morphological concerns. Endovascular coiling as the primary treatment strategy for ruptured pericallosal artery aneurysms: outcomes, problems, and follow up. The affect of configuration and site of ruptured distal cerebral anterior artery aneurysms on their treatment modality and outcomes: evaluation of our casuistry and literature evaluate. Endovascular therapy of ophthalmic artery aneurysms: assessing balloon check occlusion and preservation of vision in coil embolization. Branch retinal artery occlusion after coil embolization of a paraclinoid aneurysm. Temporary balloon occlusion to check adequacy of collateral circulate to the retina and tolerance for endovascular aneurysmal coiling. Retinal artery occlusion following coil embolization of carotid-ophthalmic aneurysms. Clinical and anatomic outcomes after endovascular coiling of center cerebral artery aneurysms: report on 30 treated aneurysms and evaluation of the literature. Endovascular remedy with naked platinum coils for center cerebral artery aneurysms.
Buy prilosec 10 mg online
In many circumstances gastritis diet ideas proven 40 mg prilosec, a relatively excessive upfront danger is suitable if the following surgical risks are decreased and long-term treatment is feasible gastritis symptoms mayo purchase prilosec 10 mg without prescription. Rapid development in endovascular know-how has enabled interventionalists to specifically target distinctive angioarchitectural options that pose the greatest threat throughout either surgery or the radiosurgery latency interval. A population-based research of brain arteriovenous malformation: long-term therapy outcomes. The effect of embolization with n-butyl cyanoacrylate prior to surgical resection of cerebral arteriovenous malformations. A prospective, multicenter, randomized trial of the Onyx liquid embolic system and n-butyl cyanoacrylate embolization of cerebral arteriovenous malformations. The natural historical past of symptomatic arteriovenous malformations of the brain: a 24-year follow-up assessment. Concurrent arterial aneurysms in brain arteriovenous malformations with haemorrhagic presentation. Comparison of n-butyl cyanoacrylate and Onyx for the embolization of intracranial arteriovenous malformations: evaluation of fluoroscopy and procedure instances. Incidence and prevalence of intracranial vascular malformations in Olmsted County, Minnesota, 1965 to 1992. A systematic review of the frequency and prognosis of arteriovenous malformations of the brain in adults. Morbidity of intracranial hemorrhage in sufferers with cerebral arteriovenous malformation. Tumors Arising from the Blood-Vessels of the Brain; Angiomatous Malformations and Hemangioblastomas. The fantasy of the Brooks methodology of embolization: a quick historical past of the endovascular treatment of carotidcavernous sinus fistula. Calibrated leak balloon microcatheter: a tool for arterial exploration and occlusive therapy. Surgery for unruptured arteriovenous malformations of the brain is best than conservative management for chosen instances: a prospective cohort study. The failure of preoperative ethylene-vinyl alcohol copolymer embolization to improve outcomes in arteriovenous malformation administration: case collection. Complications of contemporary diagnostic cerebral angiography in an educational medical middle. The relationship of coexisting extranidal aneurysms to intracranial hemorrhage in sufferers harboring brain arteriovenous malformations. Characteristics of arteriovenous malformations related to cerebral aneurysms. The natural historical past and predictive features of hemorrhage from brain arteriovenous malformations. Cerebral arteriovenous malformations and related aneurysms: analysis of 305 circumstances from a series of 662 sufferers. The influence of hemodynamic and anatomic components on hemorrhage from cerebral arteriovenous malformations. Factors associated with intracranial hemorrhage in cases of cerebral arteriovenous malformation. Large and deep brain arteriovenous malformations are related to threat of future hemorrhage. Features predictive of brain arteriovenous malformation hemorrhage: extrapolation to a physiologic model. Angioarchitectural traits of mind arteriovenous malformations with and with out hemorrhage. A supplementary grading scale for choosing patients with brain arteriovenous malformations for surgery. Angioarchitecture determines obliteration fee after radiosurgery in mind arteriovenous malformations. Angiographic options help predict end result after stereotactic radiosurgery for the treatment of pediatric arteriovenous malformations. Endovascular therapy of intracranial arteriovenous malformations with Onyx: technical features. Comparison of nbutyl cyanoacrylate and Onyx for the embolization of intracranial arteriovenous malformations: evaluation of fluoroscopy and procedure occasions. Embolization of cerebral arteriovenous malformations achieved with polyvinyl alcohol particles: angiographic reappearance and issues. Surgical embolization of cerebral arteriovenous malformations via inner carotid and vertebral arteries. Catheter embolization of intracranial arteriovenous malformations as an assist to surgical excision. Adjuvant embolization with n-butyl cyanoacrylate within the treatment of cerebral arteriovenous malformations: outcomes, problems, and predictors of neurologic deficits. Stereotactic radiosurgery for arteriovenous malformations after embolization: a casecontrol examine. Long-term results of gamma knife surgery for partially embolized arteriovenous malformations. Hemorrhagic complications after endovascular treatment of cerebral arteriovenous malformations. The most typical manifestation in patients with this lesion is hemorrhage, adopted by seizures and, less often, focal neurological deficits. The consequence of a hemorrhage is important: dying in 6% to 29% of circumstances and permanent morbidity in 16% to 35%. The most typical and universally accepted administration technique is a mix of modalities with the objectives of stopping additional bleeding, controlling seizures, and preventing the progression of neurological deficits. Although individual case series elucidate particular administration methods, considerable controversy exists over which intervention is finest for a given patient. The investigators discovered that the rate of the first consequence (death or sustained morbidity) was worse among the intervention recipients at 4 years but equal in the two groups after 4 years. This examine is weakened predominantly by its design as a nonrandomized, observational cohort research. A remedy plan ought to be decided by a multidisciplinary team that features a neurologist, a neurointerventionalist, a radiation oncologist, and a cerebrovascular neurosurgeon. In the majority of cases, endovascular embolization is the first-line therapy with the objective of lowering the dimensions of the nidus or the variety of arterial feeders, or each, in anticipation of finishing remedy with microsurgical resection or, if the lesion is sufficiently small, stereotactic radiosurgery. The role of endovascular embolization, however, has been expanding because of increasing evidence that embolization as monotherapy-facilitated by the event of better embolic agents, catheters, and techniques- may be healing in patients with sure lesion traits. The investigators concluded that the chance of stroke or demise was lower within the sufferers who obtained solely medical management (10. Of importance is that the vast majority of patients who received intervention underwent embolization or radiosurgery, each of which had lower obliteration charges than did surgical resection. Sahlein and associates11 reiterated these targets and emphasized that acknowledging the intent of the endovascular procedure a priori is essential for evaluating its efficacy. Andrade-Souza and colleagues12 in 2007 demonstrated that radiosurgery after embolization is less effective than initially hypothesized. They found that nidus obliteration was achieved in 22 (47%) of the patients who underwent preoperative embolization, whereas obliteration was achieved in 33 (70%) of the patients who had not undergone embolization.
Prilosec 40 mg generic mastercard
Central hemorrhagic merchandise are surrounded by a partial hemosiderin rim gastritis or morning sickness prilosec 20 mg generic online, and an associated developmental venous anomaly is also famous (arrow) gastritis in children generic 40 mg prilosec mastercard. The answer at present is unknown, and any theories will ultimately be proved or disproved by histochemical analysis. Garner and coworkers reported one such patient,59 and Awad and coworkers reported three. Mullan and colleagues reviewed 4 such sufferers and discussed the pathophysiology in the context of embryologic improvement of the cerebral venous system. This discovering may point out that some sufferers have legitimate hypertension and disruption of the blood-brain barrier,56 which is indicated against this enhancement. Recognition of familial clustering in a subset of sufferers with cerebrovascular malformations has led to linkage evaluation studies investigating the underlying genetic foundation for these lesions. This suggests that a genetic defect underlies a minimal of some vascular malformations. In addition to enhancing presymptomatic screening, identification of the genes accountable might lead to better understanding of the pathogenesis of these lesions and, finally, in novel remedies. Nasal, mucocutaneous, pulmonary, cerebral, gastrointestinal, and hepatic vascular beds are mostly affected. E, Funduscopy exhibits multiple dilated and tortuous retinal vessels, findings confirming the analysis of Wyburn-Mason syndrome. Knockout mice lacking endoglin die during gestation as a result of defective vascular growth, suggesting that endoglin is important for vascular growth. No mutant endoglin was expressed on the cell surface, however somewhat it was discovered solely as an intracellular homodimer. They exhibit vascular abnormalities, together with hyperdilation of vessels and abnormal fusion of capillary structures. Isolated familial predisposition within the absence of an angiodysplastic syndrome is exceedingly rare. Some authors have suggested an autosomal dominant mode of transmission with variable penetrance95-97 or an X-linked recessive sample of inheritance. To date, the involvement of genetic components in such nonhereditary syndromes has not been clearly demonstrated. The first intraembryonic angioblasts appear on the single-somite stage (during the third week of embryonic life), and interconnection with their extraembryonic counterparts is established at the two-somite stage. Advances in our understanding of angiogenesis and vascular remodeling have offered new insight into the pathophysiology of vascular malformations in the brain, and consequently, potential new treatment methods are rising. Feeding arteries and draining veins are usually mature, normal-appearing vessels, which can have a point of wall thickening. This concept of lively angiogenesis and vascular remodeling in intracranial vascular malformations is opening a model new scientific paradigm in which pharmacologic interventions are proposed to stabilize these irregular blood vessels and stop further development or hemorrhage. Research on intracranial vascular malformations has been focusing on figuring out roles of angiogenic and antiangiogenic elements of their pathophysiology. Such adjustments can trigger vascular transforming, the method of which may further have an result on local hemodynamics. Whether acquired or congenital, ongoing vascular transforming and angiogenesis, presumably triggered by aberrant native hemodynamics, have been thought-about to be a crucial element of their pathophysiology. This elevated move leads to cerebral arterial hypotension along the trail of the shunt. Despite vital cerebral arterial hypotension, most sufferers are free from ischemic symptoms. Hypotensive normal mind areas can be demonstrated, for the most half, to have comparatively normal ranges of tissue perfusion, implying some adaptive change in whole cerebrovascular resistance. A evaluation of the studies that examined interval angiograms from a total of 106 patients with imply follow-up time of 8. Angiogenesis and vascular reworking are controlled by the orchestration of a selection of angiogenesis-related components. The residual nidus grew and recruited new feeding vessels and was excised surgically. Angiopoietin and Tie-2 Angiopoietins and their receptor, Tie-2, play a crucial position in angiogenesis and vascular stability. Ang-1 and Ang-2 are each roughly 75-kD secreted proteins with considerable sequence homology; each bind to Tie-2 with comparable affinity, and neither binds to Tie-1. Ang-1 is widely expressed in embryos and adults, whereas Ang-2 seems to be current in tissues undergoing energetic vascular reworking, such as the ovary, uterus, and placenta. Ang-2 competitively inhibits the Ang-1-induced kinase exercise of Tie-2 and features as an Ang-1 antagonist. It has been suggested that Ang-2 may have a extra biologically lively position than simply being an antagonist against Ang-1. The contradictions amongst these studies underscore a fundamental issue in utilizing the immunohistochemical approach to quantitatively or semiquantitatively assess expression of angiogenic components. The angiopoietin-Tie-2 system appears to have an autoregulatory suggestions mechanism that could be regulating the general activity of the Tie-2 system in both physiologic and pathologic conditions. The gene microarray technique has turn into a robust molecular software to analyze gene expression profile by measuring expression ranges of more than one thousand genes. Such studies, coupled with findings from experimental angiogenesis models in the mind,173,174 can generate new hypotheses. There is an rising curiosity in studying expression profile of a lot of genes and their merchandise. Two unbiased research used the gene microarray technique to characterize gene expression sample in intracranial vascular malformations. Conventional molecular assay strategies, such as Western blot, Northern blot, immunohistochemistry, and in situ hybridization, are designed to measure the expression of a single gene or its product. Such components include numerous major regulators of angiogenesis and vascular transforming. Mixed vascular malformations of the brain: medical and pathogenetic issues. Acute cerebellar hemorrhage secondary to capillary telangiectasia in an toddler: A case report. A theoretical model of cerebral hemodynamics: application to the examine of arteriovenous malformations. Abnormal sample of tie-2 and vascular endothelial growth issue receptor expression in human cerebral arteriovenous malformations. Redefined function of angiogenesis in the pathogenesis of dural arteriovenous malformations. The association of cerebral aneurysms, infundibula and intracranial arteriovenous malformations. The pathogenesis of arteriovenous malformations: insights provided by a case of multiple arteriovenous malformations growing in relation to a developmental venous anomaly. Exceptional multiplicity of cerebral arteriovenous malformations related to hereditary hemorrhagic telangiectasia (Osler Weber Rendu).