
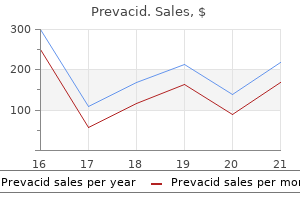
Prevacid dosages: 30 mg, 15 mg
Prevacid packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Prevacid 15 mg generic with mastercard
These research recommend that the Chwalle membrane gastritis diet oatmeal prevacid 30 mg buy, which has been thought to type from the urogenital sinus gastritis diet 8 jam buy cheap prevacid 15 mg on-line, might actually be derived from luminal cells in the ureter that undergo apoptosis at a comparatively late stage, earlier than the onset of renal operate, which may be necessary for producing a patent connection between the distal ureter and bladder. Minor degrees of hydronephrosis may not be as readily identified, though modifications over time could prompt recognition. The anticipated ureteral dilation is most likely not readily detected but can be traced to the bladder. The bladder have to be inspected in all such cases to establish a ureterocele, but it may be required to await bladder filling to make this statement. The character of the renal parenchyma of the higher pole should be noted, both thickness and echogenicity. The findings ought to by no means be used alone to determine salvageability of the higher pole but may be helpful in making medical decisions. The ectopic ureter can seem equivalent to a ureterocele except on the bladder level, with a dilated upper pole, tortuous ureter, however no intravesical element. On occasion, a large ectopic ureter might impinge on the bladder and appear as an intravesical construction, termed a pseudoureterocele (Sumfest et al, 1995). These patterns are identical to the postnatal look, however their recognition does require an skilled maternal-fetal ultrasonographer. With a tentative prognosis of a ureterocele or ectopic ureter, careful analysis of the opposite renal items and bladder must be made. Ipsilateral lower pole or contralateral dilation suggests reflux or much less generally obstruction from the ureterocele or the dilated ectopic ureter. Bladder outlet obstruction by a ureterocele can happen and manifest as hydronephrosis of all renal units (Ogunyemi, 2001; Quintero et al, 2001; Godinho et al, 2013). Although it is extremely unusual to determine bladder obstruction from a ureterocele to the extent to produce oligohydramnios, this could happen. Contralateral renal dysplasia could additionally be evident and associated with reduced amniotic fluid. The want for prenatal intervention or early delivery is outstanding and unlikely to present any vital benefit. A single-system ureterocele or ectopic ureter shall be evident with dilation of the complete kidney as nicely as ureter. It could also be impossible to differentiate this from an obstructive megaureter or severe reflux, but it will have little quick prenatal medical impact. Incidental When vital hydronephrosis is current with both an ectopic ureter or ureterocele, an incidental prognosis will occasionally be made. In some circumstances, however, this will likely result from a search for an explanation of general stomach pain that was not thought of to have a renal cause. It can be attainable that the dilated ureter will not be acknowledged as such, and instances of presumed ovarian cysts have been seen that have been really markedly dilated ureters (Mason et al, 2012). Infection Infection remains a major cause for medical presentation of both ectopic ureters and ureteroceles, which may occur at any age and have a extremely variable pattern. The abnormality prompts postnatal imaging, which is in a position to invariably decide the precise trigger, result in additional studies, and allow an enough characterization of the situation. The prenatal imaging patterns are equivalent to these seen postnatally on ultrasound imaging, yet may be misinterpreted. While these are described in the chapter on prenatal prognosis (Chapter 124), a quantity of parts should be emphasized. The identification of a duplex system prenatally could additionally be difficult except when one of the moieties is dilated. In either case, generalized urosepsis could be the presenting clinical scenario, and a renal bladder ultrasound will normally provide the diagnosis. The excessive variability of high quality of prenatal imaging makes this advice tenuous, and it would appear prudent that an ultrasound examine be obtained in all kids with urosepsis. The value of early detection is the potential for early treatment, which may be a simple drainage process. Ectopic ureters will incessantly manifest with a less acute pattern evidenced by ongoing low-grade fever with periodic spikes. This medical sample ought to prompt an ultrasound study, which can usually reveal a dilated upper pole or entire system. In boys, a similar generalized subacute pattern of infection could also be present, but more often these boys have epididymitis on presentation. Some have had recurrent episodes of epididymitis earlier than the underlying cause is detected. Prolapse Ureterocele prolapse is an unusual but distinctive presenting sign that will nonetheless confuse the clinician. These are normally smooth, congested mucosal-covered intralabial plenty, and the child may be experiencing issue voiding. An ultrasound examination of the bladder will often confirm the analysis, and kidney photographs will additional assist this. Incontinence Clinical Patterns Urinary incontinence may be attributable to an ectopic ureter in a girl, but not in a boy. The toilet-trained woman with verified continuous urinary leakage should be evaluated for an ectopic ureter. Imaging research might not instantly detect this situation as a end result of the affected renal moiety will not be dilated, and the extent of suspicion have to be guided by a cautious history and occasionally bodily examination. Before rest room training it could be difficult to detect continuous incontinence, although some dad and mom will notice persistent dribbling throughout altering. Persistence will normally prompt evaluation, and the characteristic historical past can be obtained. When requested if the kid can be dry for 30 to 60 minutes, the mother or father will normally say no. It is important to be cautious in questioning, because some mother and father with kids who wet for other causes might state, "She is all the time moist," when in fact the kid could be dry for durations of time. In uncommon sufferers it has been intermittent, maybe caused by intermittent leakage by way of a membrane of Gartner duct. In older kids in whom the prognosis has not been recognized, attribution of the symptoms may be to dysfunctional voiding, laziness, and even sexual abuse (Lane, 1962; Carrico and Lebowitz, 1998). During the history taking, signs of typical voiding dysfunction such as voiding postponement, posturing, and constipation must be sought to assess probability of these being an explanation for the wetting. LatePresentation Presentation of both ectopic ureters and ureteroceles within the teen or grownup has been reported, normally associated with an infection or stomach ache and rarely incontinence (Idbohrn and Sjostedt, 1954; Abrahamsson et al, 1981; Amitai et al, 1992; Westesson and Goldman, 2013). The nonobstructing ureterocele, often related to a single system, is well acknowledged within the grownup, typically with a stone in the small ureterocele (Singh, 2007; Mizuno et al, 2008). Vaginal wall prolapse has also been related to an ectopic ureter (Chai et al, 2014). Pain Pain is uncommonly associated with either an ectopic ureter or a ureterocele.
Prevacid 15 mg buy generic line
A window of the dartos pedicle is made gastritis diet ������������� prevacid 30 mg buy generic on-line, and the penile shaft is brought by way of this window gastritis emocional buy prevacid 15 mg mastercard. An alternative is the use of single or a quantity of Z-plasty procedures to correct the defect (Mokhless et al, 2011). The location may be suprainguinal (most common), infrainguinal, or perineal (Lamm and Kaplan, 1977; Elder and Jeffs, 1982). This anomaly has been related to cryptorchidism, inguinal hernia, and bladder exstrophy in addition to with the popliteal pterygium syndrome (Cunningham et al, 1989). In one evaluate, 70% of boys with a suprainguinal ectopic scrotum exhibited ipsilateral upper urinary tract anomalies, together with renal agenesis, renal dysplasia, and ectopic ureter (Elder and Jeffs, 1982). Another research indicated that an associated perineal lipoma was found in 83% of those youngsters; 68% of those with a lipoma had no associated anomalies, whereas one hundred pc of those with no lipoma had associated genital or renal malformations (Sule et al, 1994). Because the embryology of the gubernaculum and of the scrotum are intimately associated chronologically and anatomically, the ectopic scrotum might end result from a defect in gubernacular formation that forestalls migration of the labioscrotal swellings (Hoar et al, 1998). Patients with an ectopic scrotum should bear upper urinary tract imaging with ultrasonography. Scrotoplasty and orchiopexy could additionally be performed at 6 to 12 months of age or earlier if other surgical procedures are necessary for associated anomalies. ScrotalHypoplasia Scrotal hypoplasia, the underdevelopment of one or both sides of the scrotum, happens mostly in boys with an undescended testis and in infants with genital ambiguity. The deformity could result from lack of gubernacular swelling of the labioscrotal folds. In one case, a number of anomalies have been discovered; in the second case an isolated hemiscrotal agenesis was reported. In addition, the testes on the affected side were in what would have been the traditional location (Flum et al, 2012; Yilmaz et al, 2013). Scrotoschisis Meconium peritonitis might occasionally trigger genital manifestations, including meconium hydrocele (Ring et al, 1989) and congenital rupture of the scrotum, termed scrotoschisis (Gongaware et al, 1991; Salle et al, 1992; Chun and St-Vil, 1997; Kojori and Demaria, 2007; Premkumar et al, 2009). When scrotoschisis is detected the clinician ought to suspect meconium peritonitis and proceed with the appropriate evaluation. Treatment entails scrotal exploration with orchiopexy and primary closure of the scrotal wall defect. Hemangiomas are on the pores and skin, are sometimes congenital, and should show vital development within the postnatal period followed by gradual involution. Vascular malformations are current at birth within the subcutaneous tissues and tend to persist or to enlarge, which may happen secondary to trauma, sepsis, or hormonal modifications (Ramos et al, 1999). Vascular malformations can be subdivided into both slow-flow (capillary, lymphatic, venous) or fast-flow (arterial, arteriovenous) types. Strawberry hemangiomas are the most typical sort and outcome from proliferation of immature capillary vessels. These are also categorized as cutaneous hemangiomas as a outcome of they happen on the pores and skin. Although the lesions could undergo a interval of speedy development lasting 3 to 6 months, gradual involution is widespread, and most lesions require no remedy (Casale and Menashe, 1989; Girard et al, 2006). If ulceration develops, intervention is important to stop complications from bleeding. Treatment with laser therapy allows selective photothermolysis and destruction of superficial blood vessels (Kennedy et al, 1993; Ward et al, 1998). CongenitalHemangiomas Congenital hemangiomas are widespread and affect the genitalia in approximately 1% of all hemangiomas (Alter et al, 1993). The processus vaginalis types during the third month of gestation as the peritoneum bulges into the inguinal canal simply earlier than the onset of testicular descent. On completion of testicular descent, the processus vaginalis obliterates and the portion adjacent to the testes becomes the tunica vaginalis. Obliteration of the processus vaginalis continues postnatally, and its failure to obliterate accounts for nearly all inguinoscrotal abnormalities seen in infancy and childhood. In an post-mortem series, Mitchell found closure of the processus vaginalis in 18% of full-term infants at start (Mitchell, 1939). Among 1965 youngsters present process unilateral inguinal hernia restore, Rowe identified a patent contralateral processus vaginalis in 63% of sufferers youthful than 2 months and about 40% of these 1 to 2 years of age, with similar frequency up till age sixteen years (Rowe et al, 1969). The incidence of incidental patency observed in older youngsters and adults at post-mortem or laparoscopy is about 20% (Ajmani and Ajmani, 1983; van Wessem et al, 2003). In contrast to cutaneous hemangiomas, which tend to involute, cavernous hemangiomas are probably to enlarge progressively and ought to be handled with care. Definitive treatment by en bloc resection is advised, and preoperative angioembolization might cut back the dimensions of the mass and the chance of bleeding. EpidemiologyandPathogenesis Inguinal Hernia and Communicating Hydrocele Inguinal hernias develop in 1% to 5% of kids. The incidence is 5 to 10 times more frequent in boys and considerably extra common among untimely infants (13% of babies born earlier than 32 weeks and almost 30% of infants weighing less than 1 kg). The propensity for the best side (3: 1) is attributed to the later descent of the proper testicle. Female gender, prematurity, age younger than 1 yr, and historical past of cryptorchidism are danger factors for bilaterality (Ein et al, 2006; Brandt, 2008). One examine suggests a protecting impact of breastfeeding towards the event of inguinal hernias (Pisacane et al, 1995). Whereas hernias may happen at any time throughout childhood, the average age at presentation is three to four years, with nearly one third of instances manifesting before age 6 months (Kapur et al, 1998). Concomitant hydroceles are frequently seen; 19% of 6361 cases were discovered by Ein and colleagues (2006) (70% scrotal, 26% twine, and 4% both) (Ein et al, 2006). The majority of new hydroceles occurring after delivery and before puberty are related to a patent processus vaginalis. In an observational research, 59% of 302 newly identified hydroceles in sufferers 1 to 18 (mean four. Seventy (65%) of the apparently noncommunicating and 5 (29%) of the twine hydroceles have been adopted, and spontaneous resolution was noted in 39 and 3, respectively. Among boys undergoing hydrocele repair, full obliteration of the processus vaginalis was famous in 0% to 22% of instances (Elder, 1992; Barthold and Redman, 1996; Han and Kang, 2002). Klippel-Tr�naunay-WeberSyndrome Klippel-Tr�naunay-Weber syndrome is a triad of cutaneous vascular malformation, most commonly nevus flammeus, together with soft tissue and bone hypertrophy. The anomaly manifests at delivery, usually involving a decrease extremity, but it might additionally contain the trunk or face. In a evaluate of 214 sufferers from a single establishment, Husmann and colleagues (2005) discovered that 30% had genitourinary cutaneous or visceral involvement. Of the forty eight (22%) who had cutaneous genital involvement, 29% developed intractable bleeding. These lesions are congenital but are usually not diagnosed until the teenage years or younger maturity.
Diseases
- Harrod Doman Keele syndrome
- Porphyria, hereditary coproporphyria
- Strongyloidiasis
- Sudden infant death syndrome
- Retrograde amnesia
- Renal genital middle ear anomalies
Buy prevacid 30 mg on-line
Children with meatal involvement must be noticed postoperatively because of the risk of recurrent meatal stenosis gastritis symptoms upper right quadrant pain discount 30 mg prevacid amex. An strategy that spares the prepuce was described by Wilkinson and colleagues on 104 uncircumcised boys for whom triradiate preputial incisions and injection of triamcinolone intralesionally had been performed gastritis attack diet prevacid 15 mg buy low price. The improvement of meatal stenosis occurred in considerably fewer boys than in those who underwent preliminary circumcision (Wilkinson et al, 2012). AbnormalPenileNumber Aphallia Penile agenesis outcomes from failure of growth of the genital tubercle (Roth et al, 1981). The disorder is rare, with an estimated incidence of 1 in 10 million to 30 million births. The urethra typically opens on the anal verge adjacent to a small skin tag or may open into the rectum. The incidence of stillbirth or neonatal demise is approximately one in three circumstances (Gilbert et al, 1990). Associated malformations are frequent and include cryptorchidism, vesicoureteral reflux, horseshoe kidney, renal agenesis, imperforate anus, and musculoskeletal and cardiopulmonary abnormalities (Skoog and Belman, 1989; Evans et al, 1999). Skoog and Belman (1989) reviewed 60 reports of aphallia and located that the more proximal the urethral meatus, the larger the likelihood of neonatal demise and the incidence of different anomalies. Sixty p.c of patients had a postsphincteric meatus situated on a peculiar appendage at the anal verge; these sufferers had the highest survival fee (87%) and the bottom incidence of other anomalies (1. Twenty-eight percent of sufferers had presphincteric urethral communications (prostatorectal fistula), and there was a 36% neonatal mortality price. This group had the very best incidence of different anomalies and a 100% mortality fee. Children with this lesion should be evaluated immediately with a multidisciplinary strategy. Testing ought to embrace a karyotype and different applicable research to detect related malformations of the urinary tract or different organ techniques. Consequently, the recommendation to carry out gender reassignment ought to be made carefully and solely after full analysis by an ambiguous genitalia assessment group and parental counseling. Some of these sufferers have a male gender identity regardless of reconstruction as a feminine, presumably because of in utero or postnatal sex steroid imprinting (Reiner, 1996; Diamond and Sigmundson, 1997; Diamond, 1999). As a male, the affected person would potentially be fertile; though present advances in phalloplasty and urethroplasty enable for sexual and voiding perform (De Castro et al, 2013; Garaffa et al, 2014), reproductive function is unknown. Gender reassignment involves orchiectomy and feminizing genitoplasty in the neonatal interval (Bruch et al, 1996; Gluer et al, 1998) and neovagina at a later age. Urinary tract reconstruction with simultaneous building of an intestinal neovagina through a posterior sagittal and stomach approach in sufferers with penile agenesis has been described (Hensle and Dean, 1992; Hendren, 1997). Diphallia Duplication of the penis is a uncommon anomaly with an incidence of 1 in 5 million stay births (Hollowell et al, 1977) and has a variety of appearances from a small accessory penis to complete duplication (Gyftopoulos et al, 2002). In some cases every phallus has just one corporal body and urethra, whereas others appear to be a variant of twinning, with every phallus having two corpora cavernosa and a urethra. Other related anomalies are widespread, together with hypospadias, bifid scrotum, bladder duplication, renal agenesis or ectopia, and diastasis of the pubic symphysis (Maruyama et al, 1999). Evaluation ought to embody imaging of the complete urinary tract, together with a renal ultrasonogram and voiding cystourethrogram. Treatment have to be individualized, with consideration of the associated anomalies with the aim of attaining a satisfactory functional and cosmetic outcome (Dean and Horton, 1991). InconspicuousPenis An inconspicuous penis is one that seems to be small but with normal stretched penile length measured from the pubic symphysis to the tip of the glans (see Table 146-2) and normal diameter of the penile shaft (Bergeson et al, 1993). This situation could be congenital or acquired and is normally of nice concern for parents. Several entities are included in this disorder, together with buried penis, trapped penis, and webbed penis (Palmer and Kogan, 1995). These circumstances must be differentiated from micropenis, during which the penis is abnormally small. Buried Penis A buried penis, additionally referred to as a hidden or concealed penis, is a form of inconspicuous penis (Cromie et al, 1998). This condition may be categorized into three categories based mostly on explanation for the concealment (Maizels et al, 1986; Casale et al, 1999): (1) poor penopubic fixation of the skin on the base of the penis, (2) obesity, and (3) a trapped penis from cicatricial scarring after penile surgical procedure, typically a circumcision. The acquired form from weight problems sometimes seen in older youngsters and adolescents is caused by ample fat on the belly wall hiding the penile shaft. The other acquired form, a trapped penis, outcomes from embedding of the penis within the suprapubic fat pad from scar formation over the glans. This deformity may happen after neonatal circumcision in an toddler with significant scrotal swelling as a outcome of a hernia or hydrocele or after routine circumcision in an toddler with a webbed penis. Also, in some neonates the penile shaft seems to retract naturally into the scrotum; and if circumcision is performed on this state of affairs, the pores and skin on the base of the penis might kind a cicatrix over the retracted phallus. This situation must be differentiated from a transient buried penis ensuing from a large suprapubic fat pad noted in early childhood that resolves with increased age and ambulation (Eroglu et al, 2009). On examination, a buried penis should be differentiated from a micropenis with an irregular penile stretched length. The clinician ought to determine whether the glans could be exposed by retracting the skin covering the glans. However, if the penis is trapped by physiologic phimosis within the uncircumcised or cicatricial scarring. Patients with buried penis secondary to weight problems should have the underlying condition treated with referral again to the primary care provider for a weight loss and train program, which is essential; surgical procedure might now not be needed. Young kids with secondary cicatricial scarring after penile surgery can be managed with forceful dilation of the cicatrix with a nice hemostat in the workplace after the application or injection of analgesic. Another option is the mixture of topical betamethasone and manual retraction (Palmer et al, 2005), which yielded full resolution in the majority of boys or released the closing cicatrix, allowing for a simple incision of the phimotic ring; this lowered the necessity for formal surgical restore by 79%. If topical corticosteroid application is ineffective, correction underneath common anesthesia is important, with the usual suggestion of elective repair when the child is no less than 6 months of age. A number of surgical strategies have been described to appropriate the buried penis (Maizels et al, 1986; Casale et al, 1999; Elder, 2001; Frenkl et al, 2004; Gillett et al, 2005; Borsellino et al, 2007; Karapetian and Palmer, 2007). In moderately severe cases the dysgenic bands of tissue, that are positioned primarily on the proximal dorsal surface of the shaft of the penis, should be eliminated. In addition, the subcutaneous tissue on the dorsal side of the penis should be fixed to the pubic fascia, and then the subcutaneous tissue of the scrotum must be mounted to the ventral aspect of the base of the penile shaft. During correction one have to be careful to keep away from harm to the neurovascular bundles (Baskin, 1999; Baskin et al, 2000). Skin protection can be completed by penoscrotal Z-plasty, lateral penile shaft Z-plasty, island pedicle of ventral preputial skin, or a skin graft. Rarely, in essentially the most extreme cases the suspensory ligament of the penis have to be divided, the suprapubic fats excised, and the spermatic cords protected. Liposuction has been reported to be useful in severe cases (Maizels et al, 1986; Shenoy et al, 2000). However, this technique must be reserved for adolescent boys because prepubertal boys could lose their fats pad with somatic growth.
Buy prevacid 30 mg fast delivery
They noted a very low incidence of detrimental impact on gastrointestinal perform in a select group of patients with neurogenic dysfunction gastritis diet cheese cheap 30 mg prevacid. Hydraulic Valves Benchekroun (Benchekroun gastritis diet ������ 15 mg prevacid buy overnight delivery, 1982; Benchekroun et al, 1989) developed a hydraulic valve as a continence mechanism that was modified by Guzman and colleagues (1989). Urine from the reservoir and generated stress is allowed to enter a sleeve of ileum across the catheterizable channel. Compression of the inside tube theoretically supplies continence, and early expertise was encouraging. Initial continence charges approached 75% after which 90% with a single revision (Benchekroun et al, 1989). Others have been unable to duplicate these results (Sanda et al, 1988; Leonard et al, 1990b). Koff and associates (1989) added a similar hydraulic sleeve across the efferent limb of an Indiana pouch, but the utilization of such valves has largely been deserted. Continent Vesicostomy Yachia (1997) described creation of a bladder tube fashioned from a wide flap of the anterior bladder wall. An try and present a continence mechanism was customary by weaving the bladder tube by way of the rectus muscle for compression and continence. Continence in their small, short-term collection was reported to be 100%, however this has not been duplicated. Hanna and associates (1999) described a continence mechanism based on either a flap of bladder or intestinal tissue fashioned after prior enterocystoplasty and used it on a very small collection of patients. The bladder is plicated around the proximal 3 cm of the tube using nonabsorbable suture to create a kind of nipple just like gastric fundoplication. Macedo and Srougi (2000) described a similar continence mechanism created on the time of initial augmentation. Their approach is doubtlessly interesting for patients requiring augmentation and having no appendix due to the simplicity; nevertheless, continence is predicated on a sort of nipple valve that historically has been difficult to maintain fastened. Casale (1991) has described a type of continent vesicostomy during which the continence mechanism relies on a flap valve created from a tubularized strip of bladder mucosa. Parallel incisions three cm apart are made into the anterior bladder and used to create a long rectangular flap. The abdominal wall should be measured to be positive that the strip is long enough to attain the skin with out rigidity. The muscle portion is left broad to come round without tension and supply good blood provide. The edges of this strip are mobilized until it can be tubularized alongside its whole size. It could additionally be helpful to mobilize only one edge over to the other facet to avoid overlapping suture traces. Casale (1991) originally incised the mucosa transversely on the end of the intravesical strip to be tubularized; Rink and colleagues (1995b) then suggested that it could be left intact. More in depth mobilization of the aspect reverse that mobilized for the internal tube allows closure with out overlapping suture lines, which can help avoid fistula formation and incontinence. A, Parallel incisions are made in the bladderdome,formingafull-thicknessbladderstrip. Continence charges have been good, as with most flap valves (Cain et al, 1999, 2002). Stomal stenosis remains a significant problem, 45% in the experience at Indiana University (Cain et al, 2002). Skin flaps and avoidance of pressure to reach the pores and skin could reduce this risk but not get rid of it. Advantages embrace avoidance of an intraperitoneal procedure and bowel anastomosis; the appendix can be reserved to be used with enemas. It does use some bladder and decrease capacity, which may not be applicable for many sufferers. The appendix is simple to use, suitable for most youngsters, and related to superb continence charges. Nipple valves are essentially the most complex continence mechanism and therefore have an extended learning curve. Continence rates approaching 85% could be anticipated with stapled nipple valves (Kaefer et al, 1997b; Benson and Olsson, 1998) after extensive experience. With use of the other efferent limbs, continence charges above 90% and approaching 95% have been reported in kids (Duckett and Snyder, 1986; Hensle and Ring, 1991; Kaefer et al, 1997b; Surer et al, 2003; Ardelt et al, 2012). The incidence of complications after continent diversion will undoubtedly enhance with longer follow-up. These patients might be topic to the identical complications seen with bladder augmentation. All of these issues, together with an infection, hydronephrosis, calculi, spontaneous perforation, and tumor, have been reported after continent diversion in adults if not in kids. Because more gut is often required in continent diversion than bladder augmentation, the incidence of problems might in the end be greater than with easy augmentation. Already, serum adjustments of elevated chloride, decreased bicarbonate, and acidosis have been famous in some sufferers after continent diversion (Allen et al, 1985; Ashken, 1987; Thuroff et al, 1987; Boyd et al, 1989; McDougal, 1992a). The most typical complication in pediatric continent diversion, up to now, has been stomal stenosis. Stenosis happens extra commonly at the umbilicus with use of appendix in contrast with tapered ileal segments (Fichtner et al, 1997; Kaefer et al, 1999b). Ardelt and associates, after intensive review (2012), discovered no consensus that a single sort of efferent limb is superior and instructed that the choice of method must be individualized based on the case. Preoperative analysis ought to establish upper tract obstruction or vesicoureteral reflux. Such issues must be corrected on the time of surgery, though low-grade secondary reflux will usually resolve spontaneously with correction of bladder dysfunction. It is imperative to provide the patient with an enough bladder or reservoir, one capable of holding at low stress a urinary quantity that might be produced between voidings or catheterizations. This can be accomplished by both augmentation or building of a continent reservoir utilizing any gastrointestinal segment. If adequate outflow resistance is lacking, it should be created at the bladder neck to prevent incontinence. Any patient undergoing reconstructive surgical procedure for bladder or sphincter dysfunction must be prepared and capable of performing intermittent catheterization on a reliable foundation; most will require it routinely. The urothelial lining avoids a lot of the morbidity associated with intestinal segments. If essential, nonetheless, nearly any portion of the lower urinary tract could also be reconstructed or changed utilizing intestine.
30 mg prevacid mastercard
Initially the bladder is in a collapsed state gastritis not healing cheap prevacid 30 mg line, which permits for the storage of urine at low pressure by simple unfolding gastritis diet vs regular cheap 30 mg prevacid with amex. Elasticity permits the detrusor muscle to stretch without a rise in tension until it reaches a crucial volume larger than the expected bladder capacity. The viscoelastic property permits for a subtle steady strain change throughout bladder filling. This small rise in pressure is balanced by a corresponding speedy strain decay (Zinner et al, 1976; Wagg and Fry, 1999). The viscoelastic bladder property is outlined as stress leisure and may be overcome when the rate of bladder filling exceeds regular parameters (Mundy, 1984; Finkbeiner, 1999). Properties of elasticity and viscoelasticity will ultimately be overcome in every youngster; at that time, the bladder strain rapidly rises. Favorable dynamics for applicable urine storage embrace a skinny bladder wall with an applicable composition of muscle and collagen allowing for expression of regular elastic and viscoelastic properties. Factors adversely affecting regular compliance embrace detrusor hypertrophy, fibrosis, outlet obstruction, and recurrent urinary infections (Mundy, 1984; Joseph, 1994). Continence throughout urinary storage requires a closed bladder neck and external urinary sphincter. During the passive storage section, the bladder 3330 manifestations of poor compliance, upper tract deterioration, and incontinence (Brading, 1997). Reflexive opening of the bladder neck and sequential leisure of the exterior urinary sphincter enable for low strain balanced voiding and full elimination of urine. Again, obstruction, neurogenic dysfunction, and chronic an infection may cause physiologic changes preventing coordinated operate of the detrusor, bladder neck, and exterior sphincter outlined as dyssynergy (Mundy et al, 1985). A poorly functioning exterior sphincter from denervation fibrosis can also stop appropriate relaxation, causing elevated voiding pressure against a onerous and fast outlet. Finally, detrusor pathophysiology might prevent a sustained, coordinated bladder contraction and full elimination of all urine. Dysfunction Upper Urinary Tract It is crucial to understand the dynamics of the whole urinary tract earlier than any main reconstructive procedure. Upper tract obstruction could additionally be secondary to extreme, long-standing bladder hostility involving poor bladder compliance and emptying. Nuclear renography with a urethral catheter could additionally be helpful to rule out a major upper tract obstruction. Upper tract obstruction, if current, must be corrected at the time of bladder and sphincter reconstruction. Vesicoureteral reflux within the presence of bladder hostility could also be primary or secondary, and differentiating the two may be difficult. If reflux was not current throughout earlier analysis, new onset is likely secondary to bladder hostility. Previous work has suggested that reflux secondary to bladder hostility may not want surgical correction if the bladder is sufficiently managed. It is interesting to speculate whether or not reflux is even a significant problem if a big, compliant bladder is achieved (Soylet et al, 2004). We agree that most secondary reflux will probably resolve with enough reconstruction of the bladder however will appropriate high-grade reflux if present. Caution must be taken when considering the therapy of chronically dilated and scarred ureters. Correcting reflux in that setting is acceptable but can result in obstruction if overly aggressive tapering or tunneling is performed (Hendren, 1998). Dysfunction in the upper urinary tract often manifests with hydronephrosis, pyelonephritis, or impairment of renal function. When such problems are present in patients with lower tract dysfunction, considerate evaluation and therapy are needed. All issues ought to be addressed before and on the time of reconstructive surgery to obtain one of the best outcome. In addition, persistent elevation in filling stress can lead to acquired vesicoureteral reflux (Sidi et al, 1986a; Cohen et al, 1990). A combination of medications and intermittent catheterization have a constructive impact, significantly in youngsters with neurogenic dysfunction (Rink and Mitchell, 1984; Aslan and Kogan, 2002; Verpoorten and Buyse, 2008). When compliance is unaffected by medical administration, augmentation cystoplasty could additionally be required to improve the storage traits. After reconstruction, the chance of efficient detrusor contractions and effective emptying of the bladder is diminished. Intermittent catheterization must be taught and accepted by the patient and caretaker preoperatively. Continence requires outflow resistance generated by the bladder neck and exterior urinary sphincter. Outflow resistance should stay larger than bladder pressure throughout storage throughout normal day by day exercise. When outflow resistance is diminished due to an abnormal bladder neck and exterior urinary sphincter, incontinence typically will occur. Pharmacologic administration with -adrenergic brokers can improve outflow resistance, but extra commonly operative reconstruction is required. Clinical expertise has proven that when acceptable resistance is achieved on the bladder neck by way of operative intervention, antagonistic detrusor characteristics might turn into unmasked and lead to high stress urinary storage or uninhibited contractions not beforehand documented (Bauer et al, 1986; Churchill et al, 1987; Dave and Salle, 2008). For that purpose, provocative urodynamic evaluation with occlusion of the bladder neck is important before any bladder neck reconstruction in an attempt to determine kids who shall be at risk. Normal synergistic voiding occurs when the bladder neck descends, relaxes, and opens, adopted by leisure of the external urinary sphincter and subsequent detrusor contraction leading to low stress voiding. Dysfunctional voiding during this lively bladder section occurs as a end result of uncoordinated activity of the bladder neck, external urinary sphincter, and detrusor. With such dyssynergy, high-pressure voiding results that chronically can negatively have an result on the bladder and higher urinary tract (Mundy et al, 1982; Bauer et al, 1984). Other Considerations Renal function ought to be assessed in any patient present process bladder reconstruction, significantly if hydronephrosis or extreme renal scarring is current. Demos (1962) and Koch and McDougal (1985) have demonstrated that urinary solutes, particularly chloride, are absorbed from urine in contact with the mucosa of small and large bowel. For patients with regular renal function, the kidneys are capable of handle the reabsorbed load of chloride and acid with out apparent difficulty. Patients with decreased renal function, nevertheless, could develop important metabolic acidosis secondary to such reabsorption. The first component of renal operate to deteriorate after obstruction or an infection is concentrating ability. Elevated passive filling stress turns into clinically pathogenic when a strain greater than 40 cm H2O is chronically reached (McGuire et al, 1981; Wang et al, 1988; Weston et al, 1989). Permanent intestinal diversions in youngsters are now sometimes confined to patients requiring cystectomy for cancer. The key to urinary undiversion is to perceive the original pathology that led to diversion. Patients with renal failure or different medical problems may conversely develop oliguria. Low urinary output may have an effect on an augmented bladder or bowel reservoir with higher collection and inspissation of mucus.
Generic 15 mg prevacid otc
Intraoperative occasions differ tremendously amongst these reports and are associated to surgeon experience and inherent patient components corresponding to prior surgery gastritis xantomatosa order prevacid 15 mg mastercard, working space availability gastritis symptoms difficulty swallowing prevacid 15 mg discount free shipping, and whether a pure laparoscopic or robotic-assisted approach is used. Outcomes have been much like those of open reconstruction in early follow-up (Traxel et al, 2010; Gundeti et al, 2013). Potential benefits of a minimally invasive approach embrace sooner restoration and improved cosmesis (Hasan et al, 2011). Experience with these approaches is already accumulating quickly, and thorough analysis might be needed to determine if a minimally invasive strategy is costeffective, notably in the neurogenic population. Although augmentation cystoplasty works well for most sufferers who require it and although work on alternate options to bowel cystoplasty may lower morbidity for the patient, a primary objective for each pediatric urologist is to reduce the variety of patients needing cystoplasty. Xiao and others (2005; Peters et al, 2010) continue to refine a man-made somatic-autonomic reflex pathway in children with neurogenic dysfunction. No matter what the prognosis, earlier and more aggressive therapy of bladder dysfunction may minimize the insult to the bladder and maximize restoration as well as ultimate bladder operate. Early urodynamic analysis of boys with posterior urethral valves might determine treatable bladder issues and enhance the prognosis from the standpoint of the kidneys and bladder (Misseri et al, 2002; Casey et al, 2012). Grady and associates (2003) suggested that full primary restore of bladder exstrophy leads to early bladder biking that improves eventual bladder function and reduces the chance of augmentation cystoplasty. With perhaps essentially the most compelling evidence to date, Kaefer and colleagues (1999a) found that only 17% of patients with hostile neurogenic bladder dysfunction treated instantly on prognosis required augmentation cystoplasty as in contrast with 41% of comparable patients treated expectantly. Although the sequence included no collaborative urodynamic information and might be subject to lag time bias, the authors felt that there was a big distinction within the outcomes for the two teams. On early examination, early bladder administration had not decreased the speed of augmentation cystoplasty (Lendvay et al, 2006); nevertheless, more modern re-evaluation (Schlomer et al, 2013) instructed that augmentation rates have fallen by 25% in the past decade. Critical, prospective analysis of ChoiceofSegmentandApproach Enterocystoplasty improves bladder capacity and compliance in most cases when medical management fails. All gastrointestinal segments have been used and proceed to be used with good outcomes. Unremitting medical issues are comparatively uncommon after augmentation cystoplasty if used appropriately in well-selected sufferers. No one bowel section has a clear benefit over others when all such issues are thought of. Patient prognosis, anatomy, and physiology might suggest that one bowel segment is preferable for a specific affected person. Each surgeon interested in augmentation cystoplasty ought to be familiar with the benefits and downsides of every phase in different settings. It is probably going that such improvements will minimize the necessity for cystoplasty but not utterly remove it (Cain and Rink, 2010). Ureterocystoplasty It has been noted for years that in patients with posterior urethral valves, unilateral reflux may behave as a pop-off valve to decrease intravesical pressures and shield the contralateral upper tract (Hoover and Duckett, 1982; Rittenberg et al, 1988; Kaefer et al, 1995). It was a logical extension to use ureteral tissue in that setting to increase the bladder. This incision offers access to the gut should mobilization of the ureter for augmentation be unsatisfactory. Bellinger (1993), Dewan and colleagues (1994), and Reinberg and colleagues (1995) have proven that ureterocystoplasty could be carried out via two incisions, remaining fully extraperitoneal. A standard nephrectomy is performed with great care to preserve the renal pelvic and higher ureteral blood provide. All adventitia and periureteral tissue are swept from the peritoneum towards the ureter during mobilization to shield the ureteral blood supply. As the ureter enters the true pelvis, the blood supply arises posterior and laterally. Posteriorly, this incision has typically been carried off-center directly into and through the ureteral orifice of the ureter used for cystoplasty. The ureter is folded on itself, and the ureterto-ureter and ureter-to-bladder anastomosis is performed with working absorbable suture. A suprapubic tube is left indwelling by way of the native bladder for 3 weeks during healing. Any patient attempting to void must prove that he or she can empty adequately via a examine of postvoid residuals. Alternatively, the bladder incision may be stopped approximately 2 cm from the orifice, and an analogous length of distal ureter left in situ and intact without incision. This modification of technique is simpler and may be safer in that it avoids potential injury to the blood supply of the ureter. Early experience with the procedure noted that the entire renal pelvis could be preserved, permitting extra tissue for cystoplasty (Churchill et al, 1993; Landau et al, 1994; McKenna and Bauer, 1995; Reinberg et al, 1995). As with intestinal cystoplasty, folding the ureter right into a extra spheric configuration maximizes the volume to be achieved. If a massively dilated ureter drains a functioning kidney, the distal ureter alone may be used for augmentation, with the proximal ureter either reimplanted into the bladder or anastomosed to the contralateral ureter (Bellinger, 1993). Numerous collection have reported good results after augmentation utilizing ureter, some with follow-up so lengthy as eight years. Landau and colleagues (1994) in contrast age-matched and diagnosis-matched kids undergoing ureterocystoplasty or ileocystoplasty. The whole imply bladder capacity was 470 mL within the ureterocystoplasty group and 381 in the ileocystoplasty group. Bladder volumes at 30 cm H2O had been 413 mL and 380 mL after ureterocystoplasty and ileocystoplasty, respectively. Work has proven that one dilated ureter usually is sufficient for cystoplasty (Zubieta et al, 1999; Kajbafzadeh et al, 2010). The main drawback to ureterocystoplasty is the limited affected person inhabitants with a nonfunctioning kidney draining into a megaureter. The final success of ureterocystoplasty utilizing normal ureter requires further follow-up, particularly because ImprovingQualityofLife Reconstruction to obtain continence has been assumed to enhance health-related high quality of life. Assessment of the social impression of using a catheterizable channel as a substitute of urethra is limited (Kari et al, 2013). Most analysis of surgical techniques to date has centered on outcomes and problems from the attitude of surgeons. Tools to purchase that data must be validated for longitudinal study of these sufferers and their disease processes. It has occurred most frequently in colonic segments used in the neurogenic inhabitants. Efforts have lined the spectrum from artificial materials and autologous grafts by way of creation of a bladder diverticulum (autoaugmentation) to numerous forms of neural stimulation. Some of these alternate options seem to maintain promise, however none have stood the take a look at of time compared to intestinal cystoplasty.
Round-Leafed Sundew (Sundew). Prevacid.
- Dosing considerations for Sundew.
- Coughs, asthma, bronchitis, cancer, and ulcers.
- How does Sundew work?
- Are there safety concerns?
- What is Sundew?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96881
Buy discount prevacid 15 mg line
The youngster who wets in the course of the day and night time can be said to have daytime urinary incontinence and enuresis or nonmonosymptomatic enuresis gastritis symptoms in pregnancy prevacid 30 mg buy generic on line. When pelvic flooring exercise elevated in affiliation with detrusor contractions helicobacter gastritis diet order prevacid 30 mg overnight delivery, wetting was often avoided, and sufferers usually would awaken subsequently to void. Regardless of the mechanism, urine manufacturing that normally decreases at evening secondary to these circadian techniques fails to achieve this and will subsequently lead to nocturnal polyuria, which might exceed the useful capacity of the bladder and result in an enuretic episode. Proof of this idea was demonstrated by Rasmussen and colleagues (1996), who had been in a position to really induce enuresis in normal wholesome kids by increasing nocturnal urine output. Enuresis is logically thought to result from a disruption or maturational lag in one or more of these critical domains. Parents invariably describe their youngsters with enuresis as excessively deep sleepers (Wille, 1994; Nev�us et al, 1999a). Wolfish and coworkers (1997) carried out a laboratory research of 33 boys aged 7 to 12 years (15 with enuresis and 18 age-matched controls) and located that attempts at arousal had been more often successful in control subjects than in boys with enuresis (40% vs. However, when volumes had been measured throughout general anesthesia, enuretic kids had similar imply bladder volumes to awake controls. In a considerably contradictory study, Kawauchi and colleagues (2003) found that the maximal endurable bladder capability through the daytime was related between kids with enuresis and controls. However, among kids with enuresis, the maximal voided quantity in the course of the evening (measured utilizing a diaper and enuresis alarm) was significantly smaller than the maximal daytime bladder capacity. Other sleep research, nevertheless, present that sleep patterns among kids with and without enuresis are similar (Ritvo et al, 1969; Bader et al, 2002). Treatment Conventional therapies for enuresis embody behavioral modification, the enuresis "moisture" alarm, and pharmacologic remedy. However, enuresis that happens as occasionally as once per thirty days is associated with reduced self-esteem and remedy has been reported to improve self-worth, regardless of the kind or the success of therapy (H�ggl�f et al, 1998; Longstaffe et al, 2000). It is essential to decide whether the kid is mature sufficient to assume accountability for treatment. The baby have to be extremely motivated to take part in a treatment program that will take months to achieve successful outcomes. Although general recommendation must be given to all bedwetting children, energetic therapy ought to often not be started before 6 years of age (Nev�us et al, 2010). As beforehand discussed, the voiding diary is an objective technique of documenting the voiding pattern (see part on Bladder and Bowel Diaries). A voiding diary saved by the mother and father should help assess the times at which a toddler voids; the connection between voiding and customary events corresponding to meals, breaks at college, and play actions; the prevalence of urgency or incontinence; and voided quantity. Briefly, examination ought to embody palpation of the abdomen to display screen for constipation, examination of the lower spine for cutaneous stigmata of spinal dysraphism, examination of the genitalia to screen for meatal stenosis, introital erythema or damp/wet underwear, evaluation of the sacral reflex arc, and evaluation of the motor power, tone, reflexes, and sensation in the legs for evidence of a neurogenic bladder. In terms of laboratory testing, a simple urinalysis must be performed to detect any potential glucosuria, proteinuria, hematuria, pyuria, and/or bacteriuria. Children should try to void frequently during the day and just earlier than going to bed for a total of six to seven occasions every day. Daily fluid consumption must be concentrated within the morning and early afternoon, and both fluid and solute consumption ought to be minimized in the course of the night. In apply, compliance improves when mother and father and youngsters understand regular bladder function and the pathogenesis of enuresis. A personalized calendar for recording daytime incontinence and enuresis episodes and the frequency and timing of bowel movements aids the household and child to follow their progress. They are both valid remedy choices, however affected person, caregiver, and disease-related parameters exist that will aid in providing prognostic information when it comes to which therapeutic modality must be first entertained. Proposed mechanisms include suppression of bladder emptying during sleep, rising nocturnal bladder volume (Hansen and J�rgensen, 1997), and waking to void by signaling once they urinate. Enuresis alarms are activated when a sensor, placed in the undergarments or on a mattress pad, detects moisture, with both types demon- strated to be equally efficient (Butler and Robinson, 2002). The child should then return to the bed room, change the bedding and underwear, replace the sensor, and reset the alarm before returning to sleep. A diary should be stored of wet and dry nights, with optimistic reinforcement given for dry nights as properly as profitable completion of the sequence of occasions. Approximately 30% of sufferers discontinue enuresis alarms for varied reasons, together with skin irritation, disturbance of different relations, and/or failure to wake the child (Schmitt, 1997). Alarm remedy should be continued until the child has had a minimal of 14 consecutive dry nights (Nev�us et al, 2010). Therapy with the alarm could be reinitiated for relapse (more than two wet nights in 2 weeks). During this refractory remedy interval, the possibility of long-term cure could be elevated by a technique known as overlearning (Morgan, 1978). In overlearning, further fluids are given at bedtime whereas alarm coaching is sustained after dryness has been achieved (Young and Morgan, 1972). In alarm training with out overlearning, the child trains to inhibit urination without necessarily learning to wake to void. Desmopressin is pretty straightforward to administer and its clinical effects seem instantly, with a serum half-life of roughly 2 to three hours when taken in oral type (the length of pharmacodynamic motion approximates the common length of sleep for a kid in the age vary for elementary school). The main security concern is the risk for water intoxication with resultant hyponatremic seizures ought to the drug be taken with extreme fluids. This risk appears to be somewhat greater with the intranasal type, which has a prolonged half-life, and thus use of the spray is discouraged (Robson et al, 2007). Treatment must be interrupted throughout episodes of fluid and/or electrolyte imbalance. Fluid intake is decreased to a maximum of 1 8-oz glass at the time of ingestion, with absolutely no extra fluids till morning, reducing the risk for vital hyponatremia to nearly zero (Glazener and Evans, 2009). Overall, approximately 30% of sufferers obtain complete dryness and another 40% exhibit a significant decrease in nighttime wetting (Nev�us et al, 2010). Corroborating the original examine by Austin and associates, the oxybutynin group showed a better rate of full and partial responses than the placebo group. The responders to mixed oxybutynin and desmopressin had a significantly decrease bladder quantity and wall thickness index than nonresponders. Combination Therapy the efficacy of the enuresis alarm plus desmopressin combination has been investigated in a selection of research (Sukhai et al, 1989; Bradbury, 1997; Leebeek-Groenewegen et al, 2001; Fai-Ngo et al, 2005). A discount in the number of moist nights is constantly observed when using mixture therapy of desmopressin and the moisture alarm compared to monotherapy. A second latest evaluation of complementary approaches corresponding to hypnosis, psychotherapy, and acupuncture found limited proof from small trials with methodologic limitations to help using such modalities for the therapy of enuresis (Huang et al, 2011). They confirmed a major lower in the number of wet nights per week with combination remedy. After 6 months of follow-up, however, they reported that there was no vital distinction between the 2 treatment teams regarding the efficacy and number of children who relapsed. They assigned 105 kids equally amongst groups to obtain remedy for 12 weeks, and patients were then adopted for 12 weeks after treatment. They found that the mean variety of moist nights per week was significantly lower in the mixture group than in the other groups at the conclusion of remedy.
Buy generic prevacid 15 mg online
These sufferers must be placed in essentially the most comfy place potential with out excessive contortion or flexion of the joints gastritis diet 444 purchase prevacid 15 mg free shipping. Special attention have to be paid to latex precautions in sufferers with myelomeningocele gastritis que debo comer 30 mg prevacid generic visa, and as in all cases, correct padding of strain points is obligatory. For advanced calculi occupying multiple calyces including the lower pole, a supracostal posterior entry is preferred to present visualization of the superior calyx and pelvis, access to the pelvis and ureter, and straight access to the inferior calyces allowing simpler manipulation of the working devices and minimizing torque on the collecting system (El-Nahas et al, 2008). With the C-arm in the 90-degree aircraft, the depth and medial extension of the needle are checked. The most common approach employed is serial dilation with Amplatz dilators over working wires and subsequent sheath placement beneath fluoroscopic guidance. For smaller youngsters and decrease stone burdens, an 11-Fr to 13-Fr peel-away sheath (Docimo Mini-Perc; Cook Urological Inc. This method permits dilation and sheath placement in a single step, minimizing potential parenchymal trauma and bleeding from sequential dilation with rigid dilators. In addition, 7-Fr and 8-Fr offset cystoscopes with 5-Fr working ports and 7- to 9-Fr flexible ureteroscopes can be utilized through an 11-Fr entry sheath with enough clearance to enable low-pressure irrigation (Wu and Docimo, 2004). Postoperative stenting and placement of a nephrostomy tube are affected person and surgeon dependent and vary amongst series. Risks for nephrolithiasis included dependency on totalparenteralnutrition,osteomalacia,chronicdehydration,hypocitruria,andhyperoxaluria. D, Prone view of the antegrade nephrostogram via a 6-Fr nephrostomy tube demonstrating "stone-free" standing. Findings demonstrated that the number and measurement of tracts were considerably related to postoperative hemoglobin lower (mean 1. Transfusion was related to operative time, sheath dimension, and stone burden (Zeren et al, 2002). When stratified by tract dimension (14 Fr, 20 Fr, and 24 Fr), efficacy charges were comparable in all groups, but there have been no issues or transfusions in the 14-Fr tract group (Bilen et al, 2007). A giant multicenter study demonstrated that essentially the most vital determinants affecting complication charges had been operative time, sheath dimension, midcalyceal puncture, and partial staghorn formation (Onal et al, 2014). These early experiences demonstrate that laparoscopic pyelolithotomy is possible, secure, and efficacious as an various selection to open pyelolithotomy in youngsters and warrants additional examine. However, because of their demanding technical nature, these procedures are prone to be limited to endourologic administration failures in tutorial facilities with plentiful expertise in laparoscopic and robotic pediatric surgical procedure. When stratified by age, anatomy, bilaterality, and renal perform, stone-free outcomes were equal in all groups. Endoscopic surveillance through the preliminary process can decide the necessity for second-look nephroscopy without counting on extra imaging and the related risks of radiation publicity (Roth et al, 2009). Bladder stones from kids in these developing nations are most frequently composed of ammonium acid urate. In contrast, among children from industrialized nations, bladder stones are most frequently present in children with spinal cord injuries and/or congenital abnormalities corresponding to spina bifida. These youngsters usually have undergone augmentation cystoplasty and/or handle their bladders by clear intermittent catheterization. It has been reported that 50% of those youngsters with reconstructed bladders develop bladder stones in their lifetime (Palmer et al, 1993). Urinary stasis, bacterial colonization or infection with urea-splitting organisms, retained mucus, and international bodies all can contribute to the formation of bladder stones, most of which are struvite. In kids, a smaller caliber urethra limits efficient therapy of enormous bladder stone burdens. However, percutaneous cystolithotripsy is used worldwide with the benefit of shorter hospital stays, smaller scars, and fewer indwelling catheter time postoperatively (Al-Marhoon et al, 2009). At the current time, percutaneous cystolithotripsy is the popular methodology to deal with bladder stones which have formed in reconstructed bladders (Paez et al, 2007). For instance, Salah and colleagues (2005) reported on their expertise with cystolithotripsy in one hundred fifty five kids from Pakistan and Yemen with a mean age of 4. All youngsters had been treated safely and efficiently utilizing a 26-Fr nephroscope through a 30-Fr sheath positioned through a 1-cm suprapubic incision (Salah et al, 2005). Percutaneous cystolithotripsy has been used effectively in infants youthful than 1 yr to clear bladder stones. Gan and colleagues (2010) reported on their experience utilizing a 16-Fr peel-away sheath with a ureteroscope to deal with bladder stones with an average dimension of 1. Percutaneous cystolithotripsy in kids may be performed under ultrasound or fluoroscopic steering and is most frequently an outpatient procedure. With both modality, the bladder is first stuffed to capability with water or distinction material. The baby is placed in Trendelenburg place to reduce the chance of bowel harm throughout entry and tract dilation/formation. An 18-gauge needle is positioned into the distended bladder midline, one to two fingerbreadths above the pubic bone. When correct placement is confirmed with return of fluid, a wire is passed via the needle into the bladder. Most typically, a tract is established with a balloon dilator to accompany a 30-Fr sheath. A 26-Fr nephroscope is used to extract stones smaller than 1 cm with a inflexible stone forceps, or an ultrasonic lithotripter may be used to fragment stones bigger than 1 cm. At the conclusion of a percutaneous cystolithotripsy procedure, a Foley catheter is left per urethra or per continent catheterizable stoma for 1 week. Laparoscopy and robotic-assisted laparoscopy have been used successfully in adults for remedy of calculi through the concomitant therapy of ureteropelvic junction obstruction and in the major treatment of staghorn calculi. Small collection using these strategies in kids have been described only more just lately. Of these instances, 4 had been accomplished robotically, with one affected person having a residual 6-mm lower pole stone and one affected person requiring conversion to an open process. Urinary stasis, bacterial colonization or infection with urea splitting organisms, retained mucus, and overseas our bodies all can contribute to the formation of bladder stones, most of that are struvite. However, regardless of encouraging results, concern remains concerning safety of endourologic treatment in smaller sufferers and its subsequent results on the rising kidney. Prospective studies designed to decide the "most popular" endourologic strategy to higher tract calculi in children would be helpful, albeit difficult to conduct. In this regard, individual surgeon expertise and comfort level weigh closely in choosing a treatment modality. Familiarity of pediatric urologists with percutaneous renal access and the total spectrum of endourologic tools and strategies will continue to facilitate efficacious, minimally invasive approaches to the entire pediatric urinary tract. Balancing the risks of radiation publicity for post-treatment stone detection and the risks of anesthesia for secondary procedures is a challenging dilemma for contemporary pediatric endourologists. Until the risks of radiation exposure in youngsters are extra clearly defined, surveillance in these children might be individualized based mostly on age, anatomy, stone burden, and underlying metabolic abnormalities.
Order prevacid 15 mg on-line
Palpable abdominal lots in infants and children: a report based on a evaluate of 653 instances gastritis symptoms vs ulcer symptoms safe prevacid 30 mg. Cortical microcystic illness of the kidney with dominant inheritance: a beforehand undescribed syndrome gastritis diet 5 days order 30 mg prevacid with mastercard. Acquired renal cystic disease in end stage renal illness: an post-mortem examine of a hundred and fifty five cases. Autosomal dominant polycystic kidney illness: latest advances in pathogenesis and potential therapies. Characterization of the nephrocystin-4 complex and subcellular localization of nephrocystin-4 to primary cilia and centromes. Localization of mutation producing autosomal dominant polycystic kidney illness with out renal failure. A novel gene that encodes a protein with a putative src homology 3 area is a candidate gene for familial juvenile nephronophthisis. Diagnostic puncture in renal cystic dysplasia (multicystic kidney): evidence on the aetiology of the cysts. Diverticular illness in patients with continual renal failure as a end result of polycystic kidney disease. Ambulatory blood stress monitoring in kids with unilateral multicystic dysplastic kidney. Postmenopausal estrogen remedy selectively stimulates hepatic enlargement in ladies with autosomal dominant polycystic disease. Treatment of renal cell carcinoma in von Hippel-Lindau disease: a multicenter research. Autosomal dominant polycystic kidney disease in infants: uneven disease mimicking a unilateral renal mass. Congenital anomalies of the kidney and urinary tract: position of loss of operate mutation within the pluripotent angiotensin type 2 receptor gene. Autosomal dominant polycystic kidney disease within the neonatal period: affiliation with arteriovenous malformations. The molecular foundation of focal cyst formation in human autosomal dominant polycystic kidney illness sort I. Clinical significance of acquired cystic illness of the kidneys in sufferers present process dialysis. Evaluation of ultrasonographic diagnostic criteria for autosomal dominant polycystic kidney disease 1. Epidemiology of renal and ureteral most cancers in Rochester, Minnesota 1950�1978, with special reference to clinical and pathologic features. Grey scale ultrasonography in medullary cystic disease of the kidney and congenital hepatic fibrosis with tubular ectasia: new observations. Management of hereditary pheochromocytoma in von Hippel-Lindau kindreds with partial adrenalectomy. Clinical and genetic characterization of pheochromocytoma in von Hippel-Lindau households. The gene mutated in autosomal recessive polycystic kidney illness encodes a big receptor-like protein. Somatic mutation in individual liver cysts helps a two-hit model of cystogenesis in autosomal dominant polycystic kidney illness. Ambulatory diagnostic analysis of 38 recurrent renal stone formers: a proposal for medical classification and investigation. In vitro proof from tissue cultures to prove existence of rabbit and human renotropic progress factor. Sirtuin 1 inhibition delays cyst formation in autosomal-dominant polycystic kidney disease. Rapamycin markedly slows illness progression in a rat model of polycystic kidney illness. Acquired cystic illness of the kidney in sufferers with end stage chronic renal failure: a research of prevalence and etiology. Is the risk of hypertension an indication for prophylactic nephrectomy in patients with unilateral multicystic dysplastic kidney Multilocular cysts of the kidney with intrapelvic herniation of a "daughter" cyst: report of four instances. Therapeutic impact of percutaneous puncture of simple renal cyst: follow-up investigation of fifty patients. Polycystic kidney illness and intracranial aneurysms: early angiographic analysis and early operation for the unruptured aneurysm. Risk evaluation of incidentally detected complex renal cysts in kids: potential function for a modification of the Bosniak classification. Obstructive nephrouropathies constitute the only largest entity leading to renal insufficiency in male youngsters younger than 1 12 months of age, and renal insufficiency is the biggest single explanation for renal failure needing transplantation, occurring in about 23% of kids present process transplant (Benfield et al, 2003; Seikaly et al, 2003). A large number of kids are affected by lesser levels of obstruction and may endure years of clinical monitoring and imaging research. The presence of an obstructive lesion is readily determined with present imaging, but the criteria for intervention stay controversial. This is essentially due to the absence of effective markers of the patterns and development of obstruction as properly as limited data concerning the natural history of differing degrees of obstruction (Chevalier, 2004). We are left with few guideposts along the spectrum of obstruction by which medical selections could additionally be made. This chapter will evaluation the present state of knowledge concerning the pathophysiology of congenital urinary obstruction, the means it may be correlated with clinical scenarios, and its distinction from postnatal obstruction. Obstructive hypertension appears to be renin mediated (Riehle and Vaughan, 1981; Urata et al, 1985; Mizuiri et al, 1992) and could also be reversible with surgical restore (de Waard et al, 2008). The pathologic correlates of those practical alterations have been described within the congenitally obstructed kidney to various degrees (Elder et al, 1995; Stock et al, 1995; Han et al, 1998; Poucell-Hatton et al, 2000; Zhang et al, 2000; Huang et al, 2006). The pathologic changes associated with lesser levels of obstruction have been much less thoroughly investigated, and a spectrum of qualitatively related alterations has been described. In the absence of overt useful alterations and in unilateral conditions, figuring out the state of the one affected kidney turns into a medical challenge. This problem is often tied to the question of whether or not surgical intervention is acceptable, and far controversy has emerged from this query. Clinical imaging research are presently the one extensively used modality to make this evaluation and their interpretation is variable. Progression could also be seen in two forms, one with the uncorrected partially obstructive lesion. In the first, renal function might initially seem intact on imaging tests, yet in time there will be progressive lack of absolute and relative perform of the kidney affected by the obstruction. If this have been identified prospectively, intervention would be acceptable and ought to be performed early. The problem is in predicting this situation, and few markers can be found to do this.
30 mg prevacid fast delivery
The definition of pathways and mechanisms of gubernacular growth and testicular descent downstream of hormone signaling are provided by transgenic mouse models and human syndromes with phenotypes that embody cryptorchidism (Barthold gastritis diet what to eat generic 15 mg prevacid with mastercard, 2008; Foresta et al gastritis breathing generic 15 mg prevacid amex, 2008). A theme that again emerges from these studies is the importance of myogenesis in gubernacular improvement. In mice, transgenic inactivation of genes together with Notch1 and several concerned in Wnt pathway signaling, together with Ctnnb1, Sfrp1, Sfrp2, Wnt5a, and Ror2, leads to marked disruption of fetal muscle patterning (Warr et al, 2009; Kaftanovskaya et al, 2011; Chawengsaksophak et al, 2012). Transgenic deletion of both of two homeobox genes, Hoxa10 and Hoxa11, is related to isolated cryptorchidism in mice (Satokata et al, 1995; Potter and Branford,1998) with evidence for delayed muscle growth within the Hoxa11 gubernaculum (Harisis et al, 2013). Also, the cremaster muscle is overdeveloped and associated with retractile testes in Esr1 knockout mice (Donaldson et al, 1996). Other transgenic mouse fashions that include the cryptorchid phenotype present insight into pathways required for testicular descent. These embrace targeted deletions of Tgfb2 (Sanford et al, 1997), Arid5b (Lahoud et al, 2001), Wt1 (Kaftanovskaya et al, 2013), Ptgds (Philibert et al, 2013), and Loxl1 (Wood et al, 2009) and spontaneous mutations of Ptch1 (Sweet et al, 1996) and Bmp5 (Green, 1968). Studies of rats with inherited cryptorchidism also recommend that innervation and/or muscle growth throughout the gubernaculum is disrupted (Hrabovszky et al, 2001; Barthold et al, 2008), and up to date three-dimensional images of the cryptorchid orl rat gubernaculum present muscle patterning defects (Barthold et al, 2014). The most constant perinatal components correlating with danger of cryptorchidism are prematurity and/or low birth weight for gestational age (Damgaard et al, 2008; Bay et al, 2011; Brouwers et al, 2012; Jensen et al, 2012). Epidemiology Cryptorchidism is probably certainly one of the commonest congenital anomalies, occurring in 1% to 4% of full-term and 1% to 45% of preterm newborn boys (Sijstermans et al, 2008). It is a part of almost 500 syndromes causally linked, based mostly on present data, to virtually 200 genes based on the Winter-Baraitser Dysmorphology Database ( The majority of cases are isolated, with the ratio of nonsyndromic to syndromic cryptorchidism reported as higher than 6: 1 in a big cohort (Boyd et al, 2006). Congenital Cryptorchidism Studies of the prevalence of isolated cryptorchidism at delivery are sophisticated by confounding factors that embrace subjectivity of the examination and variations in the definition of undescended testis (inclusion or exclusion of excessive scrotal testes), research populations, and experimental design (Sijstermans et al, 2008). Although most studies help a prevalence at birth of 2% to 4% and at three months of age of 1% to 2%, this varies geographically, with frequency as high as 9% in some research (Boisen et al, 2004; Virtanen and Toppari, 2008), supporting the potential for a rise over time. Perinatal risk elements most consistently related to cryptorchidism embody prematurity, low delivery weight or small dimension for gestational age, breech presentation, and maternal diabetes (Damgaard et al, 2008; Virtanen and Toppari, 2008; Jensen et al, 2012). In several population-based potential studies, the frequency of spontaneous descent by 3 months of age in boys recognized as cryptorchid at birth was reported as 50% to 87% (Berkowitz et al, 1993; Ghirri et al, 2002; Radpour et al, 2007; Wohlfahrt-Veje et al, 2009; Wagner-Mahler et al, 2011; van der Plas et al, 2013b). In smaller cohorts, spontaneous descent occurred in significantly extra Danish (68%) than Finnish (45%) boys at three months of age, presumably attributable to increased severity of the disease within the latter group (Suomi et al, 2006). In one other series, extrascrotal testes had been less prone to descend by 1 yr of age (50%) than high scrotal testes defined as cryptorchid at birth (87. In distinction, of ninety five cryptorchid infants referred to a urology apply, spontaneous descent occurred subsequently in 16% and 0% of these introduced earlier than and after 6 months of age, respectively (Wenzler et al, 2004). The decrease fee of descent in this collection could be associated to ascertainment age and severity of cryptorchidism in this referral population, as a result of spontaneous descent is widespread before 2 months of age (Kollin et al, 2013). Acquired Cryptorchidism In the past, cryptorchidism was considered a congenital anomaly identifiable at delivery. However, since first reported forty years ago (Myers and Officer, 1975), acquired cryptorchidism, or testes which might be recognized as cryptorchid after apparent full descent at start or in the neonatal period, is now totally accepted as a medical entity (Barthold and Gonzalez, 2003; Taghizadeh and Thomas, 2008; Acerini et al, 2009; Wohlfahrt-Veje et al, 2009; Hack et al, 2012). Acquired undescended testes are identified at an average age of 8 to eleven years and are more generally in a decrease place, related to a closed processus vaginalis and normal epididymis, than in instances identified as congenital. The cause for a later analysis stays unknown; theories include presence of a fibrous remnant of the processus vaginalis that tethers or foreshortens the twine over time or mobility of the testis inside an open sac (Keys and Heloury, 2012). These testes may be highly mobile and initially appear descended till somatic development ends in relative widening of the distance between testis and scrotum (Redman, 2005; Agarwal et al, 2006). Acquired cryptorchidism is reportedly extra widespread in boys with proximal hypospadias (Tasian et al, 2010; Itesako et al, 2011) and, like the congenital type, is associated with abnormal germ cell development (Rusnack et al, 2002). A prognosis of acquired cryptorchidism may be extra probably in boys with retractile testes, although testis retractility is widespread in normal populations. In a hospital-based study of unselected boys, the testis was initially suprascrotal on examination (retractile) in as much as 30% of boys at 4 years and 10% of boys 4 to 12 years of age but was intrascrotal in all boys over the age of 12 (Farrington, 1968). In population-based studies of wholesome boys, retractile testes have been present in 11% to 15% of boys as much as 11 years of age (WohlfahrtVeje et al, 2009; Goede et al, 2011) and 4% of 7- to 12-year-old boys (Inan et al, 2008). Both prospective and retrospective studies of the natural historical past of retractile testes support the idea that a subset of these turns into undescended over time. However, a selection bias exists in research of the risk of cryptorchidism in boys with retractile testes, because these referred for follow-up by specialists are doubtless these with essentially the most extreme retractility. For example, Wyllie prospectively studied a cohort of one hundred boys with unilateral retractile testis and identified 64 cases during which testicular place, as documented by the space between the pubic tubercle and midtestis and/or testicular dimension as estimated by orchidometer, was lowered after 5 years of follow-up (Wyllie, 1984). In retrospective case series it has been reported that cryptorchidism was identified in as a lot as 7% to 32% of boys with retractile testes adopted a mean of two. However, in a prospective study of 1072 boys, 520 of whom have been followed from birth to latest follow-up at 4. Although these data suggest an affiliation between retractile testes and cryptorchidism, the character of this association could reflect either difficulty in distinguishing the two entities or the truth that significant testicular retractility is a threat issue for acquired cryptorchidism. However, the smaller volume of retractile testes suggests a common pathogenesis (Goede et al, 2011). Careful serial physical examination is beneficial to accurately decide testicular position and identify cases of acquired cryptorchidism in boys with retractile testes. The true prevalence of acquired cryptorchidism is incompletely defined, as a outcome of longitudinal information that provide documentation of prior scrotal position are limited and tackle only the first few years of life. In one study, 742 infants were adopted with serial examinations for two years after birth, with complete follow-up in 326 (Acerini et al, 2009). The variety of suprascrotal testes recognized at birth in this sequence (10) was the same because the number diagnosed subsequently (10), though almost half the boys have been lost to follow-up during the research. In one other examine, 1072 boys had been adopted with serial examinations from birth to four. The prevalence of congenital cryptorchidism (including excessive scrotal testes) was 9% at birth but dropped to 1% at 18 months, whereas 8 (1. Acquired cryptorchidism most likely represents a milder presentation of congenital cryptorchidism that escapes detection in infancy. Genetic Susceptibility Genetic studies of cryptorchidism counsel that the illness is heritable, however that susceptibility is in all probability going polygenic and multifactorial. Clustering of cryptorchidism has been reported in numerous families affecting a number of individuals in the same generation and variable phenotype (Minehan and Touloukian, 1974; Pardo-Mindan et al, 1975; Czeizel et al, 1981; Savion et al, 1984). Familial aggregation suggesting reasonable genetic threat was reported in a large cohort study of more than 1 million male births in the Netherlands based mostly on intensive hospital registry data (Schnack et al, 2008). Another population-based research in Denmark, using totally different methodology, recognized higher concordance charges of cryptorchidism diagnosis in maternal (6%) than in paternal (3. Incomplete testicular descent was reported in Tgfb2-/- mice (Sanford et al, 1997) but not in Tgfbr3-/- mice, which not often survive past start. In summary, research to date are in preserving with the assumption that cryptorchidism is a genetically advanced illness, doubtless related to multiple susceptibility loci. Failure to determine consistent loci associated with cryptorchidism is most likely going related to methodology, notably insufficient sample measurement, phenotypic variability, and other confounding components similar to environmental influences. Therefore, though multiple genetic variants probably contribute to the risk of nonsyndromic cryptorchidism, most remain unknown presently.