
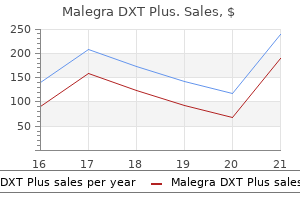
Malegra DXT Plus dosages: 160 mg
Malegra DXT Plus packs: 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Malegra dxt plus 160 mg order otc
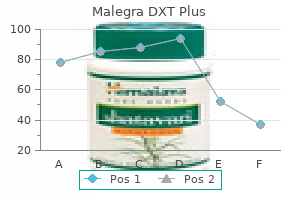
Fifth causes of erectile dysfunction in 40s malegra dxt plus 160 mg purchase otc, venous outflow from tissues converges in the pulmonary artery erectile dysfunction treatment patanjali discount 160 mg malegra dxt plus, and sixth, the blended venous blood passes through alveolar capillaries the place it once more equilibrates with alveolar gases. Gas circulate from the anesthesia machine into the respiration circuit is unidirectional. In transfers from the anesthesia machine (the contemporary gas outlet) to breathing circuit and then to alveolar airspace, anesthetic circulate can merely be understood as exchange from upstream compartments into downstream compartments. In later steps, such as exchange between alveolar gases and pulmonary capillary blood, flow of anesthetic molecules happens through diffusion between adjoining compartments separated by a permeable membrane. Distribution of anesthetic to and from varied tissues involves both bulk switch via blood flow Downloaded for alex arman davidson (arman@amazingstudy. Effective volumes are calculated as tissue volume � tissue/blood and exchange time constant for each compartment is Veff/blood move. The physiological volumes of the tissue compartments are roughly in proportion to the labeled face of the compartment, whereas the blood-tissue partition coefficients are depicted as the depth of the compartment. Relative blood circulate is approximately proportional to the width of the arrows into and out of tissue compartments, as nicely as for shunts. Quantitative modeling of anesthetic gas motion on this system was performed utilizing numerical integration of equations describing anesthetic flow into and out of each compartment (Eqs. Note that when anesthetic transfer happens between gasoline and blood or between blood and tissue, the effective volume of the downstream compartment must be adjusted with the suitable partition coefficient (see Table 20. Rate of Wash-In of the Circuit: Equilibration Between Vaporizer and Circuit Equipment for controlled supply of inhaled anesthetic medication are described elsewhere on this text (see Chapter 22). Wash-in of the ventilator respiration circuit represents an example of bulk switch exchange, wherein the gas in circuit components is replaced by recent gases emerging from the fuel outlet of the anesthesia machine. Conversely, if the Vcirc doubles to 12 L, then wash-in will proceed at half the speed (doubling the time). The fuel change process is impartial of the concentration of anesthetic within the circuit, as a result of the trade is just by way of bulk flow and mixing. However, the difference between the delivered concentration and that in the circuit determines the magnitude and path of internet anesthetic gasoline move. When the delivered anesthetic partial stress (Pdel) is bigger than that in the circuit (Pcirc), internet anesthetic flow is into the circuit (and subsequently the patient). Cross marks overlaying the curves indicate time constants under totally different fuel flow charges. Each minute leads to the fraction of old fuel within the breathing circuit dropping by 63. The half-life for the process (time for halving the vaporizer-circuit focus difference) is zero. Open (nonrebreathing) anesthetic respiration circuits are designed to have low exchange volumes and to be used with excessive fresh-gas flows. These options allow speedy changes within the delivered anesthetic focus, while minimizing rebreathing of exhaled gases. The selection of an open versus Equilibration Between Circuit and Pulmonary Airspace Transfer of anesthetic gases from the respiratory circuit to the pulmonary airspace is another bulk exchange process similar to that from vaporizer to respiration circuit. The anesthetic gas within the respiratory circuit represents a mixture of recent gas and exhaled gases. Right, A extra widespread scientific state of affairs with fixed vaporizer output (Pdel) and partial rebreathing at a 6 L/ min contemporary gas move price. Raising minute air flow accelerates the rise of Palv by delivering extra anesthetic to the lungs. However, the relative dimension of the ventilation effect is larger for soluble brokers. Increased air flow also accelerates clearance of anesthetic brokers after delivery ceases. Dead house (ventilated however not perfused pulmonary regions) reduces effective alveolar air flow (see Eqs. Left, A traditional open-circuit model with very excessive recent gas flows and due to this fact constant Pdel = Pcirc. Increasing cardiac output slows the rise of Palv by growing anesthetic uptake into blood (removing anesthetic from alveolar gases). Cardiac output additionally affects clearance of anesthetics from the lungs in the same way it affects uptake. As blood solubility (b/g) increases, the rate of rise in Palv slows, as a outcome of uptake into blood is greater for top solubility brokers. The major influence of blood solubility is the magnitude of the speedy preliminary rise in Palv, which represents a stability between anesthetic supply and uptake into pulmonary blood. Blood solubility similarly impacts clearance from alveoli after anesthetic delivery ceases. Pcirc, Anesthetic partial strain within the breathing circuit; Pdel, delivered anesthetic partial strain from the anesthesia machine fuel outlet. Pulmonary proper to left shunting can be physiologic, pathologic, or iatrogenic, similar to throughout one-lung ventilation. This is because arterial blood represents a mix of shunted mixed venous blood mixed with blood that has equilibrated with alveolar gases (Eq. Because such shunts also cut back transcapillary fuel trade within the lung and gradual anesthetic uptake (Eqs. The absolute focus of anesthetic influences its uptake and that of other gases. In the earlier discussion and illustrations, it was presumed that an inhaled anesthetic represents a small fraction of the inhaled gas combination and that transalveolar uptake of the anesthetic leads to a lower in Palv and negligible changes in alveolar fuel volume. However, when the anesthetic represents a big fraction of the inhaled gas mixture, its fast uptake results in a smaller relative alveolar anesthetic concentration drop, as a outcome of the volume of alveolar gas also decreases. Assuming cardiac output equals 5 L/min, the preliminary fee of N2O uptake is given by Eq. If we assume that half the N2O and half the isoflurane are quickly taken up following the first breath of this gas mixture, then alveolar quantity drops by 33. The curves represent anesthetic partial pressures in alveolar gases (dashed lines) and arterial blood (dash-dot lines) under conditions of 40% right-to-left shunt and no shunt (solid lines). Pulmonary right-to-left shunting bypasses alveolar uptake, so less anesthetic is faraway from pulmonary gases; this accelerates the rise in Palv. Thus Part, which determines the rate of anesthetic uptake into tissues, rises more slowly than Palv when R-to-L shunting is current. Inhaled fuel combination Additional fuel combination replaces lost quantity 1% Iso 33% O2 66% N2O zero. After an preliminary inspiratory breath, alveoli are filled with the gasoline combination in the circuit (66% N2O, 33% O2, 1% Isoflurane) at their regular end-inspiratory quantity (left panel). After half of the N2O and isoflurane are absorbed into pulmonary blood, the alveolar gas quantity is lowered by 33. At this level, the quantity of N2O equals the amount of O2 and the gas mixture is forty nine. Inflow of additional impressed gasoline combination returns alveolar volume to its unique worth, leading to a gas mixture of fifty five. The alveolar partial stress of N2O falls a lot lower than the fractional uptake (the focus effect).
Cheap malegra dxt plus 160 mg on-line
Actin in motion: the interplay between the actin cytoskeleton and synaptic efficacy erectile dysfunction causes cancer 160 mg malegra dxt plus order overnight delivery. The function of protein synthesis in memory consolidation: progress amid a long time of debate erectile dysfunction at age 21 160 mg malegra dxt plus cheap amex. The role of reconsolidation and the dynamic process of long-term reminiscence formation and storage. Extinction-reconsolidation boundaries: key to persistent attenuation of fear memories. Coherent theta oscillations and reorganization of spike timing within the hippocampalprefrontal community upon studying. Hypothesis: suppression of memory protein formation underlies anesthetic-induced amnesia. Bilateral inhibition of gamma-aminobutyric acid type A receptor operate within the basolateral amygdala blocked propofol-induced amnesia and activity-regulated cytoskeletal protein expression inhibition within the hippocampus. Research on attention networks as a mannequin for the mixing of psychological sci. Propofol disrupts functional interactions between sensory and highorder processing of auditory verbal memory. Midazolam decreases cerebral blood move in the left prefrontal cortex in a dose-dependent style. Event-related useful magnetic resonance imaging of a low dose of dexmedetomidine that impairs long-term reminiscence. The effect of sedation on cortical activation: a randomized research comparing the results of sedation with midazolam, propofol, and dexmedetomidine on auditory processing. Are event-related potential parts generated by phase resetting of brain oscillations Differentiating the results of centrally performing medication on arousal and reminiscence: an event-related potential study of scopolamine, lorazepam and diphenhydramine. The P300 eventrelated potential throughout propofol sedation: a attainable marker for amnesia Drug-induced amnesia is a separate phenomenon from sedation: electrophysiologic proof. Visual p2-n2 complicated and arousal at the time of encoding predict the time domain traits of amnesia for multiple intravenous anesthetic drugs in humans. Propofol and midazolam inhibit aware reminiscence processes very soon after encoding: an event-related potential study of familiarity and recollection in volunteers. Sequential results of accelerating propofol sedation on frontal and temporal cortices as listed by auditory event-related potentials. Effect of propofol anaesthesia on the event-related potential mismatch negativity and the auditory-evoked potential N1. Learning, reminiscence and synaptic plasticity in hippocampus in rats exposed to sevoflurane. Propofol inhibits long-term potentiation but not long-term melancholy in rat hippocampal slices. Inhibition of glutamatergic activation of extracellular signal-regulated protein kinases in hippocampal neurons by the intravenous anesthetic propofol. Etomidate targets alpha5 gamma-aminobutyric acid subtype A receptors to regulate synaptic plasticity and memory blockade. Bicuculline administered into the amygdala after training blocks benzodiazepine-induced amnesia. Propofol enhances memory formation by way of an interplay with the endocannabinoid system. Effects of ketamine, dexmedetomidine and propofol anesthesia on emotional memory consolidation in rats: consequences for the development of post-traumatic stress dysfunction. Fear conditioning, synaptic plasticity and the amygdala: implications for posttraumatic stress dysfunction. Exposure to excessive stress in the intensive care unit could have unfavorable effects on healthrelated quality-of-life outcomes after cardiac surgery. Learning during general anaesthesia: implicit recall after methohexitone or propofol infusion. Midlatency auditory evoked potentials and express and implicit memory in sufferers present process cardiac surgical procedure. Implicit reminiscence for words played during isoflurane- or propofol-based anesthesia: the lexical determination task. Analysis of reminiscence formation throughout common anesthesia (propofol/remifentanil) for elective surgical procedure using the process-dissociation process. A new degraded auditory stimulus test to measure implicit reminiscence during anaesthesia in youngsters. Implicit reminiscence formation throughout routine anesthesia in kids: a double-masked randomized controlled trial. Implicit memory formation utilizing the word stem completion task throughout anesthesia in kids. Short-term memory impairment after isoflurane in mice is prevented by the alpha5 gammaaminobutyric acid sort A receptor inverse agonist L-655,708. Inhibition of alpha5 gammaAminobutyric acid kind A receptors restores recognition reminiscence after general anesthesia. Gamma-aminobutyric acid sort A receptor alpha 4 subunit knockout mice are resistant to the amnestic effect of isoflurane. Gamma-aminobutyric acid kind A receptor beta3 subunit forebrain-specific knockout mice are immune to the amnestic effect of isoflurane. Slowing of the hippocampal theta rhythm correlates with anesthetic-induced amnesia. Cholinergic manipulations within the medial septal area: age-related results on working memory and hippocampal electrophysiology. Noradrenergic modulation of basolateral amygdala neuronal activity: opposing influences of alpha-2 and beta receptor activation. Glucocorticoid enhancement of reminiscence requires arousal-induced noradrenergic activation in the basolateral amygdala. Interactions between epinephrine, ascending vagal fibers, and central noradrenergic methods in modulating memory for emotionally arousing events. Systemic or intra-amygdala infusion of the benzodiazepine, midazolam, impairs learning, but facilitates re-learning to inhibit concern responses in extinction. Basolateral amygdala lesions block diazepam-induced anterograde amnesia in an inhibitory avoidance task. Lesions of the basolateral amygdala complicated block propofol-induced amnesia for inhibitory avoidance learning in rats. Characteristics of sleep could be quantified using questionnaires, actigraphy, or respiratory polygraphy. However, polysomnography, together with electroencephalogram, electrooculogram, submental electromyogram, and evaluation of breathing, is required to describe the cortical characteristics and quick physiological penalties. Activation of hypothalamic sleep-promoting pathways together with the ventrolateral preoptic nucleus and the median preoptic nucleus produces the physiological swap from wakefulness to sleep.
160 mg malegra dxt plus purchase with amex
Department of Transportation reveal that the greatest variety of single-vehicle accidents takes place during the early morning hours when people are at a circadian lull of alertness what causes erectile dysfunction treatment safe 160 mg malegra dxt plus. These accidents are thought to result from inadvertent lapses in driver attention brought about by extremes of sleepiness impotence pumps malegra dxt plus 160 mg discount visa. When environmental stimuli wane, physiologic sleepiness manifests itself as an awesome propensity to fall asleep. The most excessive reason for impaired vigilance is the occurrence of actual sleep episodes (microsleeps) encroaching into periods of wakefulness. They are intermittent in onset, and their impending occurrence is tough for the individual to predict. Most people underestimate their level of sleepiness when they can be objectively shown to be extraordinarily sleepy, thus making this downside much more insidious. This has important which means within the office and when driving residence after lengthy work durations. Microsleeps are an indication of maximum sleepiness and are harbingers of the onset of longer sleep durations. Typically, they occur in periods of low workload or stimulation and when a person is maximally sleepy. The sleepextended situation was included to present a real management state of maximal relaxation and optimum alertness. Ironically, though the on-call durations occurred throughout rotations that often have very busy call nights, only a few subjects have been, in reality, awake a lot of the evening. These data also point out that underneath normal working situations, the resident physicians 6 � Avoiding Patient Harm in Anesthesia: Human Performance and Patient Safety 133 studied had been physiologically sleepy to nearly pathologic ranges. Notably, these information cast substantial doubt on earlier studies of the efficiency of medical personnel that have relied on the idea that individuals working under regular circumstances are really rested. The beforehand mentioned examine also investigated the connection between subjective and physiologic sleepiness. The authors additionally found that subjects demonstrated little capacity to decide whether they had actually fallen asleep. These outcomes help the contention that medical personnel are physiologically susceptible to degraded alertness yet are unable to perceive this decrement. Thus, an anesthesia skilled might, actually, fall asleep throughout a case, awaken, and be completely unaware of the lapse in vigilance. Long work hours, fatigue, and sleep deprivation have been shown to bring about consistent and dramatic modifications in temper and emotions. Depression, anxiousness, irritability, anger, and depersonalization have all been proven to enhance throughout testing of chronically fatigued house employees. These emotions are an obvious source of stress between anesthesia professionals and their co-workers, sufferers, and families. The relationship of temper, performance, and patient security has but to be decided. Sleep inertia corresponds to the interval of lowered capacity to function optimally instantly on awakening. This phenomenon often occurs when people are awakened out of slow-wave sleep and is manifested as grogginess and impaired performance lasting so long as 15 to half-hour after awakening. Sleep inertia can even happen after being awakened from regular sleep and is commonest during the early morning circadian trough (2 to 6 am). Depending on the preexisting stage of sleepiness, people who take naps longer than forty minutes are at greater danger for sleep inertia on awakening. If pressing work could be anticipated, the sleeping particular person must be awakened with adequate time (at least 15 minutes) to decrease the fogginess and decrement in efficiency associated with sleep inertia. Another option is to not sleep longer than quick naps in conditions where immediate efficiency is required. If sleep inertia is unavoidable, it might be wise for the affected individual to ask for help till the grogginess dissipates. It is extremely unsure as to whether, how, or in what circumstances these established psychophysical adjustments may interact with clinical work processes to affect patient safety in anesthesiology. Sinha and colleagues ask: "The fatigued anesthesiologist: A threat to patient safety Even in well being care, studies have largely been carried out in hospital ward settings where, during night on-call shifts, they might have accountability for lots of patients. Critical events are unusual, and even when the chain of accident evolution has begun, the scientific group will probably have multiple alternatives to detect and correct it earlier than any substantive adverse influence has occurred. Thus, whereas anesthesia personnel may be prone to fatigue, and complaints about sleepiness and fatigue are frequent, the probability of a adverse affected person end result during anesthesia directly attributable to sleepiness alone may be very small. Conversely, measures and methods that do handle such factors are by nature non-quantitative and invasive. Secondary task probe response instances were slower after sleep deprivation, although this reached statistical significance for solely one of three probe types. No statistical distinction in case management between circumstances was reported-in fact, topics in both circumstances made vital errors. Sleep-deprived topics cycled (often rapidly) in and out of sleepy behavior, and essentially the most impaired individuals showed such habits for more than 25% of the experiment (60 minutes). Rather they usually cycled incessantly in and out of states of obvious wakefulness, drowsiness, and microsleeps all through the simulated case. Typically, when awake their efficiency was at most mildly degraded but when they showed excessive drowsiness or were really asleep their performance was essentially zero. Participants have been observed being totally asleep at one moment however awakening simply in time to occur to catch a probe stimulus or clinical event, and respond to it satisfactorily. For most topics the fraction of time spent in extremely impaired states was low as their microsleeps have been brief, in part as a result of even a quiet routine clinical setting has a selection of stimuli, including different personnel and their tasks. Strategies that institutions or practitioners can use to decrease the unfavorable effects of sleepiness and fatigue on efficiency embody: training and promotion of safety culture, improved sleep habits, relaxation breaks at work, strategic napping, medicines and social medication, and lightweight remedy. Strategies that national bodies and professional societies and organizations can name for are reasonable obligation hour necessities. One direct regulatory technique to reduce sleep deprivation has been to restrict the work hours of clinicians. For essentially the most part this has been tried just for these in coaching (who historically have labored very lengthy hours both in the course of the day and in nighttime on-call). Results of process and outcome research have various however there was no proof that such regulations, by themselves, improve affected person security. The previous studies offered addressed the effects of sleep deprivation and fatigue on physician efficiency and well-being. A first and comparatively simple and inexpensive step in addressing sleepiness and fatigue of medical personnel is to educate practitioners and the administrators of well being care institutions concerning the impression of sleep issues on work efficiency, temper, job satisfaction, and health. Educational packages masking sleep deprivation, circadian disruption and fatigue, and countermeasures have been enthusiastically adopted by an growing fraction of the aviation neighborhood. Other competing forces, for example measures of production versus security, are very highly effective and difficult for practitioners to manage. Only if fatigue is seen as an organizational issue affecting security negatively and security is made a high organizational priority with all the resulting consequences, will fatigue-related questions of safety be minimized. For additional countermeasures also see the Sentinel Event Alert of the Joint Commission255 launched earlier.
160 mg malegra dxt plus with amex
Implantable cardioverter-defibrillator remedy earlier than dying: excessive threat for painful shocks at end of life erectile dysfunction rates malegra dxt plus 160 mg effective. Discontinuing pacemakers erectile dysfunction doctors in orange county 160 mg malegra dxt plus discount fast delivery, ventricular-assist gadgets, and implanted cardioverter-defibrillators in end-of-life care. Attitudes of cancer patients, household care givers, oncologists and members of most of the people towards critical interventions at the finish of life of terminally unwell patients. A definition of irreversible coma: a report of the ad hoc committee of the Harvard School of Medicine to study the definition of mind death. Non�Heart Beating Organ Transplantation: Medical and Ethical Issues in Procurement. A matter of life and dying: what each anesthesiologist ought to know in regards to the medical, authorized, and ethical elements of declaring brain death. Voluntary assent in biomedical research with adolescents: a comparison of parent and adolescent views. Too late for luck: a comparability of postFurman exonerations and executions of the innocent. American medical association council on moral and judicial affairs: Code of medical ethics opinion 9. Conscientious objection, professional responsibility and compromise: a response to Savulescu and Schuklenk. Conscientious objection to abortion and reproductive healthcare: a review of recent literature and implications for adolescents. Anesthetics act at structures in the brainstem, hypothalamus, and basal forebrain that regulate sleep-wake states, which may account for lack of wakefulness. Anesthetics disrupt connectivity and communication across cortical and thalamocortical networks, which can account for loss of consciousness. Memory can be subdivided into explicit (conscious) and implicit (unconscious) recall; an instance of specific episodic recall is remembering a surgical event. Suppression of explicit episodic recall is probably considered one of the most potent effects of most general anesthetics. Effects on the hippocampus, amygdala, and prefrontal cortex-as properly as the connectivity of these structures-may account for anesthetic-induced amnesia, even earlier than loss of consciousness. The richness of human consciousness and memory-and the flexibility to express this richness in language-is a defining attribute of homo sapiens. Consciousness and reminiscence also have scientific relevance for the anesthesiologist; together, the expertise and specific episodic recall of surgical events is called the problem of "intraoperative awareness. Awareness: Cognitive neuroscientists and philosophers use the time period "awareness" to mean solely subjective experience. In clinical anesthesiology, we (inaccurately) use the term "consciousness" to embody both consciousness and express episodic memory7 (the taxonomy of memory will be mentioned within the next main part of the chapter). Connected versus disconnected consciousness: Connected consciousness is the experience of environmental stimuli (such as surgery), whereas disconnected consciousness is an endogenous experience (such as a dream state). Consciousness versus responsiveness: An individual could fully experience a stimulus (such because the command "Open your eyes! Advances in neuroscience, however, have enabled us to transfer beyond speculative frameworks and concentrate on a systems-based strategy to each topics. There are, nonetheless, a quantity of essential definitions and distinctions that must be thought of. Multiple neurochemical systems in subcortical regions (shown here in rodent brain) promote arousal and activation of the cortex. Monoaminergic neurons (light green) in the rostral brainstem and caudal hypothalamus innervate the cortex as properly as many subcortical regions together with the hypothalamus and thalamus. These monoaminergic areas include noradrenergic neurons (locus coeruleus), serotonergic neurons (dorsal and median raphe nuclei), dopaminergic neurons (ventral tegmental area), and histaminergic neurons (tuberomammillary nucleus). Wake-promoting signals also arise from cholinergic regions (dark green with hatching), together with the pedunculopontine and laterodorsal tegmental nuclei and basal forebrain. The following is a description of select subcortical nuclei within the brainstem and hypothalamus that mediate sleep-wake cycles14 and, potentially, some traits of anesthesia. When pentobarbital is microinjected on this area, a reversible state with anesthetic traits is induced. Studies of the dopamine agonist methylphenidate have revealed a capability to reverse the sedative results of both isoflurane and propofol. The anterior hypothalamus has long been hypothesized to play a task in sleepwake regulation. Orexinergic neurons are discovered in the lateral hypothalamus and supply an essential arousal stimulus for the cortex. There are two types of orexin (A and B), which are additionally referred to as hypocretins. Orexins attenuate the results of isoflurane,64 propofol,65 ketamine,sixty six and barbiturates,67 utilizing numerous measures. Additionally, the thalamus is important for transmitting arousal indicators from the brainstem and for regulating cortical communication. The involvement of the thalamus in arousal, sensory processing, and cortical computation is in all probability going critical for regular consciousness. As such, the thalamus has been of continued curiosity to those investigating mechanisms of anesthetic-induced unconsciousness. The hyperpolarization of the thalamus would shift tonic firing to burst firing that-as with sleep-would forestall afferent sensory stimuli from arousing the cortex. Importantly, however, sensory nuclei within the thalamus (and their connectivity to the cortex) seem to be less concerned in anesthetic-induced unconsciousness compared to the higher-order or "nonspecific" nuclei. Central thalamic activation ends in behavioral improvement in humans with traumatic mind damage. Other case studies in people suggest concurrent suppression of thalamus and cortex during induction of propofol. The potential position of the striatum (composed of the putamen and caudate) in anesthetic-induced unconsciousness has been demonstrated in a examine of rats present process isoflurane anesthesia. Sleep is clearly generated via such bottom-up mechanisms14; nonetheless, anesthetics might suppress the extent of consciousness via bottom-up mechanisms and content of consciousness by way of top-down. The thalamocortical system undergoes state-dependent changes throughout the sleep-wake cycle, and is assumed to play a crucial position in consciousness. One examine identified a propofolinduced disruption of connectivity between the thalamus and lateral frontal-parietal networks. The discovering of impaired thalamocortical connectivity in affiliation with anesthetic-induced unconsciousness has not been common. Relative to the control state of wakefulness (left column), sedation (middle panel) is marked by an increase of local/regional signal synchrony and consequent breakdown of global connectivity.
Diseases
- Proximal myotonic dystrophy
- Leishmaniasis
- Anophthalmia cleft lip palate hypothalamic disorder
- Osteochondritis deformans juvenile
- Daentl Towsend Siegel syndrome
- Phenobarbital antenatal infection
Buy discount malegra dxt plus 160 mg on-line
Provide an built-in platform for displaying anesthetic erectile dysfunction injection drugs malegra dxt plus 160 mg on line, hemodynamic erectile dysfunction urinary tract infection best malegra dxt plus 160 mg, and respiratory parameters, and for collecting this data into an digital medical record. Understanding the anesthetic workstation is essential as a result of the workstation is probably considered one of the most important items of equipment used by anesthesia care suppliers. Many workstations and their components share very similar characteristics, but the variation among them is growing. Similarly, the operational and pre-use checkout procedures are becoming more divergent, thus mandating device-specific familiarity. Unfortunately, a lack of know-how pertaining to the anesthesia workstation and a lack of know-how and utility of a correct pre-use check are common. However, as a end result of anesthesia workstations must adhere to fundamental requirements, a generic method to all machines might be presented. Although a number of subsystems are described in detail on this chapter, anesthesia providers should purchase a useful understanding of their very own workstations and make sure that their native pre-use checkout procedures are suitable for his or her machines. This article will evaluate tips for anesthesia workstations; functional anatomy including fuel supply, vaporizers, respiration circuits, ventilators, and scavenging; and the anesthesia machine pre-use checkout. Standards and Guidelines for Anesthesia Workstations Standards for medical gadgets and anesthesia workstations present tips for manufacturers relating to device minimal performance, design characteristics, and safety necessities. Additional key requirements for machine subsystems come up from the Compressed Gas Association and the Institute of Electrical and Electronics Engineers. The focus of this chapter is on design and useful elements of the anesthesia workstation related to the supply of inhaled anesthesia. The high-pressure system extends from the gas cylinders to the high-pressure regulators (dashed strains round O2 high-pressure section only). The intermediate-pressure part extends from the high-pressure regulators to the move management valves and also contains the tubing and components originating from the pipeline inlets. The gas supply system consists of the following parts: oxygen, air, and nitrous oxide might enter the anesthesia machine from both the hospital gasoline pipeline system, or from E-cylinders mounted on the back of the anesthesia machine. There are numerous safety mechanisms in place along this path to keep away from delivering a hypoxic gas combination on the fresh gasoline outlet. The gas supply system can be divided into three sections: high-pressure, intermediate-pressure, and low-pressure. The solely high-pressure parts within the anesthesia machine are the auxiliary gas tanks (E-cylinders) on the again of the anesthesia machine. The stress in these tanks (approximately 2000 pounds per square inch gauge [psig] for air and oxygen, 745 psig for nitrous oxide) is instantly stepped all the means down to an intermediate stress. The low-pressure part begins on the flowmeter control valves, contains the flowmeters and anesthetic vaporizer, and ends on the contemporary gas outlet. The low-pressure part (dashed lines) extends from the circulate control valves to the respiration circuit. Many machines have up to three and typically four E-cylinder attachment points to accommodate oxygen, air, and nitrous oxide. The hanger yoke meeting orients and safely helps the cylinder, offers a gastight seal, and ensures unidirectional flow of gases into the machine. Two steel pins on the yoke assembly are arranged to project exactly into corresponding holes on the cylinder head�valve assembly of the tank. Conditions by which failure occurred have included the next: excessive seating (jamming) of the pins again into the hanger yoke; the presence of bent or broken pins; and an excessive use of washers between the cylinder and the yoke that may override pin alignment, but enable for a gas-tight seal. The maximum strain in full Ecylinders (approximately 750 psig for nitrous oxide, 2200 psig for air, and 2200 psig for oxygen) is far larger than the normal hospital pipeline provide strain of fifty to 55 psig. The lower strain is a security function: if each the E-cylinder and the oxygen pipeline are linked and the E-cylinder is open, the anesthesia machine will draw its gasoline from the pipeline somewhat than the E-cylinder, thereby preserving the contents of the E-cylinder in case of pipeline failure. Fluctuations within the pipeline stress beneath 40 to 45 psig may enable the E-cylinder to be drained, as may silent leaks in the high-pressure system, so E-cylinders ought to be closed during regular operation. If the anesthesia machine permits two oxygen E-cylinders to be mounted on a common manifold, then each mount should have a examine valve. On some machines, a single excessive strain regulator is downstream from the 2 examine valves; on others, every mount on the manifold has its own high stress regulator and examine valve. In either configuration, transfer of gasoline from a full tank to an empty tank is prevented, and the system allows for a cylinder to be exchanged whereas the opposite cylinder on the manifold continues to provide gas to the anesthesia machine. The pressure in each of the gasoline pipelines and each of the auxiliary E-cylinder manifolds must be displayed on the entrance of the anesthesia machine. The E-cylinder pressures are correct only when the tank is open; within the case of a two-tank manifold, the stress of the open tank with higher stress shall be displayed. In methods with digital stress displays, the pipeline and tank pressures are visible only when the machine is on. The practitioner should manually open each cylinder and check the strain gauges on the entrance of the machine. In the case of a two-tank oxygen manifold, the tanks should be serially opened and checked. The oxygen flush valve may be used to vent the stress from the system after closing the first tank, so the pressure within the second tank could be precisely assessed. An open oxygen cylinder could enable the anesthesiologist to be unaware of catastrophic pipeline failure. When the oxygen cylinder is closed, the quick result of oxygen pipeline failure is a low oxygen strain alarm. The auxiliary E-cylinder can then be opened, ensuring continued move of oxygen to the patient while troubleshooting happens. Indexing is achieved by way of differing diameters of the connection parts, resulting in key-like fitting when matched connectors come together. The oxygen connector is moreover distinguished from the opposite gas connectors by a unique threaded fitting diameter and a singular thread rely. In this case, the low oxygen strain alarm only happens as quickly as the auxiliary tank has been depleted, nullifying the utility of the backup system. The primary provide supply of oxygen in a large hospital often is a large cryogenic bulk oxygen storage system. Smaller hospitals may use liquid oxygen tanks that could be changed rather than refilled on site, or maybe a financial institution of oxygen H-cylinders related by a manifold. Centrally supplied nitrous oxide arises both from a bank of H-type cylinders, or a bulk liquid storage system much like that for oxygen. Within each sort, the connectors for oxygen, air, and nitrous oxide are mutually incompatible, which helps to reduce the potential for connecting to the wrong fuel. Quick couplers, like Diameter Index Safety System connectors, are used for noninterchangeable, detachable medical gas, suction, and waste fuel connections. Indexing is completed by the configuration of pins on one plate which match to recesses on the opposite plate (shown). Once the gasoline enters the machine, it encounters a filter adopted by a pipeline check valve.
Malegra dxt plus 160 mg generic amex
Flows can be displayed numerically or generally graphically within the type of a digital zantac causes erectile dysfunction malegra dxt plus 160 mg buy generic online, digitalized flowmeter erectile dysfunction pills at gnc discount 160 mg malegra dxt plus with amex. Numerous forms of move sensor applied sciences could be utilized, corresponding to hot-wire anemometers, a differential pressure transducer methodology, or mass circulate sensors. The illustrated system relies on the principle of particular warmth to measure fuel circulate. The amount of vitality required to preserve the temperature is proportional to the move and specific heat of the fuel. Regardless of the mechanism of move measurement, these techniques depend upon electrical energy to present a show of gas move. When electrical power is completely interrupted, some backup mechanical means often exists to control (mechanical flow control) and show (flow tube) oxygen gasoline move. Mechanical move management and circulate show still stay common, even on some newer workstations, both as main or backup systems. The location of the needle valve within the valve seat changes to establish completely different orifices when the move management valve is adjusted. Gas move increases when the flow management valve is turned counterclockwise, and it decreases when the valve is turned clockwise. The oxygen move management knob is physically distinguishable from the opposite gas knobs. It is distinctively fluted, could project beyond the control knobs of the other gases, and is bigger in diameter than the flow control knobs of other gases. Flow management knobs are recessed or protected with a shield or barrier to decrease inadvertent change from a preset place. If a single fuel has two move tubes, the tubes are arranged in sequence and are controlled by a single circulate management valve. With a standard flowmeter assembly, the circulate control valve regulates the quantity of move that enters a tapered, transparent circulate tube known as a variable orifice flowmeter or Thorpe tube. A cellular indicator float inside the calibrated move tube indicates the amount of move passing via the associated move management valve. The clearance between the top of the float and the circulate tube is named the annular area. It could be thought of equal to a round channel of the same cross-sectional space. The oxygen flowmeter assembly consists of the move control valve assembly and the flowmeter subassembly. The indicator float hovers freely in an equilibrium position in the tube the place the upward pressure ensuing from gas circulate equals the downward gravity pressure on the float at a given flow price. These flowmeters are commonly referred to as constant-pressure flowmeters as a result of the lower in strain throughout the float remains fixed for all positions within the tube. The characteristics of a fuel that affect its move price via a given constriction are viscosity (laminar flow) and density (turbulent flow). Because the annular area behaves as a tube at low flow rates, laminar circulate is present, and viscosity determines the gasoline circulate rate. Because the viscosity and density of the fuel affect flow by way of annular space across the float, the calibrated move tubes are fuel specific. Viscosity is dominant in determining the gasoline circulate rate through this tubular constriction. Density is dominant in figuring out the gasoline circulate rate by way of this orificial constriction. A cease on the prime of the flowmeter tube prevents the float from occluding the outlet. Two flowmeter tubes are generally placed in series, with a nice move tube displaying low flows and a rough flow tube indicating greater flows. Anesthesia workstations are equipped with an oxygen failure protection gadget within the intermediate-pressure part that, in response to reduced oxygen pressure, either proportionally reduces or fully inhibits nitrous oxide. On anesthesia workstations with electronically controlled fuel flow, the machine is programmed to forestall the person from choosing a hypoxic gasoline mixture for supply to the recent gas outlet. For mechanically managed flowmeters, the priority is that a consumer could mistakenly select oxygen and nitrous oxide flows that may lead to a hypoxic mixture. As the oxygen flow is increased, so too is the backpressure and the rightward motion of the shaft. The counterbalance between the 2 fuel flows (backpressures) determines the positioning of the nitrous oxide proportioning valve. If the oxygen circulate is decreased to lower than 200 mL/min, the proportioning valve will close completely. The system offers mechanical integration of the nitrous oxide and oxygen flow management valves to keep a minimal oxygen focus with a maximum nitrous oxide:oxygen circulate ratio of 3:1. Independent adjustment of either valve is allowed as long as the minimal Problems With Flowmeters. Dirt or static electricity can cause a float to stick and misrepresent actual flow. Sticking of the indicator float is extra frequent within the low-flow ranges as a result of the annular house is smaller. A broken float could cause inaccurate readings because the precise relationship between the float and the flow tube is altered. Backpressure from the respiration circuit could cause a float to drop in order that it reads lower than the precise flow. Flow tube leaks are a potential hazard because the flowmeters are located downstream from all hypoxemia security units, besides the breathing circuit oxygen analyzer. A portion of the nitrous oxide circulate escapes by way of the leak, and the rest goes toward the frequent gasoline outlet. A hypoxic mixture is less probably as a end result of all of the oxygen move is superior by the nitrous oxide (this precept is identified as the Eger flow sequence). In the occasion of a flowmeter leak, a probably dangerous association exists when nitrous oxide is positioned in the downstream position (A and B). A safer configuration exists when oxygen is located in the downstream position (C and D). The Link-25 automatically will increase oxygen flow when the nitrous oxide circulate is increased above the three:1 ratio. It also will decrease nitrous oxide circulate if oxygen circulate is decreased below that ratio. A 15-tooth sprocket is attached to the nitrous oxide circulate control valve, a 29-tooth sprocket is attached to the oxygen circulate control valve and a sequence physically links the sprockets. When the nitrous oxide flow control valve is turned via two revolutions, the oxygen circulate control valve will revolve as quickly as because of the two:1 gear ratio. Differential oxygen and nitrous oxide flows and the resultant chamber backpressures determine the place of the nitrous oxide proportioning valve. The Link-25 system makes use of a stop tab on each valve stem to permit for impartial adjustment of oxygen or nitrous oxide as long as the mixture is no much less than 25% oxygen; trying to turn the valve controller past that point will engage the chain and effect a change in the different gas. If the operator subsequently will increase the set oxygen flow, the nitrous oxide flow will remain at the new, lower value with the Link-25 system, as a end result of the mechanical linkage may have physically modified the nitrous oxide control valve setting.
Malegra dxt plus 160 mg order free shipping
The authors present a set of practical security ideas and strategies to guide the reader in improving or refreshing case management-related skills and to sensitize the reader to safety-related core issues and competencies in anesthesia impotence at 55 malegra dxt plus 160 mg order visa. Nevertheless impotence 60 years old 160 mg malegra dxt plus buy overnight delivery, most of the same ideas and issues are relevant to other perioperative settings, to crucial care, and to a lesser degree, in pain drugs. They may even largely apply to emergency medication and different health care domains sharing comparable cognitive profiles. For readers with a special interest in intensive care, a number of references is given as a place to begin. The authors have tried to balance retention of basic references, where the mental content material has solely changed barely over the years, with the introduction of present literature that displays changes in considering or evidence, or newer syntheses of information and expertise. Standard reference works are available9-14 in addition to a quantity of Internet sources (Appendix 6. This article samples only a portion of this literature because it most closely relates to the work of anesthesia professionals. These elements of human elements, or ergonomics, in anesthesiology are essential in their very own right. The reader is referred to a number of publications that evaluate these issues intimately. Here, too, the reader is referred to several publications that evaluation these points in detail21-36 and likewise to different chapters on this book. Even though provision of anesthesia has turn out to be a "secure" self-discipline over the past many years by way of many scientific and technical improvements, anesthesia per se is an intrinsically hazardous enterprise. The surgical process itself may trigger or set off quite a lot of physiologic derangements and a few sufferers needing anesthesia are already severely unwell. Thus, in anesthesiology a stable scenario can turn right into a life-threatening state of affairs in seconds, minutes, or hours, whereas in plenty of arenas of health care adjustments occur in days, months, or years. Historically, an adequately skilled anesthesia professional was automatically assumed to all the time perform appropriately. Deviations from optimal outcomes were understood to result from imperfections within the art and science of anesthesiology. This notion led to heavy emphasis on the scientific and technical aspects of anesthesia training and care. Adverse outcomes were principally ascribed to unavoidable unwanted aspect effects of a medication, underlying affected person illness, negligence, or incompetence on the part of the anesthesia professional. Several sections spotlight the nature of anesthesia as a extremely advanced and dynamic working setting and the difficulties that arise for human performance and affected person safety. For instance, a evaluate of crucial anesthesia incidents by Cooper and associates revealed that human factors were contributory in 82% of the 359 incidents reported. Data from an earlier analysis of 2000 incident stories support these findings with 83% of incidents occurring because of human error. The performance of human beings is incredibly versatile, highly effective, and sturdy in some aspects however limited and weak in others. For instance, we all know that the successful conduct of an anesthetic is dependent upon having the requisite technical expertise and related pathophysiologic data. But it has also become clear that the effective real-time implementation of such experience to a big extent is decided by a number of nonmedical and nontechnical parts of performance. Human factor-related safety strategies for the person and the team are indispensable. Lapses, mistakes, and errors have the potential to hurt a patient ("first sufferer"), however also can hurt professionals themselves ("second sufferer"). Professionals suffer as second victims largely from the perceived guilt about an error that led to actual hurt. Nonetheless, the finest way to keep away from hurt to the skilled or the group is to stop antagonistic occasions or mitigate harm to sufferers. Organizational safety attitudes are essential to support excessive particular person human efficiency. Moreover, departmental and organizational management must perceive the large impact their attitudes and habits have in shaping human performance, security culture, outcomes, and in the end (in all likelihood), the level of affected person security. Historically, anesthesiology was the first medical specialty to particularly concentrate on the promotion of affected person safety. As a consequence, anesthesiology is widely recognized because the pioneering leader in patient safety efforts. Compared to other medical disciplines, the monitor report of anesthesiology is indeed a model of affected person security for the remainder of health care. In addition, the increasing "manufacturing pressure" in anesthesia practice from increasing scientific demands in the face of fixed or diminishing assets may threaten beforehand received features. Several lately revealed studies demonstrate the benefits of implementing varied patient safety strategies. That belief is reward enough for the efforts of the authors as they share with the reader what is thought about human efficiency and affected person security. To better understand these patient safety challenges which would possibly be related to human performance, the authors first describe the key traits of anesthesia work. In what follows they tackle (1) important components that categorize anesthesiology as a complex and dynamic working environment; (2) the protection challenge of inherent asymmetry between safety and production, and the effects of manufacturing strain; and (3) the safety problem of complexity and tight coupling within the anesthesia domain. The answer is that the medical setting of anesthesiology is both complicated and dynamic which, when combined with the inherent dangers of surgical procedure and anesthesia, makes disaster situations frequent and difficult to cope with. These moments of terror necessitate that anesthesia professionals be expert in disaster administration. In distinction to well-structured problems, the nature and the objective of ill-structured problems are sometimes imprecise or unclear, and lots of downside components stay unknown or ambiguous. Interdependent decisions must be made and actions taken by the anesthesia professional, surgeon, and other perioperative personnel. The affected person is the primary "system" of quick curiosity to the anesthesia skilled, simply because the aircraft is of immediate curiosity to the pilot. The medical world is aware of little or no concerning the underlying causes of particular physiologic events, though the final ideas involved can be described. It should be inferred from ambiguous patterns of scientific observations and data from digital monitors. These data are imperfect as a result of, not like industrial techniques that are designed and constructed with sensors in key areas to measure crucial variables, patients are sometimes instrumented to measure the variables which may be best to monitor, predominantly with the usage of noninvasive methods. Most physiologic capabilities are noticed indirectly through weak alerts available at the body floor which would possibly be susceptible to various forms of electrical and mechanical interference. Invasive measurements are also vulnerable to artifacts and uncertainties of interpretation. In diseased or traumatized sufferers, or in the presence of acute abnormalities, these responses may be markedly abnormal, and patients may overreact or underreact to in any other case applicable actions. Thus, the affected person as a system has considerably larger uncertainty than do engineered systems. Over the long term this could trigger a scientific "normalization of deviance" 47-50 (see part "Normalization of Deviance and Flirting with the Margin"), meaning the emergence of recent, less stringent normal behaviors which are seen as regular judgments that beforehand would have been seen as aberrant. An even more intense time stress occurs inside a case when dynamic conditions evolve rapidly and turn into time crucial. For instance, selections on surgery planning are heavily influenced and manipulated by micropolitics and energy, as investigated by Engelmann and colleagues.
Malegra dxt plus 160 mg with mastercard
The last section briefly addresses patient demographics and the way they influence anesthetic behavior erectile dysfunction treatment charlotte nc purchase malegra dxt plus 160 mg mastercard. When formulating an anesthetic erectile dysfunction vascular causes buy malegra dxt plus 160 mg without prescription, the next factors have to be thought of in determining the right dose: age; body habitus; gender; persistent exposure to opioids, benzodiazepines, or alcohol; presence of heart, lung, kidney, or liver illness; and the extent of blood loss or dehydration. This part focuses on physique habitus and age, both recognized to influence the pharmacology of many anesthetic drugs and each of which serve as glorious examples of altered pharmacokinetics and pharmacodynamics. The group of blue drops emerging from the pipe on the high right characterize a bolus dose that, when administered to the tank of water, evenly distributes within the tank. The processes of absorption, distribution, and elimination (metabolism and excretion) govern this relationship. Estimates of distribution volumes and clearances are described by pharmacokinetic parameters. Pharmacokinetic parameters are derived from mathematical formulation match to measured blood or plasma concentrations over time following a identified amount of drug dose. If an injected drug disperses and distributes instantaneously all through the tank without any drug degradation, the distribution volume is estimated utilizing the easy relationship between dose. Considering the elimination of drug from the tank and the modifications If drug elimination occurs as a first-order course of. When a drug is run intravenously, some drug stays within the vascular quantity, however a lot of the drug distributes to peripheral tissues. This distribution is usually represented as further tanks (peripheral distribution volumes) related to a central tank (blood or plasma volume). For the calculation of distribution volumes, peripheral tissue concentrations are troublesome to measure whereas plasma concentrations are simply measured. The peripheral tank represents the drug quantity of distribution in peripheral tissues. There may be a couple of peripheral tank (volume) to finest describe the complete drug disposition within the body. The more soluble a drug is in peripheral tissue relative to blood or plasma, the larger the peripheral volumes of distribution. Thus, the entire volume of distribution might even be larger than the two tanks added collectively. At 2 minutes (left panel) and 4 minutes (right panel) following a 10-mg drug bolus, tank concentrations are decreasing from 5 to 2. Accounting for elimination, estimates of the distribution quantity at every time level are both 1 L. For a bolus dose, assume that the volume of distribution is 1 L at time = zero and that it then increases to 14 L as the plasma concentration falls over the following 10 minutes. The improve of the distribution volume is due to the distribution of drug to peripheral tissue and a lower in the plasma focus. For a relentless infusion, assume the volume of distribution is once more 1 L at time = zero and that it then will increase to 5 L as the plasma concentrations also improve to a steady-state focus over the subsequent a number of hours. It is estimated as the sum of the central and peripheral obvious distribution volumes. With additional distribution volumes, the overall quantity of distribution can change over time and is a operate of how drug is administered as nicely. For instance, think about simulations of concentrations and distribution volumes over time following a bolus dose or a steady infusion of an intravenous anesthetic Clearance Clearance describes the rate of drug removal from the plasma/blood. Systemic clearance completely removes drug from the body, both by eliminating the father or mother molecule or by transforming it into metabolites. Intercompartmental clearance moves drug between plasma and peripheral tissue tanks. By means of clarification, in this chapter, the phrases compartment and tank are interchangeable. For instance, assuming a first-order process, when plasma concentrations are high, the speed of drug elimination is excessive. The concentration changes for 2 time home windows are labeled with dashed lines from 1 to 2 minutes (time window A) and from 3 to four minutes (time window B), respectively. In this simulation, the whole quantity of drug at every time can be calculated from the identified quantity of distribution and measured focus. They are completely different, and neither can be used as a parameter to characterize a measure of drug removing from the physique. For dialogue purposes, assume that focus is the power necessary to push drug out of the water tank. To standardize the elimination fee, the eradicated quantity of drug is scaled to concentration. If the time interval is narrowed in order that the time window approaches zero, the definition of clearance becomes: dA (t) Clearance = dt C (t) Clearance = zero dA (t) 0 C (t) dt (18. To illustrate the connection between clearance and quantity of distribution, consider the following simulation utilizing a generic drug dosed in milligrams right into a single compartment (tank) representing the distribution volume that has a clearance of 1 L/min. Assume that when drug is run, the tank is well stirred and has instantaneous mixing all through the entire quantity. Assume the distribution volume is four L, the total dose of drug is sixty four mg, and that drug elimination is proportional to the quantity of drug present contained in the tank at any given time. A generic drug dose of sixty four mg is run into a single compartment quantity of four L that has a clearance of 1 L/min. Drug elimination is proportional to the quantity of drug current inside the compartment at any given time, otherwise known as first-order elimination kinetics. At 1-minute intervals, one of many four L is cleared along with all drug contained in that liter. With a clearance of 1 L/min, the quantity of drug distributed to one fourth of compartment quantity (1 L) might be cleared every minute. When assuming instantaneously mixing, the ratio of the quantity of drug removed inside the cleared portion of the distribution volume to the quantity of drug throughout the total distribution volume will stay the identical as illustrated in Eq. According to mass balance, the rate at which drug flows out of metabolic organs is the speed at which drug flows into them minus the metabolic price. If practically 100 percent of the drug is extracted by the liver, this suggests that the liver has a very giant metabolic capacity for the drug. In this case, the rate-limiting step in metabolism is the circulate of drug to the liver, and such medication are stated to be "move restricted. However, average changes in hepatic metabolic operate per se could have little Extraction ratio 1. Cin and Cout point out drug concentrations offered to and leaving metabolic organs. For medication with a excessive extraction ratio, clearance is type of similar to liver blood move. For medication with a low extraction ratio, adjustments in liver blood move have nearly no effect on clearance.