
Levaquin dosages: 750 mg, 500 mg, 250 mg
Levaquin packs: 60 pills, 90 pills, 120 pills, 180 pills, 360 pills

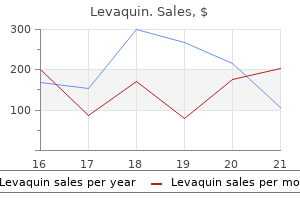
750 mg levaquin cheap free shipping
Trypsin symptoms 6 days before period due levaquin 500 mg purchase with amex, chymotrypsin medications zyprexa levaquin 750mg with amex, and other digestive enzymes may cross-activate the immune system by activating the thrombin pathway or protease-activated receptors [47�51]. The other variants may be 4 Pancreatitis loss-of-function variants that trigger pancreatic stress and injury signaling via an unfolded protein response [52, 53]. The threat of cancer in the fifth to sixth decade of life replicated the research by Lowenfels [28, 56]. A positive outcome, in the context of pancreatitis-like signs, has a very excessive probability of the symptoms coming from the pancreas. Genetic testing, sooner or later, can also present steerage on likelihood of specific syndromes, such as fixed pain or diabetes, though these ideas at present remain at a analysis stage. Thus, the illness was characterized by failure to thrive and salty sweat with demise in infancy until pancreatic enzyme alternative remedy was developed. Only after surviving pancreatic exocrine insufficiency will a toddler begin growing respiratory failure. Molecular modeling demonstrated that four totally different mechanisms have been involved in this transformation and/or regulation of bicarbonate conductance. It is useful to perceive a fancy disorder in contrast to a easy dysfunction [70]. A simple dysfunction is when a specific microorganism invades a number and causes a particular medical syndrome. In easy illnesses the pathologic agent is sufficient to cause the disease syndrome. In distinction, complex issues usually include acquired circumstances caused by complicated gene�environment, gene�gene, or a quantity of gene�environmental interactions where the pathologic brokers are neither needed nor adequate to cause the disorder. Further complexity happens if a sequence of pathologic events is needed earlier than sufficient qualifying options of the syndrome emerge to meet diagnostic criteria. The challenges of evaluating and managing a complex disorder embody creating a new mind-set about the prognosis and administration of these problems, integration of complex genetic threat into the paradigm, and developing new tools to assist the practitioner. Specifically, customized drugs calls for going beyond a simple Boolean operator of the germ theory (is a pathologic agent present, yes or no We will use the term customized medication as a medical mannequin that 6 Pancreatitis utilizes genetic info and biomarkers of illness activity to define the specific mechanism of illness inside a subject from among multiple prospects and target illness administration at the particular mechanism. In distinction, we use the time period precision medicine to outline a medical mannequin that optimizes the remedy of the affected person inside a disease mechanism. Thus, in our view, personalized drugs defines the underlying problem, whereas precision drugs defines the optimal therapy for the issue. This strategy might have profound implications for each early detection and illness administration. The new and thrilling opportunity is to define the precise danger advanced in individual patients, to monitor disease exercise and to target pathogenic pathways so that the pathologic endpoints are never reached (see Chapter 12b). This is personalised medicine [70, 71], and this must be the future course for the pancreatic illnesses management since the finish phases are irreversible. Proposal adopted unanimously by the individuals of the Symposium, Marseilles 1963. Chronic pancreatitis: an international draft consensus proposal for a new mechanistic definition. Epidemiology of persistent pancreatitis: burden of 15 16 17 18 the disease and consequences. Incidence, prevalence, and survival of persistent pancreatitis: a population-based study. Pancreas and liver harm are associated in people with elevated alcohol consumption. Marked enlargement of exocrine and endocrine pancreas with incretin therapy in people with elevated exocrine pancreas dysplasia and the potential for glucagon-producing neuroendocrine tumors. Alcohol consumption, cigarette smoking, and the chance of recurrent acute and persistent pancreatitis. Estimation of the prevalence and incidence of continual pancreatitis and its issues. The position of total pancreatectomy and islet autotransplantation for persistent pancreatitis. Clinical Gastroenterology and Hepatology: the Official Clinical Practice Journal of the American Gastroenterological Association. Total pancreatectomy and islet autotransplantation in persistent pancreatitis: Recommendations from PancreasFest. Long-term outcomes of complete pancreatectomy and islet auto transplantation for hereditary/genetic pancreatitis. Mutations within the cationic trypsinogen gene are associated with recurrent acute and chronic pancreatitis. Clinical characteristics of hereditary pancreatitis in a big family, primarily based on high-risk haplotype. Expression and penetrance of the hereditary pancreatitis phenotype in monozygotic twins. Mutations within the gene encoding the serine protease inhibitor, Kazal kind 1 are related to persistent pancreatitis. Relation between mutations of the cystic fibrosis gene and idiopathic pancreatitis. Proteaseactivated receptor-2 regulates bicarbonate secretion by pancreatic duct cells in vitro. Protease-activated receptor 2 exerts native protection and mediates some systemic issues in acute pancreatitis. Protease-activated receptor-2-mediated proliferation and collagen manufacturing of rat pancreatic stellate cells. Cigarette smoking as a danger issue fifty seven 58 59 60 sixty one sixty two sixty three 64 sixty five 66 sixty seven 68 for pancreatic cancer in patients with hereditary pancreatitis. Genetic counseling for hereditary pancreatitis-the role of molecular genetics testing for the cationic trypsinogen gene, cystic fibrosis and serine protease inhibitor Kazal kind 1. Journal of Cystic Fibrosis: Official Journal of the European Cystic Fibrosis Society. A mathematical model of the pancreatic duct cell producing high bicarbonate concentrations in pancreatic juice. Acinar cells are organized into spherical and tubular clusters known as acini with a central lumen. With neurohumoral stimulation as what happens throughout a meal, the acinar cells secrete their digestive enzyme stores into the lumenal space which is related to the pancreatic ductal system for transport of the digestive enzymes into the gastrointestinal tract. Secretion is into the lumen of the acinus which is related to the ductal system. Of observe, blockade of secretion as a outcome of total obstruction of the ductal system as happens in biliary pancreatitis, defect ductal secretion as happens with cystic fibrosis, or destruction of the filamentous actin network all result in injury of the acinar cell and pancreatitis [2�5]. Tight junctions between acinar cells and duct cells kind bands across the apical features of the cells and act as a barrier to prevent passage of enormous molecules such because the digestive enzymes into the blood [6].
Nucleic Acid (Rna And Dna). Levaquin.
- How does Rna And Dna work?
- Shortening recovery from surgery or illness.
- What is Rna And Dna?
- Are there safety concerns?
- Dosing considerations for Rna And Dna.
- Burn injury recovery.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96781
Buy levaquin 250mg online
Proceedings of the National Academy of Sciences of the United States of America 2007;104:4682�4687 symptoms enlarged spleen levaquin 250mg purchase overnight delivery. InsP(3)receptors and Orai channels in pancreatic acinar cells: co-localization and its consequences symptoms 10 days before period 500mg levaquin. Proceedings of the National Academy of Sciences of the United States of America 2013;a hundred and ten:13186�13191. Caffeine protects in opposition to experimental acute pancreatitis by inhibition of inositol 1,4,5-trisphosphate receptor-mediated Ca2+ launch. Enhancement of hysteria, facilitation of avoidance behavior, and prevalence of adult-onset weight problems in mice missing mitochondrial cyclophilin D. Role of tumor necrosis factor-alpha in acute pancreatitis: from organic basis to scientific evidence. Tumor necrosis factor- and interleukin-10 contribute to immunoparalysis in patients 55 56 57 fifty eight fifty nine 60 sixty one sixty two 63 64 sixty five with acute pancreatitis. Cytokines and organ failure in acute pancreatitis: inflammatory response in acute pancreatitis. Clinical remark of immunity in patients with secondary infection from extreme acute pancreatitis. Effect of tumor necrosis factor- inhibitors on drug-induced pancreatitis in inflammatory bowel illness. Pentoxifylline therapy in severe acute pancreatitis: a pilot, double-blind, placebo-controlled, randomized trial. A randomised, double blind, multicentre trial of octreotide in reasonable to extreme acute pancreatitis. Randomised, double blind, placebo controlled trial of intravenous antioxidant (n-acetylcysteine, selenium, vitamin C) remedy in severe acute pancreatitis. Acute pancreatitis � Progress and challenges: a report on a global symposium. Judicious use of antibiotic therapy and advances in crucial care medicine enhance the help to sufferers with pancreatitis through the preliminary severe part in addition to the second extra continual phase of disease. Remarkably few knowledge are available particularly cataloging those problems seen in the long term. This chapter supplies a quick evaluation of particular person issues, highlighting diagnosis and therapy. More than 80% of these patients will manifest a relatively gentle illness course, with spontaneous decision of ache and the inflammatory process. These therapies embrace well timed cholecystectomy for biliary pancreatitis, selling alcohol or tobacco cessation applications, and aggressive administration of metabolic situations similar to hypertriglyceridemia and hypercalcemia. Complications may arise in the course of the acute phase of illness or months to years remote from the preliminary disease insult. Anticipating these sequelae permits immediate recognition, expeditious remedy, and optimal patient outcomes. The pancreatic neck is a relative vascular "watershed" between the pancreaticoduodenal arcades supplying the head and the transverse pancreatic arterial branches from the splenic artery that provide the physique and tail [16]. As such, the neck is prone to insult from hypotension, which may perpetuate parenchymal necrosis. This method could also be both endoscopic or surgical relying on the quantity of stable necrosis, need for cholecystectomy (favors surgical), and native experience. External drainage of the disconnected tail � either percutaneous or operative � will result in pancreatic fistula. Some recommend simply eradicating the drain and that the majority of these fistulae will heal spontaneously (likely working their means into a loop of adjoining intestine). Note large peripancreatic collection in lesser sac with viable pancreatic head (long arrow) and small disconnected pancreatic tail (two quick arrows). Importantly, early enthusiasm for drainage into the fistula track (as opposed to the pancreatic remnant itself) has been tempered with time. This operation (fistula tract-jejunostomy) is simpler technically than formal pancreaticojejunostomy; nevertheless, not surprisingly, the slender, nonepithelialized tracks are most likely to shut and the sufferers present with recurrent pancreatitis or pseudocyst [18]. Clarity of terminology is important and careworn within the revised Atlanta criteria [19]. It is critically essential to not confuse walled-off necrosis with a "pseudocyst" because the remedy of these two entities is totally different. Most pseudocysts are found as a consequence of patient symptoms corresponding to pain, early satiety, or progressive bloating. Proper therapy of pseudocyst is directed by understanding the underlying pancreatic ductal anatomy [20]. Drainage into the alimentary tract may be completed endoscopically or surgically. The sturdiness of endoscopic drainage and optimum timing of endoscopic stent elimination are at present unknown. Other essential considerations are how much pancreatic parenchyma stays and the presence of venous collateral formation. Small-volume remnant pancreas produces much less pancreatic secretion and has less of an opportunity to keep the enteral connection open. The presence of venous collateral disease complicates surgical drainage; resection could also be extra prudent on this situation [14]. Endoscopic (transpapillary) stricture treatment turns into harder with strictures further out the physique and tail of the gland. Multidisciplinary input from experienced endoscopists and surgeons is necessary in treatment planning. Recurrent retroperitoneal collection/abscess Classic surgical reports from the era of open pancreatic debridement document a 10�30% incidence of recurrent intra-abdominal and retroperitoneal collections following operative debridement [4, 23]. In the contemporary period, a parallel is seen in patients handled with percutaneous drainage or the "step-up" method, many (most) of whom require multiple drain and/or upsizing of the drains to obtain definitive drainage [24]. Retroperitoneal collections may be related to persistent leak of pancreatic digestive juice or may be abscess of infectious origin. Recurrent retroperitoneal collections ought to be thought-about in a patient whose restoration plateaus or deteriorates after a period of recuperation (particularly after intervention). These collections are easily diagnosed by cross-sectional imaging and are largely amenable to drainage by the percutaneous method. Leakage of pancreatic juice from small branch ducts may trigger issues within the anatomic distribution of either the head or the tail. Treatment of retroperitoneal abscess is type of at all times potential with percutaneous drainage; systemic antibiotic remedy must be tailored to the cultured organism(s). After supply control has been achieved, the optimal duration of antibiotic treatment is poorly outlined. The clinician have to be aware that drug pharmacokinetic distribution into the retroperitoneum is different from that within the peritoneal cavity and that discontinuing antibiotics too quickly could result in recurrent abscess. We have found that a 7�10-day course is often adequate after supply management has been achieved. These resistant organisms are significantly difficult to clear from the retroperitoneum � recurrent abscess is comparatively common, and protracted programs of systemic antibiotic therapy could also be essential to achieve bacterial clearance.
Levaquin 500mg cheap
Equipment A primary set of surgical devices treatment 4th metatarsal stress fracture discount levaquin 500mg overnight delivery, including symptoms 7 weeks pregnant order levaquin 250 mg visa, at a minimal, a scalpel and 15 blade, toothed forceps, and needle holder. Closure For superficial biopsies a easy interrupted suturing approach for closure is used (absorbable sutures for the oral cavity and non-absorbable monofilament sutures for the facial skin). Postoperative care For facial lesions, clean the realm and canopy the suture with brown tape. Complications Poor beauty results are the most vital complication of facial pores and skin lesion excisions. Local pores and skin flaps might ameliorate some of these circumstances however, the place potential, poor cosmesis should be averted. This may be managed conservatively, however may have a long-term impression on salivary manufacturing, which may be relevant if the affected person receives radiotherapy to the oropharynx or neck. The majority of tracheostomy tubes in present use have a license for use for 71 month, and should be frequently changed in those patients with a long-term tracheostomy requirement. If patients develop tracheostomy-associated complications, or require a unique size or kind of tube, these modifications could also be expedited. In instances of unresolved blockage or dislodgement, it may be essential to change a tracheostomy tube as a life-saving intervention. Anatomy When making ready to change a tracheostomy tube you will need to contemplate the depth of the trachea from the pores and skin. With patients with broader necks, the trachea may lie more deeply and it might be easier to create a false passage in front of the trachea. This is likely to have been thought-about by the surgeon who positioned the tracheostomy tube and hence if an extra-long or adjustable flange tube has been used these must be used once more. Furthermore, the degree of flexion and extension of the neck is variable, and those patients with cervical spinal pathology could additionally be unable to prolong their neck. Neck extension moves the trachea more anteriorly inside the neck, making it extra accessible. These are non-dissolvable sutures placed though the trachea wall and then stuck to the skin of the skin. Indications Tracheostomy tubes are usually modified after no less than 1 week after insertion. A week is left for an enough tract to type and the tracheostomy is usually sutured in place throughout this period. Consent Verbal consent is often enough for this process or in emergency cases, where the procedure is undertaken as a direct, life-saving measure. Preoperative preparation the indication for a tube change is confirmed, any factors that may make the change troublesome are thought of. Postoperative care as quickly as the position of the tube is confirmed, sedated patients ought to be returned to their previous nursing position. The affected person ought to be carefully noticed for any respiratory modifications due to potential issues, including aspiration and pneumothorax. Potential problems embody lack of airway with consequent hypoxia, haemorrhage into the airway, creation of false tract, cardiovascular instability, bronchospasm, aspiration, and tracheal trauma. Tips and tricks In circumstances the place a troublesome change is anticipated or a false tract has beforehand been brought on, the tracheostomy tube could also be changed over a guide wire using a Seldinger method. These might involve bleeding diasthesis, poor neck extension, cervical tumours, or adipose necks. Anatomy the trachea lies within the midline from the larynx superiorly, into the thorax. Consent Consent should contemplate the indication, and the dangers and consequences of surgery. The procedure may be life-saving and is usually designed to exchange an endotracheal tube, which has its personal complications when in situ for a lengthy interval. Standard consent is commonly not at all times attainable, as the procedure may be undertaken in finest pursuits, if the affected person lacks the capacity to decide on therapy. When the patient has capacity, the effect of a tracheostomy on airway, tracheal secretions, voice, and swallow must be thought-about. The potential for blockage and an infection additionally talked about, in addition to the potential for fistula formation. In the quick time period, risks of bleeding, an infection, sudden decannulation, and pneumothorax should be mentioned. Preoperative preparation the indication is confirmed and an appropriate tube must be chosen. This may be fenestrated or not, cuffed or not, have an inner tube, and be quite a lot of makes, shapes, and sizes. Position and theatre set-up the patient is supine with a shoulder roll and head ring used to lengthen the neck. The ventilation circuit connector is hooked up and air flow is confirmed with finish tidal Co2. Closure Haemostasis is checked, while one hand frequently secures the tracheostomy tube. Postoperative care Humidification and common saline nebulizers may help manage secretions in the tube together with common suctioning and tube care. Complications Tracheo-cutaneous fistulae could additionally be closed in layers excising a rim of epithelium from the tract. Rare however feared complications of tracheostomy embody fistulae into great vessels, which can be very challenging to manage. Airway stenosis may happen as a long-term consequence of tracheostomy and this might be managed endoscopically or (rarely) with open surgical procedure. Tips and tips the positioning of the affected person is crucial to achieve sufficient surgical entry. In the larynx, microlaryngoscopy may incessantly be therapeutic when pathologies corresponding to granulomas, polyps, and cysts are excised. Bouchier microlaryngoscopy devices and laser could also be helpful if microlaryngoscopy proceeds to intervention. Further intervention, corresponding to biopsy or phonosurgery, carries further risks, together with infection and bleeding, vocal wire scarring leading to dysphonia, and (rarely) even swallow signs or swelling compromising the airway. Records from clinic, including a record of versatile nasendoscopic examination, are important. In some methods these are higher types of analyzing the pharynx and larynx, and their findings can help goal the examination. With care not to lever on the enamel, the tip if the laryngoscope is elevated and the epiglottis is identified. If laryngeal surgery goes to take place, a suspension arm could also be connected to help the laryngoscope in place while two palms are used to operate. Postoperative care If phonosurgery is undertaken, voice rest for 2�3 days is normally suggested.
Order levaquin 500 mg overnight delivery
In a randomized controlled trial [27] medications peripheral neuropathy order levaquin 250mg with visa, cocktail of antioxidant supplementation was related to aid in abdominal ache and reduce in oxidative stress treatment jerawat di palembang levaquin 250mg buy, thus supporting the oxidative stress hypothesis. These fascinating observations must be substantiated earlier than an etiological function to these factors can be assigned. In a latest evaluate, a two-hit model for the pathogenesis of tropical calcific pancreatitis was proposed. Presence of extra genetic and/or environmental elements, which represent the second hit, may lead to a number of phenotypes corresponding to stone formation, fibrosis, and/or diabetes mellitus [9]. Acinar tissue show infiltration by lymphomononuclear cells along with eosinophils. Acinar tissue is changed by fibrosis and later lipoid metaplasia replaces fibrosis with mature adipose tissue. The calculi may be smooth, rounded, or stag-horn-like in shape and are usually incarcerated in the principle pancreatic duct or its branches [42]. Maldigestion/steatorrhea Overt steatorrhea is just present in about 20% of patients. This is believed to be because of three causes: the patients are young, lean, and have low lipid ranges [8]. It probably appears that this change has been caused by adjustments in food regimen and setting caused by economic improvement in India. Cirrhosis and disseminated calcification of the pancreas in patients with malnutrition. Tropical pancreatitis � a distinct entity, or merely a sort of chronic pancreatitis Unchanged are its geographical segregation, incidence in strict nonalcoholics, and early onset of the disease [9, 47, 48]. Most patients nonetheless current with ache, although milder and sometimes managed with medication. The diabetes is milder, and can typically be managed using dietary measure and oral hypoglycemic agents; about one-third of the patients require insulin. A search for malnutrition associated diabetes mellitus in an Ethiopian diabetes clinic. Vasculopathic and cardiomyopathic modifications induced by low-protein excessive carbohydrate tapioca based diet in bonnet monkey. Anthropometric measurements of nutritional standing in persistent pancreatitis in India: Comparison of tropical and alcoholic pancreatitis. Comparative study of the medical profiles of alcoholic chronic pancreatitis and tropical chronic pancreatitis in Tamil Nadu, south India. Absence of diabetes in rural west African inhabitants with a high carbohydrate/cassava food plan. Evidence for induction of cytochrome p-4501 in patients with tropical persistent pancreatitis. International Journal of Clinical Pharmacology, Therapy, and Toxicology 1990;28: 235�240. Micronutrient antioxidant standing in tropical compared with temperate zone persistent pancreatitis. Genotype phenotype correlations in 9 patients with tropical pancreatitis and identified gene mutations. Novel mutations in the calcium sensing receptor gene in tropical persistent pancreatitis in India. Radiological appearance of pancreatic calculi in tropical and alcoholic persistent pancreatitis. Definition, prognosis and classification of diabetes mellitus and its issues. Complications in fibrocalculous pancreatic diabetes-the Pune and Madras expertise. Currently out there remedies for pancreatitis ache are insufficient and expensive, each in health-care dollars and in lost productiveness. Pain is the most common purpose for hospitalization among chronic pancreatitis patients, and as many as 40% require three or extra admissions throughout their lifetime for pain administration [1]. Improved treatments rely upon a better understanding of the mechanisms of continual visceral ache, a topic that has gained consideration lately with the event of appropriate animal models and reproducible experimental measures of sustained pancreatic ache. Pain theories Traditional theories of the origin of pancreatic ache in persistent pancreatitis centered on structural abnormalities inflicting ductal hypertension [4]. Such abnormalities ranged from stones and strictures to fibrosis as a outcome of toxic effects and ischemia [5]. Rather than a single mechanism of pain, current research has favored a more complicated relationship between these structural and morphological components, and their interaction with neurobiological mechanisms [11]. Nociceptive pathways, inflammatory mediators, and sensitization of both central and peripheral pathways have been proven to play necessary roles in pancreatic pain [12]. Manifestations and therapy of pancreatic pain Chronic ache syndrome: a downward spiral Among the numerous medical sequelae of chronic pancreatitis, pain has been shown to be crucial factor affecting high quality of life [2]. The pain often turns into the focus around which work, leisure actions, and relationships must revolve. Since eating can set off ache exacerbations, patients sometimes respond by reducing meals consumption. Many sufferers also suffer nutrient malabsorption because of pancreatic exocrine insufficiency, and this mixture Models Pancreatic atrophy and fibrosis may be induced experimentally in a wide selection of ways; nevertheless, measures of visceral ache have confirmed more difficult. Studies in rats evaluated spontaneous activity qualitatively by video monitoring and sensitivity of the stomach to mechanical Pancreatitis: Medical and Surgical Management, First Edition. This model was further characterised and modified to provide better face validity and generalization to human disease by Winston et al. This model has proved invaluable in providing perception into the complicated nature of ache from continual pancreatitis. Further progress in identifying particular pathways that might be therapeutic targets, however, was hampered by the lack of a murine model during which putative mediators might be genetically deleted. The resultant persistent pancreatitis is clear after 1�2 weeks with extreme fibrosis, monocyte infiltration, atrophy, and fatty alternative of the gland. This model can be used to examine each peripheral and central mechanisms of sustained pain and for comparison with fashions of somatic ache, similar to peripheral or spinal nerve ligation, in order that each shared and distinctive pathways may be identified. They are answerable for transmission of noxious visceral stimuli from the pancreas and the relay of this information to the central nervous system. Uncontrolled proteolysis the pancreas is wealthy in cysteine and serine proteases that could be launched following quite so much of insults and are recognized to activate, either directly or not directly, nociceptive neurons. Using a close to infrared-labeled activity-based probe that covalently modifies active cathepsins, our laboratory discovered significant accumulation of cathepsins B, L, and S in each the inflamed rodent pancreas and in human juice from patients with painful continual pancreatitis [16]. Cathepsins, in flip, cleave and activate trypsinogens, yielding lively trypsins, some of that are resistant to endogenous degradation by ubiquitous inhibitors, and are thereby free to bind and activate receptors on peptidergic neurons [17]. Evidence 172 Pancreatitis for a direct interaction between the two channels was proven by Staruschenko et al. This activation in flip mediates ache transmission via subsequent activation of nociceptive spinal neurons within the superficial laminae of the spinal twine.
Levaquin 500mg amex
Neurohistopathologic findings after a neurolytic celiac plexus block with alcohol in sufferers with pancreatic cancer ache medications nursing buy generic levaquin 250mg online. Histopathologic correlation of endoscopic ultrasound findings of persistent pancreatitis in human autopsies treatment 5cm ovarian cyst cheap levaquin 250mg mastercard. A potential, quantitative evaluation of the effect of ethanol and other variables on the endosonographic appearance of the pancreas. Diagnosis of persistent pancreatitis with endoscopic ultrasound: a comparability with histopathology. Endoscopic ultrasound, secretin endoscopic pancreatic perform take a look at, and histology: correlation in persistent pancreatitis. Interobserver settlement for pancreatic endoscopic ultrasonography decided by same day back-to-back examinations. Multicenter study of interobserver agreement of ordinary endoscopic ultrasound scoring and Rosemont classification for prognosis of continual pancreatitis. Conventional versus Rosemont endoscopic ultrasound criteria for persistent 50 51 fifty two 53 pancreatitis: interobserver settlement in identical day back to again procedures. Opioid use determines success of videothoracoscopic splanchnicectomy in persistent pancreatic pain sufferers. Indeed, pancreatic surgery lagged behind the surgery of other visceral organs, probably due to a quantity of aspects properly voiced by von Mikulicz-Radecki in 1903 [1]: "The reason for the tardy growth of the surgical procedure of the pancreas. This evaluation focuses primarily on the seminal publications/thoughts that laid the foundation for our current understanding of the surgical approaches to continual pancreatitis. The approaches to treating chronic pancreatitis which have continued to date are as follows: a. These are the ideas from which our present operative strategies to the treatment of continual pancreatitis derive. The method to the pain of continual pancreatitis differed radically from the approach to the administration of pancreatic neoplasms. Moreover, in the Forties, pancreatic resection was fraught with multiple issues associated to the reconstruction of the upper gut after a serious resection, pancreatic fistulas, and dietary support in typically malnourished patients, a lot of whom were alcoholics. Indeed, expertise was limited, and a neurectomy from a translumbar approach was a much less morbid operation. From 1942 onward, Mallet-Guy and colleagues [2�4] from Lyons, France, Pancreatitis: Medical and Surgical Management, First Edition. Consequently, his process excluded greater than half the patient inhabitants with continual pancreatitis. Interestingly, Mallet-Guy maintained that the operation was not directed at so much the pain however quite at the means of recurrent, relapsing pancreatitis. Thomas White in 1965 spent a 12 months in Lyon, France, while on a Guggenheim fellowship reviewing the records of all sufferers present process splanchnicectomy and celiac ganglionectomy performed by Mallet-Guy up to 1965 [5]. Indeed, lots of this group of patients would have been anticipated to stay pain free with or without splanchnicectomy, in addition to incurring further harm to the pancreatic parenchyma. Pancreatic resection Prior to the Nineteen Fifties, pancreatectomy was not carried out commonly, and particularly so for continual pancreatitis. Experience with resection for pancreatic most cancers was rising by way of work by Whipple, Brunschwig, and plenty of others [1] � bear in mind, there was no cross-sectional imaging available, so most resections were explorations for "painless jaundice" for presumed pancreatic most cancers. Many centers adopted this method of "creeping" proximal resections suggested early on by Child, Frey, Braasch, Warren, Clagett, Longmire, White, Cattell, Jordan, and others [8�12]. Parenchymal resections of 80% produced ache relief in 80% of sufferers, which was no better than operations similar to pancreatoduodenectomy that preserved a higher quantity of pancreatic parenchyma. Extensive pancreatic resections (80% or more) were deserted by their proponents together with Child and Frey after they presented their results with seventy seven patients at the American Surgical Association as a result of the devastating consequences of the process, which led to brittle diabetes and pancreatic insufficiency in a majority of sufferers. As said by Dr Child who originated the 95% distal pancreatectomy, "it was an experiment which failed" even surprisingly after whole pancreatectomy and eventuated in pancreatic insufficiency in an already troublesome affected person population (largely alcoholics). The success of the 95% distal pancreatectomy and pancreatoduodenectomy targeted consideration to the pinnacle of the pancreas as the principal anatomic goal in pain reduction. Longmire referred to the top of the pancreas as "the pacemaker of ache" (Traverso, private communication). This idea led Longmire in the United States to suggest a proximal resection (pancreatoduodenectomy) [13] and Beger in Germany [14] to concentrate on resecting the top of the pancreas as the supply of nearly all of the ache in continual pancreatitis. Their approach designed to protect the parenchyma of the physique and tail of the pancreas had surprisingly good results (prolonged ache reduction in as a lot as 85% of patients). The concomitant rising experience with pancreatectomy for pancreatic cancer further supported this practice and provided operative expertise with the technical aspects and postoperative care of the postpancreatic affected person. Currently, this strategy of proximal resection persists for small-duct continual pancreatitis. Ductal drainage (� partial, nonanatomic resection) Two kinds of continual pancreatitis have been noted each intraoperatively and preoperatively with the development of cross-sectional imaging: small-duct disease and 258 Pancreatitis large-duct illness. The latter was presumed to be associated to ductal obstruction with associated will increase in intraductal stress resulting in the presumed associated pain of continual pancreatitis � thus the idea of "ductal drainage" by some type of pancreaticoenterostomy. One of the earliest "profitable" ductal drainage procedures was a real tube pancreatostomy by Link in 1909 [15]; this surgeon mobilized the body/tail of the pancreas, filleted open the dilated pancreatic duct, placed a tube within the duct, closed the duct/parenchymal pancreatic incision (pancreatotomy), brought the gland via the mesocolon, and exteriorated the tube (wow! Thereafter, numerous anecdotal attempts at enteric ductal drainage had been made however have been unsuccessful. Similarly, an period of interest in sphincterotomy of the ampullary sphincter ensued underneath the impression that proximal "reduction" of the ductal obstruction by sphincterotomy would prevail [16, 17], but outcomes have been inconsistent. The first actual breakthrough got here from the work of DuVal in 1954 [18] by which he performed a limited resection of the tail of the pancreas (with splenectomy) to which a Roux limb was sewn for retrograde drainage of the pancreatic duct in two sufferers with good outcomes. The process was improved on by Puestow and Gillesby in 1958 [19], once they reported their experience with 22 sufferers in whom they not only performed the short distal pancreatectomy (with splenectomy) to assist find the pancreatic duct, however they also filleted open the duct proximally and sewed a Roux limb onto this filleted-open pancreatic ductotomy. Their work was primarily based on their five basic ideas (the following 4 of that are still largely believed to be true today): (i) the pain of chronic pancreatitis is secondary to increased intraductal pressure; (ii) calcification/stone formation is from calcium-soap formation within the duct (stasis); (iii) the pancreatic duct usually has multiple sites of obstruction, all of which require drainage; and (iv) irritation of the ductal system happens when strictures are current that stop free communication of ductal fluid all through the duct. Partington and Rochelle [20] further improved the approach by undertaking a similar, total ductal drainage through a side-to-side pancreaticojejunostomy but without the added morbidity of a distal (albeit limited) pancreatectomy and without the need for a concomitant splenectomy and its morbidity. These types of ductal drainage persisted because the procedure of selection for big duct illness till the 1980s, when the work of Frey and Smith [21] prolonged this concept by including a concomitant, nonanatomic, subtotal pancreatic head resection to the ductal drainage. This process was primarily based on their observations that drainage of the primary duct alone usually left a quantity of side branches undrained normally within the head of the gland (where the duct dives posteriorly) as a result of inflammatory obstruction of segmented ducts and on occasion an enlarged head of the gland. Frey and Smith "cored out" the top of the pancreas without the necessity for full mobilization of the posterior surface of the gland, usually the trickiest a half of the mobilization for either a Beger procedure or a pancreatoduodenectomy, and particularly so in some sufferers with extreme, continual inflammatory changes involving the retropancreatic superior mesenteric vein. Islet cell autotransplantation With the growing success of organ transplantation, the transplant surgeons approached this dysfunction in a special and complimentary style within the mid- to late-1960s. From a metabolic standpoint, one of many main drawbacks of any pancreatic resective process is the potential for the development of pancreatic insufficiency and especially the brittle diabetes that can ensue in an already compromised (often alcoholic) affected person. Why not resect the offending organ (the pancreas), however then (auto)transplant the islets to prevent (or in any case ameliorate) the resultant diabetes.
Levaquin 250mg cheap without a prescription
Marsupialization could be a sole process to decompress a cyst medicine encyclopedia 750mg levaquin, selling its shrinkage and infilling with bone symptoms miscarriage 500 mg levaquin generic overnight delivery, but is more normally followed by enucleation of a now smaller space. Indications (typical) Facilitation of histopathological diagnosis for persistent or enlarging radiolucencies. Procedure Aspirate the cyst with a 21G 40mm needle on a 10ml syringe and submit fluid for microbiology and histopathological examination. Tips and methods the bone and mucosal window have to be a minimum of a 3rd the size of the cyst for marsupialization to prevent closure and recurrence. Indications (typical) To replace an individual tooth with an appropriate abutment. Postoperative care Radiograph to guarantee cowl screw or abutment fully seated. Complications Damage to adjacent constructions, together with inferior alveolar nerve, inferior alveolar artery, lingual artery, and maxillary sinus. Indications (typical) To augment the posterior maxillary sinus previous to implant placement in sufferers with less than 8mm native bone top. Complications Tips and methods Small tears of 1�6mm can be patched with a collagen membrane. Position and theatre set-up Supine with mouth prop between molars of affected side. Procedure Stones anterior to the duct crossing the lingual nerve Pass a suture into the floor of mouth around the duct behind the stone to forestall it from transferring backwards. Stones posterior to the duct crossing the lingual nerve Incise the sublingual fold from the 1st molar to simply wanting the sublingual papilla, staying lateral to the submandibular duct. Tips and tricks Infiltrate local anaesthetic into the floor of the mouth to help haemostasis and supply some hydro-dissection. Position and theatre set-up Position is dictated by the place of the laceration. Tips and methods For oblique wounds, take deeper bites at the thicker edge for higher approximation-this shelves the wound. Anatomy the floor marking of the duct is alongside the middle-third of a line drawn from the tragus to the midpoint of the upper lip. Procedure Modify a 16G closed-end epidural catheter by slicing off the closed tip and cannulate the duct intra-orally. Tips and methods If the proximal end is throughout the substance of the parotid gland, ligate to induce gland atrophy as repair is impossible. Such moderate dysfunction, however, is still considerably higher than the morbidity associated with complete lack of facial nerve function. Indications (typical) Permanent motor deficit in the distribution of the affected nerve. Preoperative preparation Preoperative assessment of facial nerve perform using house�Brackmann scale. Preoperative preparation Irreversible visual loss occurs when ischaemia is >120min; surgical procedure have to be carried out instantly. Canthotomy Clamp the lateral canthus for 30�60s with artery forceps reaching laterally to the sting of the orbit, one arm overlying the surface of the skin, the other between the canthus and the globe. Indications (typical) Prolonged fixation during conservative fracture therapy. Preoperative preparation Check dentition and occlusion to ensure arch bars can be utilized; a deep overbite or extreme periodontal illness might preclude use. Procedure Attaching the arch bars Mobilize and cut back the fracture to align the dental arch. Applying intermaxillary fixation If that is carried out prior to extubation, ensure any throat packs are removed and the oropharynx is carefully suctioned. Ideal placement of plates is due to this fact as superiorly as possible without harm to the enamel. In the symphysis area there are extra torsional forces requiring an extra plate. In normal fractures a load-sharing (or functionally adequate) method with a semi-rigid miniplate and two monocortical non-locking screws on each side of the fracture is mostly utilized. Rigid buttressing of the fracture fragments by shut apposition creates mechanical stability. A load-bearing method with a inflexible reconstruction plate and three bi-cortical locking screws all sides of the fracture is required. Obviously there are intermediate conditions and experience aids selection of hardware. Anatomy the angle is the zone posterior to the 3rd molar and anterior to the posterior inferior attachment of masseter. Indications (typical) Displaced mandibular fractures inflicting malocclusion of tooth. Preoperative preparation Position and theatre set-up Supine with head stabilization. Extra-oral submandibular � submental method Incision length relies on the quantity of access required. Closure Close in layers utilizing 3-0 absorbable sutures, approximating the mentalis muscle first, then the mucosa. Postoperative care Prophylactic antibiotics if poor oral hygiene/immunocompromised. Complications (specific to the procedure) Tips and tips Blunt dissection to free the mental nerve will permit easier gentle tissue retraction. Anatomy the facial nerve enters the parotid gland virtually immediately after leaving the skull and divides within it to provide the facial muscles. Indications (typical) Absolute Unable to achieve occlusion with closed approach. Complications (specific to the procedure) Tips and tricks Low fractures and lateral override fractures are easiest. These are referred to as tripod fractures as they displace at three points: the zygomatic arch (zA), lateral orbital rim, and infraorbital margin. Anatomy the zygoma has three processes that terminate at suture strains: the zygomaticomaxillary (zM), zygomaticofrontal (zF), and zygomaticotemporal (zT) sutures. Open reduction internal fixation Zygomaticomaxillary (zygomatic) buttress Make a full-thickness upper vestibular incision 5mm from the attached gingiva, extending from canine to 1st molar. Zygomaticofrontal suture Lateral eyebrow method: Apply a corneal defend to defend the globe and infiltrate a vasoconstrictor within the line of incision. If plates are used proceed antibiotics for 5 days Removal of sutures at 5�7 days.
Syndromes
- Changes in pulse
- Infective endocarditis
- Seaweed
- Blisters
- Pain in the lower abdomen or back
- Thickened wall of the right ventricle (right ventricular hypertrophy)
- Drowsiness
Order 250mg levaquin with visa
High levels of quartz publicity attainable in farming symptoms you are pregnant purchase levaquin 750mg free shipping, but silica-associated illness not often described medications known to cause miscarriage discount levaquin 500mg fast delivery. Usually cleansing or preparation for the coating of metallic items, but in addition uncommon applications. Fine silica used for llers in paints, coatings, plastics, rubber, explosives, dental supplies, etc. Comment Mining related Small-scale mining Major industrial sources Agriculture Ceramics Glass manufacture Furnace masonry Construction Stone-working and monumental masonry Abrasive blasting with sand (sandblasting) or siliceous materials Minor industrial sources Fillers and scourers Jewellery Diatomaceous earth Craft work Manufacture of siliceous materials Source: Modi ed with permission from the International Union in opposition to Tuberculosis and Lung Disease. Pneumoconiosis-not at all times with typical silicotic nodules-from prolonged publicity to desert mud, particularly desert storms, has been documented in China, India, Israel and Saudi Arabia (Derbyshire, 2007). The agate and slate pencil industries in India are welldocumented examples of this kind of exposure (Bhagia, 2012). Although convincing evidence exists that pneumoconiosis happens in farm staff (Schenker et al. More intensive case nding might reveal that farming is a extra important supply of silica-related ailments than currently thought. However, these small mines are often poorly regulated and hazard management is prone to be inadequate. For example, Chinese pottery staff had decrease silicosis dangers for a given exposure than Chinese tin and tungsten miners (Chen et al. Very ne particles and freshly cut surfaces improve toxicity, whereas aged quartz, using wet processes and, importantly, the presence of aluminium-containing clay minerals cut back toxicity (Meldrum and Howden, 2002). Obtaining representative office concentrations requires cautious planning and choice of applicable employees during periods of ordinary manufacturing. Estimates of the percentage of silicosis in eleven research at three levels of cumulative silica exposure varied significantly: from zero. Thus, overexposure might have occurred despite measurement knowledge suggesting it has not. Experienced occupational hygienists using calibrated equipment and quality-controlled laboratories are needed for dependable measurement. Cohort studies that adequately follow-up workers nd greater charges of disease: 47%�77% in a single evaluate (Steenland, 2005). There is uncertainty regarding whether silica publicity with out silicosis causes the malignancy (Erren et al. The studies showing that non-silicotics are at increased danger are, nonetheless, based mostly on the absence of radiological silicosis, which is an important consideration, as silicosis can be current without radiological proof of illness (Hnizdo et al. Unusual options, together with a brief publicity history, ought to prompt additional investigation. Review of previous chest radiographs could also be useful, and unchanged opacities over a few years assist a analysis of silicosis. In poorly managed settings, illnesses may manifest after only a few years of publicity (Akgun et al. The use of respiratory-protective gear could produce a false sense of safety, as inappropriate or inadequately used respirators are commonplace. Areas of peri-hilar ground-glass density and/or consolidation are frequent radiographic features (Xipell et al. The imaging options of groundglass density, centrilobular nodules and consolidation seen in acute silicoproteinosis are histopathological correlates of accumulation of intra-alveolar proteinaceous materials (Marchiori et al. Upper zone predominance is the rule, and these giant opacities are probably to occur within the periphery of the lung and migrate centrally over time. Both unilateral and bilateral densities (either symmetrical or asymmetrical) have been described (Chong et al. The necessary differential diagnosis is lung cancer, particularly within the context of unilateral or asymmetrical opacities. An upper and posterior lung distribution is frequent, though isolated lowerlobe masses are also recognised (Chong et al. A variety of calci cation patterns may be seen, particularly punctate, with intensive dense calci cation being less widespread. Avascular necrosis is a characteristic of huge lesions, with initial areas of decreased attenuation progressing to cavitation and air� uid levels. The imaging features of silicotuberculosis encompass the fast development of uneven nodules, consolidation and cavitation. Other issues that could be apparent on imaging embrace pulmonary arterial hypertension, proper heart failure and non-tuberculous infections. A cough, with or with out sputum, dyspnoea and wheezes or crackles on auscultation, is most frequently reported. The scientific features of accelerated silicosis are the same as for continual silicosis, except that they might current earlier in the course of the illness. Chest ache, clubbing, haemoptysis, fever and weight reduction are unusual in uncomplicated silicosis and may prompt additional investigation for potentially treatable diseases. The small number of studies in a single trade means that it has not been conclusively proven that elimination from further exposure will reduce development to extra superior illness. Sudden increases are, however, dif cult to de ne exactly, however noticeable modifications inside 2 years are uncommon, except past exposure has been very intense. In these circumstances, imaging turns into much more important than traditional, offered the radiological features, that are regularly atypical, are recognised. Mediastinal lymphadenopathy and the looks of large opacities are also of concern (Solomon, 2001; Solomon and Rees, 2010). Proportions of patients whose illness advances could additionally be very high-88% in a examine of long-service South African gold miners (Hessel et al. Although one would anticipate continued publicity to lead to extra fast progression of silicosis in higher proportions of topics, few studies have examined this problem. Silicosis circumstances from a mining company entered into a Swedish case register showed higher disease progression if postdiagnosis publicity continued relative to publicity cessation (Westerholm, 1980). Nodules additionally develop on the visceral pleura and in the peri-bronchial and hilar lymph nodes, which will be the rst sites of involvement (Murray et al. Calci cation of affected lymph nodes leads to a characteristic eggshell radiographic look. Early lesions of chronic silicosis comprise aggregates of macrophages with scanty reticulin and collagen bres; accelerated silicosis exhibits a predominance of those cellular lesions, and absolutely developed brotic nodules may be sparse. Silica particles are solely weakly birefringent under polarised gentle, with any sturdy birefringence being due to accompanying silicates such as mica and talc. As the illness progresses, the nodules prolong to involve the mid and lower zones of the lungs. Acute silicoproteinosis is characterised by a lipoproteinacious materials lling of the alveolar areas. The material consists of denatured alveolar surfactant, resembling that of primary alveolar proteinosis (Craighead et al. Very ne silica particles could also be seen on this exudate with the utilization of electron microscopy. Diffuse interstitial pulmonary brosis, pathologically resembling idiopathic pulmonary brosis, has occasionally been reported to happen in silica dustexposed patients with and with out nodular silicosis; nonetheless, neither the pathogenesis nor the scientific options are properly understood (Arakawa et al.
Purchase levaquin 500mg on-line
Non-fluoroscopic endoscopic ultrasound-guided transmural drainage of symptomatic non-bulging walled-off pancreatic necrosis medicine used during the civil war levaquin 750mg amex. Preliminary report on a new medicine vs dentistry levaquin 250 mg discount with amex, totally covered, steel stent designed for the therapy of pancreatic fluid collections. Factors impacting remedy outcomes in the endoscopic management of walled-off pancreatic necrosis. Dual-modality drainage of infected and symptomatic walled-off pancreatic necrosis: long-term clinical outcomes. Outcomes after implementing a tailored endoscopic step-up method to walled-off necrosis in acute pancreatitis. Interventions for necrotizing pancreatitis: abstract of a multidisciplinary consensus conference. Endoscopic transluminal necrosectomy in necrotising pancreatitis: a scientific evaluate. Endoscopic and percutaneous drainage of symptomatic walled-off pancreatic necrosis reduces hospital keep and radiographic resources. Endoscopic transgastric vs surgical necrosectomy for contaminated necrotizing pancreatitis: a randomized trial. Safety and efficacy of video-assisted retroperitoneal debridement for infected pancreatic collections: a multicenter, prospective, single-arm part 2 research. These cases typically resolve throughout the first week by partaking in solely medical therapy. Up to half of all deaths happen inside the first week, secondary to an overactive systemic inflammatory response and subsequent multiple organ dysfunction. Mortality after the second week results from native complications, infection, and/or sepsis. In both scenarios, organ failure is a major determinant of disease severity and a standard final event immediately associated with the overwhelming majority of deaths. Initial retrospective research outlining organ system dysfunction in acute pancreatitis date to the Seventies [1�3]. Respiratory dysfunction stays the most common extrapancreatic organ failure, reported in as a lot as 25% of circumstances. More particularly, early deaths most often end result from progressive respiratory deterioration followed by cumulative involvement of renal and cardiovascular systems. Despite the dearth of uniform diagnostic standards amongst early research, organ system dysfunction has been long recognized as a major prognostic factor in acute pancreatitis. The prognostic value of organ dysfunction was contemplated in the 1992 Atlanta severity classification system for acute pancreatitis [4]. Severe disease was outlined by the incidence of either organ failure or local problems. Definitions for particular local complications and organ failure had been additionally proposed. In the mid-2000s, the importance surrounding the time of onset and period of organ failure was further explored [5�7]. Furthermore, early organ failure was present in 44�60% of patients with extreme acute pancreatitis. Organ dysfunction persisting more than forty eight hours was related to higher mortality (34. In comparison, mortality in extreme acute pancreatitis without early organ failure was only 2. As an entire, it turned clear then that persistent organ failure is a significant determinant of disease severity. The objective of this project was to refine the severity classification, as well as to evaluation and clarify definitions of local and systemic complications [8]. A new intermediate severity group (moderately extreme acute pancreatitis) was described by the presence of either transient organ failure (<48 hours) or local Pancreatitis: Medical and Surgical Management, First Edition. The determinant-based system is a severity classification system proposed almost simultaneously to the 2012 revised Atlanta model, with a further larger risk category characterized by both organ failure and contaminated necrosis (critical acute pancreatitis). Physiological scoring methods have also been proposed to predict persistent organ failure in acute pancreatitis. Unfortunately, accuracy to predict persistent organ failure at admission is merely modest [13]. Consequently, the definition of "severe illness" was limited to patients with organ failure persisting past 48 hours. The a quantity of organ dysfunction rating, also called Marshall rating [9], was also used to simplify and standardize the clinical assessment of organ dysfunction (Table 8. The Marshall scoring system was originally developed to quantify multiple organ dysfunction syndrome within crucial illnesses. Scoring of respiratory, renal, hepatic, cardiovascular, hematologic, and neurologic dysfunction is predicated on objective and reproducible physiologic measures. A modified model of the Marshall score limited to the respiratory, renal, and cardiovascular techniques was proposed by the 2012 revised Atlanta classification. It may be engaged on admission and repeated day by day and is also applicable for sufferers managed exterior the crucial care unit. Stratification of organ dysfunction severity primarily based on this score is also possible however was not included in the Atlanta classification system. The similar six organ methods had been originally included, but the descriptor for the cardiovascular system reflects requirement for vasopressor help, instead of physiologic parameters. Respiratory failure is reported in 10�25% of all circumstances [16], but variable diagnostic standards primarily based on respiratory fee, hypoxemia levels, and/or treatment-related parameters have been classically employed. Mortality normally outcomes from cumulative involvement of other organ techniques because of a persistently overactive inflammatory cascade or a secondary insult (most usually infection). Respiratory failure accounts for about 60% of all deaths from acute pancreatitis [17]. Acute lung injury within acute pancreatitis is characterised by diffuse lung inflammation. The preliminary exudative section outcomes from elevated permeability of epithelial and endothelial pulmonary membranes Chapter eight: Treatment of systemic issues and organ failure 87 resulting in interstitial and alveolar infiltration with exudate and inflammatory cells. Systemic launch of pancreatic proteases additionally seems to contribute to the inflammatory lung damage [18]. Edema and diffuse injury to respiratory membranes cause impaired oxygen change and hypoxemic respiratory failure, typically within the absence of increased cardiac filling strain. At this stage, however, a second insult, similar to ventilator-induced lung harm, pneumonia, bacterial translocation, or catheter-associated an infection, can rapidly intensify respiratory dysfunction and result in a number of organ failure. Chest radiographs reveal nonspecific alveolar infiltrate in 10�26% of patients [15].
Discount levaquin 750mg otc
Genome sequence of Coxiella burnetii 109 medicine review buy levaquin 750 mg free shipping, a doxycycline-resistant medical isolate medications zolpidem levaquin 750mg generic without prescription. Q fever outbreak in Cheltenham, United Kingdom, in 2007 and the utilization of dispersion modelling to investigate the risk of airborne spread. Report of invasive Rhodococcus equi infections in Taiwan, with an emphasis on the emergence of multidrug-resistant strains. Diagnosing Rhodococcus equi infections in a setting where tuberculosis is highly endemic: A double problem. Missed sentinel case of naturally occurring pneumonic tularemia outbreak: Lessons for detection of bioterrorism J Am Board Fam Pract sixteen:339�42. Risk of occupationally acquired diseases from biological menace agents in unvaccinated laboratory employees. Exposure of laboratory staff to Francisella tularensis despite a bioterrorism procedure. Epidemiologic and molecular analysis of human tularemia, United States, 1964�2004. Cavitary histoplasmosis occurring throughout two giant urban outbreaks: Analysis of medical, epidemiologic, roentgenographic, and laboratory features. Subclinical Legionella infection in workers close to the supply of a big outbreak of Legionnaires illness. Prevalence of Legionella waterline contamination and Legionella pneumophila antibodies normally dental practitioners in London and rural Northern Ireland. Two outbreaks of occupationally acquired histoplasmosis: More than workers at risk. Immunologic, genetic and social human risk components associated to histoplasmosis: Studies in the State of Guerrero, Mexico. Penicillium marneffei an infection and up to date advances within the epidemiology and molecular biology aspects. Risk elements for disseminated or deadly histoplasmosis: Analysis of a giant urban outbreak. Serological examinations for antibodies against Legionella species in dental personnel. Legionella antibodies in a Danish hospital workers with identified occupational publicity. A case of melioidosis in all probability acquired by inhalation of dusts during a helicopter ight in a healthy traveler returning from Singapore. The epidemiology and medical spectrum of melioidosis: 540 instances from the 20 year Darwin potential study. Pulmonary melioidosis: Clinical�radiologic correlation in 183 cases in northeastern Thailand. Clinical options and epidemiology of melioidosis pneumonia: Results from a 21-year research and evaluation of the literature. Outbreak of invasive pneumococcal disease at a Belfast shipyard in males uncovered to welding fumes, Northern Ireland, April�May 2015: Preliminary report. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. High incidence of hospital admissions with multidrug-resistant and extensively drug-resistant tuberculosis among South African well being care staff. The creation of equipment that enables a diver to carry extra gas to breathe revolutionised human exploitation of the underwater world, but also launched new hazards. Diving is normally related to immersion in uid (water in the overwhelming majority of cases), but most of the same environmental effects act on a person who enters a dry pressurised environment. Diving will almost always be related to a raised environmental pressure and often with immersion. It is necessary to distinguish between the results of these two elements of diving when assessing particular person instances. Saturation diving requires more subtle technical assist and is used nearly exclusively for deep business diving initiatives. The disadvantages are the practical limitation on gasoline provide and dif culty locating the diver if lost. Gas is stored at excessive stress in vessels that are typically cylindrical or spherical in form. The major distinguishing characteristic of various types of self-contained equipment is whether the exhaled gas is exhausted into the water (open circuit), partially recycled (semi-closed circuit) or reused to the utmost extent potential (closed circuit). Equipment that recycles breathing gas will embrace a counter-lung into which exhaled gasoline is collected and may be returned to the diver with carbon dioxide scrubbed out and oxygen levels replenished. Hose supply Hose provide (also known as floor supply in surfaceorientated diving) can provide plentiful quantities of fuel and permits different services to be delivered to the diver alongside the respiration gas, corresponding to hot water for heating, hard-wired communications, camera surveillance, electricity for lighting and reclaim of exhaled gasoline for recycling. Older diving equipment, such because the basic standard diving helmet, offered a free ow of gasoline. The diver completes the deliberate work, returns to the bell, which contains respirable gasoline, after which a hatch is closed so as to forestall the interior strain from altering as the bell is hoisted to the floor. At the surface, the bell occupants transfer to a living chamber and remain at elevated strain till the subsequent working shift, when the pressurised bell will ship the diver again to the worksite. The diver is tHe WoRking enViRonment For a working diver, the dive is a means of reaching work that could involve heavy handbook labour in an area akin to a construction web site, expert duties or inspection for commercial, scienti c, archaeological, entertainment, educational, police or defence functions. A big selection of instruments and different equipment have been Diving 467 adapted for underwater use, introducing hazards which are familiar to these working on the surface (such as vibration and trauma from an angle grinder or cognitive decrement because of respirable heavy steel particles from grinding and welding in an enclosed space) and new ones (such as uncontrolled depressurisation because of entanglement with a buoyant lifting bag that breaks free). Since the strain at sea level is roughly one hundred kPa, this means that pressure will be doubled at 10 m depth beneath sea level. This contrasts dramatically with the modifications in stress skilled in air where, in order to halve the ambient stress, an ascent to an altitude of approximately 5500 m (18,000 feet) could be required. As the lungs include free gas, the partial pressures are affected in an analogous method. Nitrogen is taken into account to be chemically and physiologically inert at normal atmospheric strain. Oxygen at high partial pressures, as an example, becomes toxic to many tissues by overwhelming antioxidant defences after which causing oxidative injury. This contrasts with the scenario in air the place the stress utilized to all components of the physique is almost equal. The pressure differential in the water acts on blood, which generally occupies the more distensible blood vessels in the lower limbs and redistributes it extra evenly. Intrathoracic vessels turn into engorged with the displaced blood and scale back pulmonary capacity. The redistribution of blood also is determined by the degree of vasoconstriction caused by ambient water temperature. In an identical means, the pressure exerted on the chest wall will exceed that utilized to the mouth and nose. These two results add further force in opposition to which the diaphragm and inspiratory muscles must act in order to inhale. When in water, the standard functional residual capacity of the lung on land can be restored by delivering gas to the mouth at the similar strain as a notional point within the chest often identified as the lung centroid. This is roughly 19 cm beneath and 7 cm behind the sternal notch in a mean human male (Francis and Denison, 1999).
Levaquin 750 mg generic with visa
Note: Population exposures have been derived from the distributions across eight (asthma) or 9 (chronic obstructive pulmonary disease) occupational groups medicine zolpidem order levaquin 250mg online. Overall symptoms 4dpo 750 mg levaquin order with visa, the estimated variety of lung illness deaths because of occupational causes fell slightly (from 389,462 to 370,276) between 1990 and 2010. Note: the ranges re ect variations within the relative wealth of different international locations within the regions- see textual content. This is completely to be anticipated, given the history of European and North American nations that underwent very related experiences; history, in spite of everything, teaches that people and governments have never learned something from historical past. It is doubly unlucky that discussions of non-communicable ailments in creating international locations often make no point out of occupational exposures; as a substitute, the emphasis is on personal dangers similar to tobacco, salt and alcohol overuse and obesity. The world burden of non-malignant respiratory disease as a outcome of occupational airborne exposures. Review of estimates of the worldwide burden of harm and illness because of occupational exposures. Occupational safety hazards confronted by youngsters working in brick kilns in Afghanistan. The function of environmental and occupational hazards in the grownup well being transition. A comparative danger evaluation of burden of disease and injury attributable to 67 danger factors and threat issue clusters in 21 areas, 1990�2010: A systematic evaluation for the Global Burden of Disease Study 2010. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020. The international burden of chosen occupational illnesses and damage dangers: Methodology and abstract. Epidemiologic estimate of the proportion of fatalities related to occupational elements in Finland. Temporal pattern, geographic distribution, and publication high quality in asbestos analysis. Family docs within the United Kingdom, for example, recorded an occupation in only one in seven of their patients with bronchial asthma who were of working age (Walters et al. This uninspiring experience is repeated in many other surveys, with the outcome that a considerable proportion of occupational disease is unrecognised, or is identified late, with necessary consequences for sufferers, employers and regulatory authorities. Quite why docs nd the matter so dif cult is unclear, but it might re ect the insularity-mistaken as privacy-of the traditional doctor�patient relationship, and maybe the socioeconomic demography of most medical doctors, comparatively few of whom have had any experience-direct or indirect-of conventional labour. This in turn is re ected within the low priority given to occupational well being in most medical college curricula, despite evidence that such training is effective (Storey et al. In the investigation of (adult) respiratory illness, the difficulty must be taken more critically, since a considerable proportion of the caseload is directly attributable to workplace exposures, and patients with non-occupational respiratory disease frequently nd that their symptoms are provoked by exposures or actions of their work, which can threaten their employment. A full occupational historical past requires considerable time and experience, each of which are briefly provide. It is for this reason-and to counter the dif culties described above-that some authorities advocate easy screening questions to be utilized by each doctor caring, for example, for an adult of working age with bronchial asthma, and referral onwards for more specialist enquiry and investigation if acceptable (Fishwick et al. In every case, an understanding of the types and ranges of publicity required to induce disease will help to focus the occupational historical past. There are two broad classes of occupational causation: those who re ect cumulative publicity and people re ective of hypersensitive or toxic mechanisms. These in turn are re ected in the ordinary latent durations between (rst) exposure and the clinical onset of illness, thus offering a focus for enquiry into the in all probability relevant occupational exposures in a person case. The initiation of occupational lung cancer requires time for the tumour to enhance in dimension suf ciently for detection. Tumour doubling instances differ from roughly 35 days for small-cell cancers to a hundred and sixty days for adenocarcinomas, that means that exposures within the previous 3 years (smallcell cancers) to 10 years (adenocarcinomas) earlier than detection are unlikely to be causes (Usuda et al. In contrast, for ailments in which the known latency is short-exempli ed by acute hypersensitivity pneumonitis or, most obviously, by inhalation accidents-a focus can be utilized to exposures which might be far closer in time to their onset. Diseases with the identical scientific presentation, similar to bronchial asthma and alveolitis, might happen with or without a latent interval. There have been very substantial reductions of exposures in most western nations, usually courting from around 1975, so shorter periods of publicity in earlier years relate to higher levels of cumulative publicity. Thus, an occupational history starts with the collection of a job history, targeted or in any other case as above. Understanding the jobs that patients have carried out can be dif cult and the likely exposures they incur may not be instantly apparent. Industries and the employees in them typically have their own jargon that at rst can appear impenetrable, but most patients are perfectly pleased to educate their medical doctors. Having some background knowledge of the social and industrial history of the area helps, and as consecutive sufferers contribute their occupational histories, it quickly becomes attainable to construct a better understanding of the details of the commercial processes and exposures which have taken place in a particular geographical area over time. The extra occupational histories that one takes, the greater becomes the appreciation of the likely exposures involved. Case History A 49 12 months old man offered with 2 years of breathlessness and a chest X-ray exhibiting widespread nodules without mediastinal adenopathy. He had been a coal miner from 1975 to 1985 in a low-rank coal mine, and again from 1992 to 1998 with none coal face work. Fettling steel may result in iron deposits in the lung (siderosis), however these can often be distinguished radiologically due to their higher density. Further element is required in order to determine what he was really doing as a miner. This is someone who cuts the access tunnels to the coal seam, which involves mining by way of whatever strata are present, often via silica-containing rock. From 1997 to 1998, he turned a mine deputy in management of blasting the entry tunnels. From 1992 to 1998, he was in command of the upkeep of the underground roadways (tunnels), including 1 yr roof bolting, the place long bolts are drilled into the rock above the tunnels in order to x roof supports. Some patients, particularly those that have been self-employed, could also be reluctant to declare certain jobs with high-risk exposures. Exposures can be generated from adjacent processes, and subsequently enquiry should be made about all other processes inside the same work area. Understanding the details of processes is essential in assessing how the exposures are being generated; for instance, in the form of a vapour, gas, mud or fume. These would include factors such as whether or not the method was enclosed or extracted or other native measures had been carried out to control exposure. Periods where respiratory protection was worn, and more importantly durations where protection was not worn or was inappropriate, might must be noted. Surveillance ought to have been carried out at regular intervals and many years of knowledge may be available. No physician, however, can count on to perceive all types of work, and further enquiry is often needed, as outlined below.