
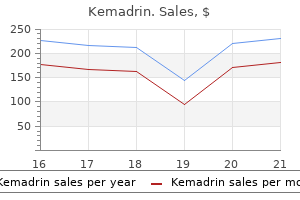
Kemadrin dosages: 5 mg
Kemadrin packs: 20 pills, 30 pills, 60 pills, 90 pills, 180 pills, 270 pills, 360 pills

Buy 5 mg kemadrin fast delivery
If the patient is relatively asymptomatic and the output is less than 200 mL/d while on a food plan medications similar buspar order 5 mg kemadrin fast delivery, consideration towards sending the affected person residence with outpatient drain management should be given medications in mothers milk purchase kemadrin 5 mg without a prescription. Distal pancreatectomy is required for the resection of pancreatic cancers of the physique and tail of the pancreas. Although, this operation is much less concerned than a pancreaticoduodenectomy, the potential for signi cant morbidity exists. In a collection Long-Term Survival After Resection of Periampullary Cancers e periampullary adenocarcinomas share a common location of origin however differ significantly of their long-term survival. In an analysis of actual 5-year survivors from 242 consecutive sufferers with resected periampullary adenocarcinoma, of which 149 (62%) had been pancreatic primaries, forty six (19%) arose in the ampulla, 30 (12%) had been distal bile duct cancers, and 17 (7%) have been duodenal cancers, there have been 58 precise survivors. Several sequence have reported survival and prognostic options for some of the particular person periampullary adenocarcinomas. In a collection of 1423 pancreaticoduodenectomies for pancreatic adenocarcinoma, the median survival 1. Resected adenocarcinoma of the pancreas-616 patients: outcomes, outcomes, and prognostic indicators. In a series of 127 resected patients with ampullary adenocarcinoma, a 5-year survival price of 36% was reported. Unanswered questions in this eld embrace the relative e ectiveness of chemoradiation versus chemotherapy alone, radiation fractionation and dosing, and optimal systemic remedy. Because current chemotherapy is relatively ine ective, the following leapforward in enhancing outcomes for these sufferers will be the development of more e ective systemic therapy. Adjuvant remedy for periampullary most cancers is greatest studied in pancreatic adenocarcinoma for which a number of prospective trials have been conducted. We are prone to see more trials in the future combining gemcitabine with radiotherapy. Gemcitabine was chosen as the only agent on this study based mostly on its bene t when used as palliative remedy. Despite this di erence, there was no improvement of overall median survival that was 22. No massive potential trials have been conducted solely for any of those periampullary cancers. Several retrospective studies have instructed a bene t for chemoradiotherapy in some situations. For example, Krishnan et al77 conducted a retrospective analysis of 96 sufferers with resected ampullary most cancers and demonstrated a development towards improved survival in those who receive chemoradiotherapy in comparability to statement. It has the potential to shrink the tumor and theoretically can decrease the extent of native illness. Patients who develop disseminated disease during neoadjuvant treatment are unlikely to have bene ted from initial resection and are spared the time dedication, morbidity, and potential mortality of resection. Ten patients (5%) received gemcitabine chemotherapy with twice-daily external beam radiotherapy with a deliberate whole dose of 3000 cGy at a hundred and fifty cGy per fraction over 3 weeks. Patients who underwent resection with minimal residual disease, and people whose tumor specimens had signi cant tumor necrosis, loved signi cantly better survival. Anderson Cancer Center expertise with neoadjuvant chemoradiation for resectable pancreatic most cancers was recently summarized. All eligible patients were required to have biopsy-proven adenocarcinoma of the pancreatic head. All four trials combined chemotherapy with radiotherapy within the neoadjuvant setting (Table 59-1). Immunotherapy Immune-based therapies can exploit both the cellular and humoral elements of the immune system. Strategies aimed at the mobile elements recruit and activate T cells that acknowledge tumor-speci c antigens. Strategies using monoclonal antibodies are being designed to goal tumor-speci c antigens that can kill tumor cells by direct lysis or by way of supply of a conjugated cytotoxic agent. Second, via the genetic recombination of their respective receptors, the B cells and T cells of the immune system are capable of recognizing a various array of potential tumor antigens. New information into the mechanisms by which T cells are efficiently activated and by which tumors evade immune recognition is driving the development of recent combinatorial approaches. Also, recent advances in gene-expression analysis have allowed for the identi cation of new pancreatic targets, including candidate tumor antigens that may function T-cell and antibody targets. In a section I trial of sufferers with surgically resected adenocarcinoma of the pancreas, 14 sufferers were handled with an allogeneic tumor cell vaccine transduced to secrete granulocyte-macrophage colony-stimulating factor. Moreover, the three long-term survivors had the strongest postvaccination responses. Countless brokers, both traditional chemotherapy and organic, are in varied levels of investigation. In this part a number of of the biological agents that have been studied in early-phase medical trials might be reviewed. Eleven sufferers (21%) had con rmed partial responses and 77% of the sufferers were alive at 6 months. K-ras Inhibitors An activating mutation of the K-ras is current in nearly 100% of pancreatic cancers. Although traditionally sufferers with these diseases had a dismal prognosis, proper staging and affected person selection have led to improved outcomes. When potential, surgical resection for treatment must be attempted as this gives the only chance of long-term survival. Surgical resection must be carried out by surgeons skilled within the management of those diseases and at centers that may aptly care for these sufferers to reduce morbidity and mortality. Approximately 20% of pancreatic cancers are Her-2 constructive, and preclinical studies have proven that inhibition of Her-2 signaling with Herceptin (trastuzumab) is associated with antitumor e ects in pancreatic cancer fashions. Two patients (6%) had a partial response, and the median survival and one-year survival had been 7 months and 19%. Contributions to the surgical procedure of the bile passages, particularly of the frequent bile duct. Reexploration for periampullary carcinoma: resectability, perioperative outcomes, pathology and long-term consequence. Multimodality staging optimizes resectability in sufferers with pancreatic and ampullary cancer. Is prophylactic gastrojejunostomy indicated for unresectable periampullary most cancers Randomized trial of endoscopic versus percutaneous stent insertion in malignant obstructive jaundice. Randomised trial of self-expanding metallic stents versus polyethylene stents for distal malignant biliary obstruction. Clinical end result of simultaneous selfexpandable steel stents for palliation of malignant biliary and duodenal obstruction.
5 mg kemadrin purchase with visa
Basically medications hair loss 5 mg kemadrin order otc, a change in the later sequences of larger than 20% medicine for stomach pain kemadrin 5 mg fast delivery, less than 20%, or in between correlates with persistent (blue), washout (red), or plateau (yellow/green) curves. This can go wrong if the scanning is began too early after distinction; a lesion that should present washout will show as plateau. A patient with very gradual circulate due to low cardiac output may peak on the second time point after contrast agent is given. In this case, the time level used to determine colour task can be changed from the primary to the second postcontrast sequence. As we change the enhancement vary assigned to plateau (pink boxes), the colour coding adjustments. The threshold is held regular at 60%, so the entire amount of colour on the pictures remains the same. This lesion is green (plateau) as a outcome of it increases in enhancement by 13% (yellow box) over the primary postcontrast image, falling within this �20% range. The lesion is due to this fact blue (persistent) as a result of 13% is exterior the �10% coding vary. The lesion is now green once more because 13% is less than the 30% threshold to be blue. A, Typically the primary postcontrast sequence is subtracted from the ultimate sequence to determine colour assignment. This may be useful for ladies with low cardiac output when the height distinction bolus occurs on the second sequence after distinction injection. There are dark traces at the skin-fat, fat-tissue, and fat-muscle interfaces (arrows). In the axial plane, the section encoding direction should be left to proper or the smear artifact will overlie the breast tissue. However, the breast needs to be centered inside the aperture and most women might want to be coached to scoot toward their ft. Soft cushioning with towels or light compression, coaching, and communication are all efficient ways of decreasing movement. It appears like a toddler took a permanent marker and drew black lines at each tissue interface. Where fats and water overlap, their out of-phase indicators cancel one another out, producing a darkish band at tissue interfaces. Chemical shift artifact could be corrected by increasing the bandwidth or the echo time so that the fat and water are in-phase. Phase encoding artifact is due to normal respiratory, vascular, and cardiac movement, which is always propagated in the part encoding direction. The part encoding path should subsequently be left-to-right in the axial airplane and top-to-bottom in the sagittal airplane. Wrap round or section wrap occurs when not all of the signal-producing tissue is within the field of view. The sign from this tissue becomes superimposed on the tissue within the area of view. Zebra artifact happens when excited tissue exterior the sector of view wraps into the realm of curiosity and there are tissues which may be both out and in of phase. Tissue from her right arm, which was down alongside her facet, was included within the field of view, leading to part wrap or aliasing of the arm over the left facet of the image (yellow arrows). Use a guide method with a molybdenum target/filter combination and the lowest potential kVp to enhance distinction for ladies with very skinny breasts and for specimen radiographs. Reduce scatter in magnification views by collimating the beam (coning) and using spot compression. Learn to recognize and proper artifacts corresponding to chemical shift that can degrade picture high quality. Zebra artifact is usually seen overlying the spine and thorax on these early slices (arrow). It may be that the images were obtained utilizing the body coil when the breast coil was not selected or the sphere of view is much too small. Radiofrequency interference is a really unusual artifact that could be difficult to recognize. Essentially, extraneous radio sign is leaking into the room or being generated throughout the room. Close-up of a left craniocaudal view (kVp 27, mAs 104, compression 41 mm, Hologic unit). A 69-year-old woman is recalled from screening due to a mass in the lateral left breast (arrow). Your sonographer brings you the following ultrasound image and states that the discovering is a cyst. How can we adjust the parameters to cut back the coloring of the background parenchyma with out changing the curve of the tissue on the indicator traces The repeat picture here obtained with a decrease publicity exhibits improved visualization of the subcutaneous tissues. Faint gridlines are seen as fine horizontal darkish lines extending throughout the image. [newline]Gridlines in the indirect airplane are seen as dark traces going from the decrease left corner to the upper proper corner. In this case, the gridlines are as a result of a malfunctioning grid somewhat than low publicity, which is correctable. The repeat image here was carried out with a better kVp, and the method is now enough. Although fibroadenomas can occasionally demonstrate some posterior acoustic shadowing, that is quite so much of shadowing, notably for a fibroadenoma in a younger woman. The round mass with ill-defined margins within the left breast corresponds to the palpable finding. On the ultrasound picture, this seems to characterize a cyst (and that is what the affected person was told). However, the focal zone is a bit low, and the image was obtained with harmonic imaging. Here is a repeat ultrasound picture obtained with out compound or harmonic imaging, which shows a solid mass with duct extension. Last, the time-gain curve must be adjusted so the fats lobules in any respect depths are the identical shade of gray. Note how the superficial fats is more echogenic than the deep fat on the preliminary image. Compound imaging was additionally used to enhance distinction and enhance analysis of the margins. The artifact could also be due to a leak in the door seal or electrical tools close by. Here are the outcomes: Only the overall quantity of color within the image has decreased. The indicated space increased in enhancement by 55% over baseline (open arrow) on each pictures. Screening mammography is essentially the most extensively used modality for detecting breast most cancers and the only one confirmed to scale back the mortality fee from the disease.
Buy kemadrin 5 mg free shipping
Economic evaluation of low-dose heparin vs the low-molecular-weight heparin enoxaparin for prevention of venous thromboembolism after colorectal surgery symptoms 3 weeks pregnant order kemadrin 5 mg. Relationship of apical lymph node involvement to survival in resected colon carcinoma medicine ball chair 5 mg kemadrin for sale. Comparison of prolonged colectomy and limited resection in sufferers with Lynch syndrome. Survival after excessive or low ligation of the inferior mesenteric artery during healing surgical procedure for rectal cancer. Neither pelvic nor abdominal drainage is required after anastomosis in elective, uncomplicated, colorectal surgical procedure. Pelvic drainage and other danger elements for leakage after elective anterior resection in rectal cancer patients: a potential research of 978 patients. Laparoscopy-assisted colectomy versus open colectomy for remedy of non-metastatic colon most cancers: a randomised trial. Laparoscopic surgical procedure versus open surgical procedure for colon most cancers: shortterm outcomes of a randomised trial. Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. Postoperative mortality and morbidity in French patients undergoing colorectal surgery: results of a prospective multicenter study. Acute colonic obstruction: scientific aspects and coste ectiveness of preoperative and palliative therapy with self-expanding metallic stents-a preliminary report. Placement of self-expanding metal stents for acute malignant large-bowel obstruction: a collective evaluate. Elective (planned) colectomy in patients with colorectal obstruction after placement of a self-expanding metallic stent as a bridge to surgical procedure: the outcomes of a potential examine. Comparison of short-and long-term outcomes following both insertion of self-expanding metallic stents or emergency surgery in malignant large bowel obstruction. Role of prolonged resection within the initial remedy of domestically superior colorectal carcinoma. In uence of hospital procedure volume on outcomes following surgical procedure for colon cancer. A randomized controlled trial of uorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. Bevacizumab plus irinotecan, uorouracil, and leucovorin for metastatic colorectal cancer. Prospectively randomized trial of postoperative adjuvant chemotherapy in sufferers with high-risk colon most cancers. Comparison of uorouracil with additional levamisole, higher-dose folinic acid, or each, as adjuvant chemotherapy for colorectal cancer: a randomised trial. Genomic pro ling associated with recurrence in patients with rectal most cancers handled with chemoradiation. Leucovorin and uorouracil with or without oxaliplatin as rst-line treatment in advanced colorectal most cancers. Survival of sufferers with advanced colorectal most cancers improves with the provision of uorouracil-leucovorin, irinotecan, and oxaliplatin in the course of therapy. With that said, not all patients will be ideal candidates and not all procedures may be performed by all surgeons. Surgeons with advanced abilities could also be snug doing a whole complete proctocolectomy and ileal pouch-anal anastomosis. All of these procedures have been technically described in this chapter to provide a variety of procedures that are feasible. As with any laparoscopic method, for example, there would be some cases where a pneumoperitoneum is contraindicated and others where the disease or technical issues characterize contraindications. Indications and contraindications and pre- and intraoperative evaluations speci c to the colon and rectal diseases and affected person circumstances are supplied, adopted by centered discussion on oncologic points relevant to colon and rectal most cancers and key points. For in ammatory bowel disease, the record of indications includes symptomatic failure of medical therapy; dysplasia; and presence of strictures, abscess, and stula. In acute colitis, pressing subtotal colectomy with end ileostomy may be performed initially as a half of a two- or three-stage procedure. Procedures could include strictureplasty, small bowel resection, segmental colonic resection, or proctocolectomy. Reduction in post-op adhesions recovering from acute diverticulitis ought to be made on a case-by-case basis and suggest the laparoscopic approach in selected patients. Solitary metastatic lesion in the liver with localized tumor within the colon can be resected laparoscopically in competent palms. Resection rectopexy and mesh rectopexy both can be carried out by way of the laparoscopic approach. Laparoscopic rectopexy has comparable long-term functional outcomes and low recurrence charges. Large multicenter trials are occurring in North America and Europe to consider the outcomes of rectal cancer for laparoscopic approach. Patients with advanced heart problems are also typically intolerant of the pneumoperitoneum, as it can prohibit the delicate dynamics of cardiac output. Finally, patients with end-organ renal failure and extreme electrolyte or uid disturbances and people with liver failure, ascites, or different sources of bleeding problems are finest served with a extra managed, open approach. Accordingly, open strains of communication between the surgeon and the anesthesiologist in addition to a willingness to convert to open surgical procedure must be the rule and not the exception. Less absolute or relative contraindications of laparoscopy embrace the presence of adhesions, cardiac abnormalities, pulmonary gas exchange abnormalities, continual liver illness, and weight problems. Rectal cancer (in controlled trials) Contraindications in rectal illnesses Chapter 37 Laparoscopic Colorectal Procedures 769 have prohibitive adhesions. At occasions, managing obese patients is facilitated by laparoscopy, corresponding to when the fats is predominantly in the stomach wall. A nal category of absolute and relative contraindications includes these speci c to the illness beneath treatment. For in ammatory bowel illness a large phlegmonous mass, complicated or giant abscess, or advanced stulizing illness are likely not appropriate for the majority of the specimen to be extracted, to not point out the challenges of mobilization. In addition to the preoperative testing, we advise that one never go away the operating room without rst con rming that the goal lesion has been con dently eliminated and identi ed in colonic location by more than one colonic section, this safety measure appears simple and warranted. Surgeons may identify small tremendous cial hepatic metastases or peritoneal tumors at the time of surgery, however that is less common than it was when laparoscopic surgery was initiated within the early Nineties. Early experiences with missed lesions and wrong-site resections brought these classes ahead. For malignant lesions Conversion of laparoscopic process to open procedure could additionally be required when di culties are encountered. A choice to convert is finest made early in the process, thus avoiding an increased danger of complications and reducing operative time. An early determination to convert will ensure that the rates of morbidity and mortality are maintained at acceptable levels.
5 mg kemadrin cheap with visa
However medicine show kemadrin 5 mg discount free shipping, pigment stones incessantly harbor viable micro organism and should potentially result in medications covered by blue cross blue shield buy kemadrin 5 mg free shipping subsequent infectious complications if allowed to remain in the peritoneal e long-term complications of retained stones, cavity. Other potential complications are pneumoperitoneum related (gas embolism, vagal reaction, ventricular arrhythmias, or hypercarbia with acidosis) and trocar related (injuries to the stomach wall, intra-abdominal organ, or main blood vessels). Perforation could occur secondary to traction utilized by the grasping forceps or because of electrosurgical thermal damage throughout removing of the gallbladder from its bed. In our experience, nearly one-third of the sufferers have had intraoperative spillage of bile or stones. When perforation does happen, the bile must be aspirated completely and irrigation used liberally. Regardless of the make of trocar, during its insertion one ought to never purpose toward the backbone or the placement of the nice vessels, and a hand is used as a brake to prevent inadvertently introducing the trocar too far. Insertion of the preliminary trocar, especially when performed in a closed trend, could cause iatrogenic harm to the bowel, bladder, aorta, iliac artery, or vena cava. In contrast, if the small-bore Veress needle enters a viscus or blood vessel, the operation can generally be accomplished and the patient monitored intently for signs of issues in the postoperative period. Prior to removal, each trocar ought to be visualized from the peritoneal aspect utilizing the laparoscope. If signi cant hemorrhage is seen, it might possibly usually be managed with cautery, intraoperative tamponade with a Foley catheter, or a through-and-through suture on all sides of the trocar insertion website. Of all of the potential issues, biliary accidents have acquired essentially the most consideration and are discussed at size elsewhere in this textual content. Constant awareness of these potential misidenti cations and technical causes of biliary injuries is one of the best technique of prevention. If a partial bile duct damage happens and is acknowledged intra-operatively, an instantaneous main restore, probably at the aspect of a T-tube ought to be carried out. A full transection of the bile duct is a rare harm and an end-to-end repair is a technically challenging procedure which will require help from an skilled hepatobiliary surgeon. When a bile duct injury is found within the postoperative period, a coordinated e ort by radiologists, endoscopists, and surgeons is important to optimize administration. Open Cholecystectomy Experience with open cholecystectomy is vast, spanning generations of surgeons and having been practiced in just about each nation throughout the world. In a collected collection of about 20,000 sufferers who underwent cholecystectomy between l946 and 1973 at 10 di erent institutions, from the United States and all through the world, the overall mortality price was l. In this latter group, the operative mortality fee for patients who underwent elective cholecystectomy was zero. In this research, morbidity and mortality were depending on age in addition to disease status. Perhaps probably the most signi cant complication that may come up during open or laparoscopic cholecystectomy is bile duct harm. Numerous reviews within the literature, including this massive population-based examine point out that the danger of bile duct damage throughout open cholecystectomy is between zero. While laparoscopy has already set a high bar for cholecystectomy as regards to perioperative and intraoperative outcomes, there are areas of surgical analysis inspecting ways that may doubtlessly make the procedure even less invasive. Chapter 48 Cholecystitis and Cholelithiasis 1007 Single-port Laparoscopic Surgery Single-port laparoscopy is a latest improvement in laparoscopic surgical procedure that entails introducing all operative devices and gadgets by way of a single pores and skin incision, normally at the umbilicus. From a technical standpoint, single-port surgery leads to all of the devices entering the operative eld consistent with the optics. Triangulation and traction or countertraction are made extra di cult, but new instrumentation is being developed to overcome these limitations. Chenodiol (chenodeoxycholic acid) for dissolution of gallstones: the national cooperative gallstone research. Falling cholecystectomy thresholds for the explanation that introduction of laparoscopic cholecystectomy. Increased cholecystectomy rates amongst medicare patients after the introduction of laparoscopic cholecystectomy. Increased cholecystectomy price after introduction of laparoscopic cholecystectomy. Prophylactic cholecystectomy or expectant administration for silent gallstones: a call analysis to assess survival. Impact of laparoscopic cholecystectomy on the administration of cholelithiasis in youngsters with sickle cell illness. Prophylactic cholecystectomy with gastric bypass operation: incidence of gallbladder disease. A multicenter, placebocontrolled, randomized double-blind, prospective trail of prophylactic ursodiol for the prevention of gallstone formation following gastricbypass-induced fast weight loss. Elective cholecystectomy during laparoscopic Roux-En-Y gastric bypass: is it worth the wait Management of cholelithiasis in coronary heart and lung transplant sufferers: with evaluation of laparoscopic cholecystectomy. Signi cance of asymptomatic biliary tract disease in heart transplantation recipients. By eliminating belly incisions, the hypothesis is that there will be much less ache, fewer complications and decreased morbidity related to belly incisions. Laparoscopic cholecystectomy is the standard for therapy of gallstone and gallbladder disease. Randomized trial of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Complications of laparoscopic cholecystectomy: a national survey of four,292 hospitals and an evaluation of 77,604 circumstances. Unusual abscess patterns following dropped gallstones during laparoscopic cholecystectomy. Retroperitoneal abscess as a complication of retained gallstones following laparoscopic cholecystectomy. Transvaginal natural ori ce translumenal endoscopic surgical procedure cholecystectomy: early evolution of the method. Management of acute cholecystitis within the laparoscopic period: results of a potential randomized clinical trial. Early versus delayed-interval laparoscopic cholecystectomy for acute cholecystitis. Routine early laparoscopic cholecystectomy for acute cholecystitis after conclusion of a randomized controlled trial. Role of prophylactic antibiotics in laparoscopic cholecystectomy: a meta-analysis. Preliminary expertise with intracorporeal laparoscopic ultrasonography using a sector scanning probe. A prospective comparison with intraoperative cholangiography within the detection of choledocholithiasis. Laparoscopic ultrasonography as in contrast with static or dynamic cholangiography at laparoscopic cholecystectomy.
Kemadrin 5 mg online
A selective method to the resection of cystic lesions of the pancreas: outcomes from 539 consecutive sufferers symptoms kidney failure cheap kemadrin 5 mg without a prescription. Mucinous cystic tumors of the pancreas: immunohistochemical assessment of the "ovarian-type stroma medicine effexor kemadrin 5 mg buy overnight delivery. Mucinous cystic tumors of the pancreas: clinicopathologic features, prognosis, and relationship to different mucinous cystic tumors. Clinical and pathological correlation of eighty four mucinous cystic neoplasms of the pancreas: can one reliably di erentiate benign from malignant (or premalignant) neoplasms Osteoclast-like big cell tumor of the pancreas related to a mucinous cystadenocarcinoma. Cystic neoplasms of the pancreas and tumor-like lesions with cystic features: a evaluate of 418 instances and a classi cation proposal. Pancreatic mucinous cystic neoplasm de ned by ovarian stroma: demographics, scientific features, and prevalence of cancer. Mucin producing neoplasms of the pancreas: an analysis of distinguishing clinical and epidemiologic characteristics. A evaluate of mucinous cystic neoplasms of the pancreas de ned by ovarian-type stroma: clinicopathological options of 344 patients. Cystic tumors of the pancreas: new clinical, radiologic and pathologic obsevations in 67 patients. Cyst uid analysis in the di erential prognosis of pancreatic cystic lesions: a pooled analysis. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, half 2: randomized controlled trial evaluating survival morbidity and mortality. Pancreaticoduodenectomy with or without extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma: comparability of morbidity and mortality and short-term consequence. Four circumstances of mucin-producing cancer of the pancreas on speci c ndings of the papilla of Vater. Pancreatic cysts: pathologic classi cation, di erential analysis, and scientific implications. Pathologically and biologically distinct kinds of epithelium in intraductal papillary mucinous neoplasms: delineation of an "intestinal" pathway of carcinogenesis in the pancreas. An illustrated consensus on the classi cation of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Intraductal papillary mucinous neoplasms of the pancreas: pathology and molecular genetics. Global genomic analysis of intraductal papillary mucinous neoplasms of the pancreas reveals signi cant molecular differences in comparability with ductal adenocarcinoma. Clinical fate of department duct and blended types of intraductal papillary mucinous neoplasia of the pancreas. Do consensus indications for resection in branch duct Intraductal papillary mucinous neoplasm predict malignancy Intraductal papillary mucinous neoplasms: predictors of malignancy and invasive pathology. Natural history of branch duct Intraductal papillary mucinous neoplasms of the pancreas without mural nodules: long-term follow-up outcomes. Cyst measurement signifies malignant transformation in branch duct intraductal papillary mucinous neoplasms of the pancreas with out mural nodules. Branch-duct intraductal papillary mucinous neoplasms of the pancreas: to function or not to function Experience with 208 resections for intraductal papillary mucinous neoplasms of the pancreas. Adjuvant chemoradiotherapy after pancreatic resection for invasive carcinoma associated with intraductal papillary mucinous neoplasms of the pancreas. Clinical signi cance of frozen part evaluation during resection of intraductal papillary mucinous neoplasm: should a constructive pancreatic margin for adenoma or borderline lesion be resected additionally Solid pseudopapillary tumors of the pancreas: evaluate of 718 patients reported in English literature. Solid and pseudopapillary tumor of the pancreas: review and new insights into pathogenesis. Solid and pseudopapillary tumor of the pancreas: a case sequence of 26 consecutive patients. Cystic pancreatic endocrine tumors: an endoscopic ultrasound-guided ne-needle aspiration biopsy examine with histologic correlation. Acinar cell carcinoma of the pancreas within the United States: prognostic factors and comparability to ductal adenocarcinoma. Acinar cell carcinoma with a distinguished intraductal progress pattern: case report with evaluate of the literature. Pancreatic cysts attributable to carcinoma of the pancreas: a pitfall within the analysis of pancreatic carcinoma. Main-duct intraductal papillary mucinous neoplasms of the pancreas: scientific predictors of malignancy and long-term survival following resection. Pancreatic ductal adenocarcinomas in long-term followup patients with branch duct intraductal papillary mucinous neoplasms. Predictors of the presence of concomitant invasive ductal carcinoma in intraductal papillary mucinous neoplasm of the pancreas. Synchronous and metachronous extrapancreatic malignant neoplasms in patients with intraductal papillary-mucinous neoplasm of the pancreas. Frequency of extrapancreatic neoplasms in intraductal papillary mucinous neoplasm of the pancreas: implications for administration. Intraductal papillary mucinous tumors of the pancreas: imaging research and therapy methods. Cystic neoplasm of the pancreas: a Japanese multiinstitutional study of intraductal papillary mucinous tumor and mucinous cystic tumor. Mucin-hypersecreting tumors of the panceas: assessing the grade of malignancy preoperatively. Predictive factors for malignancy in intraductal papillary-mucinous tumors of the pancreas. Intraductal papillary mucinous neoplasms of the pancreas with multifocal involvement of branch ducts. Intraductal papillary mucinous neoplasms of the pancreas: di erentiation of malignant and benign tumors by endoscopic ultrasonography nding of mural nodules. Intraductal papillary mucinous neoplasms of the pancreas: efficiency of pancreatic uid analysis for constructive analysis and the prediction of malignancy. Cameron Periampullary cancers are composed of a group of malignant neoplasms arising in the region of the ampulla of Vater. Less generally, acinar cell carcinomas or pancreatic endocrine neoplasms occur in the periampullary area of the pancreas. Periampullary cancers are sometimes mentioned as a bunch based on their related presentation, workup, and surgical management. In addition, pancreas most cancers can be mentioned with this group because the pure historical past for both proximal and distal pancreatic lesions is similar-di ering primarily in the sort of resection carried out. He described a local ampullary resection with reanastomosis of the pancreatic and bile ducts to the duodenum in a patient who presented with obstructive jaundice.
Kemadrin 5 mg cheap mastercard
One normally suture-ligates the superior hemorrhoidal vessels in order to ensure hemostasis symptoms detached retina purchase kemadrin 5 mg visa. After dividing the superior hemorrhoidal artery medicine 3605 v 5 mg kemadrin purchase amex, you will want to nd the right airplane of dissection on the sacral promontory. Only 25% of patients have distinct branches of the center rectal vessels in these ligaments. When performing a cancer resection, one should take both layers of this membranous fascia o the seminal vesicles and higher prostate if potential. A number of pathologic research reveal that tumor spread inside the mesorectum not often extends beyond four cm distal to the caudal fringe of the tumor; often most nodes or mesorectal implants are within 3 cm of the distal fringe of the tumor. Fewer than 2�4% of tumors will have mucosal or submucosal spread beyond 2 cm distally. Once the rectum has been mobilized, a tumor measured at 5 cm by inflexible proctoscopy usually may be moved to 8 cm from the dentate line, a distance that permits an sufficient resection margin and sphincter preservation. When the distal extent of the tumor and the location of transection have been established, electrocautery is used to dissect the mesorectal fat away from the rectum. It is essential to maintain the dissection of the mesorectum perpendicular to the site of transection. A 3-0 Prolene is used to take full-thickness, 1- to 2-mm bites to trend a purse-string stitch across the anvil. If there are any gaps, a further 3-0 Prolene suture can be utilized to take another full-thickness chew, and this suture may be tied across the shaft as properly. One can even carry out an analogous placement of the anvil on the antimesenteric facet of the colon for a side-to-end anastomosis. Rectum re ected anteriorly and posterior avascular airplane entered between the presacral fascia of Waldeyer and the fascia propria of the rectum. Attention then is turned to the pelvis, which is irrigated and inspected for hemostasis. A rectal examination is carried out, and the anus is dilated gently with two to three ngers in order to accommodate the stapler. C B that the trocar will exit either 2�3 mm anterior or posterior (we elect to do this posteriorly in girls so as to keep away from the vaginal wall) to the staple line. When the trocar protrudes through the bowel wall, make sure that the trocar is fully superior in order that its bottom is visualized. If bubbles are detected, extra sutures are placed in suspected areas, and a diverting loop ileostomy is constructed. After the trocar of the circular stapler penetrates behind the staple line, the trocar is removed before reconnecting the anvil to the shaft. Other risk elements for anastomotic breakdown embody a history of radiation, perioperative steroid use, malnutrition, elderly ladies with a thin rectovaginal septum, or elderly sufferers undergoing preoperative combined-modality remedy with deliberate postoperative chemotherapy. Ileostomies can be closed within 8 weeks however typically are left in place until the patient completes adjuvant chemotherapy. A Gastrogra n (diatrizoate meglumine) enema is used to examine the patency and integrity of the anastomosis prior to takedown of the anastomosis. Coloanal Anastomosis Anastomoses at or simply above the anorectal ring typically result in increased frequency of stool, incontinence or soilage, and impaired quality of life owing to an insu cient reservoir. Diet restrictions and time after surgery normally will improve these signs, but two alternative strategies of reconstruction handle these postoperative problems and sometimes allow for improved operate to be attained extra quickly. For all other resections, placement of a drain could also be decided on a case-by-case basis. A double-stapled anastomosis as described or a hand-sewn anastomosis then is performed. Multiple potential, randomized research have demonstrated superior perform of a coloanal J-pouch over a straight coloanal anastomosis, especially within the rst 6 months after ileostomy takedown. Postoperative Care e nasogastric tube is removed on the end of the procedure or on postoperative day 1, and the patient can drink sips of clear liquids. Sequential compression gadgets are worn by the affected person until the patient is ambulating well. If an epidural has been When the pelvis is too slim for a J-pouch or the length of the pouch is inadequate, a transverse coloplasty may be customary. In addition to these perioperative issues, signi cant long-term morbidity is related to a everlasting colostomy. In a affected person survey, 66% of sufferers complained of signi cant leaks from their stoma appliance, 67% experienced sexual dysfunction, and only 40% of patients working preoperatively in the end returned to work. Variations in recurrence rates rely upon location of the tumor inside the rectum, changes in surgical approach, and the addition of adjuvant remedy. Technique e affected person is marked preoperatively by the enterostomal nurse for a permanent colostomy. Please see the section Low Anterior Resection With Total Mesorectal Excision for particulars regarding extra preoperative care, positioning, incision, and rectal mobilization. Once this level is reached, the perineal excision eld can start both by the surgeon or by a second team. A marking pen is used to draw an ellipse 2 cm outside the tremendous cial external sphincter and increasing from the perineal physique anteriorly, coccyx posteriorly, and ischial tuberosities laterally. Two Gelpi retractors are placed at forty five degrees to the anus so as to facilitate deep dissection. A pair of huge scissors is used to poke by way of the ligament; the scissors are absolutely unfold and, while wide open, are pulled straight back. Hooking the index and middle ngers under the levator muscles and transecting with electrocautery frees the rectum laterally. An assistant retracts the skin and subcutaneous tissue anteriorly with an army-navy retractor. Care is taken to hold the posterior wall of the vagina or the prostate anterior to the aircraft of dissection. A tongue of omentum or omental pedicle ap may be used to cowl the pelvis to prevent the small bowel from dropping deep into the pelvis if radiation is contemplated. Omentum also helps healing, particularly in an irradiated perineum or when patients also have undergone prostate or vaginal resections. If using a two-team approach, the perineal wound may be closed after the pelvis has been irrigated and hemostasis achieved. Two layers of interrupted 2-0 Vicryl suture are used to approximate the subcutaneous tissue. One layer of 3-0 Vicryl in a vertical mattress trend is used to approximate the pores and skin. Because this space is usually radiated, a quantity of layers lower the risk of the wound breakdown extending into the pelvis.
Trusted 5 mg kemadrin
As mentioned within the earlier part symptoms insulin resistance kemadrin 5 mg cheap without prescription, the three major issues that need to treatment internal hemorrhoids kemadrin 5 mg quality be palliated include obstructive jaundice, gastric outlet obstruction, and ache. Nonoperative Palliation of Obstructive Jaundice Nonoperative biliary drainage may be achieved either via a percutaneous or an endoscopic strategy. Percutaneous transhepatic approaches are aided by the truth that the intrahepatic ducts are usually dilated in sufferers presenting with obstructive jaundice. In a randomized trial evaluating endoscopic versus percutaneous stent placement in 70 sufferers, the success rate, overall complication rate, and procedure-related mortality rate was signi cantly decrease within the endoscopic group. Plastic stents are generally momentary and are available in di erent diameters and lengths. Because the diameter of the accent channel of endoscopes is limited, normally the most important plastic stent that could be positioned is 12F. Polyurethane-covered stents are currently being developed and used, they usually most likely have better patency and results. Division of the bile duct and removing of the stent can simply be carried out at the time of operation. Nonoperative Palliation of Duodenal Obstruction Until lately, duodenal obstruction in sufferers discovered to be un t for surgical bypass was handled with placement of gastrostomy tubes. Gastroduodenal stenting is profitable in 80�90% of sufferers and supplies enough reduction of obstruction in most sufferers. Several randomized managed scientific trials evaluating percutaneous celiac plexus nerve blocks to commonplace oral analgesics have demonstrated signi cant diminution in ache and narcotic use in the majority of the patients. Twelve percent of sufferers had a clinically signi cant postoperative pancreatic stula. Other problems included intra-abdominal abscess (5%), small bowel obstruction (5%) and new-onset diabetes (7%). A postoperative pancreatic stula following distal pancreatectomy is managed in the same manner as that following a pancreaticoduodenectomy. Despite low mortality charges, the incidence of postoperative complication remains high. In a series of 650 consecutive pancreaticoduodenectomies, the mortality price was 1. Patients are usually handled with parenteral nutritional assist and nasogastric decompression until the situation resolves. Erythromycin, a motilin agonist, has been proven to enhance gastric emptying after pancreaticoduodenectomy and is sometimes used. In the great majority of patients, the pancreatic leak will seal with conservative administration. Most facilities place intraoperative closed-suction drains close to the pancreatic anastomosis to management potential leaks. Comparison of duodenal stent placement with surgical gastrojejunostomy for palliation in patients with duodenal obstructions brought on by pancreaticobiliary malignancies. Prospective randomized double-blind trial of neurolytic coeliac plexus block in patients with pancreatic most cancers. Six hundred fty consecutive pancreaticoduodenectomies in the Nineties: pathology, problems, outcomes. Erythromycin accelerates gastric emptying following pancreaticoduodenectomy: a potential, randomized placebo managed trial. Carcinoma of the ampulla of Vater: factors in uencing long-term survival of 127 sufferers with resection. Molecular biology and the analysis and remedy of adenocarcinoma of the pancreas. Risk of pancreatic cancer following diabetes mellitus: a nationwide cohort research in Sweden. Pancreatitis and the risk of pancreatic cancer: International Pancreatitis Study Group. Core signaling pathways in human pancreatic most cancers revealed by global genomic analysis. Carcinogenesis of cancer of the papilla and ampulla: pathophysiological information and molecular biological mechanisms. Identi cation of k-ras mutations in pancreatic juice early in the diagnosis of pancreatic cancer. Detection of k-ras mutations within the stool of sufferers with pancreatic adenocarcinoma and pancreatic ductal mucinous cell hyperplasia. Values and limitations of 18Fuorodeoxyglucose-positron-emission tomography with preoperative analysis of patients with pancreatic plenty. E ect of preoperative biliary decompression on pancreaticoduodenectomy-associated morbidity in 300 consecutive sufferers. Preoperative biliary stents in patients undergoing pancreaticoduodenectomy: increased threat of postoperative problems Predicting resectability of periampullary cancer with three-dimensional computed tomography. Utility of staging laparoscopy in subsets of peripancreatic and biliary malignancies. Prospective trial of a blood supply-based technique of pancreaticojejunostomy: e ect on anastomotic failure within the Whipple process. A prospective randomized trial of pancreaticogastrostomy versus pancreaticojejunostomy after pancreaticoduodenectomy. Relation of perioperative deaths to hospital volume amongst sufferers undergoing pancreatic resection for malignancy. Relationship between hospital volume and late survival after pancreaticoduodenectomy. Pancreatic cancer-adjuvant mixed radiation and chemotherapy following healing resection. Interferon-based adjuvant chemoradiation therapy after pancreaticoduodenectomy for pancreatic adenocarcinoma. A multivariate mannequin for figuring out threat of early death after pancreaticoduodenectomy and adjuvant remedy for periampullary adenocarcinoma: significance for understanding post remedy outcomes. Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer: a randomised controlled trial. Role of adjuvant chemoradiation remedy in adenocarcinomas of the ampulla of Vater. Signi cance of histological response to preoperative chemoradiotherapy for pancreatic cancer. Novel allogeneic granulocyte-macrophage colony-stimulating factor-secreting tumor vaccine for pancreatic cancer: a phase I trial of security and immune activation. Erlotinib plus gemcitabine in comparison with gemcitabine alone in sufferers with advanced pancreatic most cancers. Even with the prognosis, administration can be di cult because localization is the important thing to the remedy. Benign and malignant neuroendocrine tumors appear histologically related, as clustered nests of regular islet cells.
Buy kemadrin 5 mg mastercard
Functioning insulinoma-incidence medications just for anxiety 5 mg kemadrin cheap otc, recurrence 9 medications that can cause heartburn kemadrin 5 mg generic amex, and long-term survival of sufferers: a 60-year examine. Left-sided pancreatectomy: a multicenter comparison of laparoscopic and open approaches. Surgical experience with pancreatic and peripancreatic neuroendocrine tumors: evaluation of a hundred twenty five sufferers. Preoperative detection of gastrointestinal neuroendocrine tumors using endoscopic ultrasonography. Angiography and arterial stimulation venous sampling in the localization of pancreatic neuroendocrine tumours. Evans Dr Wolfgang, Dr Schulick, and Dr Cameron provide an extremely complete chapter on the analysis and therapy of sufferers with cancer of the periampullary area and speci cally the pancreatic head. As all of you understand, over the past two to three a long time, Dr Cameron has demonstrated the way to surgically manage sufferers with pancreatic cancer to achieve optimal consequence. Importantly, there has been an incredible advance in each the understanding of the molecular biology of pancreatic most cancers as properly as our capability to precisely picture the pancreas and periampullary area previous to surgical procedure. Such accurate assessment of the related anatomy is essential for both pretreatment staging and for planning the technical steps in performing pancreaticoduodenectomy, especially if vascular resection and reconstruction could additionally be indicated. Although very experienced surgeons such as the authors can accurately assess resectability on the time of laparotomy, the ability to preoperatively classify sufferers as resectable, borderline resectable or regionally superior permits for the appropriate triage of sufferers for optimal therapy sequencing (surgery rst or after neoadjuvant therapy), the analysis of sufferers for investigatorinitiated and cooperative group medical trials, and for the referral of sufferers to higher quantity facilities. In an attempt to clarify the anatomy of resectable, borderline 61A resectable, and locally advanced disease, Varadhachary and colleagues from the University of Texas M. However, this de nition was developed for the conduct of clinical trials of neoadjuvant therapy sequencing and was not intended to assist a surgery- rst strategy for sufferers who could require vascular resection and reconstruction. Katz and colleagues in 2008 reported a hundred and sixty patients with borderline resectable illness (using the Varadhachary de nition) and introduced three subtypes of the borderline class, often referred to as Katz varieties A, B, and C. Type C sufferers had been borderline resectable due to a marginal efficiency standing or signi cant preexisting medical comorbidity thought to require protracted analysis that precluded immediate surgical procedure. By de nition, kind C sufferers have been thought to have reversible causes of their present symptoms corresponding to hyperbilirubinemia-induced anorexia and fatigue. Katz and colleagues provided compelling information in support of induction chemotherapy (followed by chemoradiation) for patients with borderline resectable illness. De nitions: abutment, 180� or 50% of the vessel circumference; encasement, >180� or >50% of the vessel circumference. Many incorporate a interval of induction systemic remedy, particularly in these with arterial abutment, to include no much less than 2 months of chemotherapy before chemoradiation. Experience using chemotherapy alone is relatively untested, the plain concern being the danger for native tumor recurrence. Probably an important technical facet of pancreaticoduodenectomy is the dissection of superior mesenteric artery. Adenocarcinoma of the pancreas has a predisposition to unfold along neural tissue, and this is probably liable for the excessive frequency of local recurrence. As our systemic therapies turn out to be more e ective, native recurrence might become a more dominant pattern of failure. It is inconceivable to argue with the approach described by Dr Wolfgang because the operation of pancreaticoduodenectomy is arguably accomplished better at Johns Hopkins Hospital than some other establishment within the Chapter 61A Perspective on Pancreatic Neoplasms 1229 world. Students, residents, and even skilled surgeons will bene t greatly by careful evaluation of this chapter. Chapter fifty eight by Dr Maley and Dr Yeo is equally complete in their excellent discussion of cystic neoplasms of the pancreas. Regarding serous cystadenoma, this histology demonstrates fascinating tumor biology. However, they are often locally invasive and erode into adjacent bowel (duodenum, transverse colon, stomach) and sometimes can obstruct the splenic vein (resulting in sinistral portal hypertension) or the superior mesenteric and/or portal veins (resulting in extrahepatic portal hypertension). In 2011, the diagnosis of a serous cystadenoma is usually not di cult; nevertheless, understanding when to intervene with surgical procedure is often challenging. As patient age and operative danger (medical comorbidities) increase, the bene t to surgery in an otherwise asymptomatic patient may be low. In our practice, we try to rigorously weigh threat versus bene t in asymptomatic sufferers. A advice for remark is all of the extra compelling in sufferers of advanced stage and with medical comorbidities. Because this is a premalignant neoplasm, it will be very di cult to assist a advice of remark in a patient of this age. In patients without cancer, we do have to pay extra attention to preservation of islet cell mass in an e ort to keep away from the intermediate and long-term issues of insulin-dependent diabetes (in addition to the lifestyle adjustments introduced with insulin dependence). Our selection for operation in this affected person would be a center phase pancreatectomy with pancreaticojejunostomy for the distal pancreas and creation of a serosal patch sewn to the proximal pancreatic transection site. However, the increasing use of cross-sectional imaging has resulted in many more patients being diagnosed with cystic neoplasms of the pancreas. Is there a job for enucleation or ablative therapies in sufferers where the chance for invasive carcinoma is approaching zero If the right or left facet of the pancreas requires resection, we commonly ship the pancreatic transection margin for frozen-section evaluation. When performing an prolonged distal pancreatectomy, one must make sure that the proximal pancreatic transection margin shall be adverse, particularly if the affected person may be treated with an extended pancreaticoduodenectomy and thereby preserve some islet cell mass. In common, the preservation of some islet cell mass does facilitate improved blood sugar control even if not obviating the need for insulin. Further, why should the biology of sufferers with Zollinger-Ellison syndrome di er primarily based on whether or not the first tumor is in the pancreas or the duodenum and what determines where the tumor arises Equally mystifying is why duodenal gastrinomas are so small, often lower than 1 cm in diameter and infrequently associated with liver metastases. Gastrinomas, when located within the pancreas, are normally discovered within the pancreatic head or uncinate process (gastrinoma triangle) and people 3 cm in size and larger are incessantly related to liver metastases. Consistent with the biology of duodenal gastrinoma, sufferers with carcinoid tumors of the duodenum additionally rarely have synchronous or metachronous liver metastases although lymph nodes metastases are very common. Recent studies counsel that pancreatic, but not duodenal, gastrinomas categorical pancreatic-duodenal homeobox1 (Pdx1) and that solely duodenal gastrinomas categorical sonic hedgehog signifying a di erent molecular origin for the 2 tumors. Such sufferers may be di erentiated from those with Zollinger-Ellison syndrome by the absence of gastric acid manufacturing. In the outpatient heart, placement of a nasogastric tube with aspiration of gastric juice for pH testing will easily make this diagnosis. A pancreatic or duodenal producing tumor is a much much less frequent reason for hypergastrinemia. Careful attention to regional lymphadenectomy is an underemphasized and essential element of their surgical management. It is critically essential to con rm the diagnosis of insulinoma by allowing the glucose to decline to a degree of lower than forty five mg/dL (at which point the patient is often symptomatic) and observing the reduction of symptoms with the Chapter 61A Perspective on Pancreatic Neoplasms 1231 administration of glucagon. Intravenous glucagon is related to an elevation of serum glucose of roughly 20 mg/dL. However, if the insulinoma is incompletely enucleated, an area recurrence can develop; such native recurrences might not happen for years after the primary operation. When we carry out an enucleation of a benign insulinoma, we usually use bipolar forceps and are extraordinarily cautious to keep away from violation of the tumor capsule. Proper technique for enucleation is rather more essential than whether or not the operation is done laparoscopically or open. In the event of a pancreatic stula, the presence or absence of an stomach incision becomes insigni cant.