
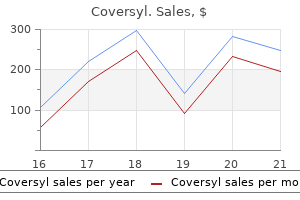
Coversyl dosages: 8 mg, 4 mg
Coversyl packs: 10 pills, 30 pills, 60 pills, 90 pills

Coversyl 8 mg buy generic
Complications from vestibulectomy embody occlusion of the Bartholin gland leading to treatment without admission is known as 4 mg coversyl generic mastercard growth of cysts symptoms quiz purchase coversyl 4mg line. Most are thought to be acquired and current in ladies between 30 and 60 years of age (Lee, 2005). They often current as a mass of the anterior vaginal wall and characterize approximately 84% of periurethral plenty (Table 18. Most urogynecologists have noted a decline in the prevalence of this situation since the early 1990s. The majority of cases are initially recognized in reproductive-age females, with the height incidence in the fourth decade of life. The symptoms of a urethral diverticulum are nonspecific and are equivalent to the symptoms of a decrease urinary tract an infection. To diagnose this elusive situation, one ought to suspect urethral diverticulum in any lady with persistent or recurrent decrease urinary tract symptoms. The anatomy of the urethra has been described as a tree with many stunted branches that represent the periurethral ducts and glands. It is assumed that the majority of urethral diverticula outcome from repetitive or continual infections of the periurethral glands. The suburethral infection could trigger obstruction of the ducts and glands, with subsequent manufacturing of cystic enlargement and retention cysts. These cysts could rupture into the urethral lumen and produce a suburethral diverticulum. Malignancy has been reported in 6% to 9% of instances, principally adenocarcinoma (Foley, 2011). The most typical signs associated with urethral diverticula are urinary urgency, frequency, and dysuria occurring about 90% of the time as the presenting symptom. Other authors have stressed the three Ds associated with a diverticulum: dysuria, dyspareunia, and dribbling of the urine. It is attention-grabbing that in most massive collection, roughly 20% of the ladies are asymptomatic. A classic sign of a suburethral diverticulum is the expression of purulent material from the urethra after compressing the suburethral space during a pelvic examination. Although the sign of manufacturing a discharge by guide expression is particular, its sensitivity is poor. Historically, the 2 commonest methods of diagnosing urethral diverticulum have been the voiding cystourethrography and cystourethroscopy. Approximately 70% of urethral diverticula shall be crammed against this materials on a postvoiding radiograph with a lateral view. Cystourethroscopy will show the urethral opening of the urethral diverticulum in roughly 6 of 10 circumstances. Ultrasonography, carried out translabially (or introitally) might assist in the assessment of the mass being cystic or solid. Positive-pressure urethrography is finished with a particular double-balloon urethral catheter (Davis catheter). Classically, the recordings of the stress profile of the urethra reveal a biphasic curve in a lady with a urethral diverticulum. If a woman has a urethral diverticulum and urinary incontinence, performing a stress urethral strain profile will help to differentiate the etiology. The differential analysis contains the Gartner duct cyst, an ectopic ureter that empties into the urethra, and Skene glands cysts. Operative methods may be divided into transurethral and transvaginal approaches, with most gynecologists preferring the transvaginal method as described by Lee (Lee, 2005). Following operations, roughly 80% of patients get hold of complete relief from signs. The recurrence fee varies between 10% and 20%, and heaps of failures are as a outcome of incomplete surgical resection. The most serious consequences of surgical repair of urethral diverticula are urinary incontinence and urethrovaginal fistula. Postoperative incontinence normally follows operative repairs of huge diverticula which are close to the bladder neck. The cysts are often found within the posterior or lateral partitions of the decrease third of the vagina. Similar to inclusion cysts of the vulva, inclusion cysts of the vagina are extra frequent in parous women. Obstetrics & Gynecology Books Full 18 Benign Gynecologic Lesions that the central material is sebaceous. Similar to vulvar inclusion cysts, the cause is either a small tag of vaginal epithelium buried beneath the surface following a gynecologic or obstetric process or a misplaced island of embryonic remnant that was destined to type epithelium. Whether the cysts arise from the mesonephros (Gartner duct cyst), the paramesonephricum (M�llerian cyst), or the urogenital sinus (vestibular cyst) is predominantly of academic quite than medical importance. Occasionally pressure produced by the cystic fluid produces flattening of the epithelium, which makes histologic diagnosis much less dependable. The cysts are usually 1 to 5 cm in diameter and are usually found in the upper half of the vagina. A giant cyst presenting on the introitus may be mistaken for a cystocele, anterior enterocele, or obstructed aberrant ureter. Embryonic cysts of the vagina, especially these discovered on the anterior lateral wall, are normally Gartner duct cysts. In the embryo the distal portion of the mesonephric duct runs parallel with the vagina. It is assumed that a phase of this embryonic structure fails to regress, and the obstructed vestigial remnant turns into cystic. Most of these benign cysts are asymptomatic, sausageshaped tumors which are found solely incidentally throughout pelvic examination. In a sequence of 25 ladies present process operations for symptomatic dysontogenetic cysts, a variety of signs had been reported, including dyspareunia, vaginal pain, urinary symptoms, and a palpable mass. Rarely, considered one of these cysts turns into contaminated, and if operated on during the acute phase, marsupialization of the cyst is most well-liked. Excision of the vaginal cyst may be a a lot more formidable operation than anticipated. The cystic structure could extend up into the broad ligament and anatomically be in proximity to the distal course of the ureter. The latter, related to toxins elaborated by Staphylococcus aureus, is mentioned in Chapter 23. Wearing tampons for a couple of days has been related to microscopic epithelial changes. The majority of women develop epithelial dehydration and epithelial layering, and some will develop microscopic ulcers. In a research of colposcopic changes related to the tampon, Friedrich found serial adjustments of epithelial drying, peeling, layering, and finally microulceration (Friedrich, 1981). In his study, 15% of women sporting tampons only during the time of normal menstruation developed microulcerations.
Syndromes
- Pain with ejaculation
- Burns in the mouth and throat
- Erythema nodosum
- Ulipristal is taken as a single tablet.
- Infection
- Electrolysis
- Painful, very red, swollen, and warm skin underneath the sore (lesion)
Purchase coversyl 4mg on line
Mastectomy may be essential in cases of constructive margins after additional surgical reexcision symptoms 14 dpo order coversyl 8mg online. Contraindications to lumpectomy embrace the necessity for radiation therapy during pregnancy medications 230 coversyl 8 mg order with amex, intensive illness not amenable to resection by a local excision with a single incision leading to satisfactory cosmetic end result, and diffuse suspicious or malignant appearing microcalcifications. Sentinel node biopsy has decreased the need for full axillary lymphadenectomy. By injecting with radioactive colloid tracers and dyes, the surgeon can determine the first set of regional lymph nodes that obtain lymphatic drainage from the tumor. In a large multi-institutional trial, Krag and colleagues have been able to identify the sentinel nodes in 93% of the circumstances. The accuracy of sentinel node mapping on this collection for predicting the status of axillary nodes was 97%. The positive predictive value was one hundred pc, and the adverse predictive value was 96% (Krag, 1998). No difference was noted in local recurrence, disease-free survival, or total survival. Breast reconstruction should be thought of for any lady undergoing mastectomy for breast cancer. Variousfactors influence the kind of reconstruction including patient desire, smoking history, physique habitus, comorbidities, and radiation remedy plans. Obesity and smoking increase the risk of wound therapeutic problems and flap failure. Postmastectomy reconstruction with implants could be performed by either instant placement of a everlasting subpectoral implant or by placement of a subpectoral tissue expander implant. The pectoral muscle is stretched with gradual growth of the expander implant by the addition of saline. In sufferers present process postmastectomy radiation, placement of a tissue expander on the initial process followed by implant placement after completion of radiation therapy is most well-liked. If autologous tissue is used, reconstruction should be delayed till no much less than 6 months following completion of radiation therapy. Radiation Therapy the majority of women handled with breast-conserving surgery are candidates for breast radiation remedy. After breast-conserving surgical procedure, external beam complete breast irradiation is usuallyadministered. Additionally, a significant reduction within the 15-year danger of breast most cancers dying (21. Randomized trials have shown each a diseasefree and general survival benefit of chest wall and regional node irradiation in these girls. Chest wall irradiation can be beneficial in women with adverse nodes however with major tumor higher than 5 cm or optimistic surgical margins. Medical Therapy Along with earlier detection, developments in systemic adjuvant remedy have resulted in a decrease within the breast cancer mortality rate. Clinicopathologic factors together with stage, tumor grade, and vascular house invasion are used to calculate the danger of disease recurrence. Hormonal Therapy the presence and concentration of receptors ought to be obtained at the preliminary diagnostic biopsy or surgery. When estrogen receptors are optimistic, roughly 60% of breast cancers will respond to hormonal remedy; an 80% response fee is noted when each estrogen and progesterone receptors are present. If estrogen receptors are negative, less than 10% of tumors respond to hormonal manipulation. Hormonal remedy is often completed by drugs that change endocrine perform by blocking receptor sites or blocking synthesis of hormones. Hormonal remedy is efficient in producing a response in superior metastatic carcinoma for roughly 1 year. Metastatic disease in soft tissue and bone is essentially the most sensitive to hormonal manipulation. Tamoxifen, a selective estrogen receptor modulator, is a incessantly prescribed hormonal agent for breast carcinoma. Treatment with tamoxifen was associated with an increased danger of thromboembolic illness, strokes, intrauterine polyps, as well as endometrial hyperplasia and carcinoma. The general incidence of uterine cancer was low and confined to girls over fifty five years. Most tamoxifen-related endometrial cancers were stage I, grade 1, and had been efficiently treated with surgical procedure alone. As one would count on, tamoxifen is of higher benefit in women with tumors which have estrogen receptors than in tumors that are adverse for estrogen receptors. However, even in receptor-negative patients, 5 years of tamoxifen use will decrease the danger of a second primary or contralateral breast most cancers by as much as 45%. Trials of tamoxifen in the adjuvant treatment setting for breast cancer confirmed that 10 years of tamoxifen improved outcomes in comparison with 5 years. The reductions in adverse breast most cancers outcomes appeared to be much less extreme before than after 12 months 10 with halve breast cancer mortality during the second decade after analysis. Basedontheseresults and people of other major trials, the American Society of Clinical Oncology updated the follow tips on the optimum duration of remedy of adjuvant endocrine therapy, notably adjuvant tamoxifen (Burstein, 2014). Pre-orperimenopausalwomenwho have acquired 5 years of adjuvant tamoxifen should be offered tamoxifen for a duration of 10 years. Cessationof ovarian operate may be definitively attained by oophorectomy or pelvic radiation. Several trials have proven important enchancment in end result and have been stopped early due to the improved outcomes in contrast withplacebo. Treatment with trastuzumab is associated with a higher threat of cardiotoxicity together with congestive heart failure and a decrease in left ventricular ejection fraction. Chemotherapy Chemotherapy is utilized in the therapy of breast most cancers in each the adjuvant and neoadjuvant settings. It is utilized to estimate each the risk of recurrence of early-stage breast most cancers and the benefit from adjuvant chemotherapy. TheMammaPrinttestanalyzes70genes(Amsterdam70gene prognostic profile) and calculates both a high-risk or low-risk recurrence rating for early stage breast most cancers. Combination therapy of cytotoxic medicine is vastly superior to single-agent regimens. The addition of 4 to five cycles of paclitaxel to four to six cycles of the Adriamycin and cyclophosphamide routine improved disease-free and overall survival rates in patients with node-positive breast most cancers. Overall, chemotherapy regimens based mostly on anthracyclines and taxanes cut back breast cancer mortality by about one third. In the neoadjuvant setting, chemotherapy has the potential to change unresectable tumors to resectable ones and reduce the extent of surgery essential to obtain sufficient resection. Neoadjuvant remedy is often utilized in patients with inflammatory breast most cancers and may confer a survival profit in this population of patients.
4mg coversyl buy with amex
Hematomas result from intermittent or slow symptoms 1dpo coversyl 4mg fast delivery, steady venous bleeding and are almost at all times self-limiting medications elderly should not take coversyl 8mg order with amex. Eventually, the pressure of the increasing hematoma will exceed the venous pressure and a stable clot will kind. The extent of the hematoma is determined partially by the potential size of the compartment into which the bleeding occurs. B, Postembolization left uterine arteriogram shows occluded left uterine artery (long arrows) with no evidence of lively bleeding. By the fifth postoperative day, the hematoma liquefies and could additionally be simpler to outline during bimanual examination. Distinguishing between an uninfected hematoma and a hematoma that has become secondarily infected is tough earlier than incision and drainage. Both scientific conditions produce tenderness and fever secondary to the inflammation surrounding the hematoma. The prognosis of a retroperitoneal hematoma could also be made by bodily examination; most helpful is a cautious rectovaginal examination. If not handled, most massive hematomas will turn into secondarily contaminated, even if handled with parenteral antibiotics. Effective drainage of most pelvic and broad ligament hematomas usually can be completed vaginally or radiographically. The exact incidence of this worrisome complication is tough to set up however is estimated to be from 1 in 1200 to 1500 laparotomies, usually with correct sponge counts at the time of surgery. When this mass is discovered after the quick postoperative course, sufferers are sometimes asymptomatic or exhibit minimal tenderness. The risk of a retained overseas body ought to be thought-about within the differential analysis of pelvic hematomas and abscesses. As such, the surgeon must be conscious of the potential issues of thromboembolism throughout the postoperative course. However, prophylaxis should be continued throughout the hospital stay and, in certain high-risk instances, even after discharge. Without particular pointers, the size of time for thromboprophylaxis must be individualized. Superficial thrombophlebitis is regularly overlooked or disregarded as a reason for postoperative fever. Women with established superficial varicosities within the lower extremities are especially susceptible due to localized stasis or strain through the operative process and inactivity through the first 24 hours after operation. Patients with superficial thrombophlebitis of the legs can also have concomitant deep venous disease. Some series have documented the affiliation of inherited thrombophilias with superficial phlebitis, increasing the danger by 4- to 13-fold, with the stronger thrombophilias contributing to the upper risk. Recurrent superficial phlebitis, in varying anatomic websites, may be a sign of occult malignant disease. The classic symptom of phlebitis is inflammation of the subcutaneous tissue along the course of a vein or over the realm of merging varicosities. However, a Cochrane evaluate in 2013 confirmed no proof to assist routine catheter change with out evidence of irritation, infiltration, or blockage (Webster, 2013). Superficial phlebitis is a standard reason for an enigmatic postoperative fever through the first postoperative week. The medical administration of gentle superficial thrombophlebitis Obstetrics & Gynecology Books Full 25 Perioperative Management of Complications contains relaxation, elevation, and native heat. Deep Vein Thrombosis Fifty p.c of thromboembolic complications occur inside the first 24 hours and 75% occur within seventy two hours. Because women typically die within a couple of hours of the appearance of preliminary signs, emphasis have to be positioned on prevention rather than remedy of this complication. Many girls develop continual venous insufficiency or postphlebitic syndrome of the legs as a serious sequela following thrombophlebitis. The resulting damage to valves of the deep veins produces shunting of blood to superficial veins, chronic edema, ache on exercise, and skin ulceration. The incidence of thrombosis is immediately depending on threat factors corresponding to the kind and length of operation, age of the girl, history of thrombophilia, or deep vein thrombosis, peripheral edema, surgical blood loss, restrictions in preoperative ambulation, obesity, immobility, malignancy, sepsis, diabetes, current oral contraceptive or hormone use, and conditions that produce venous stasis, similar to ascites and coronary heart failure (Box 25. Older and obese women have an elevated incidence of thrombosis because of dilation of their deep venous system. There is a two- to fourfold increased danger for venous thrombosis in women taking postmenopausal estrogen therapy. The length of the surgical procedure additionally has an important affect on the development of thrombosis. If the operation is 1 to 2 hours in period, approximately 15% of women develop the illness; if the surgical procedure is longer than 3 hours, the risk is bigger (Table 25. It is estimated that 75% of pulmonary emboli originate from a thrombus that started within the leg veins. If one leg is concerned, the contralateral leg could have a thrombus in approximately 33% of women. Usually, the thrombus stays localized, it lyses spontaneously, and the local symptoms resolve. In roughly 1 in 20 circumstances the process extends centrally to the veins of the higher leg and pelvis. Involvement of the femoral vein often ends in swelling brought on by obstruction of this huge vein. Pulmonary emboli from calf veins alone are rare, with solely 4% to 10% of pulmonary emboli originating from this area. In 1854, Virchow described the three key predisposing or precipitating components within the manufacturing of thrombi: an increase in coagulation factors, injury to the vessel wall, and venous stasis. Subsequent studies have documented that every one three events happen with gynecologic operations. Kakkar has described the cascade of events resulting in the event of thrombosis. Stasis leads to localized anoxia with subsequent technology of thrombi on the anoxic web site. This produces changes in the lining of the vessel, with exposure of the basement membrane, platelet adhesion, and native coagulation. Thus an important event in thrombosis is the technology of thrombi within the presence of venous stasis. A thrombus might generate in an area of stasis or it may generate wherever a vessel wall is damaged, with resultant publicity of the subendothelial collagen, to which platelets will adhere. The thrombus propagates and grows by repetitive layers of platelet aggregation and deposition of fibrin from fibrinogen. The most recently shaped portion of the propagating thrombi are free-floating (not connected to the vein) and are most probably to turn out to be pulmonary emboli. The body makes an attempt to repair the area of thrombosis via an invasion of fibroblasts from the vein wall to encompass the base of the thrombus. Eventually, the thrombus is hooked up to the vein wall, the realm is reepithelialized, organization happens, and signs resolve.
Cheap coversyl 4 mg otc
Individual areas vary from 1 mm to giant chocolate cysts larger than 8 cm in diameter treatment bipolar disorder order coversyl 4 mg with mastercard. Larger cysts are normally densely adherent to the encompassing pelvic sidewalls or broad ligament medications to treat anxiety 8 mg coversyl generic free shipping. The three cardinal histologic features of endometriosis are ectopic endometrial glands, ectopic endometrial stroma, and hemorrhage into the adjacent tissue. Previous hemorrhage could be found by figuring out large macrophages filled with hemosiderin near the periphery of the lesion. In the majority of circumstances, the aberrant endometrial glands and stroma reply in cyclic trend to estrogen and progesterone. These modifications may or will not be in synchrony with the endometrial lining of the uterus. The ectopic endometrial stroma will endure basic decidual changes much like pregnancy when uncovered to excessive physiologic or pharmacologic levels of progesterone. The chronic pelvic ache normally presents as secondary dysmenorrhea or dyspareunia (or both). Secondary dysmenorrhea often begins 36 to 48 hours previous to the onset of menses. However, roughly one third of patients with endometriosis are asymptomatic, with the illness being discovered by the way during an stomach operation or visualized at laparoscopy for an unrelated drawback. Conversely, endometriosis is found in approximately certainly one of three ladies whose primary symptom is continual pelvic pain. Clinicians have appreciated the paradox that the extent of pelvic pain is usually inversely related to the quantity of endometriosis in the feminine pelvis. Women with large, fixed adnexal lots typically have minor signs, whereas other patients with only a few small foci with deep infiltration may expertise average to severe chronic pain. The cyclic pelvic ache is related to the sequential swelling and the extravasation of blood and menstrual particles into the surrounding tissue. The chemical mediators of this intense sterile irritation and ache are believed to be prostaglandins and cytokines. Infiltrative endometriosis, which entails intensive areas of the retroperitoneal area, often is related to average to severe pelvic pain. Studies of ache mapping by laparoscopy under minimal sedation have discovered that pelvic pain arises from areas of regular peritoneum adjacent to areas of endometriosis. Secondary dysmenorrhea is a typical element of pain that varies from a dull ache to severe pelvic pain. It could additionally be unilateral or bilateral and should radiate to the decrease back, legs, and groin. Patients often complain of pelvic heaviness or a notion of their internal organs being swollen. Unlike major dysmenorrhea, the pain might final for many days, including several days before and after the menstrual move. The dyspareunia related to endometriosis is described as ache deep within the pelvis. The explanation for this symptom appears to be immobility of the pelvic organs throughout coital activity or direct strain on areas of endometriosis within the uterosacral ligaments or the cul-de-sac. The acute pain, experienced during deep penetration, might proceed for several hours following intercourse. On the opposite hand, patients with endometriosis regularly have ovulatory dysfunction. Approximately 15% of girls with endometriosis have coincidental anovulation or luteal dysfunction. An elevated incidence of first-trimester abortion in girls with untreated endometriosis has been reported, although this notion has been challenged and stays an unproven affiliation. Less frequent, yet troublesome, are the signs ensuing from endometriosis influencing the gastrointestinal and urinary tracts. Cyclic belly ache, intermittent constipation, diarrhea, dyschezia, urinary frequency, dysuria, and hematuria are all potential symptoms. One rare clinical manifestation of endometriosis is catamenial hemothorax, bloody pleural fluid occurring throughout menses. In these cases, a presumptive prognosis of endometriosis is made by visualizing the extraordinary inflammatory response and the large macrophages filled with blood pigment. The pathophysiology of development from subtle endometriosis to extreme disease may be anticipated from the multiple mechanisms of potential illness acceleration mentioned earlier, with immune function more than likely involved. Clinical Findings (Physical Exam) the classic pelvic discovering of endometriosis is a set retroverted uterus, with scarring and tenderness posterior to the uterus. The attribute nodularity of the uterosacral ligaments and culde-sac may be palpated on rectovaginal examination in women with this distribution of the disease. Advanced instances have extensive scarring and narrowing of the posterior vaginal fornix. The ovaries could also be enlarged and tender and are often fastened to the broad ligament or lateral pelvic sidewall. Speculum examination might reveal small areas of endometriosis on the cervix or upper vagina. Lateral displacement or deviation of the cervix is visualized or palpated by digital examination of the vagina and cervix in approximately 15% of women with moderate or severe endometriosis. The prognosis may be confirmed in most cases by direct laparoscopic visualization of endometriosis with its related scarring and adhesion formation. In many patients, endometriosis was found for the first time during an infertility investigation, though routine laparoscopy is no longer being carried out within the infertility investigation. There is a attribute hyperintensity on T1-weighted pictures and a hypointensity on T2-weighted images (de Venecia, 2015). When laparoscopy is undertaken to set up the analysis of endometriosis, you will want to describe systematically the extent of the pathology. The focus right here was supposed to present characterization of illness extent for fertility and not for ache assessment. Although a benign illness, endometriosis reveals characteristics of both malignancy and sterile irritation. Therefore, the frequent considerations within the differential analysis include continual pelvic inflammatory disease, ovarian malignancy, degeneration of myomas, hemorrhage or torsion of ovarian cysts, adenomyosis, main dysmenorrhea, and practical bowel illness. Occasionally a large endometrioma of the ovary might rupture into the peritoneal cavity. This ends in an acute surgical stomach and brings into the differential prognosis circumstances similar to ectopic being pregnant, appendicitis, diverticulitis, and a bleeding corpus luteum cyst. Ultrasound examination reveals no particular sample to screen for pelvic endometriosis however may be helpful in differentiating solid from cystic lesions and should help distinguish an endometrioma from different adnexal abnormalities. Because the lesions are vascular, elevated Doppler flow could additionally be demonstrated in endometriosis.
Coversyl 4mg buy low cost
In addition symptoms 5 days before missed period 4mg coversyl with amex, performance of robotic radical trachelectomy continues to rise and we anticipate will further advance use of the abdominal approach symptoms knee sprain 4 mg coversyl visa. This is essential, as a end result of these adhesions play a role in the severity of bowel issues if postoperative radiotherapy is given. Minimally invasive surgical procedure is related to shorter size of keep, much less ache, few postoperative infections, fewer thromboembolic problems, and reduced blood loss compared with belly procedures. For gynecologic oncologists in practice, the lengthy studying curve associated with laparoscopy has been an impediment to advancement. The most recent minimally invasive technique, robotic laparoscopic surgery, offers new advantages. The robotic extra closely replicates the wristed motions that surgeons use during open circumstances, presents three-dimensional imaging, and utterly eliminates the tremor of the surgeon and the assistant holding the camera. Sentinel Node Biopsy Cervical most cancers, like most strong tumors, spreads primarily by lymphatic spread. Surgical administration of solid tumors, as pioneered greater than a hundred years in the past by Halsted, is predicated on the resection of all regional lymph nodes and lymphatic channels connecting the lymph nodes to the first tumor. Implicit in this approach is that each one regional lymph nodes have the same danger of containing metastatic disease. Morton, working in patients with cutaneous melanoma, has demonstrated that there are sentinel lymph nodes which would possibly be the first nodes to obtain lymphatic drainage from the first tumor and are therefore the first website of metastases (Morton, 2001). Cervical cancer is a wonderful target for the sentinel lymph node idea because the tumor is simple to inject and the regional lymph nodes may be reached via an incision. Lymphatic drainage of the cervix is complex; nevertheless, most sentinel lymph nodes of the cervix are discovered along the external iliac artery or vein, obturator house, or parametrium. A number of investigators have reported their experience with sentinel lymph node biopsy in radical hysterectomy patients. So far, the procedure has shown great promise; nevertheless, the false-negative charges have been larger for cervical most cancers patients than for these with, for instance, vulvar most cancers. It is most likely going that sentinel lymph node biopsy will finally be included into the surgical administration of cervical cancer. Surgical Complications Minimally invasive techniques for therapy of cervical cancer are engaging for several reasons. Lymph nodes can be removed safely via laparoscopic ports, especially if removed in a protective bag prior Following radical hysterectomy, many patients experience longterm problems. Montz and associates noted a 5% frequency of small bowel obstruction, which increases to 20% if radiation is used postoperatively (Montz, 1994). The low rate seems to result from the administration of antibiotics, prevention of retroperitoneal serosanguineous collections, and avoidance of direct manipulation of the ureter to keep away from injury to the periureteral blood supply. In part, this appears to be caused by disruption of the sympathetic nerve provide to the bladder. Low and associates famous a rise in bladder pressure with a lower in urethral stress following radical hysterectomy (Low, 1981). The bladder can develop hypotonicity, and overdistention can then become an issue. If overdistention of the bladder and an infection are averted, progressive improvement of bladder perform normally happens. Forney correlated the degree of bladder dysfunction after radical hysterectomy with the extent of resection of the cardinal ligament (Forney, 1980). Those who had a complete resection of cardinal ligaments may void satisfactorily at an average of 51 days compared with 20 days for these with solely partial resection of the ligaments. Newer nerve-sparing surgical strategies the place the uterosacral ligament is transected after separation of the hypogastric nerve and preservation of the bladder branches of the pelvic plexus have been related to improved bladder function with out compromising oncologic outcomes and survival. In a 1999 study from Sweden, Bergmark and coworkers noted compromised sexual activity, decreased lubrication, and shortened vagina in women treated for cervical cancer by surgical procedure or radiation (Bergmark, 1999). During the consent process, patients must be informed concerning the potential influence of radical hysterectomy on their sexual function. Lymphedema is another complication of radical pelvic surgical procedure that may affect quality of life. Lymphedema massage could assist cut back this downside, however treatment choices are restricted and of only modest effectiveness. Patients with constructive or shut margins or constructive lymph nodes have the very best risk of recurrence and poor outcome. A randomized study has shown that postoperative chemoradiation improves survival in sufferers with positive lymph nodes and optimistic surgical margins (Peters, 1999). Radiation Treatment Most sufferers with carcinoma of the cervix are treated by radiation. The principles of external megavoltage therapy (teletherapy) and native implants (brachytherapy) are reviewed in Chapter 26. External beam radiation is administered in fractions, normally 180 cGy/day, 5 days/week, to destroy the tumor with out causing everlasting harm to normal tissues. This delivers uniform doses to the complete pelvis, including the regional pelvic nodes. The native implant delivers its highest energy domestically to the cervix, surface of the vagina, and paravaginal and paracervical tissues. The uterus and cervix serve as a receptacle for arranging and holding the intracavitary applicator stem (tandem) and accompanying vaginal applicators (ovoids) in a fixed and optimal place for delivering the desired radiation dosimetry. Usually, the tandem and ovoids or a tandem and ring are inserted with within the woman, and a pack is placed into the vagina to stabilize the apparatus and enhance the space from the mucosa of the bladder and rectum. After the place of the applicator has been confirmed to be satisfactory by imaging, the radioactive supply, similar to cesium-137 or Iridium 192, is inserted (afterloading technique). Other types of applicators are available, but the precept of delivering intense radiation to the cervix and paracervical areas is identical. The aim is to enhance the total dose of radiation to the maximum allowable to obtain tumor management without introducing a major risk of problems and harm to adjacent normal tissue. In common, external remedy is given first to deal with the regional pelvic nodes and shrink the central tumor mass, which then is extra amenable for a neighborhood implant. In some sufferers, external therapy can result in excessive shrinkage of the vaginal apex, making secure, efficient implantation of native radiation sources difficult. Occasionally, in those sufferers, the implantation is finished first, particularly for smaller stage I tumors. Intraoperative ultrasounds could additionally be helpful particularly in tough cases for optimum implant positioning. In some cases, the central pelvis is shielded during external radiation therapy to permit for subsequent larger doses from the implant. Occasionally, interstitial remedy within the form of needles implanted into the world of the tumor is required to achieve efficient local tumor control. Intracavitary radiation remedy could also be delivered at either a low-dose rate or a high-dose rate. High-dose-rate brachytherapy and low-dose-rate brachytherapy have related survival and toxicity and high-dose-rate brachytherapy has turn into the commonest type of brachytherapy out there throughout the world. The number of fractions varies from two to five; the most typical one within the United States is 5. Point B is 5 cm lateral to the cervical canal and three cm lateral to level A, which locations Obstetrics & Gynecology Books Full 29 Malignant Diseases of the Cervix but an increase in toxicity (Keys, 1999).
Creosote Bush (Chaparral). Coversyl.
- Arthritis, cancer, sexually transmitted diseases, tuberculosis, colds, skin conditions, stomach ailments (cramps, gas), weight loss, urinary and respiratory infections, and chicken pox.
- Are there any interactions with medications?
- How does Chaparral work?
- What is Chaparral?
- Dosing considerations for Chaparral.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96770
Coversyl 8 mg quality
Racial and ethnic disparities in benign gynecologic circumstances and associated surgeries medications that cause tinnitus cheap 4 mg coversyl mastercard. Decreased levels of the potent regulator of monocyte/macrophage activation medicine wheel teachings coversyl 8mg overnight delivery, interleukin-13, in the peritoneal fluid of sufferers with endometriosis. Zur Frage der heterotopen Epithelwucherung, insbe Suggested Readings can be discovered on ExpertConsult. Treatment of endometriosis with a long-acting gonadotropin-releasing hormone agonist plus medroxyprogesterone acetate. Increased expression of cyclooxygenase-2 in local lesions of endometriosis sufferers. Sexual activity, contraception, and reproductive elements in predicting endometriosis. Cortical and trabecular bone mineral content in women with endometriosis: impact of gonadotropin-releasing hormone agonist and danazol. Clinical, endocrine, and metabolic effects of two doses of gestrinone in remedy of pelvic endometriosis. Depot leuprolide acetate versus danazol for remedy of pelvic endometriosis: adjustments in vertebral bone mass and serum estradiol and calcitonin. A randomized, managed trial of clomiphene citrate and intrauterine insemination in couples with unexplained infertility or surgically corrected endometriosis. Serial laparoscopies over 30 months present that endometriosis in captive baboons (Papio anubis, Papio cynocephalus) is a progressive disease. Role of K-ras and Pten within the improvement of mouse models of endometriosis and endometrioid ovarian cancer. Lupron depot (leuprolide acetate for depot suspension) within the remedy of endometriosis: a randomized, placebo-controlled, double-blind research. Superovulation with human menopausal gonadotropins within the remedy of infertility associated with minimal or mild endometriosis: a managed randomized examine. Treatment of adenomyosis-associated menorrhagia with a levonorgestrel-releasing intrauterine gadget. Endometrial patterns during danazol and buserelin therapy for endometriosis: comparative structural and ultrastructural research. Gonadotropin-releasing hormone agonist plus estrogen-progestin "add-back" therapy for endometriosis-related pelvic pain. Gestrinone Italian Study Group: Gestrinone versus a gonadotropin-releasing hormone agonist for the remedy of pelvic pain associated with endometriosis: a multicenter, randomized, double-blind study. Massive uterine enlargement with necrosis: an unusual manifestation of adenomyosis. Peritoneal macrophages from patients with endometriosis release development issue exercise in vitro. Adenocarcinoma arising in extragonadal endometriosis: an immunohistochemical study. Soluble vascular endothelial growth factor receptor 1 inhibits edema and epithelial proliferation induced by 17 beta-estradiol in the mouse uterus. Results of laparoscopic therapies of ovarian endometriomas: laparoscopic ovarian fenestration and coagulation. Administration of nasal nafarelin as in contrast with oral danazol for endometriosis: a multicenter double-blind comparative medical trial. Pregnancy after medical therapy of adenomyosis with a gonadotropin-releasing hormone agonist. A randomized double-blind potential trial of two doses of gestrinone in the therapy of endometriosis. Use of nafarelin versus placebo after reductive laparoscopic surgery for endometriosis. Leuprolide acetate depot and hormonal add-back in endometriosis: a 12-month study. Nuclear peroxisome proliferatoractivated receptors alpha and gamma have opposing results on monocyte chemotaxis in endometriosis. Peritoneal endometriosis: endometrial tissue implantation as its primary etiologic mechanism. Pathogenesis of endometriosis based mostly on endometrial homeoplasia, direct extension exfoliation and implantation, lymphatic and hematogenous metastasis. Allelotyping of endometriosis with adjacent ovarian carcinoma reveals evidence of a common lineage. Production of fibronectin by peritoneal macrophages and concentrations of fibronectin in peritoneal fluid from patients with or with out endometriosis. Detection of aromatase cytochrome P-450 in endometrial biopsy specimens as a diagnostic test for endometriosis. N-terminal truncated forms of insulin-like progress issue binding protein-3 in the peritoneal fluid of women without laparoscopic evidence of endometriosis. Mucosal modifications in the large bowel with endometriosis: a possible cause of misdiagnosis of colitis. Pelvic Pain Study Group: randomized managed trial of depot leuprolide in sufferers with chronic pelvic pain and clinically suspected endometriosis. Long-term consequence of nonconservative surgery (hysterectomy) for endometriosis-associated pain in girls <30 years old. Vascular endothelial progress issue and interleukin-6 in peritoneal fluid of girls with endometriosis. Relation of endometriosis and the neuromuscular illness of the gastrointestinal tract: new insights. Historical prospective cohort research of the recurrence of pain after discontinuation of treatment with danazol or a gonadotropin-releasing hormone agonist. Treatment of endometriosis with estrogen-progestin mixture and progestogens alone. Goserelin acetate (Zoladex) with or with out hormone substitute therapy for the therapy of endometriosis. Nafarelin for endometriosis: a large-scale, danazol-controlled trial of efficacy and security, with 1-year followup. Long-term administration of adenomyosis with a gonadotropin-releasing hormone agonist: a case report. Peritoneal endometriosis, ovarian endometriosis, and adenomyotic nodules of the rectovaginal septum are three completely different entities. Smooth muscle metaplasia and innervations in interstitium of endometriotic lesions related to pain. Transforming growth factor-activity is increased in peritoneal fluid from girls with endometriosis. Postsurgical medical remedy of superior endometriosis: outcomes of a randomized medical trial. Malignancy arising in endometriosis associated with unopposed estrogen replacement. Zoladex Endometriosis Study Group: Zoladex (goserelin acetate implant) within the treatment of endometriosis: a randomized comparison with danazol.
Coversyl 8mg for sale
Shepherd and coworkers noted that sufferers older than sixty nine years medicine 018 generic 4mg coversyl visa, those who had a recurrence inside 3 years symptoms 4dpo effective 4 mg coversyl, or those who had persistent disease or constructive resection margins had a poorer prognosis for the procedure (Shepherd, 1994). This process requires multidisciplinary superior surgical support and carries high danger of surgical morbidity, but it might be contemplated as a possible healing possibility for very select sufferers. Before an exenterative operation is undertaken, the affected person is completely evaluated for any proof of disease spread outside the pelvis. At operation, abdominal exploration is carried out to make positive that the tumor is resectable. Biopsy specimens of any enlarged lymph nodes or suspicious areas outside the pelvis are taken, and frozen-section studies are performed, including analysis of the operative margins. The introduction of continent urinary diversion supplies another incontinent urinary conduit. Generally, the urinary stoma is situated in the abdomen on the proper side and the intestinal stoma on the left facet. The use of intestinal 681 stapling devices generally permits preservation of the rectal sphincter and anal function and avoids a permanent colostomy. Long-term problems are normally ureteral stricture or issue catheterizing the intestinal reservoir. Continent conduits require the woman to catheterize the pouch each 4 hours, however no external equipment is required. Severe postoperative and intraoperative issues can happen with this extensive procedure and perioperative mortalities as excessive as 10% to 20% have been reported prior to now. However, current surgical methods of preoperative bowel preparation, use of antibiotics, careful intraoperative fluid and volume monitoring, and use of parenteral vitamin have reduced the instant postoperative mortality to less than 5%. The use of a peritoneal graft or an omental flap, created from the right or left side of the omentum and positioned within the pelvis to protect the denuded pelvic ground, might help avoid bowel obstruction and cut back postoperative morbidity. Occasionally, gracilis myocutaneous grafts are used to create a new vagina and convey a new blood supply to the previously irradiated pelvis, which aids in wound therapeutic. Morley and associates reported on a 5-year survival fee of 61% in one hundred patients aged 21 to seventy four years (Morley, 1989). Localized recurrences in areas not previously irradiated are sometimes handled by radiation. In this trial, patients were randomized to single-agent cisplatin versus cisplatin and topotecan. There has been a major step ahead in the therapy of sufferers with recurrent or metastatic cervix with the addition of focused therapy. There was no distinction in outcomes between the 2 chemotherapy regimens; nevertheless, the addition of bevacizumab considerably improved general survival (17 months vs. In addition to more robust prevention and screening methods, better therapeutic methods must be explored, including determining prognostic components, the administration of novel brokers which will enhance the therapeutic index of definitive chemoradiation, and various immunotherapeutic approaches. In the United States, squamous cell carcinoma is extra frequent in blacks than in whites. Definitive prognosis of microinvasive carcinoma is established solely by the use of cervical conization, not biopsy. The margins of the cone ought to be freed from neoplastic epithelium before conservative therapy is undertaken. Microinvasive carcinoma of the cervix could be effectively treated by total hysterectomy, with a 5-year survival fee of virtually 100 percent, but recurrent neoplasia can develop after 5 years. Cervical carcinomas are domestically invasive tumors that spread primarily to the pelvic tissues after which to the pelvic and paraaortic lymph nodes. Improved total survival charges have been reported for sufferers with tumors smaller than 4 cm in diameter treated by preliminary brachytherapy adopted by radical hysterectomy. Surgery produces less scarring and vaginal fibrosis than radiation and is most well-liked for ladies with a pelvic mass, pelvic an infection, or historical past of circumstances similar to inflammatory bowel disease, which improve the risk for radiation problems. Current applications normally use cisplatin, 40 mg/m2 weekly, during exterior remedy and with brachytherapy. Most cancers of the cervix are treated by radiation remedy (teletherapy and brachytherapy). Radiation doses range with tumor dimension and stage however are approximately 50 to 65 Gy at point B and 80 to 85 Gy at point A. Current follow is to combine radiation with simultaneous chemotherapy to optimize the outcomes. Improved remedy rates of cervical cancers are obtained with increased doses, which also lead to an elevated frequency of problems. Complications following radiation are related to dose and quantity of tissue treated; these embody radiation irritation of the bladder or bowel, which can result in ache, bleeding, or, sometimes, fistula formation. Approximately one third of patients treated for cervical carcinoma develop tumor recurrence, and roughly 50% of those recurrences are situated within the pelvis; most happen within 2 years. Patients whose recurrences occur more than three years after primary therapy have a greater prognosis than those with earlier recurrence. Pelvic exenteration in fastidiously chosen sufferers with central pelvic recurrence can result in a 5-year survival rate of 50% or better. Reducing uncertainties concerning the results of chemoradiotherapy for cervical cancer: a systematic evaluation and meta-analysis of individual affected person information from 18 randomized trials. Radical hysterectomy after radiotherapy for recurrent carcinoma of the uterine cervix. Total pelvic exenteration: the Albert Einstein College of Medicine/Montelior Medical Experience (1987 to 2003). Total mesometrial resection: high resolution nerve-sparing radical hysterectomy based on developmentally outlined surgical anatomy. Concurrent mitomycin C, 5-fluorouracil, and radiotherapy within the therapy of locally advanced carcinoma of the cervix: a randomized trial. Ureteral stricture as a late complication of radiotherapy for stage Ib carcinoma of the uterine cervix. Small bowel obstruction following radical hysterectomy: threat elements, incidence, and operative findings. Lymphatic mapping and sentinel lymphadenectomy for melanoma: previous, current and future. Randomized trial of cisplatin versus cisplatin plus mitolactol versus cisplatin plus ifosfamide in superior squamous carcinoma of the cervix: a Gynecologic Oncology Group study. Cisplatin, 5-fluorouracil plus radiation remedy are superior to radiation therapy as adjunctive therapy in high-risk, early-stage carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy. Radical vaginal trachelectomy: a fertility-preserving option for younger girls with early stage cervical most cancers. Early invasive cervical cancer with pelvic lymph node involvement: to complete or not to complete radical hysterectomy Laparoscopic extraperitoneal para-aortic lymphadenectomy in locally advanced cervical most cancers: a potential correlation of surgical findings with positron emission tomography/computed tomography findings. Psychoeducational group increases vaginal dilation for younger women and reduces sexual fears for girls of all ages with gynecologic carcinoma handled with radiotherapy. A fertility-sparing different to radical hysterectomy: what quantity of patients may be eligible Novel modification of the vertical rectus abdominis myocutaneous flap for neovagina creation.
8 mg coversyl order visa
Effect of hormone substitute therapy on cardiovascular occasions in lately postmenopausal women: randomised trial medications quit smoking 8mg coversyl purchase visa. Release of 17-beta-oestradiol from a vaginal ring in postmenopausal ladies: pharmacokinetic analysis medications while breastfeeding coversyl 8mg buy generic online. The affect of exogenous estrogen use on survival after diagnosis of endometrial cancer. A potential analysis of clomiphene citrate problem test screening of the final infertility population. Effect of estrogen on brain activation patterns in postmenopausal ladies during working memory task. Affective adjustments with estrogen and androgen alternative therapy in surgically menopausal girls. The impact of different doses of estrogen and progestin on temper and sexual conduct in postmenopausal ladies. Hormone remedy and in-hospital survival after myocardial infarction in postmenopausal women. Effects of childhood leukemia and chemotherapy on puberty and reproductive perform in ladies. Hormone alternative therapy formulations and danger of epithelial ovarian carcinoma. Low molecular weight follicle-stimulating hormone receptor binding inhibitor in sera from premature ovarian failure patients. Changes in physique composition in women over six years at midlife: ovarian and chronological aging. Anti-mullerian hormone and inhibin within the definition of ovarian growing older and the menopause transition. Oestrogen therapy and subsequent pregnancy in two sufferers with extreme hypergonadotropic ovarian failure. Reproductive and gonadal perform within the female after therapy for childhood malignancy. A multifactorial intervention to cut back the risk of falling among elderly individuals residing in the community. Estrogen receptors colocalize with low-affinity nerve progress factor receptors in cholinergic neurons of the basal forebrain. Effects of gender and age on the levels and circadian rhythmicity of plasma cortisol. Age at pure menopause in a population-based screening cohort: the role of menarche, fecundity, and lifestyle factors. Twenty-four hour rhythms in plasma concentrations of adenohypophyseal hormones are generated by distinct amplitude and/or frequency modulation of underlying pituitary secretory bursts. The aging musculoskeletal system and obesity-related concerns with train. Anti-Mullerian hormone: an ovarian reserve marker in primary ovarian insufficiency. Treatment with oral piperalzine oestrone sulphate for genuine stress incontinence in postmenopausal women. Intrauterine administration of levonorgestrel 5 and 10 mg/24 h in perimenopausal hormone replacement therapy: a randomized medical trial throughout one year. Incidence of endometrial hyperplasia in postmenopausal women taking conjugated estrogens (Premarin) with medroxyprogesterone acetate or conjugated estrogens alone. Estrogen remedy in post-menopausal ladies: results on cognitive perform and dementia. Twenty-four hour imply plasma testosterone concentration declines with age in normal premenopausal women. Obstetrics & Gynecology Books Full 15 Breast Diseases Detection, Management, and Surveillance of Breast Disease Samith Sandadi, David T. Regardless, the position of the gynecologist in the management of breast illness has been addressed in a variety of published scientific opinions and apply bulletins from the American College of Obstetrics and Gynecology. A change or abnormality incessantly ignites a fear of breast most cancers and strong psychological issues. The objective of this chapter is to current a clinically oriented approach that allows the practitioner to better understand breast anatomy, the necessary diagnostic and scientific elements of benign breast illness, and the epidemiology, detection, and management of breast most cancers. Ducts and acini are derived from ectoderm, whereas supporting tissue arises from mesenchyme. Ductal tissue and secretory lobule improvement occurs underneath the affect of the hormonal adjustments that occur during puberty (see Chapter 38). Actual milk production is initiated by hormonal modifications that happen during and after being pregnant. The breasts are large, modified apocrine/sweat glands positioned in the superficial fascia anterior to the deep pectoralis major fascia of the chest wall. Posteriorly, the retro mammary space, a loose connective tissue aircraft, allows free motion over the chest wall. The breast tissue is suspended from the clavicle and deep clavipectoral fascia by the suspensory ligaments of Cooper that weave by way of the breast tissue and fasten to the dermis of the skin. Clinically, malignant involvement of these ligaments often produces pores and skin retraction, suggesting the presence of advanced breast carcinoma. Breast size and form depend on genetic, racial, and dietary factors in addition to age, parity, and menopausal status. On average, through the reproductive ages the grownup breast weighs approximately 250 grams. Typically, a superolateral projection Guidelines have questioned the profit of breast self-examination, although many ladies determine their own breast most cancers. Glandular tissue composes approximately 20% of the mature breast with the remainder being adipose and connective tissue. Breast density refers to the proportion of fibrous/glandular tissue to adipose tissue. The periphery of the breast is predominantly adipose, and the central space accommodates a higher proportion of glandular tissue. Typically, glandular tissue regresses and is changed by adipose tissue after menopause. A breast consists of 12 to 20 varying-sized, triangularshaped lobes distributed radially from the nipple. Each lobe incorporates its own duct system draining the ten to a hundred lobules with alveoli (acini). Secretory cells drain into alveoli, which drain into "terminal" ducts that then coalesce into larger accumulating ducts, and join with ducts from other lobules to finish in lactiferous ducts, terminating at the excretory ducts of the nipple. The principal blood supply of the breast is derived from the perforating branches of the interior mammary arteries that originate from the internal thoracic artery.
Coversyl 8 mg cheap
For larger lesions medicine 524 buy 8mg coversyl visa, the dose of the exterior element of radiation remedy is elevated medications safe while breastfeeding coversyl 4 mg, with a concomitant discount in the local vaginal part of remedy of the first tumor. Usually, a total tumor dosage of roughly 7500 cGy Obstetrics & Gynecology Books Full 31 Malignant Diseases of the Vagina Table 31. Clear cell adenocarcinoma of the vagina and cervix secondary to intrauterine exposure to diethylstilbestrol. Kucera and Vavra, in a collection of 434 sufferers handled with irradiation, noted that outcomes have been best for low-stage tumors, these in the upper third of the vagina, and when the tumor was well-differentiated (Kucera, 1991). Kirkbride and colleagues have reported that stage, tumor measurement, and tumor grade are prognostic and that the tumor dose must attain at least 7000 cGy, in keeping with other studies (Kirkbride, 1995). Survival Overall 5-year survival charges for patients with primary carcinoma of the vagina have been reported to be approximately 45%. The use of concomitant chemotherapy with radiation can be anticipated to produce improved survival charges (Creasman, 1998). Therapeutic issues are similar to these for squamous cell carcinoma, taking into account the younger age of the patients present process remedy. Cervical clear cell adenocarcinomas are handled in the same manner as main cervical carcinomas. The outcomes of therapy for vaginal and cervical clear cell adenocarcinoma in younger ladies are discussed together on this section. The general results of remedy, primarily based on the stage of the tumor on the time of treatment, are shown in Table 31. The survival rate is related directly to the stage of the tumor, much like other gynecologic malignancies at these websites. In basic, surgery is the first treatment modality due to the young age of the patients. Because metastases to regional pelvic nodes can happen, even with small stage I tumors, retroperitoneal lymph node dissections are often performed before local therapy. Local excision of the tumor may be performed before irradiation to facilitate native utility. Senekjian and associates have famous that the survival of patients with small vaginal tumors treated by local excision after which native irradiation is comparable with that obtained with conventional in depth remedy (Senekjian, 1989). The best candidates are those with tumors smaller than 2 cm in diameter, a predominant tubulocystic pattern. Patients with larger tumors, nonetheless, receive full pelvic irradiation, in addition to an intracavitary implant. This process is preferably utilized to central recurrences that develop after main irradiation. Three predominant histologic patterns are present in patients with clear cell adenocarcinoma. Note hobnail cells extruding into the lumina of tubular buildings (H&E stain, � 180). Vaginal and cervical abnormalities, including clear cell adenocarcinoma, associated to prenatal publicity to stilbestrol. Pathology and pathogenesis of diethylstilbestrol-related problems of the female genital tract. This distinction is related to a extra favorable outcome for these with the tubulocystic pattern of clear cell adenocarcinoma, the most frequent histologic pattern found in older patients. In addition, smaller tumor diameter and superficial depth of invasion correlate with improved affected person survival. If the regional pelvic nodes are free of tumor, the prognosis can be extra favorable. It is extra likely that the regional pelvic lymph nodes shall be free of tumor if different factors are favorable. Clear cell adenocarcinomas can unfold domestically, in addition to through lymphatics and blood vessels. Metastases to regional pelvic nodes are present in approximately one sixth of stage I cases. Depending on the location of the tumor recurrence, remedy has consisted of extra radical surgical procedure or intensive radiation in localized pelvic illness and systemic chemotherapy Obstetrics & Gynecology Books Full 31 Malignant Diseases of the Vagina in cases of metastatic disease. Unfortunately, no single agent or combination of chemotherapeutic brokers has emerged as an effective therapy. Prolonged follow-up is important for these patients as a end result of recurrences have been reported as long as 20 years after primary therapy, particularly within the lungs and supraclavicular areas. The most common presenting signs are vaginal discharge, bleeding, and a palpable mass. These lesions seem as darkly pigmented, irregular areas and may be flat, polypoid, or nodular. Vaginal melanomas tend to metastasize early, by way of the bloodstream and lymphatics, to the iliac or inguinal nodes, lungs, liver, brain, and bones. Patients with vaginal melanoma have a poorer prognosis than these with vulvar melanoma, partially in all probability because of delay in analysis as compared with vulvar carcinomas and partially because of their mucosal location, which appears to predispose sufferers to developing early metastasis (Kirschner, 2013). Treatment often consists of surgical procedure with extensive excision of the vagina and dissection of the regional nodes (pelvic, inguinal-femoral, or both), relying on the location of the lesion. Improved outcomes have been related to the elimination of all gross disease (Buchanan, 1998). Surgery, radiation, chemotherapy, and immunotherapy have all been described, but no single therapy or combination therapy is uniformly profitable. Prognostic indicators include tumor measurement, mitotic index, and Breslow tumor thickness. However, Neven and coworkers have famous that among nine patients, all those with melanomas greater than 2 mm thick died or had a recurrence no matter kind of therapy, emphasizing the significance of tumor thickness in melanoma prognosis (Neven, 1994). When these tumors happen in the vagina or rectovaginal septum, the everyday scientific presentation is pain, vaginal bleeding, or the presence of a vaginal mass in a lady who has beforehand undergone prior extirpative surgical procedure for endometriosis. The most typical histology is endometrioid adenocarcinoma, adopted by sarcomas (25%) and other tumors of m�llerian differentiation. Leiserowitz and colleagues have reported a comparatively favorable prognosis for girls with endometriosis-related malignancies, with 70% alive at a mean follow-up of 31 months (2003). This tumor secretes -fetoprotein, which provides a helpful tumor marker to monitor patients handled for these neoplasms. Approximately sixty nine cases of this uncommon malignancy originated within the vagina of infants, predominantly those younger than 2 years of age. Copeland and colleagues have reported related good results with mixture chemotherapy and excision (Copeland, 1985). Rarely does it happen in a young baby older than eight years, although cases in adolescents have been reported. The most typical symptom is abnormal vaginal bleeding, with an occasional mass present at the introitus.
Trusted 8 mg coversyl
Overall medicine 2 times a day buy discount coversyl 8mg online, advanced atypical hyperplasias had the best danger of progression to carcinoma medicine wheel teachings coversyl 4 mg purchase. Simple hyperplasia had a 1% fee of development to most cancers, advanced hyperplasia without atypia had a 3% rate of progression to cancer, and complex atypical hyperplasia had a 29% rate of progression to most cancers. In addition to potential progression to cancer, 40% of ladies who endure hysterectomy for complicated atypical hyperplasia have a concurrent endometrial cancer of their hysterectomy specimen. This excessive rate of most cancers suggests that advanced atypical hyperplasia might regularly be current with low-grade endometrial most cancers and that endometrial sampling might not identify an endometrial cancer when admixed with a posh atypical hyperplasia. In younger sufferers, hyperplasia may develop during anovulatory cycles and will even be detected after prolonged intervals of oligomenorrhea or amenorrhea. It can happen at any time through the reproductive years but is most common with irregular bleeding in the perimenopausal period. Premenopausal women with irregular vaginal bleeding and postmenopausal women with any vaginal bleeding ought to be evaluated with an office endometrial sampling or a D&C. The workplace sampling instruments, corresponding to a thin plastic Pipelle, are launched via the cervical os into the endometrial cavity and can present very correct information (see Chapter 10). Many patients tolerate workplace endometrial sampling with out an analgesic agent, but paracervical block can be an effective anesthetic help, notably in nulliparous girls. Some sufferers profit from an oral nonsteroidal antiinflammatory drug taken approximately half-hour earlier than biopsy. Transvaginal ultrasonography has been evaluated as an adjunct for the prognosis of endometrial hyperplasia and most cancers. These research have been carried out in several populations, together with asymptomatic postmenopausal ladies, girls taking tamoxifen, and girls presenting with postmenopausal bleeding. Langer and associates, in a study of 448 asymptomatic postmenopausal women, found a threshold of 5-mm endometrial thickness had only a 9% predictive value for detecting endometrial abnormalities (Langer, 1997). Its higher use was eliminating the analysis of neoplasia for those with thickness less than 5 mm (negative predictive value of 99%). These findings have been confirmed in a literature review by Smith-Bindman and colleagues, who found that 96% of women with carcinoma had an irregular ultrasound scan (endometrial thickness >5 mm). Conversely, 8% of postmenopausal women with an irregular scan had no histologic abnormality, and the percentage grew to 23% for those on hormone replacement therapy. However, both of those research have been conducted in postmenopausal asymptomatic girls. One case of hyperplasia and considered one of carcinoma have been discovered, and most sufferers had atrophic endometrium. The authors concluded that the false-positive price of transvaginal ultrasonography on this inhabitants was too high to warrant its use as a screening modality, they usually recommended using irregular vaginal bleeding as a sign for endometrial sampling (Cecchini, 1996). In the study by Barakat and colleagues, routine screening with transvaginal ultrasonography was not of value, and they concluded that sampling should be carried out if the affected person experiences bleeding. In postmenopausal girls with any vaginal bleeding, Gull and colleagues discovered that an endometrial stripe of lower than 4 mm had a 100 percent adverse predictive value (Gull, 2000). A finding of endometrial thickness less than four mm is a reasonable predictor of lack of endometrial pathology, even in a postmenopausal patient with bleeding. However, persistent vaginal bleeding should result in endometrial sampling regardless of the ultrasound findings. Endometrial ablation is typically undertaken to management severe uterine bleeding (see Chapter 26). However, pathologic evaluation of the endometrium must be carried out before ablation in order to rule out an underlying endometrial hyperplasia or cancer. For girls with easy hyperplasia or advanced hyperplasia without atypia, the danger of creating endometrial cancer is low, 1% and 3%, respectively. A diagnostic D&C can be therapeutic, and progestins or mixture oral contraceptive brokers will doubtless be effective. For complex atypical hyperplasia, the risk of developing endometrial most cancers could also be 29%, and, as stated beforehand, a concurrent endometrial cancer may be current. Women who need preservation of childbearing function are handled with high-dose progestin therapy, usually megestrol acetate forty mg three times every day to 4 occasions day by day. The patient ought to have long-term follow-up and periodic sampling, the first at three months and a minimal of every 6 months thereafter. In these patients, the chance components that led to the development of complex atypical hyperplasia are more probably to stay. Therefore as soon as the complicated atypical hyperplasia is cleared, consideration should be given to periodic progestin treatment or oral contraception until the affected person chooses to attempt pregnancy. For older sufferers with advanced atypical hyperplasia, the risk of carcinoma may be elevated. Kurman and associates studied the uteri of sufferers after curettage had been performed, and atypical hyperplasia was found in the curettings. In their research, 11% of these youthful than age 35, 12% of those 36 to 54, and 28% of those older than age 55 with atypical hyperplasia have been discovered to have carcinoma of their uterus. Thus in older sufferers with reasonable or severe atypical hyperplasia generally a hysterectomy is really helpful. In addition, those that fail progestin remedy and particularly those with severe cytologic atypia also needs to be thought of for hysterectomy. Studies are being carried out to consider the position of the progesterone containing intrauterine device. The prognosis of endometrial carcinoma is established by histologic examination of the endometrium. Initial prognosis can incessantly be made on an outpatient basis, with an office endometrial biopsy. If endometrial carcinoma is found, endocervical curettage could additionally be carried out to rule out invasion of the endocervix. A routine cytologic examination (Pap smear) from the exocervix, which screens for cervical neoplasia, detects endometrial carcinoma in solely roughly 50% of the instances. The endocervix is first sampled to rule out cervical involvement by endometrial most cancers, hysteroscopy is done to visualize the endometrial cavity, after which a complete uterine curettage is performed. Grading is decided by the percentage of strong components found in the tumor: grade 1 has lower than 5% strong elements, grade 2 has 6% to 50% stable components, and grade three has more than 50% strong elements. Previously, the time period adenoacanthoma was used to describe a well-differentiated tumor and adenosquamous carcinoma to describe a poorly differentiated carcinoma with squamous components. More just lately, the term adenocarcinoma with squamous components has been used with an outline of the degree of differentiation of both the glandular and squamous parts. They suggested the term adenocarcinoma with squamous differentiation, and this has been usually adopted. Uterine serous carcinomas are a extremely virulent and a less widespread histologic subtype of endometrial carcinomas (5% to 10%). They beneficial a radical operative staging (see subsequent section) in all circumstances of these tumors because of the excessive threat of extrauterine illness even in cases admixed with different histologic types (endometrial or clear cell). Histologically, they resemble clear-cell adenocarcinomas of the ovary, cervix, and vagina. Clear-cell tumors are inclined to develop in postmenopausal women and carry a prognosis much worse than typical endometrial adenocarcinomas. Survival rates of 39% to 55% have been reported, much less than the 65% or better normally recorded for endometrial carcinoma.