
Astelin dosages: 10 ml
Astelin packs: 1 sprayer, 2 sprayer, 3 sprayer, 4 sprayer, 5 sprayer, 6 sprayer, 7 sprayer, 8 sprayer, 9 sprayer, 10 sprayer

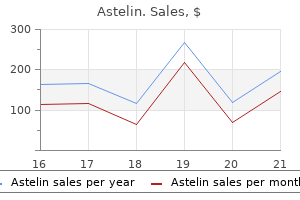
10 ml astelin buy fast delivery
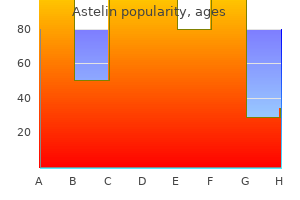
Elongated papillae with dilated capillaries and infiltration of eosinophils allergy medicine xyzal astelin 10 ml buy online, neutrophils allergy symptoms aches pains proven 10 ml astelin, and plasma cells mark the lamina propria. This encapsulated assortment of ganglion cells, with associated nerve fibers and supportive cells, lies between the two muscle layers of the muscularis externa. Smaller supportive cells and fibroblasts, which have extra condensed nuclei, surround several large ganglion cells (arrows) with spherical, euchromatic nuclei. Postganglionic sympathetic nerves and synapses between pre- and postganglionic parasympathetic nerves occur in the plexus. Smooth muscle cells (Sm) in the muscularis externa are sectioned longitudinally in the bottom and transversely in the prime. The bigger myenteric (Auerbach) plexus, between internal and outer layers of smooth muscle within the muscularis externa, mainly regulates easy muscle contraction, peristalsis, and gastrointestinal motility. The smaller submucosal (Meissner) plexus largely regulates glandular secretion and native blood flow. Areas of the digestive tract the place these features are minimal have a sparse submucosal plexus. Motor neurons modulate exercise of targets corresponding to smooth muscle, enteroendocrine, and glandular epithelial cells. Sensory neurons transmit impulses activated by mechanical or chemical stimuli in the mucosa. Interneurons, or interstitial cells of Cajal, are pacemaker cells that relay and combine info between different neurons. Parasympathetic nerve fibers normally activate physiologic digestive processes; sympathetic nerves are mainly inhibitory. The carcinoma is seen to come up from the mucosa and extends deeply into the wall, invading muscularis mucosae, submucosa, and reaching the muscularis externa. Tumor cells are organized into epithelial cords and nests separated by a unfastened connective tissue stroma, and the tumor cells appear to partially recapitulate the organization of stratified squamous epithelium. Individual cells have massive hyperchromatic nuclei, typically exhibiting mitoses, and the cords exhibit epidermoid "pearling," resembling keratinized islands (*), near the mucosal surface. The tumor from which this biopsy was taken was a big ulcerating neoplasm about 4 cm in diameter. While virtually 400,000 new cases are recognized annually, the incidence of this malignant epithelial tumor varies regionally, being more frequent in underdeveloped and rural areas of the world. It most frequently happens in adults over age 45 and sometimes impacts more males than girls. While long-term alcohol use and smoking are essentially the most vital risk components, exposure to sure food carcinogens. In contrast to esophageal adenocarcinomas, which generally develop in the lower finish of the esophagus, squamous cell carcinomas are more regularly discovered within the mid-esophagus, the place they usually cause strictures. Progressive dysphagia, excessive weight loss, fatigue, and anorexia are the most typical signs. By the time symptoms initially appear, the tumor is usually well advanced as it can quickly invade the esophageal wall, spreading to submucosal lymphatic vessels, simply penetrating the mediastinum (due to the absence of an outermost serosa in this part of the digestive system), and metastasizing to distant sites. Molecular mechanisms that result in this type of esophageal cancer include useful losses of the tumor suppressor gene p53. Whereas surgical resection in addition to neo-adjuvant radiation and chemotherapy are current types of treatment, prognosis is usually poor with a 5-year survival rate of 10%. Stomach Esophagus Lung bud Thyroid gland Pharynx Dorsal pancreas Hepatic diverticulum Midgut Hindgut Proctodeum Cut edge of amnion Arrow passing via right pleural canal from stomach coelom to pericardial coelom Esophagus Stomach Spleen Dorsal mesogastrium Celiac trunk Dorsal pancreas Mesoduodenum Common bile duct Duodenum Ventral pancreas Superior mesenteric artery Dorsal mesentery of midgut Inferior mesenteric artery Mesocolon of hindgut Developing right pleuroperitoneal membrane Ventral mesentery (lesser omentum) Septum transversum Gallbladder Liver (cut surface) Ventral mesentery (falciform ligament) Yolk sac stalk Allantois Umbilical wire Proctodeum Cloacal membrane Stomodeum Cardiac space Cut fringe of amnion Allantois Yolk stalk Yolk sac Body stalk At four weeks. Liver (cut surface) Gallbladder Falciform ligament Cecum passing to proper above coils of small intestine Cloaca At 5 weeks. Diaphragm Greater curvature of abdomen rotated 90� to left Spleen within dorsal mesogastrium bulging to left to form omental bursa Pancreas inside mesoduodenum Superior mesenteric artery inside dorsal mesentery Mesocolon Colon Urinary bladder Rectum Urorectal septum Yolk sac stalk Allantois Umbilical cord Genital tubercle Urogenital sinus Anus Ureter At 8 weeks. Abdominal distention showing hypertrophy of sigmoid and descending colon, reasonable involvement of transverse colon, and constricted distal phase. Later, lateral and cephalocaudal folding forms a protracted, cylindrical endodermal tube extending the length of the embryo; this turns into the primitive gut tube after which the digestive tract. A midgut within the center at first communicates with the yolk sac however then loses the connection. The endoderm turns into mucosal epithelium of the digestive tract and offers rise to the parenchyma and ducts of all intramural and accent digestive glands. Neural crest ectoderm migrates to the gut wall to give rise to myenteric and submucosal neural plexuses. The foregut provides rise to the pharynx, esophagus, stomach, proximal duodenum, liver, gallbladder, and pancreas. The hindgut types the the rest of the transverse colon, descending colon, sigmoid colon, and rectum. The foregut rotates ninety levels clockwise; the midgut, 270 degrees round its blood provide. Sheet-like mesenteries, derived from splanchnic mesoderm, droop and connect elements of the tube to the physique wall and serve as conduits for blood vessels, nerves, and lymphatics. Congenital megacolon (Hirschsprung disease)-the most typical intestine motility dysfunction caused by failure of migration of neural crest cells to the hindgut during weeks 5-12 of gestation-leads to partial or full obstruction, normally of the sigmoid colon and rectum, with aganglionic segments that lack Meissner and Auerbach plexuses. Meckel diverticulum-the most prevalent developmental anomaly of the bowel-is a small outpocketing (usually about 5 cm long) of the gastrointestinal tract caused by incomplete obliteration of the vitelline (yolk sac) stalk within the seventh gestational week. Usually asymptomatic, it might generally lead to intestinal obstruction, perforation, and bleeding. A thick mucosa (formed principally of tightly packed gastric glands) traces the lumen (*). The rectangle signifies a ruga consisting of a submucosal connective tissue core lined by mucosa. A thick layer of mucus secreted by surface cells varieties a barrier over the mucosa for defense of tissues from acid and proteolytic enzymes within the lumen. It stores and mixes meals and reduces it to a semisolid mass, known as chyme, which it delivers to the duodenum. As in other parts of the digestive tract, the wall has four concentric layers: mucosa, submucosa, muscularis externa, and serosa. The internal lining shows irregular longitudinal folds, often recognized as rugae, which can be seen by the naked eye in a contracted abdomen. This epithelium often dips to kind small gastric pits, or foveolae, which lead to long tubular gastric glands. Gastric pits and glands provide up to 800 m2 of total surface space for secretion of mucus, acid, and digestive enzymes. The three types of glands have the same general structural plan but with regional histologic variations. In the physique and fundus, main gastric glands, the most important and most numerous, make up about 75% of the mucosa. The pyloric space close to the duodenum accommodates small pyloric glands that represent about 15% of the mucosa and resemble cardiac glands. The most common diagnostic test is gastroscopy-passage from mouth to abdomen of a skinny, versatile tube with a camera attachment-for inspection of the gastric mucosa.
Buy astelin 10 ml with amex
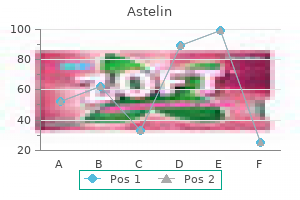
These junctions dissociate temporarily after which reassemble as germ cells move toward the lumen allergy treatment pipeline buy discount astelin 10 ml on-line. Basal cytoplasm of Sertoli cells contains a Golgi complicated allergy zone 10 ml astelin order amex, lipid droplets (Li), clean endoplasmic reticulum, and many mitochondria (Mi). More apical areas of those cells appear as slender, sleeve-like processes (*) that encase germ cells prior to spermiogenesis. A cleavage point of cytokinesis is seen between two intently apposed spermatocytes (oval). These columnar cells, with borders that are hard to distinguish, prolong from the basement membrane to the lumen of the seminiferous tubule. Their apices bear crypt-like recesses that maintain spermatids until launch of newly formed spermatozoa into the lumen. The cytoplasm incorporates microtubules and intermediate filaments forming a distinguished cytoskeleton, in addition to lengthy, slender mitochondria, a conspicuous smooth endoplasmic reticulum, giant numbers of lipid droplets, and lipofuscin-laden lysosomes. Adjacent cells are linked by basolateral tight junctions, such that the epithelium is split into basal and adluminal compartments. The resulting blood-testis permeability barrier separates spermatogonia and first spermatocytes from extra apical secondary spermatocytes and spermatids. Contents in the seminiferous tubule lumen are thus isolated from circulating antigens, thereby protecting spermatocytes and spermatids from autoimmune reactions and blood-borne substances. Sertoli cells phagocytose spermatid remnants and secrete fluid and tons of substances, together with androgenbinding protein, important for spermatozoa survival. Cell junctions are closely associated to actin filaments and endoplasmic reticulum at websites known as ectoplasmic specializations, which may modify to modifications in junctional structure as spermatozoa transfer towards the lumen. The extensive cytoskeletal network of Sertoli cells helps provide for spermatozoa motion. Spherical lipid droplets are electron dense, and tubulovesicular mitochondria (arrows) are scattered in cytoplasm. Their foamy, washed-out cytoplasm is due to excessive lipid content, as they retailer cholesterol for synthesis of testosterone. These massive polyhedral cells have an eccentric spherical nucleus with one or two distinguished nucleoli, and cell surfaces have numerous small microvilli. Relatively few ribosomes and tough endoplasmic reticulum, numerous scattered mitochondria with tubulovesicular cristae, a large juxtanuclear Golgi complex, and heaps of spherical lipid droplets of varied sizes also occupy the cytoplasm. Rectilinear crystalloid inclusions (crystals of Reinke) possessing a highly ordered pattern of inner structure additionally occur in human Leydig cells, however their function stays enigmatic. The amount of lipofuscin pigment related to tertiary lysosomes additionally increases in old age. The etiology is unknown, but disruption of the hypothalamic-pituitary-testicular axis causing extreme stimulation of Leydig cells could contribute to tumorigenesis. Prepubertal boys normally show indicators of precocious virilization; adults usually exhibit gynecomastia and lack of libido. Treatment options are surgical enucleation when the tumor is encapsulated or radical inguinal orchiectomy with excessive ligation of the spermatic twine. Many brief microvilli project from the cell surface and abut the outer facet of the capillary endothelium. The tubulovesicular cristae of mitochondria (arrows) seem just like these in different steroid-secreting cells. Structural complexity of the internal mitochondrial membranes on this cell most likely enhances floor area for operate. After transport proteins transfer ldl cholesterol to their internal cristae, mitochondria play a job in changing cholesterol to pregnenolone underneath the influence of luteinizing hormone. Produced constantly by these cells, testosterone diffuses throughout the cell membrane, which is studded with microvilli that amplify its floor area. Testosterone released into the extracellular space associates rapidly with steroid-binding proteins within the circulation. The crescent-shaped epididymis consists mainly of a highly tortuous duct held together by unfastened connective tissue and covered by the visceral tunica vaginalis (arrows). A dilated cyst-like structure (*) within the head of the epididymis corresponds to the appendix epididymis, a mesonephric duct remnant. The epididymis, derived from the mesonephros in the embryo, is divided into three components: an initial (head) segment, a body (the major a half of the duct), and a caudal (tail) region. Several cross and oblique views of the same duct are normally seen in histologic sections-evidence of the extremely convoluted nature of the duct. In 25% of males, the head accommodates a pedunculated cystic structure, the appendix epididymis, which is believed to be an embryologic remnant. The head receives efferent ductules that emerge from the rete testis and is engaged primarily in absorption of fluid and particulate matter. The efferent ductules are lined by ciliated columnar epithelium; the cilia beat in the path of the epididymis and may help motion of spermatozoa. In younger males it normally arises as a complication of gonorrhea or as a sexually acquired an infection with Chlamydia. Retrograde unfold of infection from the urethra and decrease urinary tract often happens. In older men, this dysfunction is usually associated with urinary tract infections attributable to coliform bacteria similar to Escherichia coli. Chronic epididymitis is characterised histologically by accumulation of plasma cells and macrophages adopted by fibrosis and duct obstruction. The wall consists of tall pseudostratified epithelium of uniform thickness with apical nonmotile stereocilia. Tall columnar cells have elongated, euchromatic nuclei and long, apical stereocilia. This noninvasive imaging modality is useful in detecting problems of the testis, epididymis, and scrotum. Stereocilia amplify the cell surface space and performance in absorption of extra fluid that accompanies spermatozoa from the testis. The epididymis can additionally be a protracted storage duct via which spermatozoa pass slowly, their journey taking one to several weeks. Loose connective tissue and a few circularly organized clean muscle are additionally found outside the ducts. The easy muscle in the head of the epididymis undergoes spontaneous peristaltic contractions. In the epididymis tail, nevertheless, contraction is stimulated by adrenergic innervation during sexual stimulation, which promotes ejaculation. Around the mucosa is a outstanding three-layer coat of tightly spiraled smooth muscle, the muscularis. Blood vessels, nerves, and lymphatics journey through an adventitia of loose connective tissue that covers the ductus externally.
Diseases
- Weleber Hecht Bigley syndrome
- Chromosome 3, trisomy 3p
- Neurocysticercosis
- Moloney syndrome
- Collins Sakati syndrome
- Criss cross syndrome
Discount astelin 10 ml amex
Damage to pyramidal cells in both areas that has been attributable to ischemia and/or excessive levels of corticosteroids is synergistic penicillin allergy symptoms joint pain buy 10 ml astelin overnight delivery. Brain sixty nine Interventricular foramen Corpus callosum (cut) Cut fringe of tela choroidea of third ventricle third ventricle Choroid plexus Internal cerebral vein Superior thalamostriate vein (vena terminalis) Head of caudate nucleus Septum pellucidum Columns of fornix Anterior tubercle Stria terminalis Interthalamic adhesion Pes hippocampi Inferior horn of lateral ventricle Dentate gyrus Collateral eminence Hippocampus Fimbria of hippocampus Lamina affixa Stria medullaris Habenular trigone Pulvinar (lifted) Lateral geniculate body Medial geniculate body Brachium of superior colliculus Posterior commissure Brachium of inferior colliculus Habenular commissure Pineal gland Collateral trigone Cerebellum Calcar avis Posterior horn of lateral ventricle Superior colliculus Inferior colliculus Calcarine sulcus (fissure) 3 allergy testing instruments cheap astelin 10 ml with visa. The complete right aspect of the brain, just lateral to the thalamus, has been eliminated, the head of the caudate nucleus has been sectioned, the corpus callosum and all tissue dorsal to the thalamus have been removed, and the third ventricle has been opened from its dorsal floor. The pineal gland is present within the midline, just caudal to the third ventricle; it produces melatonin, a hormone that helps regulate circadian rhythms, sleep, and immune responses. The superior and inferior colliculi are shown, depicting the dorsal surface of the midbrain. On the left, the temporal horn of the lateral ventricle, with the hippocampal formation, has been uncovered to show the connection of these structures to the thalamus. The terminal vein and choroid plexus accompany the stria terminalis alongside the lateral margin of the thalamus. Many of these thalamic nuclei are "particular" thalamic nuclei that are reciprocally related with discrete regions of the cerebral cortex. Some nuclei, corresponding to these embedded within the inner medullary lamina (intralaminar nuclei such because the centromedian and parafascicular nuclei) and the outer, lateral shell nucleus (reticular nucleus of the thalamus), have very diffuse, nonspecific associations with the cerebral cortex. Initially, all sensation is lost in the contralateral physique, epicritic more fully than protopathic. Even light stimulation can evoke such pain (hyperpathia), and other sensory stimuli or emotionally charged conditions can lead to these painful sensations. If the vascular lesion contains the subthalamic nucleus or associated basal ganglia circuitry, the patient can also expertise hemiballismus (or choreoform or athetoid) movements in addition to the sensory deficits. The three cerebellar peduncles (superior, center, and inferior) are sectioned and the cerebellum removed. The dorsal roots present input into the spinal twine, and the cranial nerves provide enter into and obtain output from the mind stem. The fourth nerve (trochlear) is the one cranial nerve to exit dorsally from the brain stem. The tubercles and trigones on the ground of the fourth ventricle are named for nuclei simply beneath them. The superior and inferior colliculi type the dorsal surface of the midbrain, and the medial and lateral geniculate our bodies (nuclei), related to auditory and visual processing, respectively, are shown on the caudalmost region of the diencephalon. The superior peduncle conveys the main efferents to the pink nucleus and thalamus (especially the ventrolateral nucleus), whereas the inferior peduncle conveys the most important efferents to the vestibular and reticular nuclei. Afferents enter the cerebellum especially through the inferior peduncle but additionally by way of the superior peduncle. Damage to the lateral hemisphere of the cerebellum or its associated peduncles ends in ipsilateral symptoms, together with limb ataxia, mild hypotonia, dysmetria (misjudgment of distance), decomposition of movement (especially motion involving a number of joints), intention tremor (with movement), dysdiadochokinesia (inability to perform speedy alternating movements), and incapability to dampen movements appropriately (rebound phenomena). The cerebral peduncles, direct caudal extensions of the posterior limbs of the internal capsules, carry corticospinal and corticobulbar fibers from the internal capsule to the spinal wire and mind stem, respectively. The decussation of the pyramids marks the boundary between the caudal medulla and the cervical spinal wire. In circumstances of elevated intracranial stress within the anterior and middle cranial fossa, such as that brought on by a tumor, edema from harm, or different space-occupying lesions, the mind stem can herniate via the tentorium cerebelli, a rigid wing of dura. The resultant transtentorial herniation can compress the third nerve on one facet (ipsilateral fixed and dilatated pupil ensuing from parasympathetic disruption; and paralysis of medial gaze resulting from motor fiber disruption) and compress the cerebral peduncle on that very same aspect, resulting in contralateral hemiparesis. The medullary pyramids comprise the descending corticospinal tract fibers from the ipsilateral cerebral cortex, particularly from the motor and premotor cortex. The main crossing of the corticospinal tract takes place in the decussation of the pyramids (80%), producing the crossed, descending, lateral corticospinal tract within the spinal wire. Damage to other descending techniques, from both the motor-related cortices or other higher motor neurons within the brain stem, should accompany pyramidal tract harm to produce spasticity. Thus, the time period pyramidal tract syndrome, when used to describe spastic hemiplegia, is a misnomer and is anatomically incorrect. The anterior, center, and flocculo-nodular lobes of the cerebellum are conventional anatomic subdivisions with well-described syndromes derived from lesions. The vermis, paravermis, and lateral hemispheres are cerebellar cortical zones that have particular projection relationships with deep cerebellar nuclei (vermis with fastigial nucleus and lateral vestibular nucleus; paravermis with globose and emboliform nuclei; lateral hemispheres with dentate nucleus) which, in turn, present neuronal feedback to specific higher motor neuronal methods that regulate specific forms of motor responses. These relationships are key to understanding how the major higher motor neuronal techniques are coordinated for particular practical duties. The anterior cerebellum additionally helps to regulate tone in the limbs via connections to the lateral vestibular nucleus. In some alcoholic patients, the anterior lobe of the cerebellum shows selective cortical degeneration. The affected person reveals a wide-based stance and gait with some ataxia however little involvement of dysarthria or oculomotor dysfunction. The gait tends to be stifflegged, in all probability reflecting disinhibition of the extensor-dominant lateral vestibular nucleus. BrainStemandCerebellum seventy five Decussation of superior cerebellar peduncles Cerebral peduncle Medial longitudinal fasciculus 4th ventricle Superior medullary velum Fastigial nucleus Globose nuclei Dentate nucleus Emboliform nucleus Lingula Cerebellar cortex Vermis Superior cerebellar peduncle Section in aircraft of superior cerebellar peduncle Purkinje cell layer White matter zone Molecular layer Granular cell layer Molecular layer External floor Cerebellar architecture. The infolding of cerebellar folia demonstrates the architecture of the cerebellar cortex. Molecular layer Dendritic bushes Dendritic bushes Basket cell arborizations Purkinje cells Granular cell layer Cerebellar cortex. Purkinje cells with their large planar dendritic bushes arborizing into the molecular layer. Densely-packed granule cells sit deep to the Purkinje cells within the granular layer. The outer zone, the cerebellar cortex (three-layered), is infolded to form quite a few folia. Deep to the folia is the white matter, carrying afferent and efferent fibers associated with the cerebellar cortex. Deep to the white matter are the deep cerebellar nuclei, cell groups that receive many of the output from the cerebellar cortex via Purkinje cell axon projections. The deep cerebellar nuclei additionally receive collaterals from mossy fiber and climbing fiber inputs to the cerebellum. These direct afferent inputs to the deep nuclei provide a rough adjustment for his or her output to upper motor neurons, whereas the loop of afferent enter through the cerebellar cortex back to the deep nuclei offers fine changes for his or her output to upper motor neurons. The cerebellar peduncles are inside to the deep nuclei; these huge fiber bundles interconnect the cerebellum with the brain stem and the thalamus. Such impingement can cause excruciating, radiating pain if dorsal roots are concerned and might trigger loss of motor management of affected muscular tissues if ventral roots are concerned. In the adult, the spinal twine extends caudally solely so far as the L1 vertebral physique, leaving the lumbar cistern (the subarachnoid space) accessible for withdrawal of cerebrospinal fluid.
10 ml astelin buy otc
Treatment of vulvovaginal lichen planus with vaginal hydrocortisone suppositories allergy forecast helotes best 10 ml astelin. The association of lichen sclerosus and erosive lichen planus of the vulva with autoimmune illness: a casecontrol examine allergy symptoms face numbness buy 10 ml astelin amex. Patient satisfaction after the treatment of vulvovaginal erosive lichen planus with topical clobetasol and tacrolimus: a survey research. Real-life expertise of managing vulval erosive lichen planus: a case-based evaluation and U. Erosive vulvar lichen planus: retrospective evaluate of characteristics and outcomes in 113 sufferers seen in a vulvar specialty clinic. Possible Complications: Vulvar lesions are sometimes chronic and may endure malignant change. Workup and Evaluation Laboratory: Thyroid function research should be thought-about because up to one-third of patients have coexisting hypothyroidism. Punch biopsy of the skin will set up the diagnosis, however may not be required in lots of instances. Diagnostic Procedures: History, physical examination, and biopsy of affected space. Pathologic Findings Loss of regular vulvar structure with loss of rete pegs; a homogeneous dermis with edema, fibrin, and lack of vascularity; elastic fibers; and dermal collagen. Chronic irritation is frequent, and spongiosis of the basilar epithelial cells is usually present. Specific Measures: Topical steroid therapy is preferred over the traditional testosterone cream. This is related to a excessive rate of recurrence and the danger of postsurgical scarring. Lower-potency steroids (hydrocortisone) may be used after initial remedy or in youngsters. Prolonged testosterone propionate remedy may be related to clitoral enlargement or pain, local burning, or erythema. Areas that turn into hyperplastic on account of scratching are thought to be at elevated threat for premalignant or malignant modifications (lifetime threat of squamous cell carcinoma is 3%�5%). Expected Outcome: Initial response is generally good, however recurrence is common, often necessitating lifelong therapy. Possible Complications: Scarring and narrowing of the introitus may be adequate to preclude intercourse. A double-blind, randomized potential research evaluating topical clobetasol propionate 0. Long-term administration of adult vulvar lichen sclerosus: a prospective cohort study of 507 girls. Vulvar lichen sclerosus: effect of long-term topical software of a potent steroid on the course of the disease. Lichen sclerosus with vaginal involvement: report of two circumstances and evaluation of the literature. A synchronous second malignancy, mostly cervical neoplasia, is found in as much as 22% of patients with a vulvar malignancy. The majority of girls have had signs for greater than 6 months earlier than a prognosis is made. Specific Measures: Initial treatment consists of broad native excision (1-cm margins). Subsequent therapy, together with node dissections and adjunctive remedy (radiation), is set by the stage of disease, cell sort, and surgical margins. A 5% acetic acid resolution may be applied, and the vulva is examined by colposcopy. Some evaluations have suggested that imiquimod is an various choice to surgical administration in choose patients. Pathologic Findings Histologic varieties embody squamous cell (90%), melanoma (5%), basaloid, warty, verrucous, giant cell, spindle cell, acantholytic squamous cell (adenoid squamous), lymphoepithelioma-like, basal cell, and Merkel cell. Possible Complications: Distant spread and disease progression, secondary infection. Expected Outcome: If tumor invasion is less than 1 mm, the risk of lymph node involvement is essentially zero, and excessive success rates may be expected. Five-year survival rates decline with advancing stage: 20% with deep node involvement. Prevalence of mucosal and cutaneous human papillomaviruses in numerous histologic subtypes of vulvar carcinoma. Patterns of unintended genital trauma in young ladies and indications for operative management. Genital and anal accidents requiring surgical restore in females less than 21 years of age. Retrospective review of unintentional female genital trauma at a pediatric referral heart. Expected Outcome: Most hematomas steadily resolve with conservative management solely. In addition, the tissues of the vulva symbolize a rich ecosystem, with interactions between tissues, fluids, hormones, and microbes. Objectives of Management: To establish a timely diagnosis and administration plan for these sufferers with vulvar lesions. Just as in other areas of the body, the vulva is susceptible to inflammatory and dermatologic diseases. Intertrigo, pimples inversa, psoriasis, seborrheic dermatitis, Fox-Fordyce disease, fifth illness, adjustments caused by Beh�et or Crohn diseases, viral infections, and parasites could all have an result on the pores and skin of the vulva. The pores and skin of the vulva can be weak to irritation from vaginal secretions, recurrent urinary loss, or contact with external irritants (such as cleaning soap residue, perfumes, material softeners, or infestation by pinworms). Changes could happen because of the effects of diabetes or hormonal alterations and dermatoses such as hypertrophic dystrophy, lichen sclerosus, and psoriasis. Strategies: the character of the lesion or vulvar findings may be used to establish a working diagnosis for a affected person with a vulvar lesion. It is essential to consider that many circumstances that trigger vulvar lesions could current in a number of types. Consequently, in any decision tree based mostly on lesion morphology, some diagnoses could also be represented on the end of multiple department (eg, seborrheic keratosis or nevus). When cystic constructions are encountered, the possibility of congenital remnants such as mesothelial cysts (cysts of the Canal of Nuck), Wolffian duct remnants, and periurethral cysts have to be considered. Lipomas, neurofibromas, rhabdomyomas, schwannomas, and leiomyomas might present as fleshy tumors of the vulva. Of special significance are lesions that contain important necrosis: necrotizing fasciitis and pyoderma gangrenosum. Both of those processes symbolize a significant threat to the life and well being of the patient and require prompt and aggressive treatment. Prevalence: Some estimates place it at 15% of all women, however significant, disabling signs are much much less widespread.
Cheap astelin 10 ml otc
Arranged in pairs allergy testing mackay qld cheap 10 ml astelin, they include a folding of endothelium with a thin collagenous connective tissue core allergy forecast colorado order astelin 10 ml with visa. The commonest causes of this life-threatening condition are issues from malignant lymphoma and trauma brought on by thoracic, mediastinal, or cardiac surgical procedure. Treatment choices embrace pleural drainage; thoracic duct ligation by way of thoracoscopy; omitting fat from the food regimen; and treatment with noninvasive subcutaneous drugs, similar to synthetic analogues of somatostatin, to prevent fluid effusion. Fatty streak at margin Lumen Thrombus Plaque rupture 209 Calcification Adventitia Media * Necrotic core with ldl cholesterol deposits Intima Angina pectoris. Discomfort in left chest is most often attributable to partial or complete occlusion of coronary arteries by atherosclerosis, which develops over a period of a long time. The arterial lumen (*) is an attenuated slit that contains some blood at its decrease margin. The dark-purple staining is calcification of the intima (known as M�nckeberg calcific sclerosis; first described in 1903), which localizes to intima and some to media. At high magnification, conspicuous brown "foam" cells-rich in lipofuscin deposits-represent dying macrophages. Surrounding the artery in the adventitia (Top Left of Upper Image) is an abundance of inflammatory (lymphoid) cells, which may or will not be current in atherosclerosis. Typically progressing with out symptoms for years, clinical onset may be gradual or abrupt. A major danger issue is hypercholesterolemia: excessive circulating levels of low-density lipoproteins. Blood monocytes migrate across the endothelium to become macrophages, which accumulate lipids. Smooth muscle cells in the media additionally migrate to affected intimal websites and turn out to be cholesterol-laden foam cells, which can set off formation of a thrombus that may obstruct lumina of affected arteries. To enhance quality of life and decrease threat of demise, targets of remedy are modification of threat factors, mostly hypertension, hyperlipidemia, and diabetes mellitus. Appropriate bodily train, dietary management to treat acute ischemic symptoms, and pharmacotherapeutic approaches. Lymphatics of higher limb Tonsils Three-dimensional view of jejunal wall Organization of lymphatic system. Its major features are thus to function a source of immunocompetent cells that may react with and neutralize antigens and to distinguish self from nonself. The system comprises lymphoid tissues and organs whose major constituents are aggregates of lymphocytes and other cells of the mononuclear phagocyte system. These cells are enmeshed in a supportive framework (stroma) of reticular cells and fibers, so lymphoid tissue is classed as a specialised reticular connective tissue. More densely packed, spherical clusters of lymphocytes referred to as lymphoid nodules (or follicles) may be present in these and other websites. The nodules may appear as single collections of lymphocytes or as extra everlasting, multiple aggregates, similar to tonsils and Peyer patches. Discrete lymphoid organs may be encapsulated (lymph nodes, thymus, and spleen) or unencapsulated (bone marrow). Primary lymphoid organs-major websites of lymphocyte manufacturing and maturation-include bone marrow, the place B lymphocytes are produced, and thymus, where T lymphocytes mature. B cells mediate humoral immunity by giving rise to plasma cells, which synthesize antibodies (or immunoglobulins) that inactivate overseas antigens. Immune responses occur in secondary lymphoid organs, corresponding to lymph nodes and spleen. All lymphoid tissue derives embryonically from mesoderm, apart from the thymus, which arises from mesoderm and endoderm. Flattened endothelial cells line its lumen (*), which is full of pink precipitate rich in proteins and lipid. A valve (arrows) facilitates movement of lymph in one path by stopping backflow. Like venous valves, lymphatic valves are composed of endothelial-lined leaflets with a really thin connective tissue core. The lumen (*) incorporates nucleated blood cells, mostly lymphocytes, and a flocculent precipitate, which corresponds to the lightly eosinophilic protein of lymph. The arteriole has the thickest wall with two layers of smooth muscle in its media. The venule has a thinner wall and comparatively larger lumen, which is filled with erythrocytes. Lymphatic capillaries look much like blood capillaries except that they lack a basal lamina. Small anchoring filaments connect endothelial cells to adjoining collagen fibers and assist prevent vessel collapse. Lymphatic capillaries are most ample in connective tissue of the skin (dermis); beneath mucous membranes of the respiratory, gastrointestinal, and genitourinary tracts; and in connective tissue spaces of the liver. These vessels take in interstitial fluid, which fills the extracellular connective tissue matrix. This fluid and wandering lymphocytes are taken up and added again to the circulation. Like veins, lymphatic vessels have valves and thin partitions; contraction of surrounding skeletal muscle tissue causes lymph to transfer. The large lymphatic ducts drain into the subclavian veins, right at the angle junction the place the jugular vein and subclavian vein be part of together. This primary nodule lacks a germinal center however incorporates a densely packed, spherical cluster of lymphocytes. Lymphocytes usually migrate from the lamina propria and cross the epithelium on their method to the lumen. Lymphocytes in these areas may type lymphoid nodules (or follicles), that are dense aggregations of lymphocytes arranged as spherical, unencapsulated clusters. There are two varieties, main and secondary: a major nodule incorporates small, immature B lymphocytes. In response to antigen publicity, main nodules turn into secondary nodules, which contain pale-stained germinal centers. They are websites of in depth B lymphocyte proliferation and differentiation into 9. Also, specialized epithelial cells referred to as M cells are ample within the dome epithelium of Peyer patches. They take up small particles, similar to bacteria and viruses, which are then engulfed by submucosal macrophages that process material and present it to B and T cells. Rubella, generally known as German measles, is a contagious sickness caused by rubella virus; its hallmark is an erythematous maculopapular rash plus fever and swollen lymph nodes. Rubella happens primarily in children and younger adults; in pregnant girls it poses a severe risk to a fetus. Surrounded by a capsule (Ca), it has an outer cortex (Co) and central medulla (Me). They occur, often as chains or groups, in strategic regions such as the neck, groin, mesenteries, axillae, and abdomen. During improvement, particular regions of each node are seeded with B lymphocytes from the bone marrow and T lymphocytes from the thymus.
10 ml astelin sale
The capillary endothelium allergy shots effects on immune system discount astelin 10 ml with visa, the continuous allergy medicine makes me depressed astelin 10 ml cheap online, nonfenestrated sort, also accommodates tight junctions. Ultrastructurally, endothelial cells are organized as an interlocking, contiguous mosaic. Cytoplasm of endothelial cells contains (near the nucleus) mitochondria, Golgi complex, microtubules, microfilaments, Weibel-Palade bodies, and tough endoplasmic reticulum. Organelles are almost completely absent in slender extensions of endothelial cells, which in some areas may be fairly thin-only zero. The most hanging function of these cells is the presence of numerous vesicles, which are free in the cytoplasm or carefully associated with luminal and abluminal cell surfaces and whose main operate is to transport fluid and proteins between blood and surrounding interstitium. Short, stubby microvilli project from different parts of the cell floor (small arrows). Profiles of pulmonary capillaries (Cap) and portions of alveolar spaces (*) are additionally seen. In this optimally preserved specimen, the fingerprint construction typical of surfactant is evident. They have a single, centrally positioned, rounded nucleus, which is often euchromatic, with one or two distinguished nucleoli. Short stubby microvilli project from the cellular surface into the alveolar lumen. Their cytoplasm contains a well-developed Golgi complex, profiles of rough and clean endoplasmic reticulum, scattered mitochondria, and peroxisomes. Large, pleomorphic membrane-bound multilamellar our bodies, a singular function of these cells, can be noticed extruding their contents into alveolar areas. The bodies are filled with electron-dense lamellar materials and represent secretory vesicles. They are derived from the Golgi complex and are in the end discharged by exocytosis on the cell floor. This replicative potential is necessary for therapeutic after lung harm, because the large floor space of type I cells makes them particularly prone to harm. Primary and secondary lysosomes are a notable feature of its cytoplasm, and its nucleus has an indented margin. Also seen are thin processes of type I pneumocytes (arrows) lining the alveolus (*), and lumina of two pulmonary capillaries (Cap). They are often seen bulging into the alveolar area, typically situated at junctions between adjoining interalveolar septa. Their cytoplasm accommodates varied organelles, together with many main and secondary lysosomes. Their main function is to ingest mud and other overseas particles that have entered alveolar spaces throughout inspiration. Electron microscopy has proven that the cells have an irregular form and a floor studded with pseudopodia and brief microvilli. These motile cells are derived from blood monocytes whose precursors come up in bone marrow. They migrate across the partitions of pulmonary capillaries to the interalveolar septa. They bear maturational division in the interstitium of the lung after which enter alveolar spaces to lie free within the lumina. In sure kinds of coronary heart illness, similar to congestive coronary heart failure, erythrocytes from the bloodstream could escape into pulmonary alveolar areas, the place alveolar macrophages may phagocytose them. These swollen macrophages with ingested hemosiderin may be seen in sputum and are generally recognized as heart failure cells. Signs embrace labored breathing and cyanosis, which are brought on by inability of pulmonary alveoli to expand or stay open after inspiration. Treatment choices depend upon illness severity and prematurity of the toddler and embody supply of O2 to help respiration, mechanical air flow, corticosteroid remedy, and delivery of synthetic surfactant to the lungs. Respiratory System Developing respiratory tract (Top) at 4-5 weeks and bronchi and lungs (Bottom) at 5-6 weeks. At 20 weeks Terminal bronchiole Alveolar ducts Terminal sacs (future alveoli) Simple cuboidal epithelium Oropharyngeal membrane Mandibular (1st branchial) arch Ventral aorta Ventricle of coronary heart Pulmonary artery Esophagus Laryngotracheal ridge Trachea Bronchial buds At 24 weeks Respiratory bronchiole Alveolar duct Connective tissue Terminal sacs (future alveoli) Ventral view of pharynx. At this pseudoglandular developmental stage, the lung has a glandular look with many thinwalled tubes (arrows) and sacs (*) of various styles and sizes lined by easy squamous to cuboidal epithelium. The future larynx develops from the higher a part of the tube; the trachea, from the caudal half. Two knob-like thickenings at its most distal finish become the bronchial buds, which undergo about 20 successive divisions before birth, followed by continued postnatal development. Growth of endodermal epithelium is accompanied by invasion and condensation of surrounding splanchnic mesenchyme, which envelops the tube. The mesenchyme gives rise to connective tissue, clean muscle, and cartilage of the airways; endoderm is the source of the epithelium and its related intramural glands. Bronchi and lungs develop like an exocrine gland: Bronchi are equal to extralobular ducts, whereas bronchioles are counterparts of intralobular ducts. Five phases of lung improvement embrace the embryonic interval from 26 days to 6 weeks, with preliminary growth of lobar bronchi. In the pseudoglandular section between 6 and 16 weeks, terminal bronchioles, which appear as blind tubules lined with cuboidal or columnar epithelium, develop additional. The canalicular interval, 16-28 weeks, contains growth of acini accompanied by invasion of capillaries from surrounding mesenchyme. The saccular interval, 28-36 weeks, is adopted by the alveolar period, from 36 weeks to delivery. Alveoli vary markedly in dimension and form; many are distended and present reasonable thickening of their partitions (septae). Alveolar spaces are crammed with pinkstained homogeneous edema fluid and inflammatory cellular exudate, comprised principally of polymorphonuclear leukocytes (neutrophils). At excessive magnification, parts of bronchiolar epithelium appear damaged and disrupted. Many dark macrophages that harbor lipofuscin are present in lamina propria of bronchioles, alveolar septae, and inside alveolar areas. Inflammatory exudate Fibrin net Macrophages Congested capillaries Staphylococci (arrow) and polymorphonuclear leukocytes in sputum (Gram stain) 15. Clinical signs sometimes embrace dry or productive cough, pleuritic chest pain, sputum manufacturing, shortness of breath, fever, and chills. Lobular bronchopneumonia and lobar pneumonia are two major patterns of illness distribution. Bacterial invasion and proliferation into airways is adopted by release of poisons causing irritation and edema of alveoli with migration of neutrophils from pulmonary capillaries, accumulation of mobile debris in alveolar spaces, and consolidation (or solidification) of fluid exudate. Treatment tips differ relying on causative agent, severity of sickness, and preliminary site of pathogen publicity. To eradicate infection, scale back morbidity, and prevent issues, effective treatment of bacterial pneumonia might include antibiotic microbial remedy. Kidney Lateral border Anterior surface of proper kidney Fibrous capsule (cut and peeled back) Medial border Hilum Renal artery Ureter Renal vein Renal pelvis Psoas major m. Fibrous capsule Cortex Minor calyces Renal sinus Major calyces Renal pelvis Pelvic ureter Rectum Bladder Medulla (pyramids) Renal papilla Urethra Prostate Renal column Medullary rays Regional anatomy of the urinary system.
Boldea fragrans (Boldo). Astelin.
- What is Boldo?
- Are there any interactions with medications?
- Gallstones, achy joints (rheumatism), bladder infections, liver disease, anxiety, gonorrhea, fluid retention, constipation or flushing out of the bowels, mild stomach or intestinal spasms, and other conditions.
- Dosing considerations for Boldo.
- How does Boldo work?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96588
Astelin 10 ml order overnight delivery
Extrahepatic bile ducts include all layers of the gallbladder wall and are lined by an epithelium much like allergy shots weaken immune system astelin 10 ml cheap with visa that of the gallbladder xyzal allergy testing discount astelin 10 ml fast delivery. A thin basement membrane separates epithelium from underlying connective tissue, which accommodates a capillary. Epithelial cells often appear columnar, but anatomic and useful variations could cause them to look cuboidal, as here. Apical cytoplasm is frivolously eosinophilic; an apical brush border incorporates many brief microvilli. The epithelium rests on a delicate basement membrane that separates it from underlying lamina propria. By electron microscopy, junctional complexes, including tight junctions, link lateral cell membranes near the lumen. Basal infoldings of plasma membrane and interdigitations of adjacent cell membranes mirror the function of those cells in ion transport. Water from the lumen is absorbed into lateral intercellular spaces between epithelial cells and then to the underlying, richly vascularized lamina propria. The gallbladder shops bile, which is launched by reflex contraction of clean muscle in its wall in response to the hormone cholecystokinin. Concomitantly, sphincters associated with the frequent bile duct and the ampulla loosen up to allow bile to enter the duodenum. Occurring more regularly in men than in women, risk factors are persistent cholecystitis and cholelithiasis. Usually affecting the fundus and neck of the organ, such neoplasms are probably to metastasize rapidly to adjacent organs, so patients often have superior disease at time of diagnosis; therefore early detection and treatment are essential. Diagnosis is via transabdominal ultrasonography, endoscopic retrograde cholangiopancreatography, and magnetic resonance imaging; liver function exams show elevations of serum alkaline phosphatase and bilirubin. Surgical treatment (cholecystectomy and resection of a half of adjoining liver and lymph nodes) is healing for tumors involving the mucosa and submucosa. The pancreas is organized into vague lobules of varying dimension with tightly packed and darkly stained parenchyma surrounded by free connective tissue stroma. Situated on the posterior wall of the abdominal cavity, the gland has a retroperitoneal position at the degree of the primary and second lumbar vertebrae. Its head lies within the concavity of the duodenum; its neck, body, and tail prolong transversely to the spleen. Its serosa-covered anterior floor is separated by the omental bursa from the posterior abdomen wall. Like other parenchymal glands, the pancreas is covered by a skinny, vague connective tissue capsule, which sends inward projections, or septa, of loose connective tissue that partially subdivide the gland into indistinct lobules. The exocrine part comprises 99% of the gland by weight and is made from secretory acini and their associated ducts. The endocrine part of the pancreas consists of islets of Langerhans, which produce several hormones that have an effect on carbohydrate metabolism. Thumbnail areas in the three bins are seen at higher magnification beneath, and present completely different parts of the excretory duct system traversing the gland. Short, branching intercalated ducts-the preliminary part of the excretory duct system- drain acini and are lined by a low simple cuboidal epithelium (A). Longer intralobular ducts are lined by easy cuboidal epithelium consisting of more plump cells (B). Larger interlobular ducts are lined by easy cuboidal epithelium invested by dense fibrous connective tissue (C). Interlobular ducts, in turn, drain immediately into the principle pancreatic ducts, which ship secretions to the duodenum. Secretory cells of acini are intensely eosinophilic, have basal nuclei, and produce digestive enzymes. Pale cells within the richly vascularized islets constitute the endocrine part of the gland. They lead into small intralobular intercalated ducts that are lined by one layer of low cuboidal epithelial cells. Intercalated ducts lead into larger interlobular ducts outdoors the lobules and lined by simple cuboidal to low columnar epithelium. Interlobular ducts branch extensively, get bigger, and empty into two primary excretory ducts. The smaller accent pancreatic duct receives branches from the pancreatic head; it communicates with the primary duct and opens about 2 cm above it. Both ducts are lined by easy columnar epithelium, surrounded by a layer of connective tissue. Small mucous glands open into the bigger ducts and lubricate and protect the liner epithelium. The endocrine part of the pancreas-islets of Langerhans-secretes primarily insulin and glucagon. The darkish acinar cells encompass a small central lumen and have apical zymogen granules. Their apical cytoplasm seems granular and intensely eosinophilic; their bases stain darker. Each oval- to flask-shaped acinus consists of 1 layer of cuboidal to pyramidal cells around a central lumen. Each single, spheroid nucleus sits toward the basal part of the cell in the area with essentially the most intense cytoplasmic basophilia. Apical parts of cells are filled with distinguished secretory (zymogen) granules that stain intensely with eosin or acid dyes. Acinar cells synthesize and secrete a number of digestive enzymes or their inactive precursors, including trypsin, chymotrypsin, amylase, lipase, and carboxypeptidase. A distinctive characteristic of acini is the presence of preliminary parts of the excretory duct system, composed of centroacinar cells, which partially protrude into the acinar lumen. Centroacinar cells lead into intercalated ducts lined by simple cuboidal epithelium. Pancreatic acinar cells are normally protected against dangerous results of digestive enzymes that they secrete. However, acinar cell injury or pancreatic duct obstruction might result in inappropriate extracellular leakage of activated digestive enzymes and autodigestion of pancreatic acini. Edema and progressive fibrosis of the stroma might ensue and trigger hemorrhage and finally pancreatic insufficiency. Liver, Gallbladder, and Exocrine Pancreas Schematic section of a pancreatic acinus. Several profiles of centroacinar cells present intercellular junctions (circles) close to the luminal border. Acinar cells are polarized secretory cells with all the organelles involved in protein synthesis for export.
Astelin 10 ml for sale
The larger precursor peptide is cleaved posttranslationally to active neuropeptides allergy medicine 6 year old order astelin 10 ml without prescription, that are packaged in synaptic vesicles and transported anterogradely by the method of axoplasmic transport allergy symptoms jaw pain astelin 10 ml cheap free shipping. These vesicles are saved in the nerve terminals until released by applicable excitation-secretion coupling induced by an motion potential. Tyrosine and tryptophan compete with other amino acids-phenylalanine, leucine, isoleucine, and valine-for uptake into the brain by way of a common carrier mechanism. When a good protein source is out there in the diet, tyrosine is current in abundance, and sturdy catecholamine synthesis happens; when a diet lacks adequate protein, tryptophan is competitively ample compared with tyrosine, and serotonin synthesis is favored. This is one mechanism by which the composition of the food plan can influence the synthesis of serotonin versus catecholamine and affect temper and affective conduct. Thus, dietary content and steadiness are important to both proper brain development and ongoing affective conduct. Serotonin is synthesized from the dietary amino acid tryptophan, taken up competitively into the brain by a service system. Following release, serotonin can bind to receptors on the postsynaptic membrane, altering postsynaptic excitability, second messenger activation, or both. A swelling of the mind or the presence of mass lesions can selectively exert pressure within an individual fossa. The perforated cribriform plate permits the olfactory nerves to penetrate into the olfactory bulb, a site the place head trauma can result in the tearing of the penetrating olfactory nerve fibers. Pressure, traction, and lots more and plenty can harm structures traversing these small areas that snugly confine the constructions. However, with the presence of a tumor at a foramen, the passing structures could be compressed or broken. For instance, a tumor on the inner acoustic meatus can outcome in ipsilateral facial and vestibuloacoustic nerve damage, and a tumor on the jugular foramen can result in damage to the glossopharyngeal, vagus, and spinal accent nerves. The backbone, consisting of vertebrae and their intervertebral disks, supplies bony safety for the spinal wire. The backbone and skull articulate at the foramen magnum, where the C1 vertebral body (the atlas) abuts the occipital bone. SkullandMeninges 49 Arachnoid granulation Venous lacuna Skin Galea aponeurotica Epicranium Calvaria Dura mater (outer and inner layers) Subdural area (potential) Arachnoid Subarachnoid space Pia mater Cerebral hemisphere Superior sagittal sinus Epidural space (potential) Arachnoid granulation Arachnoid granulation indenting skull (foveola) Venous lacuna Inner layer of dura mater Falx cerebri Pia mater Dura mater (outer layer) Dura mater (inner layer) Arachnoid Subarachnoid house Inferior sagittal sinus Middle meningeal artery and vein 2. The innermost membrane, the pia mater, adheres to each contour of neural tissue, including sulci, folia, and different infoldings. It adheres tightly to glial endfoot processes of astrocytes; this association is identified as the pial-glial membrane. The arachnoid mater, a fine, lacy membrane external to the pia, extends across the neural sulci and foldings. The house between these two membranes is the subarachnoid house, an area into which the cerebrospinal fluid flows, providing buoyancy and protection for the mind. Arteries and veins run via the subarachnoid space to and from the central nervous system. The rupture of an arterial aneurysm in a cerebral artery leads to a subarachnoid hemorrhage. The dura mater, normally adherent to the internal arachnoid, is a tricky protective outer membrane. It splits into two layers in some places to provide channels, the venous sinuses, for return flow of the venous blood. The arachnoid granulations, one-way valves, extend from the subarachnoid space into the venous sinuses, particularly the superior sagittal sinus, allowing cerebrospinal fluid to drain into the venous blood and return to the center. As they enter the sinus, these bridging veins are topic to tearing in instances of head trauma. Such tearing permits venous blood to accumulate in the subdural house because it dissects the inner dura from the arachnoid. This course of may be gradual (chronic subdural hematoma) in older people or could also be abrupt (acute subdural hematoma) with extreme head trauma. A subdural hematoma, particularly when it happens acutely, could additionally be life-threatening as the outcomes of increased intracranial strain caused by accompanying edema and by the accumulation of the blood within the hematoma itself. A skull fracture could tear a branch of the middle meningeal artery, allowing arterial blood to dissect the dura from the cranium, resulting in an epidural hematoma. Blood from the tear dissects the outer layer of the dura from the cranium, forming a space-occupying mass in what was normally solely a potential space. The hematoma may compress adjacent brain tissue, producing localized indicators, and can also trigger herniation of distant brain areas across the free edge of the tentorium cerebelli (a transtentorial herniation) or across the falx cerebri (a subfalcial herniation). Such herniation could produce modifications in consciousness, breathing, and blood pressure, and altered motor, pupillary, and other neurological signs. Severe head trauma in an grownup might tear bridging veins that lead from the brain via the subarachnoid house and into the dural sinuses, particularly the superior sagittal sinus. The subsequent venous bleeding dissects the arachnoid membrane from the internal layer of the dura, and the blood accumulates as a subdural hematoma. Some of the proteins and different solutes within the hematoma appeal to edema, adding fluid accumulation to the hematoma and additional exacerbating the space-occupying nature of the bleed. A subdural hematoma also could additionally be related to bleeding directly into the brain, an intracerebral hematoma. Major dependable landmarks separate the forebrain into lobes; the lateral (sylvian) fissure separates the temporal lobe under from the parietal and frontal lobes above, and the central sulcus separates the parietal and frontal lobes from one another. Several of the named gyri are related to specific practical activities, such as the precentral gyrus (motor cortex) and the postcentral gyrus (primary sensory cortex). Some gyri, such because the superior, center, and inferior frontal and temporal gyri, function anatomical landmarks of the cerebral cortex. The insula, the fifth lobe of the cerebral cortex, is deep to the outer cortex and may be seen by opening the lateral fissure. For example, the inferior frontal gyrus on the left contains the neuronal machinery for expressive language capabilities; the occipital pole, notably alongside the higher and decrease banks of the calcarine fissure, are specialised for visible processing from the retino-geniculo-calcarine system. Some very discrete lesions in additional processing sites corresponding to vision-related regions of the temporal lobe may end up in specific deficits, such as agnosia for the recognition of faces or the shortcoming to distinguish animate objects. This data supplies some clues about how feature extraction in sensory methods might be achieved in neuronal networks. Part of the auditory cortex is visible at the inferior fringe of the lateral fissure (the transverse temporal gyrus of Heschl). Damage to these cortical areas ends in lack of specific useful capabilities. Thus, info from the contralateral hand and arm are localized laterally, the physique is represented more medially, and the lower extremity is represented alongside the midline and over the sting into the paracentral lobule. The face and head are represented in far lateral regions of these gyri, just above the lateral fissure.
Astelin 10 ml buy generic line
They release potent inflammatory mediators corresponding to histamine allergy medicine homeopathic astelin 10 ml buy online, the anticoagulant heparin allergy medicine kids generic 10 ml astelin with visa, chemotactic elements, cytokines, and metabolites of arachidonic acid that act on vasculature, clean muscle, connective tissue, mucous glands, and inflammatory cells. Histamine, a potent vasodilator and proteolytic enzyme, can destroy tissue or cleave complement components. Histamine release from mast cells will increase permeability of capillaries and venules and results in native edema and emigration of leukocytes and monocytes from circulation. They stimulate native cell proliferation, which outcomes in production of connective tissue components involved in restore of broken tissues. Chemotactic elements are necessary regulators of eosinophil and neutrophil perform. Granules are metachromatic when stained with cationic dyes such as toluidine blue as a outcome of they contain sulfated glycosaminoglycans. Mast cell membranes comprise IgE receptors, and when the receptor-bound IgE is uncovered to antigen, mast cells release contents of their granules-histamine and different saved molecules. Histamine dilates small blood vessels and increases their permeability in order that plasma leaks out; the pores and skin appears red and edematous. The wheals of urticaria, referred to as hives, are brought on by launch of histamine from mast cells. These cells also activate a pathway resulting in release of prostaglandin, leukotriene, and platelet-activating issue. It has many granules in its cytoplasm and is near a venule, which is crammed with erythrocytes. This part is on the stage of the cell nucleus, which is euchromatic with peripheral patches of heterochromatin and a prominent nucleolus (*) at its center. An irregular cell border with filopodia (arrows) is a particular function of the cell floor. The cytoplasm exhibits the granules (Gr) that fluctuate in measurement, shape, and electron density. Many granules in the cytoplasm often obscure the small, round to elongated nucleus. The cell has an irregular outline with many small floor projections, or filopodia, that stretch into surrounding connective tissue and more than likely increase surface space. The Golgi advanced performs a task in synthesis and sulfation of glycosaminoglycans similar to heparin which are packaged and stored in the granules. Degranulation of the granules is in maintaining with release of their contents into the extracellular house. He named them Mastzellen, meaning well-fed cells, because the granules led him to the mistaken perception that the cells nourish surrounding tissues. Ehrlich obtained his doctorate of drugs with a dissertation on the speculation and follow of staining tissues for histology; he confirmed how totally different dyes acted on cells. A pioneer for future work in hematology, immunology, and bacteriology, he won the Nobel Prize in Physiology or Medicine in 1908. Collections of those cells are seen in connective tissue between mucous gland acini. Its basophilic cytoplasm shows a juxtanuclear halo similar to the Golgi advanced. Lymphocytes that enter connective tissue from the circulation differentiate into plasma cells when activated. Plasma cells are free cells of the connective tissues, able to transfer slowly via them. Most are distributed widely throughout the physique, especially within the lamina propria of the gastrointestinal tract and in lymphatic organs. Their cytoplasm is deeply basophilic, the colour relying on the stain and ribosomal content material of the cell. A clear space close to the eccentric, spherical nucleus is a juxtanuclear halo (negative Golgi image), which corresponds to the Golgi complicated. The nuclear chromatin is mostly condensed and heterochromatic, alternating with gentle areas, to give a spoke-wheel or clock-face look. Increased numbers of plasma cells are seen in many hematologic issues similar to plasma cell leukemia. In this disorder, abnormal plasma cells-myeloma cells-accumulate in bone marrow and type a quantity of tumors, largely in bones. As the number of such cells will increase, other hematopoietic stem cells in the bone marrow are compromised. Improved prognosis is because of novel remedy modalities such as pulse corticosteroids, thalidomide, and allogeneic stem cell transplantation, in addition to chemotherapy. The small juxtanuclear Golgi complicated consists of flattened sacs and a few related vesicles. A single cell usually releases one class of immunoglobulin molecules, specific for one epitope of an antibody, known as a monoclonal antibody. Unlike most other protein-secreting cells within the body, plasma cells lack massive secretory granules, which reflects steady supply and discharge of secretory product at the cell floor. The nucleus reveals peripheral clumps of heterochromatin intermixed with prevailing euchromatin in a clock-face sample. One hour after a rat was injected with India ink, the liver was removed and processed for standard histology. Macrophages within the liver, called Kupffer cells, ingested carbon particles within the ink, in order that the pleomorphic cells appear black. After emigration from circulation across blood vessel wall, a monocyte turns into a macrophage, which is attracted to a wound area or inflammatory website by chemotaxis. Antibody receptors on a macrophage cell membrane bind antibody-coated international material. At the tip of phagocytosis, the cell shows few primary lysosomes and contains many dense residual our bodies, or tertiary lysosomes. Primary lysosomes of a phagocytic cell fuse with the vacuole and extrude enzymes into the resulting digestive vacuole. They belong to a family of monocyte-derived cells with broad distribution within the body: Kupffer cells in liver, alveolar mud cells of lung, microglia in brain, Langerhans cells in epidermis, dendritic cells in lymphatic tissue, and osteoclasts of bone. These avidly phagocytic cells have a extra variable look and shorter cytoplasmic processes than fibroblasts. They could additionally be mounted cells connected to connective tissue fibers of the matrix or wandering cells which are motile and migratory. Some macrophages derive from differentiating mesenchymal cells inside connective tissue, but most originate from hematopoietic stem cells in bone marrow that circulate as monocytes and migrate throughout blood vessel walls to enter connective tissues. In addition to engulfing and digesting particulate matter, infectious microorganisms such as bacteria, and damaged cells, macrophages synthesize and secrete varied biologically energetic molecules. Cytokines, development elements, and complement proteins produced by these cells exert profound effects on other cells. Macrophages are attracted to sites of inflammation and are involved within the immune response by antigen processing and presentation. Acute irritation has fast onset and short length (hours to days) with vasodilation, vascular leakage, edema, and emigration of leukocytes.
Astelin 10 ml discount online
Direct somatosensory inputs additionally assist to mediate sexual responses and oxytocin release for milk letdown from suckling allergy treatment for cats astelin 10 ml buy visa. This spinoreticular processed information ultimately reaches the nonspecific thalamic nuclei (such as the centromedian) and is conveyed to limbic structures for more subjective allergy testing overland park ks buy generic astelin 10 ml on line, interpretative features of pain and to the hypothalamus for appropriate visceral autonomic and hormonal responses to ache. This process is evoked in a simple fashion by light rubbing on or adjacent to an injured a half of the physique. These pathways consist of main sensory axons conveying nice, discriminative touch sensation, vibratory sensation, and joint-position sense (the epicritic sensations) toward the primary synapse in the secondary sensory nuclei gracilis and cuneatus in the caudal medulla. Unmyelinated main afferents (C fibers) also terminate on neurons within the dorsal horn, from which a cascading system involving recruitment, convergence, and polysynaptic interconnections originates. This system contributes to perception of excruciating ache and its emotional connotation through cortical areas such as the cingulate, insular, and prefrontal cortices. Sprouting of sympathetic postganglionic nerve fibers on 1� afferent endings and 1� sensory cell bodies pathways 2. Lowered threshold for firing of C fibers (hyperesthesia) and A delta fibers (allodynia) 3. Proliferation of alpha -adrenergic receptors on 1� sensory afferent endings and 1� sensory cell bodies 7 4. Inadequacy of central descending serotonin, norepinephrine, opioid 8 10 9 peptide pathways to management nociception eight. Immobilization by ache decreases gating of nociceptive input, limiting 5 physical remedy to initiate gating 9. Connections from the sympathetic nervous system can innervate terminals and cell our bodies of primary nociceptive neurons instantly. Descending central noradrenergic and serotonergic projections are thought to play an essential modulatory role in the processing of neuropathic and nonneuropathic ache. It is said to the kind of persistent, agonizing central ache skilled in phantom limb syndrome. Intense burning or stabbing pain is felt, with allodynia and hyperesthesia (extreme sensitivity to touch and painful stimuli, respectively). Treatment must occur quickly after detection and must make use of simultaneous vigorous therapeutic approaches. Treatment decisions usually embody analgesics, tricyclic or other antidepressants to alter pain threshold in the spinal wire, membrane-stabilizing brokers. These areas embody areas of cerebral cortex, limbic forebrain areas, hypothalamic areas together with endorphin nuclei, and sensory cortical centrifugal connections. Enkephalin and dynorphin interneurons are found in pain-processing areas, particularly within the dorsal horn of the spinal cord and the descending nucleus of V, and in many hypothalamic and limbic sites which could be concerned in the subjective interpretation of ache. The beta-endorphin neurons of the periarcuate area of the hypothalamus ship connections to the periaqueductal grey, locus coeruleus and brain stem noradrenergic nuclei, the raphe nuclei, and tons of limbic areas. The periaqueductal gray is particularly important for opioid activation of the nucleus raphe magnus and other descending monoamine pathways that activate enkephalins and assist in opiate analgesia. The periaqueductal gray�raphe connection is important for full performance of opioid analgesia. Systemic administration of synthetic opiates prompts neurons of the periarcuate region of the hypothalamus and periaqueductal grey, leading to analgesia. Although most of the trigeminal system is represented on the lateral portion of the contralateral major sensory cortex (postcentral gyrus), a part of the epicritic trigeminal projections as properly as style are represented within the ipsilateral sensory cortex. These neurons refer pain from intracranial structures to forehead, scalp, or retrobulbar sites. Ophthalmic (V1) nerve Central pain pathway Spinal nucleus of trigeminal (V) nerve Spinal ganglia C1�3 Dura of posterior fossa Posterior head Afferent nerves from occipital area, ear, and neck and from dura of posterior fossa and vertebrobasilar arteries are carried by dorsal roots of C1�3 spinal ganglia, accounting for ache referral to these sites Vertebrobasilar arteries 14. Primary headaches can come up as migraine headaches, tension headaches, and neuralgias. Taste bud Epithelium Basement membrane Microvilli Taste pore Taste cells Nerve plexus Nerve fibers rising from taste buds Large nerve fiber Intercellular area Microvilli Fibroblast Small nerve fiber Large nerve fiber Desmosomes Granules Epithelium Collagen Schwann cell Basement membrane D. They translate individual molecular configurations or mixtures of molecules for salty, sweet, sour, and bitter sensations into action potentials of both massive and small main sensory axons. The taste buds are found on the anterior and posterior areas of the tongue and, much less frequently, on the palate and epiglottis, mainly in children. Nerve fibers for style present complicated responses of electrical exercise across populations of many nerve fibers. These nonthalamic projections are related to the emotional, motivational, and behavioral elements of style and meals intake. The style buds detect candy, salty, bitter, and sour tastes; each style bud seems to be related primarily with one such modality. Combined taste receptor activation can code for a tremendous array of subtle tastes and flavors. Olfaction performs a major function in the discrimination of what a person perceives to be taste. Some cortical areas, such as the anterior portion of the insular cortex and a lateral zone of the posterior orbitofrontal cortex, are concerned in subjective features of taste and the gustatory experience. Many sicknesses, together with severe nasal congestion, liver dysfunction, autonomic issues, postradiation responses, some vitamin deficiencies, and a few drugs, could distort or alter the tastes of foods or could depart a lingering, disagreeable, distinctive style. Many chemotherapeutic agents additionally profoundly alter style sensation, maybe accounting partly for loss of appetite in such people. This fluid wave causes differential motion of the basilar membrane, stimulating hairs on the apical portion of hair cells to launch neurotransmitters that stimulate primary sensory axons of neurons of the cochlear (spiral) ganglion. The basilar membrane in the cochlea shows maximal displacement spatially according to the frequency of impinging tones, with low frequencies maximally stimulating the apex (helicotrema) and excessive frequencies maximally stimulating the base. The eustachian (pharyngotympanic) tube permits stress equilibrium between the middle ear and the outside world. The most devastating for human communication is a loss within the frequencies of speech (300 to 3000 Hz) of 40 or extra decibels. In basic, hearing loss can be subdivided into two categories: sensorineural and conductive. Sensorineural hearing loss includes damage to the hair cells, the auditory nerve, or central auditory pathways. Because of the neural injury, each air conduction and bone conduction are diminished. These two forms of hearing loss could be tested for on the bedside through the use of a tuning fork of 512 Hz. The Weber check involves placing the vibrating tuning fork on the center of the brow. With sensorineural loss, the sound is heard finest in the unaffected ear; with conductive loss, the sound is heard finest in the affected ear. The Rinne check involves holding the vibrating tuning fork in opposition to the mastoid bone. Normally, air conduction is simpler than bone conduction, and the fork will again be heard when moved adjoining to the exterior auditory meatus (air conducting sound higher than bone). If sensorineural hearing loss is present, air conduction may be greater than bone conduction, though both could also be diminished.