
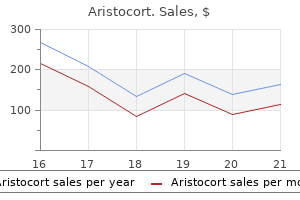
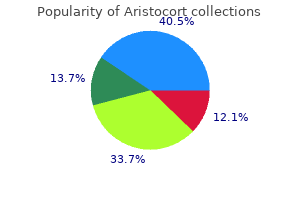
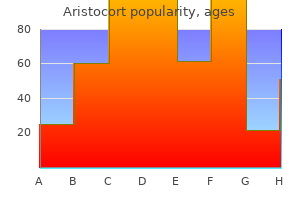
Aristocort dosages: 40 mg, 15 mg, 10 mg, 4 mg
Aristocort packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Aristocort 10 mg purchase overnight delivery
This histological sample may occur either alone or as an acute exacerbation of pre-existing interstitial lung disease allergy shampoo for dogs aristocort 10 mg buy online. Obliterative bronchiolitis sample (constrictive bronchiolitis) in rheumatoid arthritis Obliterative bronchiolitis (constrictive bronchiolitis) is a rare complication of rheumatoid arthritis allergy symptoms skin rash cheap aristocort 10 mg with visa. Clinical symptoms are nonspecific, consisting of cough, dyspnea and irreversible airflow obstruction, which progresses rapidly over weeks to months. In some cases biopsies might present only some affected bronchioles and the modifications may be inconspicuous, even in patients with marked symptomatology. Normally, the lumen must be roughly equal or only barely smaller than the accompanying pulmonary artery. The bronchiolar epithelium ought to usually be juxtaposed to the bronchiolar smooth muscle. It most commonly occurs as a sequel of persistent rejection in lung transplant patients (see Chapter 20). Treatment with corticosteroids or immunosuppressants, similar to cyclophosphamide, might profit occasional sufferers. It can additionally be a secondary discovering in patients with bronchiectasis, continual bronchitis, bronchial asthma, continual infections or cystic fibrosis. Lymphoid follicles may also have a lymphangitic distribution, alongside the interlobular septa and beneath the pleura, a sample sometimes referred to as lymphoid hyperplasia. Reactive lymphoid follicles with secondary germinal centers cluster around a terminal bronchiole. Lymphoid hyperplasia features comparable findings together with the extra presence of lymphoid follicles along the septa and pleura in a lymphangitic distribution. A continual inflammatory infiltrate permeates the wall and mucosa of this bronchiole. Small sequence and case stories with restricted pathology descriptions of pulmonary hypertension and plexogenic arteriopathy have been reported (see Chapter 18). The associated pulmonary artery should usually be of comparable measurement but is far smaller. Diffuse alveolar hemorrhage/capillaritis in rheumatoid arthritis Diffuse alveolar hemorrhage is rare but might occur as a pulmonary manifestation of rheumatoid arthritis. There is fibrinoid necrosis of the vessel wall with marked intimal edema and a blended mural and subintimal inflammatory infiltrate. Amorphous eosinophilic deposits of amyloid are diffusely current inside the wall of this small pulmonary artery. The interpretation of amyloid is confirmed by applegreen birefringence beneath polarized mild after staining for Congo pink (inset). Eosinophilic pneumonia might not often be related to rheumatoid arthritis, generally as a presenting manifestation. Typical features of eosinophilic pneumonia are present on this part with aggregates of eosinophils and histiocytes inside alveolar areas. This endobronchial biopsy reveals diffuse permeation of the endobronchial wall by massive B-lymphocytes. Other rare pulmonary manifestations of rheumatoid arthritis Other rare pulmonary manifestations of rheumatoid arthritis are reported. This histological pattern is commonly found in sufferers with acute lupus pneumonitis. Patients develop the acute onset of cough, dyspnea, fever and infrequently hemoptysis. Pleural biopsies or autopsy research typically present a thickened visceral pleura with fibrosis and chronic inflammation, consisting of lymphocytes, histiocytes and plasma cells. Patients may also develop pulmonary capillaritis and thromboemboli, as manifestations of the antiphospholipid syndrome, or pulmonary hypertension as a chronic sequel. There is diffuse alveolar hemorrhage together with intra-alveolar aggregates of hemosiderin-laden macrophages. More current studies present an growing frequency of related capillaritis in such circumstances, approaching 80%. The distinction in frequency might stem from sampling issues, larger awareness of capillaritis or revised histological standards for the recognition of extra subtle options of capillaritis. Sometimes the degree of irritation is so intense that it spills over into the adjacent alveoli. A blended inflammatory infiltrate permeates the wall of this small pulmonary artery. This risk can normally be assessed with applicable serological exams (see below). Immune complexes can be demonstrated by immunofluorescence and ultrastructural studies in many (50 to 75%), however not all, circumstances. Granular deposits of IgG may be identified within alveolar septa on immunofluorescence usually accompanied by C1q, C3 and fewer typically by other immunoreactants, together with IgM and IgA. Ultrastructurally, electron-dense deposits are current in alveolar partitions: most frequently inside the basement membrane however sometimes in a subendothelial or subepithelial location. This alveolar wall damage and the resulting bland alveolar hemorrhage might be thought-about analogous to the microangiopathy seen in lupus nephritis. Echocardiography may be helpful in detecting pulmonary hypertension, though cardiac catheterization is critical for definitive prognosis. Histologically, most cases of pulmonary hypertension present plexogenic arteriopathy with involvement of small pulmonary arteries by concentric laminar intimal fibrosis, medial hypertrophy and plexiform lesions. Antiphospholipid antibodies, anti-endothelial cell antibodies, vasculitis and vasospasm are implicated. Interstitial lung disease happens in about 1% of sufferers at prognosis, 4% within 1 yr of diagnosis and 8% after 12 years. The gradual appearance of those symptoms is in contrast to acute lupus pneumonitis, which has a extra abrupt onset. Interstitial lung illness appears to arise in two distinct scientific settings: (1) as a long-term sequel of acute lupus pneumonitis or (2) insidiously over time, without an apparent precipitating cause. Pulmonary thromboembolic disease in a affected person with pulmonary hypertension and lupus anticoagulant. Data are restricted and based mostly on isolated case reports and small retrospective collection. Recurrent miscarriages, thrombocytopenia, livedo reticularis and neurological signs are different features of this disorder. Targeted plasma proteins include apolipoprotein H (formerly termed b2-glycoprotein I), which binds cardiolipin, and prothrombin, which binds phosphatidyl serine. At post-mortem the patient additionally had multiple mind infarcts and a renal thrombotic microangiopathy. Multiorgan involvement is most distinguished in the diffuse variant, with vascular and connective tissue fibrosis affecting the skin, gastrointestinal tract, lungs and kidneys. Regardless of the form of illness, pulmonary involvement is a number one explanation for morbidity and mortality. The major type of pulmonary hypertension (12:16% of patients) is related extra incessantly with the restricted, quite than diffuse, variant of scleroderma. In the presence of such inhibition, in distinction to deficiencies of particular components, clotting time fails to appropriate upon mixing with regular pooled plasma.
Aristocort 10 mg proven
The complicated fibrovascular cores are sometimes fibrotic with lymphoplasmacytic infiltrates allergy testing edmonds wa 10 mg aristocort effective. Nuclei are giant with vesicular chromatin and no less than focally prominent nucleoli allergy relief for dogs generic 15 mg aristocort amex. The invasive carcinoma is normally acinar sample, but the other main subtypes could be seen. This pattern lacks fibrovascular cores but stromal and vascular invasion are widespread. This morphology might comprise a far larger share of tumor metastasis as compared with its percentage in the main lung carcinoma. No well-established histological or cytological grading system exists for lung adenocarcinomas. Others imagine a system combining explicit histological findings, corresponding to vascular invasion, with architectural patterns or pure nuclear criteria predict outcomes. Intracellular mucin may be identified on routine sections but mucin stains could also be required to doc the presence of no much less than 5 tumor cells with mucin in two high-power (40�) fields. Single cells usually resemble alveolar macrophages, which are often quite a few in these samples. Nuclei are uniformly spherical to oval whereas barely irregular nuclear contours could also be seen. Three-dimensional papillary fronds or syncytial preparations can also be observed. A spectrum of nuclear and cytoplasmic options is noted as cells in a single sample may resemble macrophages in a single subject however pleomorphic carcinoma in another. Basophilic cytoplasm may be finely or coarsely vacuolated and nuclei are often eccentric and may be indented by the mucin vacuoles. The cytological differential diagnosis includes chemotherapy and radiation remedy effects, viral pneumonia, infarct and metastatic adenocarcinoma. On account of chemotherapeutic considerations, discerning pulmonary adenocarcinoma from squamous cell carcinoma is now crucial. This sheet of tumor cells contains a single enlarged cell with an intranuclear pseudoinclusion. A threedimensional acinar group as properly as a separate cluster of tumor cells is seen in opposition to the neutrophil-rich background. Squamous cell carcinomas characteristic infected and necrotic backgrounds, welldefined cell borders, thick orange to yellow cytoplasm and sometimes pyknotic nuclei with rare nucleoli. Whenever possible, cytology must be evaluated at the aspect of any biopsy material. Immunohistochemistry is useful in distinguishing adeno- from squamous cell carcinoma whereas mutational analysis of each localized and superior lung carcinomas might influence the selection of chemotherapy routine. Since explicit therapeutic brokers are sub-type dependent, every effort should be made to accurately diagnose these lesions beyond the final class of non-small-cell carcinoma (see beneath; Treatment). Following such an algorithm allows one to subtype at least 80% of small biopsy samples lacking apparent morphological differentiation. When mixed with cytology, some investigators declare over 95% of small samples can be accurately subtyped. The former are electron-dense, with osmiophilic whorls resembling surfactant granules. The latter are normally connected to the nuclear membrane and are immunohistochemically constructive for surfactant protein. Discovery of particular mutations and translocations has allowed for enhancements in classification, insights into pathogenesis and, most notably, growth of agents that focus on activated molecular pathways (Table 6). Most of the kinase activating/medication sensitizing mutations are in exon 19 and exon 21. There is some extent mutation at base 858 leading to an amino switch from leucine (L) to arginine (R) or L858R. There are multiple variations of the exon 19 deletion, and some less common exon 18 mutations have additionally been recognized. Occasional salivary gland main carcinomas and some thyroid carcinomas (overall < 5%) are the most common exceptions, however still at a low rate. These mutations (most widespread is threonine to methionine, T790M) are seen in about 50% of treated patients. Asian collection report a low price (about 10%),236,256 whereas Western sequence a comparatively higher price (25%). The rearrangement could be detected by fluorescence in situ hybridization, using break-apart probes. The translocation has been recognized in each Asian267,268 and Western269 populations, and is seen in about 5% of lung adenocarcinomas. Other epidemiological issues embrace a mean younger age and a lighter smoking historical past. It has been suggested that solid, signet ring and cribriform histologies are associated with this translocation. So far, it has not been seen in squamous, small cell, massive cell, adenosquamous or pleomorphic carcinomas. Mutations are most commonly V600E (90%), but other mutations have been recognized. Copy quantity alterations Copy quantity alterations (amplifications and deletions) have been recognized in lung adenocarcinoma. Amplified loci or activating mutations can characterize mechanisms of oncogenic pathway activation. Tissue levels, elastic stains and even cytokeratin immunohistochemical stains can be utilized in order to attain a assured diagnosis. While separating synchronous lung primaries from intrapulmonary metastases is fraught with uncertainty, this algorithm seems helpful. Clinical history and radiological correlations are essential for each small and typically incidental lesions as well as bigger masses. Reactive bronchiolar and pneumocyte atypia commonly mimic each lepidic and invasive adenocarcinoma. Proliferative epithelium associated with acute and organizing pneumonia, chemotherapy or radiation therapy, or persistent fibrosing interstitial pneumonia may be hyperplastic with increased nuclear/ cytoplasmic ratios and prominent nucleoli. However, these areas are more diffuse than one sees in lepidic most cancers and cellular monotony is often lacking. Ciliated, mucinous and metaplastic squamous cells are hardly ever identified in adenocarcinomas. Recall that pulmonary nodules with architectural and morphological options of malignancy in most cancers patients treated with chemotherapy are adenocarcinomas and never pseudoneoplastic nodules. Adenocarcinoma also demonstrates extra cytological atypia with coarser nuclear chromatin and outstanding nucleoli. Atypical adenomatous hyperplasia hardly ever has more than one of these features (Table 7).
Effective 10 mg aristocort
An immune basis for lung parenchymal destruction in chronic obstructive pulmonary disease and emphysema allergy symptoms 8 months discount aristocort 4 mg online. Anti-tissue antibodies are associated to lung perform in continual obstructive pulmonary disease allergy medicine 16 month old aristocort 10 mg best. Lymphocyte population and apoptosis within the lungs of people who smoke and their relation to emphysema. Pulmonary hypertension in patients with chronic obstructive pulmonary illness: latest advances in pathophysiology and management. Update on pulmonary hypertension complicating chronic obstructive pulmonary disease. Severe pulmonary hypertension 654 Chapter 17: Chronic obstructive pulmonary disease and diseases of the airways and continual obstructive pulmonary illness. Morphologic adjustments within the muscular pulmonary arteries: relationship to cigarette smoking, airway illness, and emphysema. Pulmonary vascular construction and function in persistent obstructive pulmonary disease. The construction and performance of the pulmonary vasculature in mild chronic obstructive pulmonary disease. Effects of pulmonary artery remodeling on pulmonary circulation after lung volume reduction surgical procedure. Pulmonary artery reworking modifies pulmonary hypertension throughout train in extreme emphysema. Pathophysiology of cor pulmonale in continual obstructive pulmonary disease: part two. The relationship between small pulmonary vascular alteration and aortic atherosclerosis in chronic obstructive pulmonary illness. Left ventricular dysfunction and related cellular harm in rats uncovered to chronic intermittent hypoxia. Treatment of acute persistent obstructive pulmonary illness exacerbation improves right ventricle operate. A linkage disequilibrium between genes at the serine protease inhibitor gene cluster on chromosome 14q32. The prevalence of osteoporosis in patients with continual obstructive pulmonary illness: a cross sectional examine. Leptin, visfatin, insulin resistance, and physique composition change in persistent obstructive pulmonary illness. Genome-wide affiliation evaluation of body mass in continual obstructive pulmonary disease. Systemic inflammation and skeletal muscle dysfunction in chronic obstructive pulmonary illness: state-of-the-art and novel insights in regulation of muscle plasticity. Inflammation, oxidative stress and systemic effects in delicate continual obstructive pulmonary illness. The results of hypoxia on markers of coagulation and systemic irritation 655 Chapter 17: Chronic obstructive pulmonary illness and ailments of the airways in patients with chronic obstructive pulmonary disease. Effects of acute hypoxia on left and proper ventricular contractility in chronic obstructive pulmonary illness. Dysmorphic lungs in a case of leprechaumism: case report and review of literature. Morphogenesis of irregular elastic fibers in lungs of patients with panacinar and centriacinar emphysema. Risk of renal and colonic neoplasms and spontaneous pneumothorax in the Birt-Hogg-Dube syndrome. Nonsense mutations in folliculin presenting as isolated familial spontaneous pneumothorax in adults. Mutations of the Birt Hogg Dube gene in patients with multiple lung cysts and recurrent pneumothorax. Lung cysts, spontaneous pneumothorax, and genetic associations in 89 households with BirtHogg-Dube syndrome. Lung cysts in Birt-Hogg-Dube syndrome: histopathological traits and aberrant sequence repeats. Swyer-James (MacLeod) syndrome with placental transmogrification of the lung: a case report and evaluation of the literature. Placental transmogrification of the lung, a histologic variant of big bullous emphysema. Suppurative illnesses of the lung and pleura: a seamless challenge in 656 Chapter 17: Chronic obstructive pulmonary disease and diseases of the airways developing international locations. The cartilage of the intrapulmonary bronchi in regular lungs in bronchiectasis and in massive collapse. The aetiology of bronchiectasis (with particular reference to pulmonary atelectasis). Factors associated with lung function decline in adult patients with secure non-cystic fibrosis bronchiectasis. Resection of the right middle lobe and lingula in kids for center lobe/lingula syndrome. Rigid bronchoscopy and surgical resection for broncholithiasis and calcified mediastinal lymph nodes. Diffuse tracheo-bronchial amyloidosis: a rare 657 Chapter 17: Chronic obstructive pulmonary illness and diseases of the airways variant of a protean illness. Bronchiolitis obliterans organising pneumonia in sufferers taking acebutolol or amiodarone. Unilateral hyperlucent lung (Swyer-James syndrome) after extreme Mycoplasma pneumoniae infection. Proliferative exercise in fibrosing lung illnesses: a comparative examine of Ki-67 immunoreactivity in diffuse alveolar injury, bronchiolitis, obliteransorganizing pneumonia, and usual interstitial pneumonia. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: an under-recognised spectrum of illness. Brief report: idiopathic diffuse hyperplasia of pulmonary neuroendocrine cells and airways disease. Neuroendocrine cell hyperplasia and obliterative bronchiolitis in sufferers with peripheral carcinoid tumors. Persistent tachypnea of infancy is associated with neuroendocrine cell hyperplasia. Outbreak of bronchiolitis obliterans related to consumption of Sauropus androgynus in Taiwan. Outbreak of obstructive ventilatory impairment associated with consumption of Sauropus androgynus vegetable. Association of Sauropus androgynus and bronchiolitis obliterans syndrome: a hospital-based casecontrol research. Dose-response relationship and irreversible obstructive ventilatory defect in sufferers with consumption of Sauropus androgynus. Segmental necrosis of small bronchi after prolonged intakes of Sauropus androgynus in Taiwan.
Cheap aristocort 15 mg otc
Merkel cell carcinoma can be distinguished from metastatic small cell carcinoma utilizing antibodies to cytokeratin 20 and thyroid transcription issue 1 allergy symptoms under chin 15 mg aristocort buy free shipping. Metastatic Merkel cell carcinoma with positive expression of thyroid transcription factor-1: a case report allergy testing questions aristocort 4 mg low price. Thyroid transcription factor-1 expression prevalence and its medical implications in non-small cell lung most cancers: a highthroughput tissue microarray and immunohistochemistry research. Prognostic significance of thyroid transcription factor-1 expression in each early-stage typical adenocarcinoma and bronchioloalveolar carcinoma of the lung. Positive thyroid transcription factor 1 staining strongly correlates with survival of patients with adenocarcinoma of the lung. Thyroid transcription issue 1: a new prognostic think about lung cancer: a meta-analysis. Thyroid transcription factor 1 expression in ovarian carcinomas is an unbiased prognostic factor. Thyroid transcription factor-1 and cytokeratins 7 and 20 in pulmonary and breast carcinoma. The worth of thyroid transcription factor-1 in cytologic preparations as a marker for metastatic adenocarcinoma of lung origin. Incidence and significance of cytoplasmic thyroid transcription factor-1 immunoreactivity. Comparison of thyroid transcription factor-1 and hepatocyte antigen immunohistochemical analysis within the differential diagnosis of hepatocellular carcinoma, metastatic adenocarcinoma, renal cell carcinoma, and adrenal cortical carcinoma. Cytoplasmic immunoreactivity for thyroid transcription factor-1 in hepatocellular carcinoma: a comparative immunohistochemical analysis of four business antibodies utilizing a tissue array approach. Thyroid transcription factor 1 immunohistochemistry as an intraoperative diagnostic device at frozen part for distinction between major and secondary lung tumors. The aspartic protease napsin A suppresses tumor development independent of its catalytic activity. Value of thyroid transcription factor-1 and surfactant apoprotein A in the differential prognosis of pulmonary carcinomas: a research of 109 cases. Surfactant proteins and thyroid transcription factor-1 in pulmonary and breast carcinomas. Ultrastructural examine of nuclear inclusions immunohistochemically optimistic for surfactant protein A in pulmonary adenocarcinoma with particular reference to their morphogenesis. Immunohistochemistry in the distinction between malignant mesothelioma and pulmonary adenocarcinoma: a important evaluation of new antibodies. Immunohistochemical localization of pulmonary surfactant apoproteins in numerous lung tumors. Diagnostic value of immunohistochemically detected surfactant: apoprotein-A in malignant tumors located in the lungs: report of two cases. Immunoreactivity for epithelial and neuroendocrine antibodies are useful within the differential prognosis of lung carcinomas. Small cell lung carcinoma: clinicopathological, immunohistochemical, and ultrastructural research. Tissue fixation methods alter the immunohistochemical demonstrability of synaptophysin. Nonsmall cell lung carcinoma with neuroendocrine differentiation: an entity of no medical or prognostic significance. Stepwise progression of pulmonary adenocarcinoma: clinical and molecular implications. Expression of p63 in primary cutaneous adnexal neoplasms and adenocarcinoma metastatic to the skin. Combined small cell lung carcinomas: genotypic and immunophenotypic evaluation of the separate morphologic elements. A novel five-antibody immunohistochemical check for subclassification of lung carcinoma. Primary signet-ring cell carcinoma of lung: immunohistochemical research and comparison with non-pulmonary signet-ring cell carcinomas. Differential expression of cytokeratins 7 and 20 and thyroid transcription factor-1 in bronchioloalveolar carcinoma: an immunohistochemical examine in fineneedle aspiration biopsy specimens. Expression of thyroid transcription factor-1, cytokeratin 7, and cytokeratin 20 in bronchioloalveolar carcinomas: an immunohistochemical analysis of sixty seven circumstances. Usefulness of Cdx2 in separating mucinous bronchioloalveolar adenocarcinoma of the lung from metastatic mucinous colorectal adenocarcinoma. Comparison of the immunophenotypes of signet-ring cell carcinoma, stable adenocarcinoma with mucin manufacturing, and mucinous bronchioloalveolar carcinoma of the lung characterised by the presence of cytoplasmic mucin. Expression of estrogen and progesterone receptors in non-smallcell lung cancer: immunohistochemical research. Use of antibodies towards estrogen and progesterone receptors to determine metastatic breast and ovarian carcinomas by standard immunohistochemical and tyramide signal amplification strategies. Immunohistochemical differentiation of metastatic breast carcinomas from metastatic adenocarcinomas of different common primary sites. Expression of immunohistochemical markers in primary and metastatic malignant melanoma: a comparative examine in 70 patients utilizing a tissue microarray method. Immunoreactivity for thyroid transcription factor-1 in stage I non- small cell carcinomas of the lung. Immunohistochemical staining for thyroid transcription factor-1: a helpful help in discerning main web site of tumor origin in sufferers with brain metastases. The immunohistochemical diagnosis of mesothelioma: a comparative research of epithelioid mesothelioma and lung adenocarcinoma. Utility of thyroid transcription factor-1 and cytokeratin 7 and 20 immunostaining within the identification of origin in malignant effusions. Thyroid transcription factor-1 is extremely delicate and specific in differentiating metastatic pulmonary from extrapulmonary adenocarcinoma in effusion fluid cytology specimens. Determination of lung as the primary web site of cerebral metastatic adenocarcinomas utilizing monoclonal antibody to thyroid transcription factor-1. Utility of surfactant protein B precursor and thyroid transcription factor 1 in differentiating adenocarcinoma of the lung from malignant mesothelioma. Diagnostic utility of thyroid transcription factor-1 expression in adenocarcinomas presenting in serous fluids. Utility of thyroid transcription factor-1 and cytokeratin 20 in identifying the origin of metastatic carcinomas of cervical lymph nodes. Thyroid transcription issue 1: a marker for lung adenoarinoma in physique cavity fluids. Utility of thyroid transcription factor1 expression within the differential diagnosis of metastatic adenocarcinoma of serous effusion specimens ready utilizing the cell switch approach. Utility of tissue-specific transcription factors thyroid transcription factor 1 and Cdx2 in determining the first web site of metastatic adenocarcinomas to the mind. Monoclonal antibody to thyroid transcription factor-1: manufacturing, characterization, and usefulness in tumor analysis. Immunocytochemical expression of tissue particular transcription factor-1 in lung carcinoma. Primary oncocytic adenocarcinomas of the lung: a clinicopathologic, immunohistochemical, and molecular biologic analysis of sixteen instances.
Aristocort 15 mg buy low cost
Cells are giant and variably preserved with marked anisonucleosis allergy medicine during ivf buy cheap aristocort 15 mg on line, noticeable nucleoli and irregular allergy medicine homeopathic 4 mg aristocort buy with amex, coarsely stippled chromatin. In follow, mitoses are often abundant, with sometimes 70:eighty and up to one hundred per 2 mm2. They have copious, finely granular cytoplasm and vesicular nuclei with clumped chromatin and outstanding nucleoli. The basic "oat cell" carcinoma of the older literature accounts for not extra than 25% of circumstances. Crushing and distortion of teams of cells that coalesce and smear, the so-called "crush phenomenon", is attribute. It is a mirrored image of rapid nuclear breakdown and is seen solely hardly ever in other pulmonary tumors. Confluent necrosis is common and apoptotic our bodies and mitoses are quite a few, the latter, frequently numbering as a lot as one hundred per 2 mm2. Compared to the respiratory epithelial cells (arrow), those from the tumor have far much less cytoplasm, bigger nuclei and show pronounced nuclear molding. These advances have greatly increased our capacity to recognize, distinguish and investigate this spectrum of neoplasms and have supplanted earlier, extra capricious histochemical methods of detection. Argentaffinty denotes the ability of a reducing agent, corresponding to amines, to precipitate silver out of a solution of its salts, leading to a granular cytoplasmic precipitate. Neuroendocrine antigens Pulmonary neuroendocrine tumors categorical a variety of immunochemically detectable neuroendocrine antigens, lots of which replicate the useful attributes of synthesis and secretion of amine and peptide hormones. It was one of the earliest antigens used to detect pulmonary neuroendocrine cells and tumors. This antigen might be probably the most delicate for the neuroendocrine phenotype of those presently out there. Expression is restricted to sure subclasses and so they may be troublesome to detect in carcinoids in particular, despite their high degree of differentiation. Prevelance in these tumors varies significantly between studies, probably to some extent as a result of the utilization of totally different antibodies for its detection. Nuclei are common and the chromatin is finely dispersed with peripheral condensation, but clumping is more common. Expression of mutant p53 protein is seen in about one-quarter and loss of the Rb gene product in about one-fifth. These constructions are sometimes scanty and the electron microscopic options of these tumors are extra variable. The extremely organized association of nodular or acinar lesions can mimic neoplasms of similar structure. These embody paraganglioma (see below) and metastases from the thyroid and kidney. Adenoid cystic carcinoma, pulmonary glomus tumor and acinic cell carcinomas could pose diagnostic issues. Occasionally, low-grade sarcomas, corresponding to those differentiating in course of easy muscle or nerve sheath, must be thought of within the differential analysis. The unexpected sharing of antigens between neuroendocrine and non-neuroendocrine tumors is always a diagnostic trap. Atypical carcinoids can histologically mimic an identical vary of primary or metastatic neoplasms, however their lesser diploma of architectural regularity makes confusion extra doubtless. This is as a end result of its morphological recognition is dependent upon its architecture, which may not all the time be apparent in small samples. Such biopsies are often interpreted as "poorly differentiated non-small-cell","massive cell" or "basaloid" carcinoma, the true nature of the tumor changing into obvious solely after its excision. Even in resections, the palisading, trabeculation and rosetting that characterize neuroendocrine differentiation morphologically may be delicate. Even an adequate, well-preserved specimen may not be consultant of the whole lesion. Most issues come up when a analysis is attempted on small, distorted and inadequately fixed tissue biopsies. Immunohistochemical detection of neuroendocrine antigens and people expressed by the diagnostic alternate options are necessary aids in distinguishing these tumors. This distinction could also be inconceivable even after morphological scrutiny and intensive immunochemical evaluation. However, its expression by some poorly differentiated extrapulmonary neuroendocrine tumors renders it of little utility on this setting. They depend upon architectural and cytological assessment of a well-fixed and processed specimen of sufficient measurement. Detection of antigens is of little use in distinguishing these tumors, as a outcome of the variations of their patterns of expression are quantitative rather than qualitative. Mitoses and punctate necrosis are sometimes accompanied by loss of architectural group and a point of pleomorphism, but these are of no diagnostic utility. According to this method, no less than two of these 4 criteria must be current for a carcinoid to be categorized as atypical. Assessing a carcinoid for these options poses little problem with resected specimens, however can be impossible to assess with tissue biopsies. In apply, this requires careful assessment of a range of options, together with architecture, cell dimension, morphology and nuclear traits. The diagnosis of these tumors is often made solely after resection, following an initial biopsy diagnosis of "poorly differentiated" or "giant cell" carcinoma. Large cell neuroendocrine carcinoma is an aggressive neoplasm with a excessive price of thoracic recurrence and extensive dissemination. Most of its cells have conspicuous cytoplasm and some have vesicular nuclei with nucleoli, whereas others are smaller and have nuclei with dispersed chromatin. It is the complete morphological image somewhat one or two particular person criteria that distinguishes these two tumors. Again, this can be tough or impossible to obtain with small tissue biopsies, but a prognosis of "high-grade neuroendocrine carcinoma" ought to be possible in most cases. This is the similar old a part of the tumor to be sampled during biopsy and freezing the tissue for frozen section prognosis additional compromises the morphology. It is necessary to concentrate on the danger of this potentially serious misdiagnosis. Approximately 10% metastasize to regional lymph nodes, however this usually has little affect on survival. A morphologically typical adenocarcinoma with sturdy expression of synaptophysin, most likely probably the most specific marker of neuroendocrine differentiation presently obtainable. Up to one-third of morphologically non-neuroendocrine carcinomas of the lung show immunohistochemical or ultrastructural evidence of such differentiation. A small morule of neuroendocrine cells in a well-differentiated fetal adenocarcinoma.
Androstenetrione. Aristocort.
- Dosing considerations for Androstenetrione.
- How does Androstenetrione work?
- What is Androstenetrione?
- Improving athletic performance and other conditions.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97037
Aristocort 40 mg quality
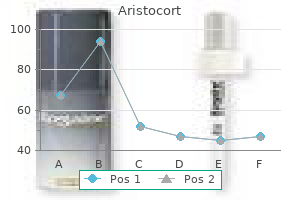
Environmental mycobacterial an infection usually produces radiographic appearances just like allergy shots for asthma aristocort 10 mg free shipping cavitary pulmonary tuberculosis allergy shots im or sq 10 mg aristocort with visa. This asymptomatic affected person from a high-prevalence country had full radiographic decision after anti-tuberculous treatment. Larger droplets influence within the airways and are removed by the mucociliary escalator, usually to be swallowed and destroyed within the gastrointestinal tract. From this point onwards mycobacteria have mechanisms that subvert the traditional host response, which results in bacterial multiplication. Once ingested, the bacteria-containing phagosome is immunologically activated by interferon-g, leading to fusion with a lysosome. Such exposes the organism to a low pH and antibacterial substances (principally reactive oxygen and nitrogen molecules). It can also be in a position to detoxify these host-produced reactive oxygen and nitrogen molecules and to repair the injury attributable to these molecules. Frontal chest radiograph of a younger adult revealing a large enlargement of the higher mediastinum and proper hilum as a end result of lymphadenopathy. No obvious abnormality aside from the hilar lymphadenopathy was famous within the lung parenchyma. Perhaps most significantly, the ability of the mycobacterium to evade the host immune response and to persist within the macrophage. Ingestion of micro organism into macrophages must be the key step to the demise and elimination of these bacteria. A very giant number of totally different mechanisms have been identified whereby the mycobacterium may do that. Modulation of antigen processing is one factor within the arrest of phagosome improvement. The inflammatory lesion inside the lung is a dynamic environment containing a selection of protective and regulatory cells. Effector T lymphocytes (purple) mediate management of bacterial progress and the mononuclear composition of the granuloma. Regulatory T lymphocytes (orange) additionally accumulate within the lesion and limit the ability of the acquired response to cease bacterial progress. Infected phagocytes elaborate cytokines and effector molecules that restrict the exercise of the lymphocyte response. B cells (blue) accumulate throughout the lesion within the type of nascent lymphoid follicles; these cells can affect bacterial control and the immunopathologic penalties of an infection. Resistance to reactive nitrogen intermediates could also be mediated through KatG, a catalase-peroxidase, which may inactivate reactive oxygen, but different genes corresponding to ahpC, glbN and msrA have also been implicated in mycobacterial resistance to such reactive molecules. In addition the mycobacterial proteosome could possibly restore proteins damaged by reactive oxygen and nitrogen molecules. Also, mycobacterial heat shock proteins modify nuclear transcription elements within the macrophage. Ultimately reactive nitrogen intermediates, in addition to reactive oxygen intermediates, lysosomal enzymes and toxic peptides are answerable for mycobacterial killing. Activated T cells then return to the positioning of infection within the lung via the bloodstream. These delayed-type hypersensitivity and cell-mediated immune responses often include the mycobacteria inside granulomas. Within each the macrophages and the strong caseous facilities, organisms are both inactive or replicate very slowly. The granuloma is a well-organized construction, which effectively seals off the mycobacteria from the rest of the host. Liquefaction of the central caseous necrosis creates an inviting extracellular environment for M. The pathogenesis of environmental mycobacterial infection has been little studied. An isolated tuberculoma can be seen in surgical specimens as a half of investigation of a single strong lesion. Frequently cavitated lesions are seen in upper zones and differ in dimension from 1:2 cm to as giant as 10 cm. In late-stage illness, a lot of the inflammation has resolved and has been changed by fibrosis. These organism-harboring histiocytes are surrounded by varying numbers of lymphocytes, ranging from scattered to a dense lymphocytic "belt". The facilities of these granulomas characteristic putting parenchymal necrosis however granulomas may remain non-necrotizing. The cellular response in immunosuppressed/immunocompromised individuals may be decreased and a full granulomatous response could not occur. Vasculitic process in a pulmonary artery department in a patient with tuberculous consolidation. Well-demarcated non-necrotizing granulomas in a mediastinal lymph node resemble sarcoidosis. Thin, shiny red bacilli in an space of caseous necrosis demonstrated with Ziehl-Neelsen stain. After the primary inhalation, a brief acute inflammatory response happens, followed by a delayed cell-mediated hypersensitivity reaction which ends up in the granuloma formation. The Ghon focus is usually subpleural or round fissures and may occur in either lung. Mycobacteria additionally drain to hilar lymph nodes, which may turn into enlarged by quickly established caseous and granulomatous lymphadenitis. The major pulmonary lesion related to the regional hilar lymph node granuloma is known as the primary or Ghon advanced. In infants, who may not mount a mature immune response, a rapid unfold of a main advanced can lead to tuberculous bronchopneumonia, due to erosion of the granulomatous lesion into a bronchus, atelectasis and air trapping. If erosion happens into a blood vessel, miliary disease, together with meningitis, may develop. In extreme circumstances, tuberculous lymphadenopathy may lead to erosion or perforation of the esophagus by a tracheoesophageal fistula. The average age for tuberculous pleurisy varies amongst case sequence but young adults and the elderly appear to be the most affected age teams. This lesion, whereas not calcified, is longstanding given the focally distinguished fibrous capsule. On uncommon events, granulomatous nodules on the pleural floor without parenchymal or nodal affiliation have been described. Secondary pulmonary tuberculosis the standard pathway to secondary pulmonary tuberculosis follows additional inhalation of M. Also note the presence of bronchiectasis in the lower segments (bottom left and right). The infectious process has eroded into an airway and involves an adjacent intraparenchymal lymph node. This is an try and neutralize and isolate the necrosis from the encircling lung.
Aristocort 10 mg discount visa
Scanning electron microscopic analysis of mineral fiber content material of lung tissue within the evaluation of diffuse pulmonary fibrosis allergy zone map aristocort 15 mg discount otc. Mortality of employees licensed by a pneumoconiosis reference panel as having asbestosis allergy testing geelong aristocort 10 mg generic. Autopsy circumstances of asbestosis in Japan: a statistical evaluation on registered circumstances Arch Environ Health 2000;55:447:fifty two. Mortality experience of insulation staff in the United States and Canada, 1943:1976. Pulmonary fibrosis in asbestos insulation staff with lung cancer: a radiological and histopathological analysis. The quantitative danger of mesothelioma and lung most cancers in relation to asbestos publicity. A metaanalysis of asbestos-related most cancers danger that addresses fiber dimension and mineral sort. Follow up study of chrysotile textile workers: cohort mortality and exposure response. After Helsinki: a multidisciplinary review of the relationship between asbestos publicity and lung most cancers, with emphasis on studies printed throughout 1997:2004. The "Helsinki criteria" for attribution of lung most cancers to asbestos exposure: how strong are the criteria The second diagnosis: the position of the pathologist in identifying pneumoconiosis in lungs excised for tumor. Relationship between occupations and asbestos fibre content of the lungs in sufferers with pleural mesothelioma, lung most cancers and different diseases. The optical and electron microscopic willpower of pulmonary asbestos 556 Chapter 14: Occupational lung disease fiber focus and its relation to the human pathologic response. American College of Chest Physicians Consensus Statement on the Respiratory Health Effects of Asbestos: Results of a Delphi Study. Distribution and characteristics of amphibole asbestos fibres in the left lung of an insulation employee measured with the sunshine microscope. A simple methodology for preparing ferruginous bodies for electron microscopic examination. Relationship between lung asbestos fiber kind and concentration and relative risk of mesothelioma: a case management study. Asbestos burden in circumstances of mesothelioma from people from numerous areas of the United States. Inorganic fibers in lung tissue from sufferers with pleural plaques or malignant mesothelioma. Accuracy of transmission electron microscopy for the analysis of asbestos in ambient environments. Comparisons of the pathogenicity of long and quick fibres of chrysotile asbestos in rats. Relation of particle dimension to carcinogenicity in amphibole asbestoses and other fibrous minerals J Natl Cancer Inst 1981;67:965:seventy five. Deposition pattern of inorganic particles at the alveolar degree of the lungs of rats and mice. Generation of free radicals from freshly fractured silica dust: potential position in silica-induced lung injury. Experimental alveolar 557 Chapter 14: Occupational lung illness lipoproteinosis following the inhalation of silica. Risk of pulmonary tuberculosis relative to silicosis and publicity to silica dust in South African goldminers. Certain unusual radiological appearances within the chest of coal miners affected by rheumatoid arthritis. Lung cancer and dirt exposure: results of a prospective cohort study following 3260 employees for 50 years. Occupational silica publicity and lung cancer risk: a evaluation of epidemiologic studies 1996:2005. Lung cancer mortality amongst silicotic staff in Hong Kong-no proof for a hyperlink. Proposed criteria for combined mud pneumoconiosis: definition, descriptions and tips for pathologic prognosis and clinical correlation. National Institute for Occupational Safety and Health the Work-related Lung Disease Surveillance Report 2002. Mineral dusts cause elastin and collagen breakdown in the rat lung: a possible mechanism of dust-induced emphysema. Extent of pulmonary pigmentation as an indicator of particulate environmental air pollution. Coalworkers pneumoconiosis and pneumoconiosis due to other carbonaceous dusts, Chapter 6. Risk of gastric cancer in pneumoconiotic coal miners and the impact of respiratory impairment. Particle size for differentiation between inhalation and injection pulmonary talcosis. Lung most cancers risk and talc not containing asbestiform fibers: a evaluate of the epidemiologic evidence. Effects of phagocytosis of mineral dusts on elastase secretion by alveolar and peritoneal exudative macrophages. Erionite bodies and fibres in 559 Chapter 14: Occupational lung disease bronchoalveolar lavage fluid of residents of Tuzkoy, Cappadocia, Turkey Occup Environ Med 2001;fifty eight:261:6. Vermiculite, respiratory illness and asbestos publicity in Libby Montana: update of a cohort mortality examine. Fiber contamination of vermiculites: a possible occupational and environmental well being hazard. Mortality in a cohort of vermiculite miners exposed to fibrous amphibole in Libby, Montana. Beryllium sensitization progresses to persistent beryllium disease: a longitudinal research of threat. Nonoccupational beryllium disease masquerading as sarcoidosis: identification of blood lymphocyte proliferative response to beryllium. Bronchogenic cancer and non-neoplastic respiratory disease related to beryllium publicity. Dusts and Disease: Occupational and Environmental Exposures to Selected Fibrous and Particulate Dusts. The organic motion of tungsten carbide and cobalt: studies on experimental pulmonary histopathology. Two dimensional evaluation of elements and mononuclear cells in hard metal lung illness. Cobalt exposure and lung disease in tungsten carbide production: a cross-sectional study of current staff. Giant cell interstitial pneumonia in a hard-metal employee: cytologic, histologic, and analytical electron microscopic investigation.
40 mg aristocort order visa
The arrows point out discrete nodular foci of scar tissue centered on the bronchovascular bundles allergy testing reaction aristocort 4 mg buy discount online. The lesions were categorized as complete or subtotal narrowing and lively if intra- and/or peribronchiolar mononuclear cell infiltrates have been present allergy treatment for 18 month old 4 mg aristocort purchase with mastercard. If current, mononuclear inflammatory cells are distributed inside the submucosal fibrosis and/or in the peribronchiolar tissue spaces. At scanning magnification complete luminal obstruction may be simply ignored on H&E stains and cautious attention to the parenchyma adjoining to the muscular pulmonary arteries is essential. The scar tissue can extend distally into the alveolar ducts and sacs and septal scarring is often present. Mucostasis and/or intraluminal foam cells within the distal airways are markers of airway obstruction. The pathogenesis might be multifactorial and entails recurrent bacterial or fungal infections, mucous plugging, denervation of the allograft and distal airway obstruction (see Chapter 17). Fibromyxoid plugs of granulation tissue in the small airways could be present in quite lots of organizing airway damage patterns together with resolving rejection, organizing an infection, ischemicreperfusion injury and drug toxicity. With the exception of retransplantation, therapies solely produce temporary "stabilization" within the price of decline of measured pulmonary operate. Recurrent illness in the allograft the list of issues which have recurred in the transplant allograft expands yearly and is published as case reviews and small sequence (Table 7). Infection must be excluded in all instances of granulomatous inflammation after transplantation. Future directions Great strides have been made in patient choice and management after transplant. However, numerous serious points remain and constitute impediments to lung transplantation. Firstly, the pool of lungs obtainable for transplant has remained stagnant during the last two decades despite the increasing number of potential candidates for transplant in North America and Europe. Less than a fifth of lungs are actually considered appropriate or available for donation and a 3rd or extra patients die on the wait-list. A number of methods underneath experimental and medical investigation may increase the donor pool by reconditioning marginal lungs into acceptable grafts. The method has moved into the medical area and small collection have been printed selling its success. A variety of small sequence have been printed exhibiting some success as a bridging method. The total incidence has not modified considerably though the medical onset is delayed. As molecular mechanisms are clarified, prevention somewhat than therapy becomes the goal. To date retransplantation is the one definitive remedy but there are a variety of technical, ethical and management points to be considered. The registry of the International Society for Heart and Lung Transplantation: thirteenth official pediatric lung and heart-lung transplantation report- 2010. The registry of the International Society for Heart and Lung Transplantation: twenty-seventh official adult lung and heart-lung transplant report- 2010. Analytical strategies and database design: implications for transplant researchers, 2005. Bilateral pulmonary lobe transplantation: left decrease and proper center and lower lobes. Long-term outcomes of cadaveric lobar lung transplantation: serving to to maximize assets. Lung transplantation for chronic obstructive pulmonary illness: particular issues. Increasing lung allocation score predict worsened survival amongst lung transplant recipients. Pulmonary Scientific Council of the International Society for Heart and Lung Transplantation. International tips for the choice of lung transplant candidates: 2006 update: a consensus report from the Pulmonary Scientific Council of the International Society for Heart and Lung Transplantation. Audit of referral and explant diagnoses in lung transplantation: a pathologic examine of lungs eliminated for parenchymal disease. Single-lung transplant complicated by unexpected explant carcinoma: a management dilemma. Discrepancies between medical and post-mortem diagnoses in lung transplant recipients. Molecular profiling improves diagnoses of rejection and infection in transplanted organs. Cylex ImmuKnow assay levels are lower in lung transplant recipients with an infection. Experience with monitoring in lung transplant recipients: correlation of low immune function with an infection. Evaluation of heart-lung transplant recipient with potential, serial transbronchial biopsies and pulmonary perform studies. Prospective examine of transbronchial biopsies in the management of heart-lung and single lung transplant patients. The function of transbronchial lung biopsy within the therapy of lung transplant recipients. The function of transbronchial biopsies within the management of lung transplant recipients. Yield of surveillance bronchoscopy for acute rejection and lymphocytic bronchitis/bronchiolitis after lung transplantation. Single-institution examine evaluating the utility of surveillance bronchoscopy after lung transplantation. A working formulation for the standardization of nomenclature within the diagnosis of coronary heart and lung rejection: Lung Rejection Study Group. Revision of the 1990 working formulation for the classification of pulmonary allograft rejection: Lung Rejection Study Group. Pathologic interpretation of transbronchial biopsy for acute rejection of lung allograft is extremely variable. Interpretation of transbronchial biopsies from lung transplant recipients: interand intraobserver agreement. Bronchiolitis obliterans syndrome in lung transplant recipients is related to increased neutrophil activity and decreased antioxidant standing within the lung. Role of open lung biopsy for diagnosis in lung transplant recipients: ten-year expertise. Primary graft dysfunction: definition, danger components, short- and long-term outcomes. Impact of quick main lung allograft dysfunction on bronchiolitis obliterans syndrome. Concomitant endothelin-1 overexpression in lung transplant donors and recipients predicts primary graft dysfunction.